
Abstract
Objective
The emergence of more contagious SARS-CoV-2 variants, such as EG.5 (Eris), has heightened the urgency of assessing associated risks and managing the spread of infections. Digital Contact Tracing (DCT) tools have been widely adopted to mitigate these risks, although the factors driving their acceptance are complex and multifaceted. However, there is a significant lack of research on the application of DCT within Saudi Arabia, despite its proactive use of such technologies in public health strategies. This study investigates the key determinants of DCT adoption and acceptance by integrating the Technology Acceptance Model (TAM) with psychological, social, and regulatory factors related to the context of the study.
Methods
Using a quantitative, cross-sectional design, data were collected from Saudi participants through an online survey and analysed using Structural Equation Modeling (SEM) with SmartPLS4.
Results
The results supported all the hypotheses except for the relationship between social media awareness and DCT tool usage. The findings revealed that COVID-19-induced anxiety significantly influenced technology acceptance, with social influence playing a mediating role. This study introduces a novel, context-specific model contributing to the technology acceptance field by exploring how pandemic-related factors, such as anxiety and social influence, affect DCT tool adoption. It also addresses a critical gap in the previous literature by examining the mediating role of social impact in the association between privacy and event-related fear and the moderating effect of COVID-19 anxiety on social media awareness and DCT usage. The findings offer valuable insights for governmental interventions, health institutions, and legislators in managing pandemics globally and within the Kingdom of Saudi Arabia.
Conclusion
We introduce a novel, context-specific model for understanding how pandemic-related psychological and social factors influence DCT adoption in this study. Those results provide insight into how policymakers, health institutions, and legislators can use DCT tools to manage pandemics globally and in Saudi Arabia.
Keywords
Introduction
The COVID-19 pandemic has profoundly impacted global society, economy, and politics, with over six million fatalities and infections surpassing half a billion worldwide. 1 The economic downturn in 2020 was significant, and ongoing recovery remains uncertain due to the emergence of new SARS-CoV-2 variants. Variants such as EG.5 (Eris) and FL 1.5.1 (Fornax) have exhibited increased transmissibility and potential immune evasion. 2 According to the Centers for Disease Control and Prevention (CDC), EG.5 accounted for over 20.6% of COVID-19 cases in the United States by September 2023, surpassing all other strains. 3 XBB strains also demonstrate the ability to evade immunity acquired from previous infections and vaccinations, 2 emphasizing the urgency of timely identification and mitigation strategies.
Traditional contact tracing (TCT) methods have struggled to contain rapidly spreading variants, necessitating the adoption of Digital Contact Tracing (DCT) tools. These tools enable real-time monitoring and exposure notifications, enhancing efforts to minimize viral spread.4,5 However, recent studies highlight key challenges in implementing TCT effectively, especially during high-transmission periods. Research has demonstrated that traditional contact tracing protocols had to be adapted due to resource constraints in urban settings, limiting their effectiveness in tracking and interrupting transmission chains in real-time. 6 Similarly, studies found that the emergence of COVID-19 variants of concern significantly reduced the efficiency of TCT efforts, particularly in jurisdictions with limited public health capacity. 7 Moreover, large-scale epidemiological modeling estimated that while case investigation and contact tracing prevented numerous infections and hospitalizations in the U.S., their impact diminished as case numbers surged beyond the threshold manageable by manual tracing teams. 8 These findings underscore the necessity of integrating DCT tools to complement traditional methods by enhancing speed, scalability, and accuracy in exposure notification and case identification 9 .High-density environments, such as annual Islamic pilgrimages (Hajj and Umrah) in Mecca and Medina, 10 further underscore the need for digital solutions, as millions of pilgrims congregate in confined spaces, heightening the risk of widespread transmission, where millions of pilgrims from different countries congregate in close proximity.
Despite the potential benefits of DCT tools, adoption remains hindered by challenges beyond technical implementation,11–14 issues such as limited user awareness, misinterpretation of data privacy laws, and public distrust have significantly hindered widespread adoption.15,16 Concerns over data security breaches and government surveillance have further contributed to hesitancy, exacerbated by the proliferation of misinformation on social media.5,15,17–21
Saudi Arabia has leveraged its high smartphone penetration rate and robust digital infrastructure to implement DCT solutions, 22 but adoption is still hindered. However, tackling the barriers riddling DCT accessibility cannot address other technology adoption challenges. The diffusion of innovation theory highlights a natural lag in the adoption of new technologies, 23 the urgency of pandemic response necessitates rapid scaling of DCT tools to enhance their effectiveness. 24
Knowledge gap
A deep dive into the Scopus database uncovers that the initial wave of academic literature on DCT surfaced in 2020. From that point onward, a total of 200 publications—including journal articles, reviews, conference proceedings, and book chapters—featuring DCT in their titles have been cataloged in Scopus, spanning up to February 25, 2025. This temporal distribution of research publications on DCT reflects the dynamic nature of scholarly interest in response to the COVID-19 pandemic. The provided Scopus data, illustrated in Figure 1, demonstrates a significant fluctuation in the volume of DCT-related research over the period from 2020 to 2024. In 2020, the number of publications related to DCT was relatively modest (24), likely due to the early phase of the pandemic when governments and public health authorities were initially grappling with containment strategies. During this period, traditional contact tracing methods remained the primary approach, despite their limitations in managing large-scale outbreaks. 6 As the pandemic intensified, the necessity for scalable digital solutions gained traction, leading to a marked surge in research publications in 2021, peaking at 60. This peak can be attributed to the widespread adoption of mobile-based exposure notification systems and growing investments in digital health technologies to mitigate transmission risks.4,5 Additionally, international collaborations and funding initiatives during this period accelerated the development and evaluation of DCT effectiveness.7,8 A slight decline in research output was observed in 2022 (55 publications), although the volume remained significantly higher than in 2020. This suggests continued scholarly engagement with DCT applications, particularly as new SARS-CoV-2 variants such as Omicron emerged, necessitating innovative approaches to public health surveillance.2,3 The decline became more pronounced in 2023 (31 publications) and remained stable in 2024 (30 publications). This trend may reflect the decreasing reliance on DCT tools as the pandemic transitioned into an endemic phase, coupled with persistent challenges related to user adoption, privacy concerns, and regulatory frameworks.11–14 Moreover, skepticism regarding data security and government surveillance further hindered the widespread implementation of DCT solutions, despite their potential in high-density environments such as religious gatherings and international travel hubs.10,15–17 Overall, the publication trends suggest that DCT research reached its peak in the immediate aftermath of the pandemic's initial outbreak before experiencing a gradual decline. While the urgency surrounding COVID-19 may have diminished, the insights gained from these studies remain relevant for future pandemic preparedness, particularly in refining digital epidemiological tools for real-time monitoring and intervention. Accordingly, several studies recommended focusing on integrating DCT into broader public health infrastructure, addressing privacy concerns, and enhancing public trust in digital health technologies to ensure their effectiveness beyond COVID-19.22–24 Therefore, this study examines the key factors influencing the adoption and acceptance of DCT.

Source (scopus database).
