
Abstract
Introduction
Almost half of US adults have hypertension (HTN) and those with low-income are more likely to have worse blood pressure (BP) control. To help manage BP, recent interventions have introduced remote, or at-home, BP monitoring.
Objective
To assess the feasibility of a subscriber identity module (SIM)-enabled remote BP monitoring (RBPM) intervention among individuals with HTN living in low-income housing.
Methods
A prospective, observational cohort pilot study of 15 low-income older adult participants was conducted. RBPM was delivered through CareSimple®, a cloud-based, SIM-enabled, remote BP cuff. Participants were asked to check their BP at least twice weekly for 4 months, and readings were monitored via a central dashboard. Feasibility and acceptability were measured by the feasibility of the intervention measure (FIM) and acceptability of the intervention measure (AIM) via survey and semi-structured interviews. Data analyses were by descriptive and paired t-test statistics, and qualitative descriptive analysis.
Result
Fourteen participants with an average age of 76.5 years (SD: 9.0) completed the study. The AIM and FIM mean scores at month 4 were 4.14 (SD: 0.70) and 4.27 (SD: 0.67), respectively (scale: 1–5). Facilitators of the intervention included positive perceptions of the BP device, text messaging, and the onsite champion. Barriers were BP measurement and accuracy concerns, lack of appropriate home furniture, and negative perception of text messaging. At month 4, there were non-statistically significant decreases in average systolic BP (mean difference −3.9 mm Hg), and diastolic BP (mean difference −1.4 mm Hg).
Conclusion
SIM-enabled BP remote monitoring with text messages was feasible and acceptable in older adult low-income housing residents with HTN.
Keywords
Introduction
Hypertension (HTN) is a common chronic condition that affects nearly half of adults in the United States. 1 Uncontrolled blood pressure (BP) can lead to significant mortality and morbidity including stroke, heart diseases, and target end-organ damage.2,3 Among adults with HTN in the United States, those with low income have worse BP control and outcomes.4–6 This disparity in HTN control has been shown to persist despite access to appropriate drug treatment and regular clinic follow-up visits. 4 Individuals with HTN and low income have significantly lower adherence to clinic visits compared to their higher-income counterparts. 4 To help manage BP, multifaceted approaches, including patient empowerment to use self-measured BP monitoring, have been proposed.2,7,8 Therefore, recent interventions have introduced remote, or at-home, BP monitoring.
Remote BP monitoring (RBPM) entails self-measurement of BP at home with automated or manual transmission of the measurement to healthcare providers through electronic communication technologies. 9 The healthcare providers review the BP and provide feedback to patients through electronic means. Greater BP control has been demonstrated among people with HTN participating in RBPM compared to those who were not.10,11 RBPM can also be accompanied by additional intervention components such as health education, peer mentors, nutrition support, medication adherence, and BP monitoring reminders. BP control interventions that include individually tailored support components have led to clinically significant BP reduction.12,13
Though there are several studies on the association of low income with poor BP control among adults with HTN,4–6 few have focused on the feasibility of achieving BP control with the use of an RBPM intervention. 14 Low-income housing facilities offer an opportunity to recruit individuals who are exclusively low-income earners. The objective of this study was to pilot the implementation of RBPM for individuals with HTN who resided in low-income housing. The RBPM was done using a subscriber identity module (SIM)-enabled, RBPM system and text messages. Specifically, we (1) assessed participants’ characteristics, feasibility, and acceptability of the RBPM intervention, (2) described the facilitators and barriers of RBPM with text messages in a low-income housing facility over a 4-month period, (3) quantified the percent of participants at BP goal (< 140/90) who used RBPM with text messages in a low-income housing facility over a 4-month period, and (4) assessed the satisfaction with and usefulness of an onsite champion for intervention sustainability.
Methods
Design
The study was a prospective, single-arm observational cohort pilot study that recruited 15 residents living in a low-income older adult housing property owned by the Ann Arbor Housing Commission, in Ann Arbor Michigan. We were exploring the feasibility of using this technology in supporting BP monitoring in this housing facility. There was no control group. We followed the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guideline for reporting observational cohort studies. 15
Setting
The study was led by investigators at the University of Michigan, which is a public research university. The University of Michigan Hospital, also referred to as Michigan Medicine, is the academic medical center of the university. In addition to physicians, Michigan Medicine has clinical pharmacists who manage patients with HTN. Some participants received their primary care from providers at Michigan Medicine, while others received care from providers outside the university.
Ethical considerations
The study was approved by the University of Michigan Institutional Review Board (IRBMED HUM00206203). Informed consent was obtained from participants before they were enrolled in the study. The survey and interview data collected from participants were coded prior to analysis. The BP data were only accessible to the research team with a password to the secure central dashboard and exported after the study for analysis. Study participants were offered a total of $40 for completing study activities, divided into $10 for each completed survey (baseline, Month 4) and $10 for each interview (in Month 1 and Month 4).
