
Abstract
Introduction
Although artificial intelligence (AI) can boost clinical decision-making, personalize patient treatment, and advance the global health sectors, there are unique implementation challenges and considerations in developing countries. The perceptions, attitudes, and behavioral factors among the users are limitedly identified in Ethiopia.
Objective
This study aimed to explore AI in healthcare from the perspectives of health professionals in a resource-limited setting.
Methods
We employed a cross-sectional descriptive study including 404 health professionals. Data were collected using a self-structured questionnaire. A simple random sampling technique was applied. We used SPSS to analyze data. Tables and graphs were used to present the findings.
Results
A 95.7% response rate was reported. The mean age of the respondents was 32.57 ± 5.34 SD. Almost 254 (62.9%) of the participants were Bachelors of Science degree holders. Nearly 156 (38.6%) of the participants were medical doctors. More than 50% (52.2%) of them said AI would be applicable for diagnosis and treatment purposes in healthcare organizations. This study identified that a favorable attitude, good knowledge, and formal training regarding AI technologies would foster clinical decision-making practices more efficiently and accurately. Similarly, our study also identified the potential barriers to AI technologies in healthcare such as ethical issues, privacy and security of patient data were some to mention.
Conclusions
Our study revealed that positive attitude, good knowledge, and formal training are crucial to advance healthcare using AI technologies. In addition, this study identified self-reported AI concerns of the participants such as; privacy and security of data, ethical issues, and accuracy of AI systems. Attention could be given to overcome the barriers of AI systems in the health system. Providing training, allocating time to practice AI tools, incorporating AI courses in the curricula of medical education, and improving knowledge can further the usage of AI systems in healthcare settings.
Introduction
By definition, artificial intelligence (AI) is the advancement of computer systems and software that can do activities that normally require human intelligence, such as visual perception, speech recognition, decision-making, and language translation. AI-based clinical diagnostic interventions have helped healthcare professionals to diagnose, and make clinical decisions accurately, enabling the basics for disease predictions, and determining the different courses of action for chronic and non-chronic disease management. 1 AI is a science that develops algorithms to do activities associated with human intelligence, such as learning and problem-solving. The word was first used in 1955 and its founder was. 2 Similarly, scholars define AI as the ability of machines to perform tasks that would normally require human intelligence, such as sensing, reasoning, learning, and decision-making.3,4
AI applications in healthcare sectors have evolved in many ways. Physicians use AI-based tools to diagnose, treat, and follow up patients. 5 AI can improve healthcare service management by providing real-time and updated information obtained from clinical journals, textbooks, and clinical best practices. Recently researched studies,6–9 witnessed the clinical importance of AI in classifying skin lesions using a convolutional neural network algorithm and the final output was comparable with the level of competencies of dermatologists. 10 Due to its widespread application, AI has been used for the delivery of clinical education, clinical management, and patient care.11,12 Research findings stated that newly developed AI technologies can identify signs and symptoms of certain diseases faster and more accurately than human beings. 7 Certain technological devices can perform functions that generally need human interpretation and decision-making. A study in Germany 3 about AI-supported diagnostics for detecting depression revealed that traditional diagnostic procedures are useful, but might be limited in access and subject to bias, thus leading to underdiagnoses. Thus, the research examines the potential of AI technology, specifically machine learning, to diagnose depression.3,13
AI has extensive applications in a variety of fields of study, including finance, transportation, and manufacturing. In healthcare, AI can be utilized for medical imaging analysis, tailored treatment, and a variety of other applications.11,14 Due to the advancement of AI in the global health sectors, recently available huge data surges are one AI component that demands to be studied as if the perceptions, attitudes, and behavioral factors among the users are limitedly identified.11,15 Such limitations might bring compromise in the decision-making processes of the health system. The fact behind such advanced data use and AI ability is worth managing large voluminous data with greater automation. 15
Similarly, the rapid growth of AI has had a substantial impact on healthcare. 16 Healthcare systems may become smarter, faster, and more efficient in providing treatment to millions of people around the world by incorporating AI into hospital settings and clinics. AI in healthcare is truly the future reality, and revolutionizing how patients receive high-quality treatment while lowering provider costs and improving health outcomes.16–18