Practical gap
Despite Saudi Arabia's proactive integration of DCT technologies into public health policies during the COVID-19 pandemic, a significant gap exists in academic research on the country's experience with these tools. The absence of published studies on DCT in Saudi Arabia, as evidenced by Scopus data, highlights a critical need to understand the socio-technical, psychological, and regulatory factors influencing adoption. Globally, DCT-related research is concentrated in Western nations, with the United States (34 studies), the United Kingdom (24 studies), and Germany (20 studies) leading the field (See Figure 2). In the Arab world, only a few studies have been published, with Qatar (2 studies), Jordan (1 study), and Kuwait (1 study) contributing to the discourse (See Figure 3). However, Saudi Arabia—despite implementing widespread DCT measures, including smartphone-based immunity verification 5 —has no indexed publications on the subject. This absence limits the availability of empirical data to assess the effectiveness, challenges, and public perceptions of DCT in the Kingdom.

Source (scopus database).

Source (scopus database).
This gap is particularly significant due to Saudi Arabia's high smartphone penetration, advanced digital infrastructure, and centralized governance, which enabled large-scale DCT adoption. 5 Additionally, there is a lack of comprehensive studies examining the interplay of psychological, social, and regulatory factors in DCT adoption.5,24,25 Furthermore, despite the heightened transmission risks associated with mass gatherings such as Hajj and Umrah, how DCT was utilized in these contexts remains unexplored. Without academic investigation, critical questions persist regarding public trust, data privacy concerns, and long-term policy implications. Addressing this research gap is essential for developing evidence-based digital health policies tailored to Saudi Arabia's needs. This study seeks to fill this gap by examining the socio-technical, psychological, and regulatory factors influencing DCT adoption in the country.
Theoretical gap
Numerous theoretical frameworks and models have been developed to explore and understand the determinants of technology adoption, reducing uncertainties in this field. Notably, the Technology Acceptance Model (TAM) by Davis, 26 Task-Technology Fit (TTF) by Goodhue and Thompson, 27 and the Unified Theory of Acceptance and Use of Technology (UTAUT) by Venkatesh et al. 28 have been pivotal. The TAM, a well-known theory regarding the usage and adoption of information technology (IT), has been validated through numerous studies. Its evolution through various iterations has significantly advanced the understanding of the factors influencing technology adoption. Originally proposed by Davis et al. 26 the TAM focused on perceived usefulness and ease of use as direct predictors of technology usage intention. Later adaptations like the TAM3 by Venkatesh and Bala 29 incorporated social influence, acknowledging the role of societal norms and peer influences. The integrated TAM3 further included psychological factors such as anxiety, recognizing their impact on adoption behaviors. However, TAM overlooks other significant factors like regulatory aspects, which are crucial in the context of technology usage.
Among the 200 articles indexed in Scopus with “Digital Contact Tracing” in their title, only three have examined the relationship between DCT and the Technology Acceptance Model (TAM). This highlights the limited use of TAM as a theoretical framework in DCT research. A detailed analysis of these studies reveals that: Al-Okaily et al. 30 integrated Protection Motivation Theory (PMT) with TAM to analyze factors influencing the acceptance and use of contact tracing apps (CTAs) in Jordan during the pandemic. Dowthwaite et al. 31 extended TAM2 by incorporating trust as a key factor shaping the adoption of DCT apps in the United Kingdom. Krüger et al. 32 further refined TAM by integrating pandemic-related psychological factors, social influences, and demographic moderators, providing a broader perspective on digital health technology adoption. However, this study represents a major theoretical advancement in the field of DCT adoption research. By integrating TAM with psychological, social, and regulatory constructs, it surpasses prior studies in scope. The inclusion of social media awareness, event-related fear, and regulatory concerns makes this research especially relevant for real-world policymaking and pandemic preparedness strategies.
This study proposes a model that bridges these gaps by integrating technological, psychological, social, and regulatory factors. It introduces factors such as trust in government and event-related fear, emphasizing the influence of trust and specific emotional states on user behavior. It also addresses social media awareness and contemporary concerns about data privacy through the inclusion of privacy concerns. Furthermore, while theories and models of technology usage do not apply uniformly across all contexts,33,34 this research is the first application of such models in the context of Saudi Arabia in the field of DCT (see Table 1).
Theoretical Gap.

The proposed model's holistic approach significantly contributes to the literature by providing a comprehensive framework that addresses current challenges in DCT use. By integrating a broad range of factors previously overlooked, this model offers a nuanced understanding that can explain variations in acceptance and usage behaviors in complex settings like digital government. This approach is particularly relevant in contexts requiring high levels of trust and data privacy, offering insights into how these diverse factors collectively influence the acceptance and sustained use of DCT.
Research objective
The purpose of this study is to extend the discourse on technology acceptance by integrating crisis-specific behavioral factors and established acceptance models. It is based on the Technology Acceptance Model (TAM), which posits that perceived usefulness (PU) and perceived ease of use (PEOU) are key drivers of technology adoption. To better understand the unique challenges of Digital Contact Tracing (DCT) tools adoption during the COVID-19 pandemic, this study incorporates psychological, social, and regulatory factors into TAM. Among these are Trust in Government (TIG), which measures how users perceive the government's handling of public health and data security policies, Social Influence (SI), which measures peer behavior and recommendations, and Privacy Concerns (PP), which measures how concerned individuals are about their personal information privacy. Additionally, the study examines Event-Related Fear (ERF) as a psychological driver of adoption, Social Media Awareness (SMA) as an external factor influencing perceptions of DCT tools, and COVID-19 Anxiety (CA) as a moderating factor that intensifies technology adoption behaviors. Further, the study examines the mediating role of social influence between event-related fear and DCT adoption as well as the moderating effect of health anxiety on social media awareness. By integrating these novel dimensions and using Structural Equation Modeling (SEM) with SmartPLS4, this study provides deeper insights into the public's attitudes toward DCT tools and offers actionable recommendations for policymakers to overcome adoption barriers in pandemic scenarios.
Literature review and conceptual framework
Technology adoption in times of crisis and comparison with existing studies
While Digital Contact Tracing (DCT) tools have played a critical role in managing and mitigating the COVID-19 pandemic by tracking and controlling virus transmission,35–39 their adoption dynamics differ significantly in crisis versus non-crisis scenarios. Traditional technology acceptance models such as TAM and UTAUT have been widely applied to study adoption behaviors;28,40–42 however, most prior research has focused on everyday technology use rather than emergency-driven adoption.42–47 Government-led technology initiatives often face public resistance, even when resources and infrastructure are available.48–52 The urgency, fear, and uncertainty during a pandemic reshape public perception of government-introduced technologies, influencing adoption behaviors differently than in non-crisis settings.5,52–54
Despite extensive research on DCT adoption, most studies emphasize conventional technology acceptance factors, such as perceived usefulness and ease of use, while neglecting the broader psychological, social, and regional influences that impact adoption. Our study addresses these gaps by incorporating emotional, societal, and contextual dimensions into the analysis of DCT adoption.
Several studies have examined the adoption of DCT tools through established technology acceptance frameworks. For example, Walrave et al. 55 investigated the adoption of COVID-19 contact-tracing applications using an extended Unified Theory of Acceptance and Use of Technology (UTAUT) model. Their findings highlighted privacy concerns, trust in government, and perceived benefits as critical determinants of adoption. However, their study did not account for pandemic-induced psychological factors such as health anxiety and fear, which can significantly shape individuals’ willingness to engage with digital health technologies. Our research incorporates these psychological dimensions to better understand how emotional responses impact adoption behavior.