Study sampling and participants
We used a purposive sample of older adults ≥ 62 years (the age requirement for residing in the low-income facility). The inclusion criteria were people who self-reported a diagnosis of HTN, took a medication for HTN, and had the physical and cognitive capacity to use a smartphone, cell phone or similar technology, and were willing to sign a consent form. The exclusion criteria included people who were unable to communicate in English language and those with cognitive impairment.
Power calculation
A study published by Margolis et al. 16 on home BP telemonitoring intervention reported that a mean difference in systolic BP change between the telemonitoring intervention group and the usual care group was −10.7 mm Hg (95% CI, −14.3 to −7.3 mm Hg, P < 0.001) and the mean difference in diastolic BP was −6.0 mm Hg (95% CI, −8.6 to −3.4 mm Hg, P < 0.001) at 6 months. Given these parameters and assuming we want 80% power with alpha value of 0.05, we needed total sample sizes of 29 and 47 to detect changes in systolic and diastolic BP, respectively. Given this was a feasibility study, we were comfortable with convenience sampling to help us determine study procedures and our own sample estimates.
Recruitment
The investigators had previously established a relationship with residents at the Ann Arbor housing facility, as we began providing health education sessions in June 2021. We conducted a health needs assessment, as requested by the Ann Arbor Housing Commission leadership, asking residents about their self-rated health, the location of their primary care physicians, their desire for internet for telehealth visits, and their desire to have an in-house clinic. At the same time, we asked if anyone would be interested in RBPM, and participants were able to sign a form and return it to us for future contact. We contacted individuals who expressed interest in RBPM and asked if they wanted to learn more about the study. We also posted the study flyer at the facility and hosted a group session of residents at one of their usual residents’ meetings. At the group session, the principal investigator and the research assistant (RA) provided information about the study, solicited study interest, and compiled names and telephone numbers of potential participants. Potential participants were telephoned for more discussion about the study, screened for eligibility and confirmed interest. Recruitment occurred from April 2022 to September 2022. We reached out to 34 interested individuals and enrolled 15 residents in the study (Figure 1).
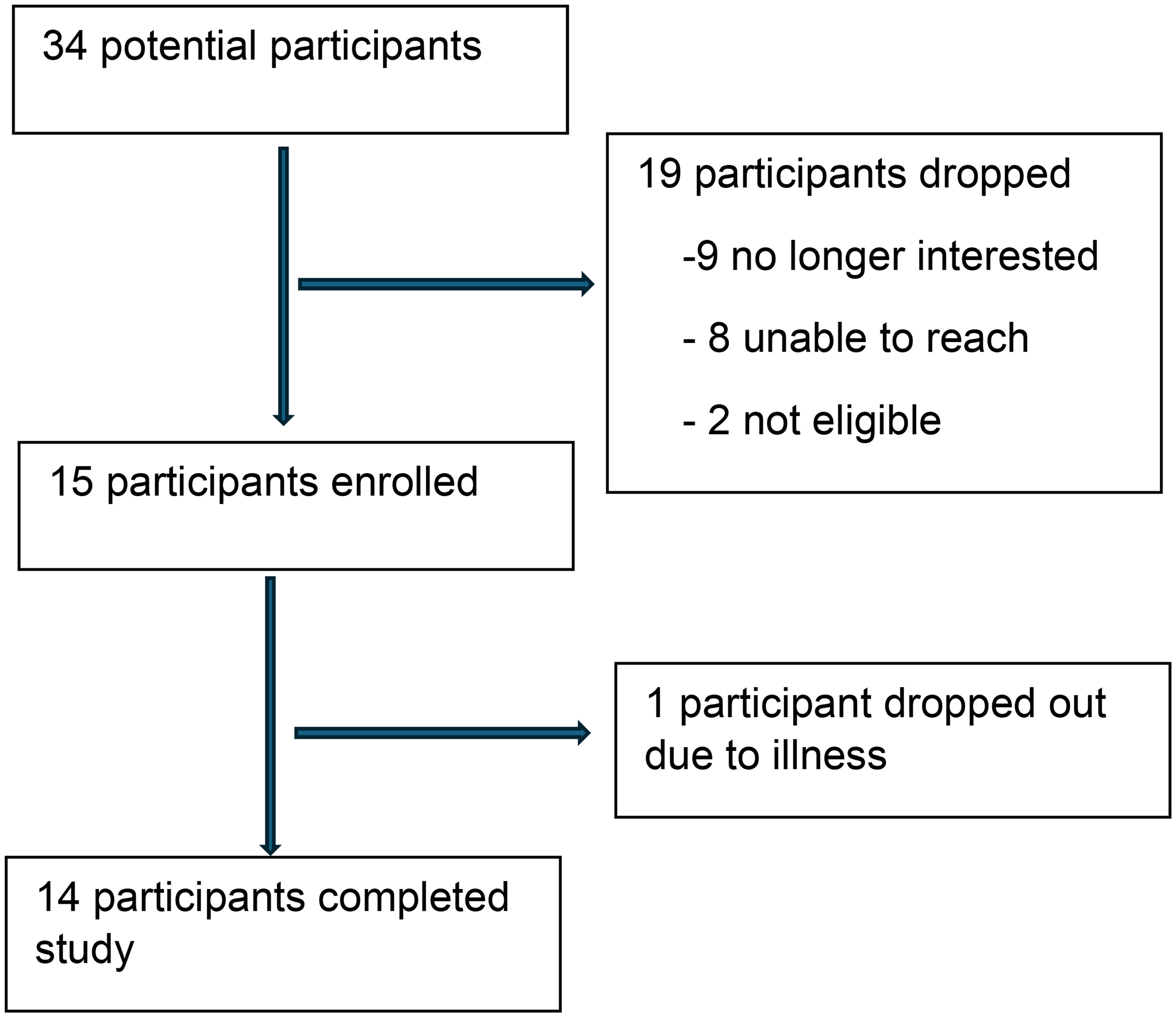
Flow chart of recruitment.