AI systems can increase healthcare personnel's knowledge and decision-making abilities, potentially leading to better patient outcomes and more efficient healthcare delivery.8,19 Dealing with health professionals’ knowledge, perspectives, and attitudes toward AI might be significant for the implementation and adoption of AI-based health systems at every corner of the health sector. As the adoption of AI varies from country to country, assessments in developing countries revealed low levels of awareness, attitude, and understanding regarding its utilization in healthcare organizations by health professionals. 20 Lack of exposure, training, and access to information on the abilities and potential applications of AI in the healthcare environment might cause this low-level range.1,19 With the same outlines, health professionals might hesitate about issues related to the accountability and liability of AI-based decisions in healthcare settings. Pragmatically, AI models revealed high accuracy for tasks from patient admission to discharge in healthcare settings in developed regions. 21 One opportunity that AI can provide for healthcare professionals is to determine accurately, using deep learning algorithms, which were first coined by Enrich, picture archiving and communications, which detect signs of different diseases using medical image modalities such as magnetic resonance imaging, computed tomography, ultrasound, and X-rays.22–24
Even though data security and privacy have become potential uncertainties that health professionals are cognizant of the utilization of AI in their health service delivery, assuring the accuracy, reliability, security, and clinical usage of medical AI systems, standards, and regulations must be established.22,25,26 Several factors can affect the utilization of AI by healthcare professionals in developing countries like Ethiopia. Such factors might be mentioned as a lack of fully installed infrastructure and readiness for technologies (factors such as accessibility of high internet bandwidth, availability of hardware and software capable of running AI applications), human capital, and digital literacy (very skewed level of digital and AI-related skills, lack of capacity of building programs to upskill the health professional), relevance and applicability of AI solutions to healthcare (alignment of AI-based tools and solutions with the specific healthcare needs are challenging), lack of knowledge sharing and collaboration (absence of cross-boundary knowledge-sharing practices), and customization and localization of AI systems to fit the local context are some to mention.
Similarly, there are study findings that support the poor knowledge and attitude of health professionals in utilizing AI tools in developing countries like Ethiopia. A prototype study in Hossaena, Ethiopia revealed that an AI-based chatbot system was employed to delve into an end-user chatbot by which personal virtual doctors can assist patients in accessing their health information needs. However, users’ interaction with the system was hampered due to low-speed internet, computer skill problems, and other behavioral factors. 9
Additionally, integrating AI in healthcare settings necessitates a thorough review to determine the benefits, obstacles, and ethical implications. The implementation of AI requires health professionals’ commitment and positive attitude to advance AI systems in their day-to-day activities. This study might be the first of its kind to elicit such impeding factors that may hinder the knowledge attitude and perceptions of health professionals toward AI in Ethiopian healthcare. The results of this study tried to reveal the magnitude of these factors and discovered the potential benefits of AI in healthcare. The final results of our study will be used as a benchmark for the next researchers to uncover other potential heterogeneities and design future implications by highlighting the existing facts of AI. Policymakers will be also advantageous to further the potential advantages of AI in the health system. Therefore, the main objective of this study was to assess AI in healthcare from the perspectives of health professionals and identify the potential barriers observed among these health professionals.
Methods
Study design and settings
Study design and period
A cross-sectional descriptive study was conducted from May 1 to June 1, 2024 among health professionals in selected health facilities of South Wollo zone, Dessie, Ethiopia.
Reasons for choosing cross-sectional design
A cross-sectional study design is a type of observational study that analyzes data from a population or a representative subset at a specific point in time. It is commonly used in fields such as public health, social sciences, and market research to investigate the prevalence of outcomes, associations between variables, or patterns within a population. Cross-sectional studies take a “snapshot” of a population at a specific point in time. This is useful for understanding the current status of a phenomenon, such as the prevalence of an illness, attitudes, or behaviors. In our case, regarding the magnitude of exploring AI among healthcare professionals, we used cross-sectional studies rather than longitudinal studies (which track participants over time); cross-sectional studies are often less expensive and quicker to undertake. Data is collected only once, avoiding the need for long-term follow-up. This helped us to bring our findings descriptively. 27 However, there are limitations to using a cross-sectional study design. A key limitation of a cross-sectional study during the current study regarding AI in healthcare is its inability to establish causality, which means it cannot definitively determine whether the observed relationship between AI usage and healthcare outcomes is due to AI or other confounding factors because data is collected at a single point in time, preventing analysis of changes over time.