Furthermore, most studies on DCT adoption have been conducted in Western contexts, with limited research in Middle Eastern countries. European and U.S.-based studies primarily analyze DCT adoption through the lenses of data privacy concerns and trust in governmental authorities. 56 In contrast, Saudi Arabia presents a unique regulatory and cultural environment where government-mandated health applications, such as Tawakkalna and Tabaud, played a central role in managing public health.4,5,57 Unlike Western nations where DCT adoption was largely voluntary, Saudi Arabia's centralized digital health strategy created a different adoption dynamic. By examining DCT adoption within Saudi Arabia, our study addresses a critical gap in global public health informatics and offers insights applicable to similar regulatory environments.
Another important but underexplored factor in DCT adoption research is the role of social media awareness. While social media's influence on public perception has been extensively studied in health communication literature, few studies have examined its direct impact on DCT adoption. Social media platforms such as Twitter, Facebook, and WhatsApp have been shown to amplify both accurate health information and misinformation.58,59 Our study incorporates social media awareness as a predictor of DCT adoption and further examines how health anxiety moderates this relationship, providing novel insights into the impact of digital information exposure on technology adoption during a pandemic.
From a methodological standpoint, most studies on DCT adoption employ Structural Equation Modeling (SEM) to validate their theoretical models. For instance, Sharma et al. 60 conducted SEM-based analysis to assess the adoption of COVID-19 contact-tracing apps, focusing on perceived usefulness, privacy concerns, and trust in data security. However, existing studies primarily focus on technological constructs, often overlooking the interplay between social, psychological, and regulatory factors. Our study utilizes SmartPLS4 for SEM analysis, incorporating multiple mediators and moderators, such as social influence, trust in government, privacy concerns, and health anxiety. This comprehensive approach enhances the predictive power of our model and provides stronger empirical insights into real-world public health technology adoption.
The novelty of our research lies in its holistic approach that extends the Technology Acceptance Model (TAM) with psychological, social, and regional influences. Unlike prior studies that focus solely on technology-related factors, our research acknowledges that pandemic-induced emotions, cultural contexts, and social media exposure play a pivotal role in health technology adoption. By addressing these critical dimensions, our study advances the understanding of digital public health interventions and provides actionable recommendations for policymakers and health authorities seeking to enhance DCT adoption and public engagement during health crises.
Conceptual framework
Several studies have demonstrated the effectiveness of the Technology Acceptance Model (TAM) in explaining technology usage behaviour.4,5,61 TAM identifies two primary factors influencing individuals’ attitudes toward technology adoption: perceived usefulness and ease of use. Perceived usefulness refers to the belief that a specific technology will enhance performance, and perceived ease of use refers to the belief that it will be simple and easy to use. 40 Furthermore, research suggests that perceived ease of use affects perceived usefulness indirectly, ultimately influencing users’ attitudes toward technology adoption.
Despite extensive validation across several domains,62–64 including health information systems, much existing research focuses on healthcare professionals, leaving a gap in understanding how consumers adopt health-related applications.65–67 Consumers are often more reluctant to adopt health technologies than professionals because they lack self-efficacy. As a result, the general public may adopt new health apps at a lower rate than professionals.45,65,68 Health apps must, therefore, be promoted to foster consumer acceptance and broader adoption.
Despite its effectiveness in predicting internal motivation, TAM has limitations when accounting for external factors affecting technology adoption. As a result, the current study extends TAM by incorporating social influence, anxiety about health, governmental trust, privacy concerns, and awareness of social media. These external factors are especially pertinent in the context of the COVID-19 pandemic, where attitudes toward DCT tools are shaped not only by the perceived usability of the technology but also by broader societal and emotional influences.
This extended framework integrates these external variables and offers a more holistic view of technology acceptance. Following this section, the theoretical model is discussed in more detail, outlining the relationships between the variables and hypotheses being evaluated.
Theoretical model and hypotheses construction
Perceived usefulness (PU)
This variable represents an individual's level of trust in accepting and using a specific technology based on its contribution to enhancing performance.26,69 Related studies have examined the impacts of perceived usefulness on the intention to use mHealth and DCT tools; to begin with Zhang et al.
70
found a positive association between the variable and using mHealth, while Binyamin and Zafar
71
found PU to have a significant influence over intention towards mHealth app use. Furthermore, previous studies4,5 have also established a strong association between PU and the DCT tool's intention to use. As a result, this study posited the following hypothesis:
Hypothesis 1 (H1): Perceived Usefulness significantly impacts the DCT tool's intention to utilize.
Perceived ease of use (PEOU)
Davis
26
defined Perceived Ease of Use (PEOU) as the belief of an individual that a particular technology will be effortless and easy to use. According to this study, PEOU is a user's perception that it is easy to use DCT tools from mental and physical perspectives. A significant association has been found between PEOU and intention to use in previous research. For example, Binyamin and Zafar
71
found that PEOU was significantly correlated with PU in the context of mHealth use. Other studies have also found that PEOU affected the intention to use mHealth apps in other studies.72,73 Furthermore, PEOU was shown to influence PU and intention to use DCT tools significantly.4,5 Thus, the following hypotheses are posited:
Hypothesis 2 (H2): Perceived Ease of Use will positively impact Perceived Usefulness. Hypothesis 3 (H3): Perceived Ease of Use will positively impact the intention to utilise DCT tools.
Intention to use DCT (DCT iu)
One of the best predictors of a person's inclination to accept innovation is their intention to embrace them. Behavioural intention is an individual's inclination or willingness to perform a particular behaviour.
74
Concerning the overall adoption of mHealth and detection apps, intention towards system use represents an individual's plan to utilise such technology. Binyamin and Zafar
71
discovered a significant correlation between the intention to use a mHealth app and its actual utilisation, which is like the finding that Alsyouf et al.4,5 reported in that intention towards use was found to affect actual DCT tools use significantly. Considering this, this study posited the following hypothesis:
Hypothesis 4 (H4): The DCT tool's intention to use significantly influences its use.
Trust in government (TIG)
According to trust literature, the element of trust reduces the uncertainties and risks in different situations,5,75,76 and the variable is commonly described as the psychological state that consists of intention towards accepting vulnerability according to the expectations of the positive intentions/behaviour of another. 77 Nevertheless, trust may also be modified and manipulated when it comes to the actual use of an app by increasing or decreasing such use based on a user's experiences. 78 Individual trust in the government also plays a role in minimising uncertainties, as most of the COVID-19 apps are government-developed. In effect, government trust can minimise the fear of using such apps. 79 Government trust is considered solid and robust in the short term.80,81
More specifically, people's trust in the government is the perception of the former of the latter's integrity and ability to provide service.5,76 Citizens trust the government's DCT tool's effectiveness and adoption differently; thus, there is a higher likelihood that those who trust the government will perceive that the government will use tool-gathered data responsibly. Also, they have a higher likelihood that the government can effectively use the tools to confine the COVID-19 pandemic and that the tools will benefit rather than harm. In the case of France, higher citizens’ trust in the government was found to be related to higher incidences of acceptability and use of contact tracing apps, 82 which a UK study also supported. 83
In the U.S. context, research has been conducted on the inclination to adopt warning apps through hypothetical situations. The results of these studies indicate that individuals carefully assess the benefits and risks associated with these technologies. 84 According to the findings, the benefits include being informed about potential risks, a sense of altruism by protecting others, and ensuring personal safety. On the other hand, the risks primarily focus on privacy concerns and the costs associated with using mobile data. A similar study in the U.S. also highlighted the importance of accuracy and privacy issues when considering adopting tracking apps. 85 Additionally, an international study found that privacy concerns were a significant factor affecting the willingness of participants to download an app, with 37% refusing to do so if sufficient data protection measures were not in place. 86 Similar findings were observed in studies conducted in Australia 87 and the UK 83 Based on these existing studies, this study posited the following hypothesis:
Hypothesis 5 (H5): Trust in government will positively impact the intention to use DCT tools.