Study procedure
If eligible and interested, the RA set a time to meet with potential participants to explain the study, confirm eligibility, obtain informed consent, and enroll them into the study. All study visits were individual and in person.
The study components included (1) letter sent to primary care providers telling them that their patient was enrolled in RBPM study, (2) RBPM device, (3) SMS text messages, and (4) onsite remote BP monitoring champion.
Notification of primary care provider
When primary care providers were within Michigan Medicine, we notified the providers and clinical pharmacists who managed BP in those clinics by HIPAA-compliant email. Where the participant's primary care provider was outside of Michigan Medicine, we sent a letter via United States mail to notify them of participation in this study. At the end of the study, we sent a copy of each participant's 4-month BP report to their primary care provider in a similar fashion.
Remote BP monitoring
The RBPM was delivered through the CareSimple® platform, 17 which is an FDA-approved, cloud-based, SIM-enabled, remote health monitoring service that offers RBPM devices. As the BP device is SIM-enabled, it does not require WiFi to transmit data to the cloud server, eliminating a potential barrier to participation in interventions like ours. Each participant received a CareSimple® portable automated in-home BP monitor with upper arm cuff and an in-person tutorial on how to use it and transmit readings. The in-home BP cuff was pre-configured to work immediately out-of-the-box (no app, pairing or WiFi required). Patients and the study team could access the collected data via a central dashboard by logging into the platform or downloading the CareSimple® App on a smartphone. For this pilot study, participants were not required to download the CareSimple® App and none asked to do so.
Along with the BP monitor, participants were provided with a paper folder which contained detailed information about the study, instructions on how to use the BP monitor, and research team contact information. The RA trained participants on proper BP measuring technique. Participants were instructed to sit upright on a chair with their back supported, feet flat on the floor, no talking, and their upper arm at their heart level before taking the BP measurement. Participants were instructed to check their BP at least twice per week for 4 months with the CareSimple® device, as they were required to submit at least 8 BP measurements for each month of the study. Participants submitted one BP each time.
Text messages
SMS text messaging is a readily accessible and acceptable way of engaging patients with HTN in BP monitoring and medication adherence.18,19 In our study, individuals received a maximum of four texts per week (Table 1, section 1). One text message was a BP-taking reminder on Mondays, the second was in response to the first BP reading sent each week, and the third was a BP medication-taking reminder. Individuals received a fourth message if only one or no BP reading had been received by Friday. We standardized messages for responding to the BP levels (Table 1, section 2). The participants’ BPs were considered as being controlled if they were ≤140/90 mm Hg.
Blood pressure program text messaging protocol*.

BP: blood pressure; SBP: systolic blood pressure; DBP: diastolic blood pressure.
The reminder texts typically occurred in the mornings, between 9am and 10am and were automated. The BP feedback texts were sent manually in the evenings between 5pm and 7pm and were tailored depending on the participant's BP measurements.
Onsite champion
An onsite champion was employed by the study to support participants with the technology, encourage its continued use, and respond to participant questions. We posted the position on the bulletin board in the facility seeking a resident who had HTN, was familiar with technology, able to use the BP remote system, had a smart phone, and was willing to talk with residents in the hallway or at meals every week about their BP monitoring. We interviewed three interested individuals to confirm eligibility, and one resident was chosen for the onsite champion position by the study team.
