
Abstract
Background
Family-centred goal setting is central to optimal care and outcomes for children with a disability. Digital innovations show promise for increased engagement and empowerment of families. While digital products have the potential to improve collaboration, there are barriers which may prevent service providers and families from using these resources.
Objective
This study aimed to: (a) understand goal sharing experiences of service providers and caregivers, and (b) identify views on a digital platform designed to share the goals of children with a disability between service providers and families.
Methods
Semi-structured interviews (n = 12) were conducted with paediatric service providers and caregivers in Australia. Transcripts were analysed using a qualitative content analysis approach.
Findings
Experiences of sharing goals were reflected in sub-categories: conversations and listening to families’ needs; collaboration and building relationships; adopting a family-driven approach; big picture and specific goals; communicating and documenting goals; goals need to be meaningful; using a structured approach; National Disability Insurance Scheme (NDIS) goals and challenges and barriers. Views on using a digital platform were captured by sub-categories: potential to empower families; collaboration and shared understanding; communication in your own time; everything in the same place; accessible and user friendly; functionality and preferred features; workload; some families might not engage with it and using new technology.
Conclusion
We developed an understanding of how the goals of children are shared and perspectives on a digital platform. These findings have implications for the development and implementation of digital health products designed to improve care for children with a disability.
Keywords
A family-centred approach to care is based on a set of underlying values, including an understanding that every family is unique and that a child's family are experts on their needs and abilities. 1 This approach emphasises partnership between service providers and families, acknowledging the important role that families have in planning and implementing care. 2 While recognised as best practice, there are barriers experienced in implementing integrated family-centred services for children living with disability in Australia. 2 Families often experience considerable burdens associated with coordinating care across multiple service providers.3,4 Fragmented care may result in duplication of services, higher costs, and negative experiences.
Collaborative goal setting is central to effective family-centred service for children with disability.5,6 Goal setting can be helpful for families and service providers in conceptualising what is planned, increasing engagement, and guiding care.2,7 Extant research has identified that although service providers often intend to use family-centred practices, there remain logistical problems when sharing and collaborating on goals.2,3,8 Goal setting occurs across multiple care providers, and there can be problems with sharing information (i.e. both with families and between organisations).
Integrated care is particularly important for people with chronic conditions and complex needs. It refers to an efficient and easy to navigate service system that is coordinated across sectors (e.g. health, social, and education) to optimally meet needs of the people using it. 9 In Australia, the ‘key worker model’ is one example of a service model for children with a disability that is designed to increase coordination of care. This model involves the delegation of a worker who is a single point of contact for a family. The model is designed to empower families, assist them in navigating services and increase the integration of care across different services.10,11
Despite the understanding that comprehensive and coordinated care leads to optimal outcomes for children with disability, there are barriers to achieving integrated care. Current health information systems may not optimally support or enable families to experience integrated information sharing across services. For example, goals are typically stored within health information technology systems that have been developed under the auspices of individual organisations (e.g. hospital records). Furthermore, families may not easily be able to contribute to their goals in a manner that is truly collaborative. Consequently, children with disability often have multiple sets of goals, which may lead to competing plans, increased fragmentation of care, and additional child and family burden.
Digital platforms and applications are emerging innovations to address the need for integrated health care.12–14 Globally, the COVID-19 pandemic contributed to a necessary and accelerated adoption of digital technologies in healthcare, leading to increased interest in its potential advantages.9,15,16 In the US, a recent set of guiding principles 9 for service provision for children with special health care needs described integration of information technology across sectors as a promising solution for improving care and reducing health disparity in access to services.
In paediatric disability care, digital platforms have the potential to allow families to set, store, share, and track goals with their child's care teams. Use of these products has potential to create a more collaborative, integrated way to share the goals of children and young people with a disability. Improved collaboration may have meaningful effects on family engagement, empowerment, quality of care, and outcomes. While digital products are promising, there are a range of potential barriers to sustainable uptake, including privacy concerns and data sensitivity, costs, training needs, complexity and usability of the product. It is clear that a wide range of considerations need to be understood and addressed for successful design and implementation of digital products in health care.12,13,17
Extant research has focused on the use of digital platforms in adult populations. For example, Babbage et al. (2024) trialled a tablet app intended to communicate goals for brain injury rehabilitation, through instructional videos. While the tablet app was found to improve collaboration in goal planning, there were challenges reported, including maintaining client engagement and integration of the tool with existing practices. 18 While the use of digital platforms to support family-centred goal sharing for children does not yet have a large research base, there is growing interest in the utility of technology in this context. A scoping review 19 on parent-led digital platforms for parents of children with disability found that the available literature has predominantly focused on the use of platforms with social interaction options (e.g. social media), search engines, medical websites, and health-related apps. Another recent study 14 reported on an implementation trial of a care-planning tool (Participation and Environment Measure-Plus; PEM+) for children with disability and found that overall it was a feasible and acceptable tool (from the caregivers perspective) to improve caregiver confidence and promote child participation.