Study setting
According to the information for the 2007 Census conducted by the Central Statistical Agency of Ethiopia, the South Wollo zone has a complete population of 2,518,862, with an increase rate of 18.60% over the 1994 census, of which 1,248,698 are men and 1,270,164 are women. It covers an area of 17,067.45 square kilometers. The population density for the zone is 147.58. While 301,638 (11.98%) are urban inhabitants, 2,217,224 (88.02%) inhabitants were reported to be rural dwellers. There are 14 public hospitals in the South Wollo zone with a total of 1123 healthcare workers to serve the catchment population of the South Wollo zone and the nearby zones, especially for the Afar region. The source population for this study was all health professionals working in public hospitals in the South Wollo zone.
Sample size determination and statistical analysis
The sample size was calculated using a single proportion formula (50%) as there were no previously conducted research findings, a study, and a 95% confidence interval with a 5% margin of error. The ultimate sample size was 422, with a 10% non-response rate. South Wollo zone, Amhara region, is home to 14 public hospitals. This study includes all permanent health professionals who worked at each hospital during the study period; proportional allocation was done for each hospital based on the actual number. The proportionate number of research subjects was calculated using the formula x = xf/X*xi, where xi is the number of health professionals in each hospital, xf is the overall sample size, and X is the total number of health professionals working in South Wollo zone public hospitals as reported by the zone office. Each health practitioner at each selected hospital was selected by applying a simple random sampling method from the list of records found in the administration office. Several pretested survey tools6,12,28–30 were used to create a structured self-administered questionnaire. We pretested the developed questionnaire at Kombolcha Comprehensive Hospital. The reliability of the items was checked using Cronbach alpha value 0.92 to use the tool for our final data collection. While Cronbach's alpha is used for measuring the internal consistency of the items used to measure, there are other reliability measures such as factor analysis, test–retest reliability, and other measures. In our study, we employed and measured Cronbach’s alpha and the items were generally consistently measured the items used in the study. Data were entered manually using Epi Data Version 3.1 and exported to SPSS version 20 for analysis. We used descriptive statistics. Tables and graphs were used to present the results of the findings.
Results
Sociodemographic characteristics of the study participants
In total, 404 health professionals sent the response from the selected health facilities with a response rate of 95.7%.
The mean age of the respondents was 32.57 ± 5.34 SD. The majority (226/55.9%) of the participants were males.
Regarding the educational status of the participants, almost 254 (62.9%) of them were Bachelor of Science degree holders. Nearly 156 (38.6%) of the participants were medical doctors followed by 125 (30.9%) nurse professionals. Nearly half, 194 (48.0%), of the participants had less than 5 years of work experience (Table 1).