The onsite champion was paid $50 per month by the study and was not a study participant. The onsite champion was considered study staff, and they completed IRB training, received training about BP goals, and use of the texts contained in the text messages plan to ensure that they responded in a similar manner if a participant discussed his/her BP. The onsite champion knew which residents in the housing facility were participating in the study, but she did not have access to participant data, including survey or interview data, text messages to specific individuals, or BP data from the CareSimple® devices. The onsite champion was informed by study staff when a participant did not submit their BPs for two weeks, and the onsite champion would talk with participants about their use of the BP device and their willingness to submit their BPs. The onsite champion could contact the principal investigator or RA via text or phone with questions at any time.
Data collection
The concepts and timeframe listed in Table 2 were measured using a paper survey (Appendix 1), key informant interviews (Appendix 2) and the data from the remote BP system assessments as outlined. Participants’ demographic data were collected. The feasibility of intervention measure (FIM) 20 was used to assess the ease of planning and use of the BP device. FIM is a validated 4-item questionnaire scored on a 5-point Likert scale ranging from completely disagree to completely agree. The higher the score, the higher the feasibility of the intervention. The acceptability of intervention measure (AIM) 20 is validated 9-item survey that assessed respondents’ acceptance of the BP device, text messages, and the onsite champion on a 5-point Likert scale. The higher the score, the greater the acceptance of the intervention. We also collected, frequency of BP checking at baseline, and number HTN medications taken.
Data collection concepts, mode and timeframe.

M1: month one after four weeks of use; M4: month four, BP: blood pressure.
Key informant interviews were conducted by the RA with participants at their housing facility in the lunchroom or similar setting. A time was selected when the setting was private and not busy. We focused on the three aspects of the intervention including RBPM device, texting, and the onsite champion, and asked about the participants’ perception of them. Examples of the questions include, “Thinking about the BP device, text messages, and your onsite champion, which did you like best and which did you like least and why?”; “Tell me the good things about the BP device, text messages, and the onsite champion”; “Tell me the more difficult things about the BP device, text messages, and the onsite champion” (Appendix 2). All interviews and survey data were collected in person. Each interview lasted about 20 min. The interviews were not recorded; rather the RA made handwritten notes recording the participants’ responses. We chose not to record the interviews because we wanted to provide a comfortable environment for participants to speak freely about all aspects of the intervention.
The data collected were stored in a locked cabinet and password-protected computers that were only accessible to the study team.
Data analysis
Survey data were analyzed using descriptive statistics or frequency distributions for participant characteristics, adoption, fidelity, and satisfaction. Scale scores for feasibility and acceptability were generated. Scores at the end of M1 and M4 were compared using a paired t-test. The percentage of participants at self-reported BP at goal was examined using a chi-square analysis for M1 and M4. For statistical testing, we considered an alpha of 0.05 as statistically significant. R statistical software, version 4.4.2 was used for all quantitative analyses. 21
Interviews gathered qualitative data about feasibility, acceptability, and usefulness. Interview summaries and analyst memos were analyzed using qualitative descriptive analysis.22,23 These data were analyzed using a hybrid thematic analysis approach. 24 First, we used structural coding as described by Saldaña 25 to segment the interview summaries based on the questions that were asked. Then, the RA and principal investigator reviewed the summaries and identified the specific aspect of the barrier or facilitator mentioned by participants; these specific aspects were then coded in a second-level coding process. Finally, we summarized and grouped our coded data into facilitators or barriers to RBPM intervention. The Microsoft Excel® was used for the qualitative analysis. The qualitative reporting followed the COREQ checklist. 26
Results
No objections from the participants’ providers regarding their participation in the RBPM study were received. One participant could not complete the study due to illness that made it difficult to adhere to study requirements. Data from 14 participants were used for the analysis.