Implementation science methodologies incorporating participatory co-design are crucial to ensuring the successful uptake of interventions to improve health care outcomes.12,20 A pre-implementation study is an important step to identifying possible barriers and facilitators for organisations, service providers, and families involved in goal setting for children with a disability. It is important to invest time in understanding the current processes and challenges, to avoid arriving at a solution prematurely. 12 Relevant end users should be engaged in the early stages of the conception of a digital innovation. 12 In the context of the current project, it was important to engage end users of the proposed digital platform, including caregivers raising a child with disability and health professionals.
The current study utilised qualitative methods to explore service provider and caregiver experiences of sharing goals and views on the use of a goal sharing digital platform. The aim of the current research was to better understand how the goals of children with disabilities are shared and to identify factors influencing use of a digital platform across health and community care systems. The following research questions guided the study:
How do service providers and caregivers describe their experiences of sharing and collaborating on the goals of children with disability? What are the views of service providers and caregivers on using a digital platform for sharing the goals of children with a disability and what factors do they perceive would influence implementation?
Method
Design
A qualitative approach was adopted to capture an in-depth understanding of caregiver and service provider perspectives. A steering committee was convened to oversee the project. The committee included experts from a range of disciplines (rehabilitation medicine, occupational therapy, psychology, physiotherapy, and digital health innovation), as well as two parents of children with disabilities. Parent members brought to the steering committee expertise from their own lived experiences of navigating health and disability services for their children. The steering committee met monthly throughout the course of the project (January 2023–March 2024). Members provided input on the study design, interview guide, recruitment, interpretation of findings, and the development of key recommendations. The design of the study is presented in Figure 1.

Qualitative data collection and analysis.
Ethical approval to conduct this study was granted by the Royal Children's Hospital, Melbourne, Human Research Ethics Committee (HREC94833). As per the approved protocol, all participants provided verbal informed consent prior to their participation in the research. This process involved emailing participants a study flyer and written information letter prior to the interview, confirming receipt of the letter and obtaining consent prior to commencement of the interview. A script was used to support this process, and verbal consent was documented on a standardised form. The design, procedure, and reporting of the study were informed and guided by the Standards for Reporting Qualitative Research. 21
Interview participants
Participants were recruited via convenience sampling, that is, a research flyer was distributed through networks of the steering committee and relevant organisations. As recruitment progressed, a purposive approach was employed to ensure that a range of disciplines and work settings were represented in the service provider sample. For the caregivers, purposive sampling ensured inclusion of parents of older and younger children.
The sample included nine service providers: medical rehabilitation specialists (n = 2); physiotherapists (n = 2); occupational therapists (n = 2); a speech pathologist (n = 1); a paediatrician (n = 1); and a social worker (n = 1) and three caregivers. At the time of interview, seven of the service providers worked in hospital (inpatient or outpatient) paediatric rehabilitation settings and two clinicians worked in paediatric private practices. These settings provided services for children with a range of disabilities, including cerebral palsy, spinal cord injury, acquired brain injury, and neurodevelopmental disorders.
All service providers identified as female and described their cultural background as Caucasian, Anglo-Saxon, and/or Australian. Service providers were in Australia: Victoria (n = 6); New South Wales (n = 2); and Western Australia (n = 1). Service providers reported an average of 20 years (range = 4–40 years) of experience in their discipline.
The three caregivers interviewed were all mothers of children with a disability. All caregivers had more than one child but focused their interview primarily around their experience with one of their children. Caregivers reported accessing a wide range of medical and disability services for their children (currently and historically). All caregiver participants lived in Victoria, Australia. Caregivers described their cultural background as Caucasian, Anglo-Saxon, and/or Australian.
Caregiver One was mother to a 17-year-old daughter attending a specialist school, with multiple diagnoses (intellectual disability, communication difficulties, delayed motor skills, oppositional defiant disorder, and autism) in the context of a genetic condition. Caregiver Two was mother to an 18-year-old daughter in a post-school program, with multiple diagnoses including autism, intellectual disability, cerebral palsy, and epilepsy. Caregiver 3 was mother to a 6-year-old son in his first year at a specialist school with multiple diagnoses (intellectual disability, physical disability, and epilepsy) related to a genetic condition.