Knowledge of artificial intelligence among health professionals in South Wollo zone, 2024.

aOthers: psychiatry, pharmacy.
Health professionals knowledge of AI
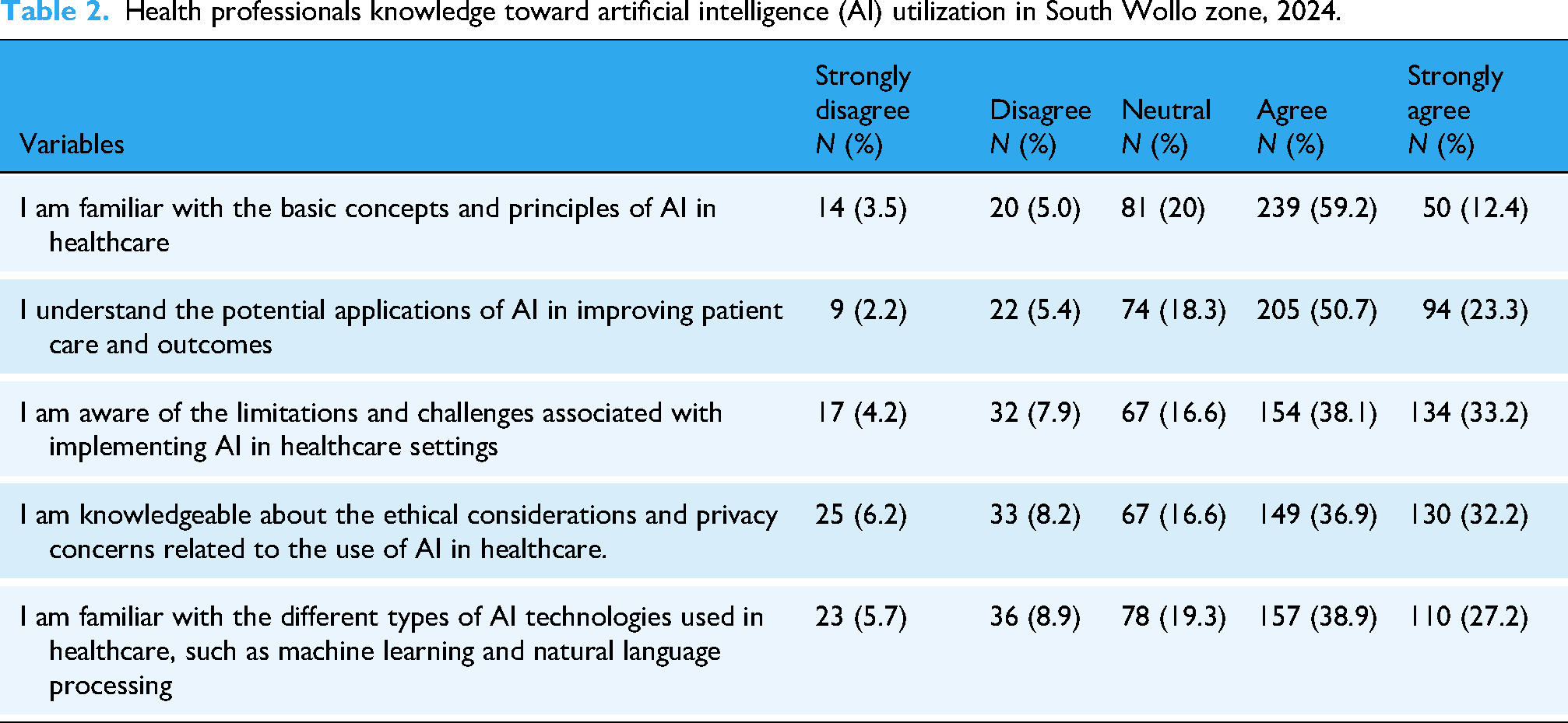
We assessed the knowledge of health professionals about AI using five closed-end Likert scale questions. The questions were ranging from “Strongly Disagree = 1,” “Disagree = 2,” “Neutral = 3,” “Agree = 4,” and “Strongly Agree = 5.” The total knowledge score was added up by considering the median value, which was 20 (interquartile range (IQR) = ±4). More than half 230 (59.2%) of the participants involved in this study agreed as they were familiar with the basic principles of AI applicable in healthcare. Participants were also asked to present their self-reported knowledge of AI, and almost half 205 (50.5%) of them agreed that they understood the potential applications of AI in improving patient care and outcomes. Most 157 (38.9) of the health professionals were able to agree on their familiarity with the different types of AI technologies used in healthcare, such as machine learning and natural language processing (Table 2).
Health professionals knowledge toward artificial intelligence (AI) utilization in South Wollo zone, 2024.
Health professionals’ attitude toward AI
Regarding the health professionals’ attitude toward AI, we employed 12 Likert scale questions ranging from “Strongly Disagree = 1,” “Disagree = 2,” “Neutral = 3,” “Agree = 4,” and “Strongly Agree = 5.” The data was not normally distributed and we computed the median as a measure of the distribution of the attitude responses of the participants. Hence, the median value was found to be 44 (IQR = ±8). Of the total study participants, the majority 197 (47.5%) of them agreed that AI has the potential to significantly improve diagnostic accuracy and patient outcomes in healthcare. The study participants were confident in their ability to adapt to and efficiently use AI systems in their clinical practice. Almost 43.6% of them were adaptive to the use of AI in their clinical expertise. Almost 189 (46.8%) of the total participants agreed and perceived that AI as a tool can assist healthcare professionals rather than replace them. Similarly, participants were shown their positive attitude in integrating AI systems into healthcare systems would have the paramount advantage to enhance patient care. Nearly 47% of them agreed with this idea too (Table 3).
Health professionals attitude toward artificial intelligence (AI) utilization in South Wollo zone, 2024.

Similarly, health professionals were asked to put their opinion about the most promising applications of AI in healthcare. More than 50% (52.2%) of them were said AI would be applicable for diagnosis and treatment purpose in the healthcare organizations. Exactly half (50%) of the participants declared their opinion about the healthcare application areas of AI would be used for monitoring patients and provide appropriate care. Nearly 36.6% of the participants stated that AI is also a promising tool for drug development in healthcare organizations (Figure 1).

Opinions about the promising applications of artificial intelligence (AI) among health professionals in South Wollo zone, 2024.