Participants’ demographics
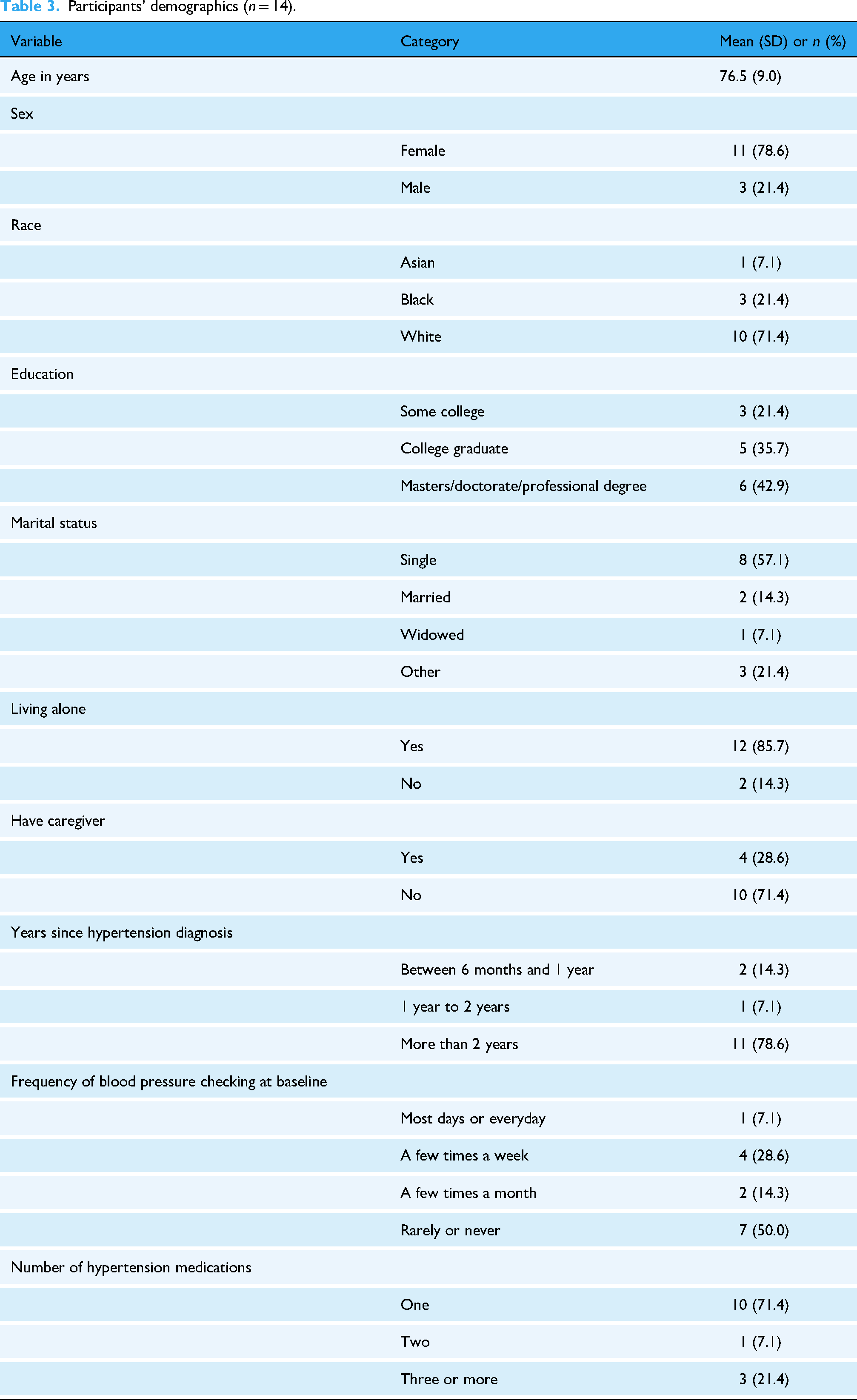
The mean age of participants was 76.5 years (SD 9.0) (Table 3). Participants were predominately female (78.6%). All participants were non-Hispanic (100%), and mostly White (71.4%). All participants had attended some college or completed higher education. Most participants were single (57.1%) and only two were married. All participants lived alone except for the two who were married. Most participants had an HTN diagnosis for over two years (78.6%) and half of them rarely or never checked their BP prior to enrollment in the study. Arthritis or osteoporosis were common comorbidities (78.6%) followed by depression (50%).
Participants’ demographics (n = 14).
Feasibility of intervention
The feasibility of the intervention in terms of ease to do RBPM means increased significantly in month 4 (M4) compared to month 1 (M1) (Table 4).
Mean feasibility of intervention scores at M1 and M4.

Acceptability of intervention
The acceptability of intervention mean scores were high at month 1 (M1) and remained high at month 4 (M4) with no significant change between the months (Table 5).
Mean acceptability of intervention scores at M1 and M4.

BP monitoring
Most participants submitted more than the required 8 BP measurements for each month. In the first month (M1), a total of 246 BP submissions were made giving an average of 17.6 (SD 7.0) submissions per participant. From the first month to the fourth month, a total of 892 BP measurements were received from all participants. Submission of 8 BP measurements per month was defined as 100% adherence to the BP monitoring for each month, and 9 of 14 participants showed perfect adherence to the protocol. Most participants (64.3%) submitted 8 or more BP measurements for each month of the study.
The BP measurement submissions in the first month of intervention were used as the baseline BP (Figure 2) and graphically show decreases in BP. The mean systolic BP at baseline was 141.1 mm Hg (SD: 16.6), and at the end of study (M4) was 130.7 mm Hg (SD: 19.0) with a mean difference of −3.9 mm Hg, (p = 0.22; effect size (Cohen's d) = 0.34). The mean diastolic BP at baseline was 79.2 mm Hg (SD: 10.1), and at M4 was 74.0 mm Hg (SD: 9.7) with a mean difference of −1.4 mm Hg, (p = 0.35; effect size (Cohen's d) = 0.26). The percentage of participants with controlled BP at baseline was 42.9% and increased non-significantly to 57.1% at the end of the study.