Social media awareness (SMA)
Monitoring the pandemic on social media has the power to shape health behaviours through social media influencers. However, monitoring can also increase public fear, pushing them to embrace preventive measures. 88 Multiple studies have shown that mass media usage can benefit individuals’ health behaviours. 89 Moreover, it has been observed that these changes tend to avoid any adverse effects. 89 The observations and concomitant changes are reflected in the frequency of listening to the radio and reading newspaper reports and the corresponding minimised occurrences of contracting diseases because of the high inclination towards vaccinations. 90 They may also be evident through the TV usage frequency, which was found to be positively correlated with water-, sanitation- and hygiene-related behaviours. 91 Additionally, Facebook and Twitter, which are prominent social media platforms, present innovative approaches to prevent pandemics. The implication is that social media facilitates reciprocal communication between health organisations and the general public, demonstrating its effectiveness in preventing hazardous sexual behaviours, 92 enhancing attitudes and understanding regarding skin cancer, 93 promoting the adoption of maternal influenza vaccines, 94 and validating lifestyle modifications.
Likewise, Lim et al. 95 found the possibility of driving people towards adopting, supporting, disseminating, and sharing innovations or behaviour's using socially mediated social media. In this regard, social media can connect social norms with the society's capability to access health information, news, and behavioural patterns related to health. This connection occurs through the impact of social media on individuals and their observations of others. 96 Essentially, the extent to which people use social media to obtain health information and manage diseases can greatly impact their health behaviour outcomes.
Furthermore, Alhuwail and Ab-dulsalam's
97
study showed that individuals prioritise using platforms like YouTube over Twitter, Snapchat, and Facebook when seeking health-related information. Similarly, Stawarz et al.'s
98
research highlighted the effective utilisation of mobile technologies in addressing mental health issues. Building upon these previous works, it becomes imperative to investigate the correlation between social media awareness and the adoption of Digital Contact Tracing (DCT) tools to curb the transmission of COVID-19. Therefore, based on the studies mentioned above, this study posited the following hypothesis:
Hypothesis 6 (H6): Social media awarness significantly impacts DCT tool utilisation.
Social influence (si), event-related fear (ERF) and perceived privacy (pp)
Due to the inability of individuals to personally test COVID-19 DCT tools or communicate with the developers, they resort to other methods of acquiring information, such as seeking input from peers who have already adopted the app. The more individuals perceive that their peers are supportive and convinced of the efficacy of the COVID-19 digital contact tracing app, the more likely they are to adopt and use it themselves. This process is known as social influence, where individuals gauge the opinions of those close to them to reduce uncertainties surrounding contact tracing apps.
28
This study proposes that understanding individuals’ social surroundings preferences can measure their views about using the app. Thus, this study posited the following hypothesis:
Hypothesis 7 (H7): Social Influance significantly impacts the use of DCT tools.
Event-Related fear
This type of fear refers to people's judgment concerning event danger, which is based on the people's feelings at a specific period rather than the actual probability of the severity.
4
In this regard, fear as an emotional state significantly correlates with risks that could result in emergencies.
99
Based on the Zika and H1N1 outbreaks several years back, studies showed that event-related fear contributes to public health emergencies, and thus, those having high fear levels are likely to be more worried about COVID-19. As a result, they may obtain information concerning the virus and how they can be protected from it. People whose peers use DCT may be more likely to be convinced of their effectiveness in preventing the virus's spread and use the tools themselves. Social influence can, therefore, prevent negative event-related fear effects on DCT use. High levels of event-related fear could lead to high adoption and use of DCT, particularly if peers are also using such tools. Thus, this study posited the following hypothesis:
Hypothesis 8 (H8): Social Influance will mediate the association between event-related fear and DCT use.
Privacy
In addition to the above, DCT users are often concerned about privacy issues, and this is true for human rights entities who are forever questioning governments who develop apps to be adopted by societal members. 5 Privacy perception is the intensity to which the users believe that their personal information is protected and secured.4,5 Privacy is a complex concept that many factors affect, with past studies on privacy violations indicating that these include an organisation's data collection trustworthiness and perceived advantages of sharing information.
Moreover, individuals concerned about their privacy will not be inclined to use DCT tools as they think their personal information can be accessed and shared without their permission and consent. Nevertheless, if peers use DCT tools, individuals may adopt them as they respect their peers’ knowledge concerning the risks and benefits of such use. They may be convinced that their peers make informed decisions when using the tools.
Social influence can mitigate perceived privacy concerns surrounding DCT tool use because, upon observing their peers’ use of DCT tools, individuals highly concerned with privacy are more likely to use them. Hence, this study posited the following hypothesis:
Hypothesis 9 (H9): Social Influance will mediate the relationship between perceived privacy and DCT tools use.
The moderating role of health anxiety sensitivity on COVID-19 (ca)
During the ongoing pandemic, individuals across the globe have been grappling with a persistent sense of health anxiety. This overwhelming fear can permeate every aspect of their lives, leading them to adopt avoidance strategies, suffer from heightened stress levels, and grapple with intrusive negative thoughts that seem to haunt them relentlessly. Alarming as it may be, the impact of health anxiety extends even further, manifesting in a range of negative and ineffective preventative behaviours and actions. In support of this, several prior studies100–103 have shed light on the correlation between these psychological effects and individuals’ tendency to engage in counterproductive measures to protect themselves and others during the crisis.
Gaygisiz et al.'s 100 study found that numerous factors contributed to health-related anxiety among individuals. With this understanding, it becomes crucial to delve deeper into these perceptions to develop effective health applications during the ongoing COVID-19 pandemic. It is no secret that this global health crisis has unleashed a wave of fear, leaving many people feeling vulnerable to death, sickness, and helplessness. A prominent issue has also emerged concerning the stigma associated with the virus. An in-depth study of this phenomenon can provide insight into individuals’ mental health status during this challenging period. Moreover, it can help us better understand the specific needs and support that individuals require so we can provide them with an opportunity to mitigate the adverse effects of health-related anxiety associated with the pandemic. 104
Furthermore, anxiety has a significant correlation with risks and may result in emergencies, 99 and in the past, Zika and H1N1 outbreaks have provided evidence that anxiety contributes to public health emergencies.
Some individuals have experienced heightened anxiety due to the COVID-19 pandemic. Several factors contribute to this anxiety, including the fear of contracting the virus and the uncertainty surrounding the situation. Although anxiety can be detrimental in some ways, it can also be beneficial in others. It encourages individuals to become aware of the protective measures that can be taken to avoid spreading the infection. As part of this heightened awareness, individuals will become more familiar with and understand the various available DCT (Disease Control and Prevention) tools. People have become more aware of the importance of implementing preventive measures as they attempt to protect themselves and their loved ones from COVID-19. Consequently, the combination of increased anxiety and heightened awareness regarding DCT tools creates a more substantial commitment to practising protective measures and preventing the contraction and spread of the virus.
This commitment would lead to a stronger link between social media awareness and DCT tools use among those with high anxiety rather than those with low ones. People who are highly anxious about COVID-19 are more likely to be convinced of the effectiveness of DCT tools in preventing the spread of the pandemic and the higher benefits vs. risks of the tools. Thus, this study hypothesises that;
Hypothesis 10 (H10): COVID-19 anxiety will moderate the association between social media awareness and DCT tools use.