As if AI had many important promising applications in healthcare, the participants further described their concerns while using AI technology in healthcare settings. Approximately 47% of health professionals were worried that the usage of AI would result in disclosing the patient's privacy and data security. As a matter of fact, AI would also have an impact on health professional's liability and accountability issues. Thereby, those health professionals may be apprehensive about the privacy and security implications of sharing patient data with AI systems, particularly if the patient data are accessed by unauthorized users. In addition, from the perspective of healthcare professionals (nearly 40% of the health professionals depicted), the accuracy and reliability of AI systems used in healthcare is a major area of concern (Figure 2).
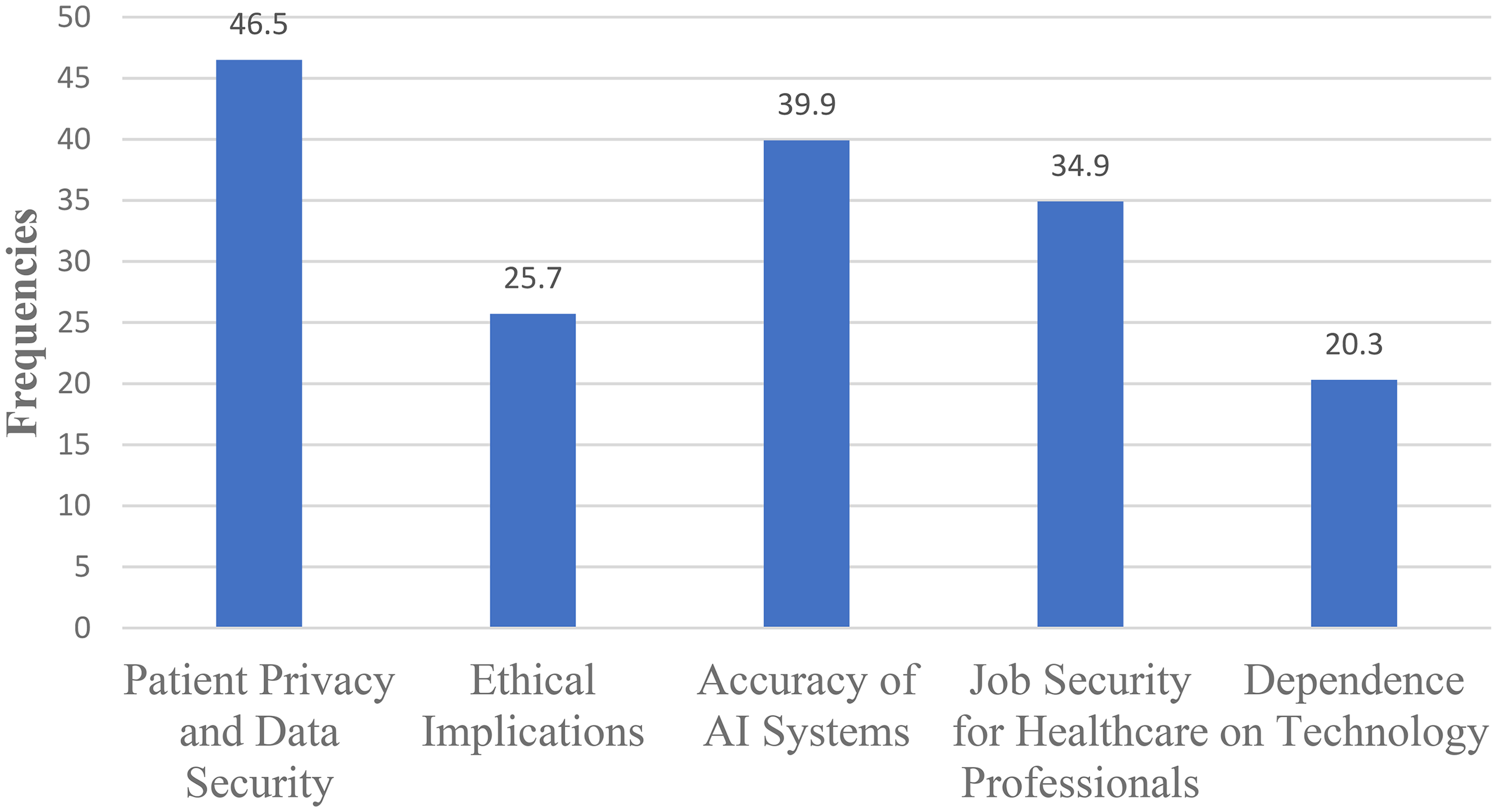
Primary concerns regarding the use of applications of artificial intelligence (AI) among health professionals in South Wollo zone, 2024.