Mean systolic and diastolic blood pressure through M1 to M4 (red lines show overall means and confidence interval).
A total of 896 text messages including BP checking reminders, BP medication taking reminders, and BP feedback messages were sent to all participants throughout the 4-month study duration with each participant receiving a mean number of 64 (SD: 7.4) messages. The mean number of text messages sent to the participants in the first, second, third, and fourth months were 18.9 (SD: 3.8), 18.4 (SD: 5.0), 13.2 (SD: 1.8), and 13.5 (SD: 1.1), respectively. The reminder messages for BP and medication taking constituted an average of 10.5 (SD: 1.6) text messages per participant monthly. A total of 234 feedback text messages were sent in response to the BP measurements received from participants with an average of 16.7 (SD: 5.2) messages per participant. These messages served as reminders and as encouragement and assurance that someone is working with them in their BP management journey.
Facilitators of RBPM intervention with text messages
The analysis of the interview notes from the participants resulted in three categories of facilitators including positive perceptions on the BP device, text messages, and onsite champion.
Positive perception of the BP device
The participants noted the following attributes of the BP device as being very helpful in their engagement in the RBPM intervention: Simplicity and ease of use, automated quick measurement output just with a touch of a button, device portability, remote BP data transmission without note-taking, accuracy of BP measurement, and the knowledge that someone is remotely monitoring your health with you.
Positive perceptions of text messaging
Most participants expressed that the reminder messages were helpful with their BP taking and medication adherence. The feedback BP messages were considered informative, motivative, and encouraging. The messages provided confirmation that the BP measurements were transmitted, and someone was watching and caring for them. The consistency and timeliness of the messages were appreciated.
Positive perceptions of the onsite champion
The participants supported the idea of having someone who is knowledgeable about the RBPM intervention and lives among them, so they can reach out anytime for questions and concerns.
Barriers to RBPM intervention with text messages
The barriers to RBPM intervention with text messages were categorized into four parts including improper BP measurement techniques, accuracy of measurement concerns, lack of appropriate environmental resources, and negative perceptions of text messaging.
Improper BP measurement technique
Participants expressed some challenges with being able to fit their BP cuffs themselves. Most needed more practice with the cuff to get comfortable with it. As soon as they were able to grasp the technique, they were excited about doing their BP self-monitoring.
Accuracy of measurement concerns
The concern for the accuracy of BP measurements stemmed from improper BP cuff fitting. Some participants were getting different BP readings that made them question the accuracy of the BP measurements. It also came from the concern that sometimes their home BP readings measured with the CareSimple® BP device were different than their clinic BP readings and other company's home BP device.
Lack of appropriate home furniture
Some participants noted that they lacked adequate furniture, such as tables and chairs, to use for BP measurement. Appropriate BP measurement requires that the individual be in a position where they can comfortably sit upright with support for their back, feet flat on the floor, and have support for their arm to be at heart level.
Negative perception of text messaging
Two participants thought the text messaging was stressful and annoying. They felt they didn’t need reminders and could take care of themselves. One of them expressed that it made them feel like they are children that needed to be reminded to do things. They thought the messages were too short and not very informative, needing more information.
Onsite champion
The satisfaction and usefulness of the onsite champion were assessed quantitatively within the acceptability of intervention survey and qualitatively during the participants interviews. The acceptability mean score for the onsite champion was 4.14 (SD 0.86) at month 1 and decreased to 3.86 (SD 1.03) at month 4 (Table 5). At the interviews, the participants expressed satisfaction with having an onsite champion. They acknowledged the necessity of having someone who lives among them to approach with questions or concerns. However, at the end of the study, very few participants found the onsite champion useful, as most participants expressed not having reasons to reach out to the onsite champion.
Discussion
Overall impact of SIM-enabled RBPM intervention
This study investigated the implementation of RBPM for participants with HTN who lived in low-income housing and demonstrated that SIM-enabled RBPM is beneficial and acceptable. Overall, the RBPM device was easy to use, and the text messages were effective in providing feedback about participants’ BP. The onsite champion was acceptable in the early phases but not needed later on. Participants enjoyed knowing someone was monitoring their BP, but statistically significant differences in BPs and BP control were not shown.