Research methodology
Study context
Saudi Arabia responded to the COVID-19 pandemic by creating two apps, Tabaud and Tawakkalna,4,5,57 to help control its spread. It utilises the Apple/Google exposure notification API and offers three main services to users. It sends notifications to individuals in close contact with someone infected with Covid-19. The Saudi government launched the Tawakkalna application to prevent the spread of Covid-19. The Saudi Data and Artificial Intelligence Authority (SDAIA) developed the app to manage relief efforts electronically and establish control for governments and private sector workers. The aim was to limit the spread of the pandemic within the country. During the “return with caution” period, new services were introduced in the Tawakkalna app, which helped achieve a safe return while maintaining the user's privacy and security through coloured codes.
Design, sampling, and data collection procedures
This research utilises quantitative cross-sectional designs to assess and validate the research framework. Due to governmental-forced lockdown actions and mandatory community separation, data collection was impossible. The authors distributed an online survey questionnaire during the lockdown period. The survey was created using a web-based Google form and translated into Arabic through back translation, as recommended by Brislin.105,106 The survey used a five-point scale ranging from 1 representing strongly disagree to 5 representing strongly agree, to gauge these study items. Five academics reviewed and gave feedback on the survey. The measurement scales used in the survey were adapted from related articles, and the items can be found in section “Theoretical model and hypotheses construction”.
The research investigated smartphone users in the Kingdom, considering that DCT was made compulsory nationwide. Due to challenges in acquiring a comprehensive record of smartphones user's, the survey was instead shared on various social media. The study examined public perceptions of Covid-19, particularly attitudes towards contact tracing. Data were collected over two months, from December 2021 to January 2022. Participants were obtained through Saudi COVID-19-related groups, local community groups, and university communities consisting of faculty members, employees, and students. Their involvement in the study was voluntary and without any financial incentives.
Regarding exclusion criteria, none were used considering demographic data, except for the ages of the participants (at least 18 years). This study sample size selection was based on Krejci and Morgan's 107 method and formula, whereby 384 samples were considered acceptable in this study. Four hundred surveys were retrieved, all of which were complete and devoid of missing data.
Measures
The initial version of the questionnaire was translated into Arabic using a different process, considering it is the respondents’ native tongue. The contents were created using proven methods found in the literature. A score of 1 indicated strong disagreement, while a score of 5 represented strong agreement. The adopted items were taken from relevant and related works; COVID-19 Anxiety and Event-Related Fear comprise 9 and 3 items, respectively, adopted from.4,5 Moreover, Trust in Government comprised 4 items adopted from. 5 PU and PEOU comprise 4 items, each adopted from.4,5,70,71 Social Influence, Digital Contact Tracing Tool Intention to Use, and Digital Contact Tracing Tool Usage consisted of 3 items for each, adopted from.4,5,41 Perceived Privacy comprised 6 items, and social media awareness comprised 5 items adopted from. 5
Data analysis techniques
The study employed descriptive statistics, moderation, and mediation regression analysis. SPSS generated descriptive statistics. SmartPLS4 was used for hypotheses testing, and its bootstrapping method was used for estimating path coefficients and standard errors. 108 Based on its robustness through bootstrapping, SmartPLS4 was selected for the analysis of complex models with multiple moderating and mediating variables examined in the current work. Also, the contingent influence of COVID-19 anxiety and the mediating effect of social influence were analysed using a 5000 bootstrapping sample, with a 95% confidence interval (CI) at 0.05 significant level. Before conducting Smart PLS4 analysis, SPSS Version 23 was used to obtain descriptive results.
Results
Demographic characteristics
The demographic information of the respondents via SPSS indicated that most were male (210, 52.5%), 18–34 years of age (196, 49%), and held bachelor's degrees (216, 54%). The results also showed that most respondents hailed from the Western Saudi province (236, 59%). Table 2 tabulates the demographic characteristics of the respondents in terms of age, gender, educational level, and residence location.
Demographic characteristics of the respondents.

Validity and reliability
The study used SmartPLS4 to measure the outer model and establish the validity and reliability of the obtained data. More specifically, convergent validity was established using Cronbach's alpha (α), composite reliability (CR), and Average Variance Extracted (AVE), with the values obtained considered acceptable,109,110 at more than 0.70, 0.70 and 0.50, respectively. Individual study variables obtained the following Cronbach's alpha, CA, and AVE, respectively: COVID-19 anxiety was 0.714, 0.821, and 0.537, event-related fear was 0.909, 0.939 and 0.837, DCT tool intention to use variable obtained 0.917, 0.948, and 0.858, perceived ease of use was 0.854, 0.901, and 0.695, while perceived privacy was 0.914, 0.933, and 0.699. Moreover, for the other variables, Cronbach's alpha (CA), CR and AVE values were as follows: perceived usefulness was 0.929, 0.950, and 0.826, respectively; social influence was 0.909, 0.943, and 0.846 respectively; social media awareness was 0.819, 0.868 and 0.570, respectively, while trust in government was 0.857, 0.913 and 0.778, respectively. See Table 3.
Internal constructs consistency.

Fornell and Larcker (1981) were used to evaluate the measurement model and data validity109,110 (refer to Tables 4 and 5).
Fornell-Larcker criterion.
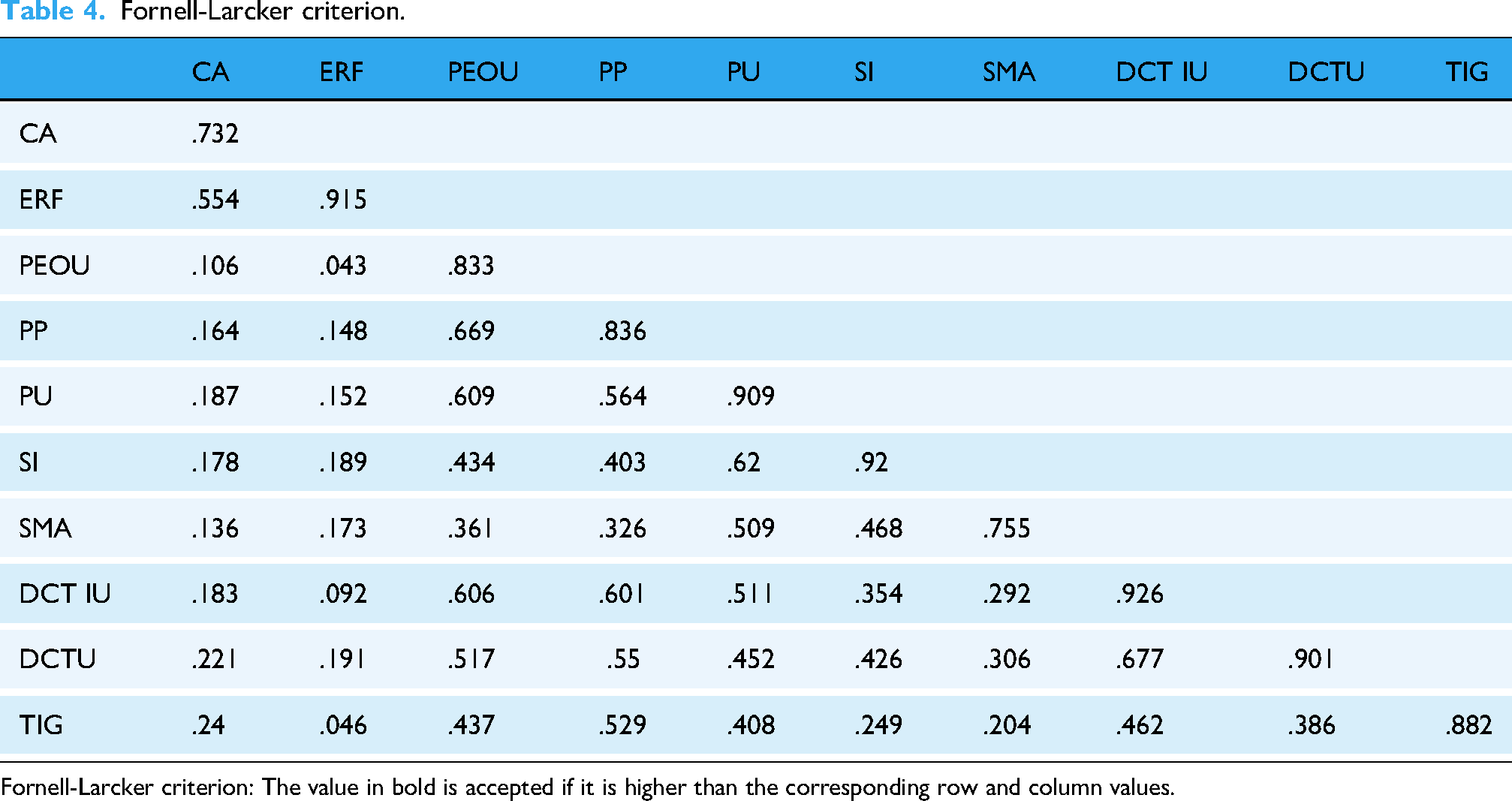
Fornell-Larcker criterion: The value in bold is accepted if it is higher than the corresponding row and column values.