Organizational factors mentioned as an impeding issue to the use of AI in healthcare
Health professionals were asked to mention the possible organizational factors hindering the applicability of AI in their working healthcare environment. As a result, 142 (35.1%) of the health professionals involved in this study took formal training on AI concepts and applications. However, the majority of them, nearly two-thirds (64.9%) of them did not take formal AI-related training. Similarly, a small (35.9%) number of the participants had participated in workshops, and courses related to AI in healthcare. Regarding the possible AI information sources, the participants were able to access information from scientific journals, and online platforms such as Google, PubMed database, Artificial Intelligence in Medicine, etc. Accordingly, 140 (34.7%) of them had access to these AI information sources. Additionally, one-third (32.7%) of the participants got support from their organization to learn AI as an innovative tool applicable to healthcare. Time as a constraint factor to use AI in healthcare, also plays a role as an organizational factor. Thus, more than one-third (34.4%) of the study participants mentioned that they had sufficient time to dedicate to learning and staying updated on AI in healthcare (Table 4).
Organizational factors affecting the applicability of artificial intelligence (AI) among health professionals in South Wollo zone, 2024.

In our current study, 52.2% of male study participants had shown having favorable attitude toward AI utilization in healthcare. While 43.8% of female study participants reported that they had good knowledge of AI in healthcare (Table 5).
Linkage between sex, knowledge, and attitude of health professionals toward artificial intelligence in South Wollo zone, 2024.

Discussion
Even though this study is the first as to the knowledge of the author, it tries to uncover the current status of AI and its applicability concerning the perspectives of the study participants in the Ethiopian context. This study aimed to explore how AI impacted the healthcare system with the view of the first-line healthcare providers and describes the potential or powerful nature of AI to improve patient care, diagnosis, medical treatment, and patient monitoring systems in the healthcare delivery system. AI allows for the creation of individualized treatment strategies by assessing genetic and clinical data. Policymakers can push for policies that encourage research and implementation of personalized medicine, hence improving patient outcomes. AI-powered telemedicine systems can improve access to healthcare, notably in Ethiopia. Policymakers should advocate for regulations that enable the deployment of telehealth technologies, enabling fair access to medical treatments. Therefore, leveraging formal training on how to use AI for decision-making by individuals is a mandatory task for health policymakers to adopt a reliable AI system. 31
Health professionals were favored to utilize AI in their working environment. We found that almost 198 (49.0%) of the participants in this study had shown a favorable attitude toward AI and the result of our study is consistent with a study done in Turkey 12 and the Philippines. 32 The possible reason might be having a positive attitude toward AI in healthcare is so important to significantly enhance healthcare delivery, leading to improved patient outcomes. Another possible explanation might be AI can help healthcare providers make better-informed decisions and provide more effective patient care. On the other hand, the result of this study was smaller than the evidence found in Croatian universities. 29 Similarly, the qualitative result of a study 33 witnessed the health professionals’ favorable attitude toward AI which is consistent with our current study. The possible justification could be that health professionals such as nurses, physicians, and others are welcoming the AI technology as it transforms individual treatment/therapy and patient care and it improves and streamlines quality health service delivery. However, factors such as digital literacy, infrastructure, and exposure to AI can significantly influence how healthcare professionals and patients perceive and interact with AI technologies. Digitally proficient or literate health professionals would embraced AI than those who are not literate. 34 Considering such factors would be beneficial while adopting AI technologies in healthcare.
Integrating poor nations’ AI experiences into global AI efforts is crucial for guaranteeing inclusive, equitable, and long-term advances in AI. While wealthier nations frequently lead in AI research, innovation, and deployment, poorer countries provide distinct views, difficulties, and possibilities that can considerably improve global AI endeavors. 35
Our study revealed that 49% of the participants had positive/favorable attitudes toward AI whereas the study in the mentioned universities indicated a high percentage (64.5%) of the participants had positive attitudes toward AI in healthcare. The difference could be due to the fact of sampling bias. The sample size used in Croatian universities was 336 with an average positive attitude of 64.5%, while our study sample was a larger sample resulting smaller favorable attitude. That means, the method used to select the smaller sample may have introduced a bias, leading to the overestimation of the individuals with a particular attitude.