Facilitators of participation in the RBPM study included the easy-to-use SIM-enabled BP device that did not require WiFi, text message reminders, and the availability of an onsite champion. In general, most patients had favorable responses to the implementation of the SIM-enabled RBPM system as indicated by the feasibility of intervention scores. A study conducted by Albrecht et al. which qualitatively examined the usability and acceptability of RBPM in elderly individuals had similar conclusions to our study which indicated that the use of SIM-enabled BP monitoring is acceptable and has favorable usability amongst study participants. 27 Providing patients with a tool that is accessible, relatively easy to use, and involves a patient-centered process that is inclusive of their healthcare team can be beneficial in improving health outcomes. Having an at home-BP cuff provides benefits to patients, such as having the ability to conduct multiple BP measurements, reproducibility, eliminating the possibility of white coat HTN, and providing patients with the opportunity to learn and understand more about HTN and managing it. 28 A SIM-enabled home-RBPM cuff provides all the benefits of at home-BP cuff with additional benefits including automatic transmission of BP measurement to patient's healthcare provider, removing the burden from the patient (especially the elderly) and ensuring the accuracy of transmissions. 14 Automatic BP transmissions can also increase health providers’ oversight, and integration of BP data with the patients’ electronic health records would reduce workflow changes. A SIM-enabled device reduces health disparity among low-income populations by eliminating the need for expensive high-speed internet and cloud services for RBPM services. 29 A SIM-enabled at home-RBPM device provides a readily available, simpler way of improving BP control and saving healthcare cost in the long term. 30 We found that participants in our study had a positive perception of the SIM-enabled BP device itself due to its ease of use, accuracy, and ability to allow a member of their healthcare team to monitor their health with them.
Also, most participants had a positive perception of the text messaging feature, which was found to be helpful in reminding them to take their BP and take their medications. Text messaging has been found useful in HTN control studies as it is a readily accessible and easy-to-use technology.18,19 The negative perceptions on text messaging could be managed in a future intervention by limiting the number and content of the messaging to individual patient's preferences. Individual preferences could be determined over time for these messages. The onsite champion was initially positively perceived by participants, as well, because it provided them with a sense of comfort knowing that there was an individual designated to assist with questions and concerns that they may have. Having a social support system has been shown to improve adherence to BP monitoring and medications among people with HTN.31–33 Over time, this resource did not seem necessary because our study participants became more comfortable with using their BP device and did not feel the need for support any longer.
Barriers to RBPM participation noted during the study included participants facing challenges with fitting their BP cuffs, which was remedied after practice. When this was an issue, it led to concerns as to whether BP was being measured correctly. This points to the importance of acquiring the skills and knowledge needed to engage in digital services like RBPM, also known as electronic health literacy. 34 High electronic health literacy would enable participants to differentiate issues with the BP monitor itself versus the use of the cuff. Healthcare providers providing patients’ training on these skills routinely could be very beneficial. With the appropriate literacy, digital BP monitors can be used correctly thereby increasing trust in the measurements produced.35,36 As well, having the proper home environment was also noted by participants due to some not having a table or chairs to be able to properly sit and position themselves for a more accurate BP reading. This barrier draws attention to an environmental challenge that could be easily overlooked. Home BP monitoring is one of the recommended guidelines for HTN diagnosis and monitoring because it helps eliminate white coat and masked HTN. 29 Having appropriate furniture to take the BP measurements at home is therefore essential. Wrong BP measurements could result in worsening health conditions and even greater health costs in the elderly and low-income population. In addition to providing access to RBPM devices, individuals training patients on home BP measurement techniques could inquire about the availability of appropriate BP measurement settings in patients’ homes. When the inquiry suggests inability to provide the appropriate furniture, healthcare providers could encourage patients to reach out to local, community, or non-profit organizations that could help them with these resources. It may also be possible to access an appropriate setting with the right table and chair within their apartment building (but outside their home) like our study participants did to remedy the situation.
Impact on HTN control
Studies have reported that an average of 5 mm Hg reduction in systolic BP is clinically significant in reducing major cardiovascular risks by 10%. 37 Therefore, the mean 3.9 mm Hg reduction in systolic BP findings from our study, though non-statistically significant is clinically significant and likely reduced participants’ cardiovascular risks by some percentages. The non-statistically significant result is likely due to our study having sample size with insufficient power to detect significant BP differences. Additionally, the number of participants with controlled BP increased from baseline to the end of the study. These results support the beneficial nature of implementing a SIM-enabled, RBPM system, which is an exemplary method in improving chronic diseases such as HTN. Several studies have found that the implementation of an RBPM system significantly improved BP levels in patients.38–41 A RBPM study in a rural low-income population reported significant decreases in both systolic and diastolic BP at 6-month follow-up. 14 These results align with our findings that RBPM is beneficial in achieving improved BP levels. Therefore, implementing the use of SIM-enabled, RBPM system can be helpful in achieving improved BP control for many patients.
Importance of working with housing communities
Housing and income levels are significant factors that may impact the development of health disparities. 42 Through our study, we were able to collaborate with the Ann Arbor Housing Commission and focus on a patient population that resided within a low-income housing community to better improve HTN outcomes for these patients. A study conducted by Digenis-Bury et al. found that individuals who resided in low-income housing in Boston reported having HTN two times more than individuals who were not from low-income housing areas. 43 This highlights the unique nature of our study, which focused on low-income participants, and the importance of conducting research with a patient population that is faced with health disparities because it allows us to identify and bridge any gaps that exist.