Discriminant validity (HTMT ratio).

HTMT Ratio < .85 is valid.
For discriminant validity confirmation, the items’ cross-loadings can also be used.111,112 For acceptable cross-loadings, the items’ loadings must be higher on their corresponding constructs than on other constructs (refer to Appendix A).
Coefficient of determination (R2)
Based on the PLS4 output coefficient of determination values (R2) of DCT tools use was 0.513, that of DCT tools intention to use was 0.435, perceived usefulness was 0.370, and that of social influence was 0.179. The results showed that in combination, CA, DCTIU, PU, ERF, PP, PEOU, SMA, SI, and TIG explained 0.513 of the variance in DCT tool use among Saudi citizens. Additionally, perceived ease of use was found to explain 0.370 of the perceived usefulness of the tools; perceived privacy and event-related fear explained 0.179 of social influence on DCT tools use. In this regard, a higher R2 value means a higher predictive ability of the structural model, and in this study, R2 was substantial based on Cohen. 113
Study hypotheses testing
The models (main effect, moderating, and mediating) were all examined to examine the structural model and test the formulated hypotheses. The path coefficients were generated using the PLS path algorithm to evaluate the significance of the different model effects. Following past studies, the structural model was exposed to a bootstrapping procedure with 5000 re-samples.109,111,114 Last, the path coefficients were employed to test the direct, moderating, and mediating effects (See Table 6 and Figure 4).

SEM figure.
Summary of direct effect, moderating effect, and mediating effect.

Table 6 tabulated results supported hypothesis 1, which posited a significant and positive association between the DCT tool's intention to be used by citizens and perceived usefulness (β = 0.177, t = 2.694, p < 0.01).
In addition, a significant and positive relationship was found between perceived ease of use and perceived usefulness of DCT tools, supporting H2 (β = 0.609, t = 14.883, p < 0.01), and a positive and significant relationship was found between PEOU and DCT tools intention use, supporting H3 (β = .406, t = 5.797, p < .01).
Moving on to the proposed relationship between the DCT tool intention to use and actual use, the results supported the association (β = 0.584, t = 13.235, p < 0.01), supporting H4. H5 was also supported because the results showed that trust in government had a positive relationship with DCT tools use (β = 0.213, t = 3.973, p < 0.01). However, H6 was rejected as the association between SMA and DCT tools use was insignificant (β = 0.035, t = 0.803). As for social influence, the results supported its positive and significant relationship with DCT tools use (β = 0.191, t = 4.175, p < 0.01), supporting H7.
Following the results of the above direct relationships, the mediating relationships proposed in H8 and H9 were tested. Social influence mediated the association between event-related fear and perceived privacy with DCT tools use (see Table 5). This test involved bootstrapping analysis on event-related fear and its indirect effect on using DCT tools through social influence — supporting mediating effect (β = 0.025, t = 2.153, p < 0.05). Similarly, perceived privacy indirectly affected DCT tools through social influence (β = 0.073, t = 3.667, p < 0.01). These results supported the mediating effect of social influence on the association between event-related fear and perceived privacy, with DCT tools usage (H8 and H9).
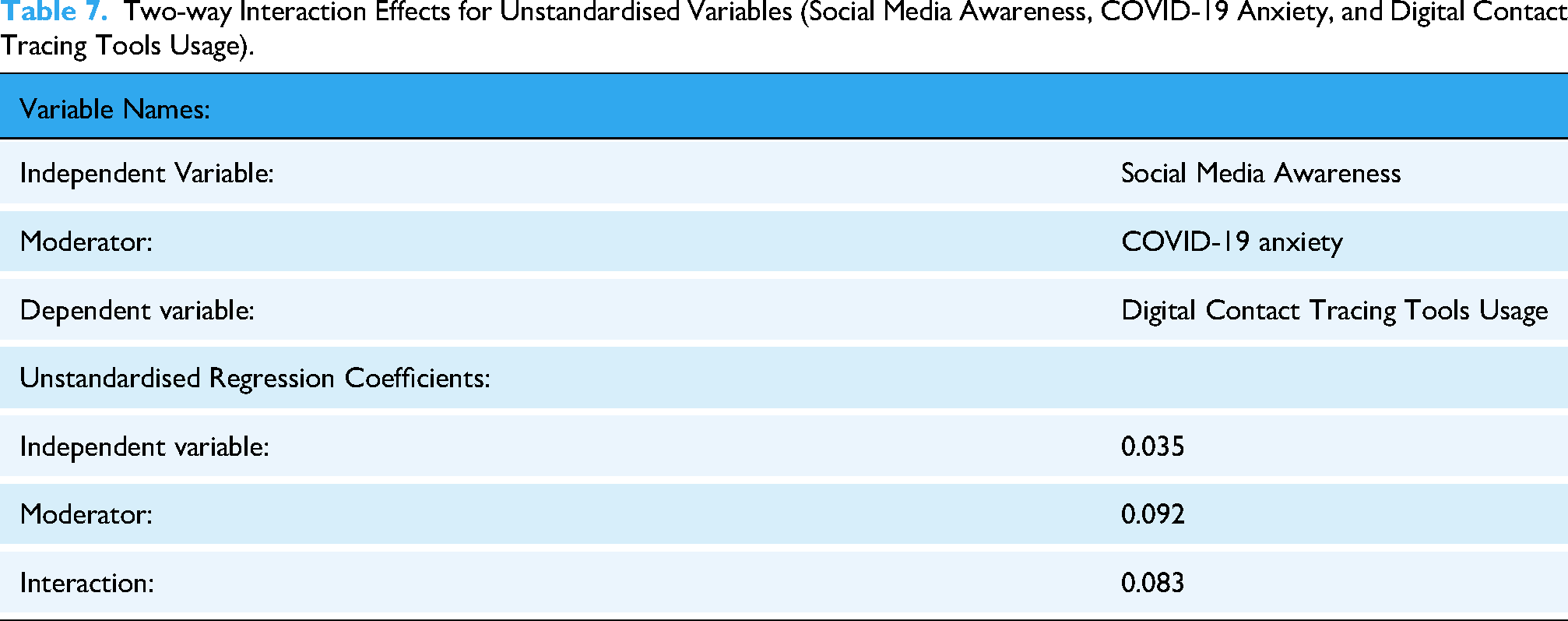
Regarding other indirect effects, a positive moderation path coefficient was found (β = 0.083, t = 2.139, p < 0.05) for the moderating effect of COVID-19 anxiety on the association between social media awareness and DCT tools use, indicating that anxiety from COVID-19 had a positive contingent influence on the association between social media awareness and DCT tools usage (H10). In other words, the association between social media awareness and DCT tools use was moderated and strengthened by the anxiety brought on by COVID-19 (see Figure 5 and Table 7). Moreover, Table 6 shows the two-way interaction effects for unstandardised variables for social media awareness, COVID-19 anxiety, and digital contact tracing tools usage.