Similarly, our study explored the health professional's knowledge of AI and figured out that nearly 43% of the samples reported having good knowledge of the current AI systems in healthcare. The result of our study is in line with the research findings of Central Catalonia Health Region 30 and University of Toronto. 17 The reason for this consistency might be due to health professionals’ good knowledge of AI in healthcare would empower the successful integration and effective implementation and use of AI in healthcare settings. Thus, health professionals’ good knowledge of AI is essential for the development of AI models that can accurately interpret medical data and able to make clinical decisions by providing meaningful insights. 16 AI as a new technology has been incorporated into many health sectors to date. Health professional's familiarity with these branches of AI would strengthen and significantly reshape healthcare by enhancing medical diagnosis and treatment. 18 In relation to this, our study revealed that nearly 157 (38.9%) of the health professionals are agreed and familiar with the different types of AI systems used in healthcare, such as machine learning and natural language processing (Table 2). Similarly, a health professional's deep insight into AI would provide highlights about the ethical implications of AI in healthcare such as issues related to patient privacy, data security, and the potential for bias or discrimination. Approximately 47% of the health professionals in this study were worried that the usage of AI would result in disclosing the patient's privacy and data security (Figure 2). As a result, health professionals’ involvement would ensure to the development of AI-based solutions and enable them to deploy the system in a manner that prioritizes patient welfare and lining up to ethical guidelines.26,36–38
Our study provokes action to the widespread deployment and use of AI technologies in health organizations in which physicians, nurses, public health experts, and other health professionals could be assisted by these modern technological tools. In this study, we examined the potential application areas of AI systems in healthcare, and the majority of the study participants reported that AI can be applied for diagnosis and treatment plans, drug development, patient monitoring, and care, and facilitating the management of medical records (Figure 1). The result is supported by the reports indicated.3,18
In addition, our study identified the potential areas of concern such as patient privacy and data security, ethical implications, accuracy of AI systems, job security for health professionals, and dependency on such technology. 6
Indeed, ethical concerns are the major barriers to implementing AI systems. Particularly, ethical concerns about AI in healthcare, those related to privacy and data security, are critical to be addressed since they significantly impact the acceptability and use of AI technology. AI must be trustworthy, and for users to trust the AI technology, it has to be transparent. To develop a responsible AI, which is a set of principles that help in guiding the design, development, deployment, and use of AI-building trust in AI solutions having the potential to empower the end users. Responsible AI aligns AI technologies with stakeholder values, legal standards, and ethical principles. Building a responsible AI would foster the trust of AI utilization in healthcare. 39 Similarly, policymakers have to play a critical role in developing frameworks that protect patient rights while fostering innovation, ensuring that AI systems contribute positively to the healthcare landscape without compromising ethical standards. This can be addressed by anonymizing individual data, building transparency and accountability, maintaining data breach protocols to mitigate the damage, and increasing stakeholder engagement to develop a comprehensive regulation beginning from the design stage of AI systems. Adopting a regulatory framework to address the ethical concerns regarding AI utilization in healthcare is mandatory. 38 Similarly, healthcare professionals are concerned that the increasing integration of AI into healthcare would result in the displacement of human medical professionals by AI technologies as a study indicated in Bangladesh. 40
In our study regarding privacy and data security majority (46.5%) of participants felt frustrated (Table 2). The finding was absolutely maintained by, 18 who stated that data privacy is especially critical because AI systems collect vast amounts of personal health information, which might be misused if not managed properly. Furthermore, suitable security measures must be implemented to prevent sensitive patient data from being used for malevolent purposes. 36 Similarly, the participants raised issues regarding the accuracy of AI systems and most (39.9%) of them explained their fear on the top. Even though participants of this study are concerned about the accuracy of the AI systems, there are preliminary studies that suggest AI-based technologies are getting more accurate given that more frequent training to bring the most preferred quality results from a given data set.19,41 This concern can also be lessened by merging numerous classifier outputs into a single classification framework that can help achieve improved accuracy and perform automated big data analysis. 42
Although our study was the first of its kind in the Ethiopian context, and explored the AI paradigm from the healthcare providers’ perspective, we mapped and compared it with other countries’ experiences accordingly. Implementing AI in healthcare needs investment in local capacity building, culturally sensitive AI design, and ongoing stakeholder engagement as compared to a study revealed in low- and middle-income countries. 43
Despite the importance of AI in healthcare and gaining attention in medical research, real-world implementation remains challenging. Therefore, in the current study, the study participants mentioned their self-reported challenging issues while they practiced AI in their working area. The challenges are mainly sourced from the level of the organization, such as lack of formal training, lack of workshops or seminars, lack of courses related to AI in the curriculum, lack of access to online resources, and lack of support from supervisors. In our study, a small number (35.1%) of participants reported that they got training related to AI applicable to healthcare. The findings of the current study are consistent with study results in, 12 which states that a small number of the study participants received training about AI. Similarly, the findings of the study stipulated that a lack of medical education curricula related to AI would hamper healthcare settings.