Incorporating SIM-enabled RBPM technology into the low-income patient care plan with the goal of improving health outcomes is feasible.
Cost, scalability and long-term sustainability of SIM-enabled RBPM
The cost of SIM-enabled RBPM system includes the initial cost of BP device, data transmission fees (SIM card/data plan), platform and personnel costs for monitoring and follow-up. The cost may appear high at the beginning for low-income populations. However, the SIM-enabled device already eliminated the cost of internet subscription. Insurance coverage and grant-funding programs can help offset these costs.44,45 Moreover, the reduction in clinic visits, emergency visits and hospitalization makes RBPM cost-effective in the long run. Systematic reviews on RBPM have reported cost-effectiveness of the intervention in HTN management.46,47 RBPM efficacy and cost-effectiveness in minority, underserved low-income populations have also been reported.14,48,49
The vast availability of cellular networks makes SIM-enabled RBPM system very accessible in underserved areas. The simplicity of the device makes it user-friendly for older adults. Older adults who may find the BP cuff challenging can benefit from training and caregiver support. Integrating the RBPM system with electronic health records and clinical workflow will reduce healthcare providers’ work burden and improve buy-in. 45 Long-term reimbursement of RBPM services is crucial for its’ sustainability. Having regulatory frameworks that support telehealth and remote monitoring are essential for long-term viability of RBPM. Sustained RBPM system use also requires ongoing patient engagement through education, technical support and perceived benefits. 44 Tailoring RBPM to individual patient's needs may increase effectiveness. 50
Implications for health policy
Given the benefits of the SIM-enabled RBPM, health policies should ensure its’ equitable accessibility and adoption by providing funding or subsidies for the devices, patient education, and support services. Integration of data from SIM-enabled BP monitors into the electronic health records for healthcare providers’ utilization should be encouraged to promote interoperability standards.
Study limitations
Our study is limited by the purposive small sample who were all non-Hispanic, mostly female and White, and have all attempted some college or higher education. Our study is also limited by the single center, non-randomized and older adults (≥ 62 years) sample used and lack of control group. However, our study is unique in that participants from low-income housing settings were able to utilize an electronic device to help record their BP and be a part of a process where they were monitored by a healthcare professional. They were provided relevant feedback through SMS-text capabilities, which was found to be a motivating element for some participants. This dynamic nature of achieving health-related goals and outcomes provides a holistic approach to the care process.
Future research directions
Our study was also a single-group pre-post comparison focused on implementation. Future research can focus on using this technology and similar methodology to investigate its benefits using stronger pragmatic designs including control group and in a larger low-income population with more diverse demographics. Exploration of feedback from patient's primary care physicians would be helpful in assessing intervention effectiveness from healthcare providers perspective. Further studies assessing long-term effectiveness and patient outcomes are essential to fully understand the benefits and challenges of using SIM-enabled BP monitoring system. Our study can serve as a baseline for the logistics on how to approach remote programs for other disease states.
Conclusion
SIM-enabled RBPM was feasible and acceptable amongst individuals with HTN living in low-income housing and could help in their HTN management. Expanding the use of such automated BP device that does not need WiFi to remotely send home measured BP readings to healthcare providers, combined with low-cost text messaging engagement can help improve individuals’ confidence in their care and may improve health disparities that exist among low-income population.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251347732 - Supplemental material for Facilitators and barriers of a subscriber identity module enabled, remote blood pressure monitoring system for residents of a low-income housing: A feasibility study
Supplemental material, sj-docx-1-dhj-10.1177_20552076251347732 for Facilitators and barriers of a subscriber identity module enabled, remote blood pressure monitoring system for residents of a low-income housing: A feasibility study by Chinwe E Eze, Hilary M Mansoor, Vincent D Marshall, Antoinette B Coe, Lorraine R Buis, Reema Kadri and Karen B Farris in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors acknowledge the use of CareSimple® devices and remote patient monitoring services. The authors have no financial relationship with CareSimple®.
ORCID iDs
Ethical considerations
The study was approved by the University of Michigan Institutional Review Board (IRBMED HUM00206203) on January 5, 2022.
Consent to participate
All participants provided signed written informed consent prior to participating.
Author contributions
Conceptualization: KBF, ABC, LRB and RK. Data curation: KBF, CEE, and VDM. Formal analysis: KBF, CEE, and VDM. Investigation: CEE and HMM. Project administration: KBF and CEE. Supervision: KBF. Writing original draft: CEE and HMM. Writing review and editing: CEE, HMM, VDM, ABC, LRB, RK, and KBF.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The study data is available upon request to the authors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.