COVID-19 anxiety strengthens the positive association between Social Media Awareness and Digital Contact Tracing Tools Usage.
Two-way Interaction Effects for Unstandardised Variables (Social Media Awareness, COVID-19 Anxiety, and Digital Contact Tracing Tools Usage).
Discussion
The study findings validated TAM's ability to predict DCT tools use among Saudi citizens in response to the evolving COVID-19 pandemic by showing support for its assumptions and the included additional variables, further contributing to the model's predictive abilities. Based on the findings, the model successfully explained 0.513 of the use of DCT tools, 0.435 of DCT tools intention to use, 0.370 of perceived usefulness, and 0.179 of social influence. Also, the study found the R2 value substantial based on Cohen's 113 R2 classification.
Touching upon individual direct results, perceived usefulness prediction of DCT tools usage intention (β = .177, t = 2.694, p < .01) was supported for H1. Past relevant studies on mHealth found perceived usefulness to be a top predictor of behavioural intention toward mHealth types of usage.45,70,71,115 This result means that if citizens believe that DCT tools are effective in safeguarding them from the COVID virus, they desire to be more likely to use them.
In the second hypothesis (H2), perceived usefulness was proposed to have a significant and positive influence on perceived ease of use, and the correlation was supported (β = 0.609, t = 14.883, p < 0.01). Studies concerning this relationship in literature illustrated that perceived ease of use in utilising DCT tools may convince people of its usefulness.4,5,71–73 Thus, the likelihood of finding DCT tools useful lies in their easy-to-use features.
The third hypothesis of this study proposed a significant relationship between perceived ease of use and DCT tool intention to use (β = .406, t = 5.797, p < .01). Like past studies, the current research indicated that PEOU among users concerning DCT tools could result in the intention to use and eventually actual use of such tools.4,5,71,116,117 The importance that the citizens place on the perceived ease of use of DCT tools may explain this result. Prior studies in the acceptance of health informatics applications among citizens revealed the differences between their acceptance and that of professionals65,68 and that consumers do not have the same high SE level and hold adverse perceptions of a technologies usability, making them more likely to face challenges in the usage of an application. It is thus essential to provide the proper assistance to citizens when convincing them to accept apps.
The fourth hypothesis proposed a positive association between intention towards using DCT tools and actual use. The findings supported this relationship (β = 0.584, t = 13.235, p < 0.01), like past studies.4,5,118,119 This finding shows that the behavioural intention to use the users reflects their acknowledgment and usage of innovations. Stated differently, the individual's intent towards adopting DCT tools is a predictor of their actual usage and adoption of the similar, as supported by the current and past studies in the literature.
Trust in government and intention towards using DCT tools was also positively significant (β = .213, t = 3.973, p < .01), supporting H5. This result supports prior reported results that indicated trust in government among the citizens plays a role in their positive perceptions, attitudes, and behaviours toward DCT tools, enhancing their actual use.82,83,120 This result may be explained by the fact that people trusting governments are convinced that the latter will responsibly use the tools based on their purpose and objectives. They will perceive the government to be responsible enough when using their personal information, only using it for their own good. This belief in the government's development and implementation of effective public health measures contributes further to government trust. It enhances their belief that they can reap benefits from using government-made tools. The government ensures privacy and provides benefits like preventing the spread of the pandemic while outweighing the risks of tool usage. Consequently, trust in the government influences the usage and adoption intention of DCT tools and, eventually, actual usage among the citizens.
Regardless of the positive effect of social media awareness on DCT tools use among Saudi citizens, the effect was insignificant (β = 0.035, t = 0.803), rejecting H6. DCT tool usage was made mandatory among the public in Saudi Arabia. Social media messages were used to disseminate information, but such messages may not have affected the use of the app itself. The Kingdom adopted a paternalistic response to the pandemic emergency to promote the importance of the whole over the individual. 121 The public health policies that the Kingdom developed are directed towards protecting the population's health as opposed to protecting individual rights and interests, making DCT tools mandatory for everyone's usage. This led to social media awareness not impacting the public's use of the DCT tools.
Additionally, the effect of social influence over the use of DCT tools was assessed in H7, and a significant correlation was found (β = 0.191, t = 4.175, p < 0.01). In past studies, the impact of social influence on the use of DCT tools was significant.122,123 Thus, there is a likelihood that social network members have a higher likelihood to use DCT tools if their important others are also using them. In other words, the use of DCT tools among individuals is promoted by the use among their important others or peers because individuals need to be validated for their responsibility and inclination towards taking protective measures to ensure that they and their loved ones remain protected.
The results show that indirect effects of social influence significantly mediated the association between event-related fear and DCT tools use (β = .025, t = 2.153, p < .05). Thus, H8 was supported. This result makes a new contribution to literature. The current study found that social influence directly affected the use of DCT tools and mediated the relationship between such use and event-related fear. No past practical results have been reported on the mediating effect of SI on the two variables. This result may be attributed to the likelihood that individuals who fear contracting COVID-19 are influenced by the opinions and behaviours of their loved ones and those who are dear to them. Therefore, they are more open to seeking information and support from the latter. Peers highly influence their use of DCT tools. Event-related fear may also be minimised through social influence using DCT tools. Their peers may persuade those who fear contracting COVID-19 to use DCT tools for information, which will minimise such fear. Moreover, people whose fear of contracting COVID-19 is higher have more reason to use the DCT tools for information and statistics to protect themselves and others, and this is supported by the use of their peers of such tools.
Similarly, H9 of this study proposed that social influence would mediate the relationship between perceived privacy and DCT tools (β = 0.025, t = 2.153, p < 0.05). This hypothesis was supported based on the results, marking another new contribution to the literature. The positive, direct, and significant results supported the mediating influence of perceived privacy on DCT tools use and social influence. The direct effect of social influence over DCT tool usage was also validated, but prior empirical findings did not document the mediating effect. The result of this study may be explained by the likelihood that people concerned about their privacy may be influenced by the opinions and behaviours of their peers regarding how privacy is dealt with when using DCT tools. In other words, peers and loved ones are more likely to urge individuals to use DCT tools by ensuring privacy measures are in place.