Moreover, this study explored the essence of motivations to use AI systems from supervisors and allocating more time to engage and use AI tools to support better patient care and improve clinically best decisions. Allocating more time to use AI tools would significantly improve diagnosis and early detection of disease by analyzing medical images, lab results, and other patient data more rapidly and accurately.44,45 This can bring fast interventions, improve patient outcomes, and lessen the health costs 46 to be allocated. The result of our findings is in line with research done in China, 47 which supposes the impact of glaucoma screening with AI automated diagnosis from a budgetary standpoint by using a Markov model.
Limitations and strengths of the study
Our study tried to map the current experience of health professionals regarding AI and the healthcare system will adopt the AI system as an integrated tool to diagnose, treat, and support both the healthcare providers and the patient. Despite describing the status of AI utilization among healthcare professionals, this study could not assess healthcare professionals’ AI tools and utilization using advanced models. It simply tried to describe the healthcare professionals’ current level of understanding about AI, without establishing causal relationships which made it difficult to determine whether AI interventions directly lead to improved health outcomes. In addition, the current study might have been exposed to a social desirability bias due to the nature of self-reported data. Participants might provide answers they believe are more socially acceptable rather than their true feelings or knowledge. That is the knowledge and attitude responses might have been affected due to their desire and belief. Despite the limitation, we employed data collectors outside of the study participants’ working area to minimize the social desirability bias at a maximum effort.
Conclusions and recommendations
We applied a cross-sectional descriptive method to highlight AI in a healthcare setting from the perspective of health professionals in Ethiopia. Our study depicted that a positive attitude, good knowledge, and formal training are the points of attention being crucial for the advancement of healthcare using AI technologies. In addition, this study revealed self-reported AI concerns such as privacy and security of patient data, ethical issues, and accuracy of the AI system. Similarly, attention should be targeted to overcome the potential barriers of AI system utilization in the health system. Identifying the factors that hampered the utilization of AI systems in healthcare would enhance the health admins to tackle and find solutions to these barriers. Providing training, allocating more time to practice AI tools, incorporating AI courses in the curricula of medical subjects, and improving knowledge would further the usage of the AI system in healthcare. In addition to recommending AI training and curriculum inclusion in the perspective of utilizing AI in healthcare, actionable steps have to be taken by the policymakers to collaborate with AI developers, build and structure AI training modules, and advance AI-assisted decision-making protocols to step up the health sectors. We also urge that future researchers analyze the utilization of AI in healthcare using more advanced methods such as observations to understand and evaluate the applicability of the AI system in healthcare.
Footnotes
Acknowledgments
We would like to extend our deepest gratitude to the study participants and the data collectors. Further more the principal investigator would like to acknowledge his student Nebiyat Birara (Neba) for her genuine support to enter part the collected data to the data entry software.
Guarantor
Mulugeta Desalegn Kasaye.
Ethical considerations
The Wollo University College of Medicine and Health Sciences institutional review board provided ethical clearance (Ref. No. = wucmhs 5884/13/24). A supportive letter was acquired from the Department of Health Informatics. Following an explanation of the study's purpose, each study participant provided written informed consent to participate in the current study. The study participants were informed about the significance and benefits of the study. The study participants were given the right to participate, refuse, or withdraw at any time. The data collection technique was conducted anonymously, and the participants’ anonymity was safeguarded.
Author contributions/CRediT
Mulugeta Desalegn Kasaye contributed to the design and conception of the study, collection, and analysis of the data, and interpretation of the findings, and contributed to writing the manuscript. Amare Gebrie Getahun has made substantial contribution to the design and conception of the study and supervised the whole research process during the data collection and write-up. Mulugeta Hayelom Kalayou has contributed to the design and conception of the study, collection, and analysis of the data, and interpretation of the findings, and contributed to writing the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.