Additionally, social influence may minimise perceived privacy concerns regarding DCT tool usage. Privacy-concerned individuals will be more inclined towards using such tools if their peers convince them that it is beneficial to use them. Social influence can be directed towards promoting DCT tools by mitigating privacy concerns among privacy-conscious individuals. Steps can be taken to ensure that privacy is established among users through the words of trusted peers and loved ones who use such tools, thus further promoting and spreading their use.
Last, the tenth hypothesis (H10) proposed that COVID-19 anxiety would moderate the relationship between social media awareness and DCT tools use. The positive moderating role of anxiety from COVID-19 was supported (β = .083, t = 2.139, p < .05), marking another novel contribution to literature. Such a result may have stemmed from the fact that SM usage increased during the epidemic, with more and more people engaging and interacting with others online, thus increasing information-sharing.124,125 Unfortunately, social media also have a key role in disseminating misinformation and sensationalism surrounding COVID-19, resulting in heightened anxiety and directing the focus elsewhere. 126 Anxiety about COVID-19 played a significant influence in increasing awareness of DCT tools. Individuals experiencing high levels of anxiety were more likely to seek out information on how to protect themselves, leading to greater awareness and adoption of DCT tools. Social media amplified this heightened anxiety, where both accurate and misleading information spread rapidly. As a result, anxious individuals were more likely to adopt protective measures for themselves and their loved ones, influenced by the information they encountered online.
Practical implications
The study results have several important practical implications for government agencies, health policymakers, and healthcare institutions. First, they highlight the critical role of Digital Contact Tracing (DCT) tools in managing COVID-19 risks, especially in high-density environments such as religious gatherings or public events. Even after quarantine measures have been lifted, health authorities can increase public trust and usage by understanding the factors influencing the adoption and use of DCT tools.
Further, the findings on trust regarding government and privacy concerns suggest that improving transparency and safeguarding data privacy are essential to improving DCT adoption. Governments should build public trust through clear communication and robust data protection policies to ensure widespread adoption.
Finally, the study emphasises the role of social influence and anxiety in shaping individuals’ behaviour toward using DCT tools. As part of long-term pandemic management strategies, health campaigns that leverage social media platforms and emphasise collective action can further encourage using these tools. The insights gained from these studies can be applied to future health crises, providing a framework for implementing effective technology-driven interventions.
Limitations and future studies recommendations
This study has some limitations, despite its contributions. As a first point, the study is based on Saudi Arabia, which adopted DCT as a requirement. To assess the generalizability of findings, future research should examine voluntary adoption contexts in other regions. The role of government credibility in technology adoption can be further elucidated by studies that compare countries with different levels of public trust.80,81 A second aspect of the study is that it captures adoption behaviour at a particular time. As the pandemic evolves, a longitudinal study could examine trust, anxiety, and social influences. During crises, public trust in government policies can fluctuate, and tracking these shifts could shed more light. 102
Moreover, while this study focuses on Saudi Arabia, the implications of DCT adoption extend beyond the country. Public gatherings, such as religious events, sports tournaments, and cultural festivals, pose similar risks to public health. In previous research on the Hajj pilgrimage 10 and the Olympics, 127 the importance of digital health technologies has been emphasized. In future studies, it would be useful to assess the effectiveness of DCTs in cultural and regulatory contexts across the globe. Additionally, differences in privacy concerns and trust in government between countries with different political systems 83 suggest that comparative research may provide valuable insights into tailoring public health interventions based on governance structures and cultural expectations.
The third factor that should be explored in future research is cultural differences, political ideologies, and digital literacy, which may also affect adoption behaviours. Using models such as Delone and McLean's IS Success Model could be useful in understanding user satisfaction and the continued use of health technologies.128,129 As a final point, qualitative methods such as in-depth interviews or focus groups could provide a richer understanding of individual perceptions and barriers to DCT adoption. 130 To capture both statistical relationships and personal experiences, future studies could use mixed-method approaches.
Conclusion
This study examined factors influencing the adoption of the digital contact tracing (DCT) tool during the COVID-19 pandemic in this study. This study extended the technology acceptance model (TAM) to incorporate external factors such as SI, TIG, anxiety, privacy concerns, and social media awareness. According to the findings, perceived usefulness, perceived ease of use, and trust in government significantly influence users’ intentions to adopt DCT tools, which predicts actual usage. In addition, the study provides novel insights into the role social influence plays in mediating the relationship between event-related fear and privacy concerns. Additionally, anxiety induced by COVID-19 strengthens the association between social media awareness and the usage of DCTs.
These findings show that trust in government and social influence are critical factors in encouraging health-related technology adoption. By addressing privacy concerns and fostering trust, governments can make DCT tools more widely available to manage future pandemics and other large-scale health threats. In addition, the study emphasizes the value of recognizing emotional and societal factors that affect technology approval.
The study validates the relevance of TAM in the context of health technologies and offers an extended framework to account for the unique challenges of a global pandemic. The insights gained from these studies can help health institutions and policymakers design, communicate, and implement technology-based solutions to manage public health.
Supplemental Material
sj-docx-3-dhj-10.1177_20552076251336271 - Supplemental material for Predicting digital contact tracing tool adoption during COVID-19 from the perspective of TAM: The role of trust, fear, privacy, anxiety, and social media
Supplemental material, sj-docx-3-dhj-10.1177_20552076251336271 for Predicting digital contact tracing tool adoption during COVID-19 from the perspective of TAM: The role of trust, fear, privacy, anxiety, and social media by Adi Alsyouf, Ala’a M Al-Momani, Nizar Alsubahi, Abdalwali Lutfi, Khalid Anwer Al-Mugheed, Mohammed Amin Almaiah, Rami J Anshasi, Main Naser Alolayyan, Abdallah Alsaad and Mahmaod Alrawad in DIGITAL HEALTH
Supplemental Material
sj-xlsx-6-dhj-10.1177_20552076251336271 - Supplemental material for Predicting digital contact tracing tool adoption during COVID-19 from the perspective of TAM: The role of trust, fear, privacy, anxiety, and social media
Supplemental material, sj-xlsx-6-dhj-10.1177_20552076251336271 for Predicting digital contact tracing tool adoption during COVID-19 from the perspective of TAM: The role of trust, fear, privacy, anxiety, and social media by Adi Alsyouf, Ala’a M Al-Momani, Nizar Alsubahi, Abdalwali Lutfi, Khalid Anwer Al-Mugheed, Mohammed Amin Almaiah, Rami J Anshasi, Main Naser Alolayyan, Abdallah Alsaad and Mahmaod Alrawad in DIGITAL HEALTH
Footnotes
ORCID iDs
Ethical considerations
Ethical approval for this study was obtained from the Institutional Review Board (IRB) of King Abdulaziz University, College of Business, under reference number COB/2021/12. In addition, all participants were assured that their participation was voluntary, and written informed consent was obtained from all participants prior to their participation. All methods were carried out in accordance with relevant guidelines and regulations, specifically the Declaration of Helsinki. Respondents were assured that their responses would remain anonymous and confidential, and they were not required to disclose their names. All collected information was securely stored on a password-protected personal computer to ensure data security.
Author contributions/CRediT
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Deanship of Scientific Research (DSR) at King Abdulaziz University, Jeddah, under grant no. GPIP: 1083-849-2024. Therefore, the authors acknowledge DSR’s technical and financial support with thanks.
Conflict Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.