Workshop participants
All interview participants were invited to attend a workshop. The workshop was attended by eight of the interviewed participants including: services providers from paediatric rehabilitation settings (n = 4), a private clinician (n = 1), and caregivers of young people with a disability (n = 3). A representative from a hospital health data analytics team (n = 1) attended the workshop to provide a digital health perspective.
Procedure
Interviews
Semi-structured interview guides were developed for service providers and caregivers (see supplementary material). The interview guides were informed by an implementation science framework, the Consolidated Framework for Implementation Research. 22 Questions and prompts were refined in consultation with the project steering committee.
Questions were focused on two main areas related to the research questions: (a) participants’ experiences of sharing and collaborating on children's goals, and (b) views on using a purpose-built digital platform to collaborate on goals. To set the scene, participants were informed that the digital platform would be designed specifically to share goals, be family-centred, and meet security requirements. A semi-structured interview approach allowed scope for participants to focus on details most pertinent to their own experience, and flexibility for the interviewer to probe for further details.
Interviews occurred between August and November 2023. Most interviews (n = 11) were conducted via a video conferencing platform. One interview was conducted over the phone due to technical difficulties. The majority of interviews were conducted by the first author (MW), with one completed by the second author (BO). The length of interviews ranged between 24 and 55 min. Caregiver participants received a $25 gift card to recognise the contribution of time from those in caregiver roles. Audio from the interviews was transcribed by a professional service. Transcripts were checked for accuracy and de-identified for analysis by MW.
Workshop
To verify and assist in the interpretation of the interview findings, a 2-h online workshop was facilitated by MW and project steering committee members (BO & RB) in February 2024. The workshop facilitators included two clinician-researchers and a parent of a child with disability. The aims of the workshop were to (a) obtain feedback on findings and (b) assist in the interpretation of findings. The structure of the workshop involved a presentation of the proposed categories and sub-categories from the interview analysis. The presentation was followed by a discussion guided by the following questions:
Which findings resonate with you? Are there any ideas that stand out as most important? Have we missed anything? Are there ideas that you thought might be identified that are not presented here? What do you think a digital platform would need to do to improve collaboration on goals? What do you think are the important considerations for implementing a goal sharing digital platform?
Caregiver workshop participants received an $80 gift card for their contribution. The workshop was recorded and professionally transcribed. The transcript was checked for accuracy and de-identified for analysis. Analysis involved one round of coding the transcript for main ideas (completed by MW), resulting in a categorisation of key discussion points. The discussion points were then mapped on to the categories that were identified through the interviews with the aim of confirming findings and providing an opportunity to extend on these ideas through reflection on the workshop discussion. The project steering committee de-briefed and finalised recommendations, informed by the interviews and workshop.
Analysis
Theoretical and analytic approach
This study used qualitative methods to explore the perspectives of key stakeholders in the context of paediatric disability settings. A critical realist position was taken, allowing an understanding of participants’ interpretations of their personal experiences. An inductive content analysis (ICA) was adopted for the analysis of interview transcripts, following the steps outlined by Vears and Gillam, 2022. This method has been described as a useful approach for data that is intended to inform practice or policy in health research. 23 The purpose of ICA is not to verify a pre-existing framework, but to derive a comprehensive understanding on the topic by identifying categories, supported by evidence in the dataset. 23 In ICA, there is not a focus on calculating frequencies of ideas in the data set; instead, the views of participants are coded, organised into categories, and described. In qualitative research, there is not an agreed method for determining adequate sample size. 24 In a practical sense, sufficient data is needed to address the research question. For this study, it was determined that enough interviews had been completed when transcripts were coded without the need to create new codes. Data saturation was determined to have been reached by discussion and agreement within the research team and members of the steering committee.
Data coding and organisation of categories
The following steps were followed: (a) carefully reading the transcripts, (b) organising the content into broad categories related to the research questions, (c) identifying sub-categories and refining, and (d) synthesising the categories and producing the final report. 23 Transcripts in the dataset were analysed in multiple rounds of coding (i.e. an iterative process) to refine the categories. Through this process, sub-categories were collapsed to avoid overlap or divided into separate codes when warranted. The codes prioritised semantic content (provided explicitly by participants) over interpreted latent ideas. Each sub-category was intended to convey a coherent meaning or idea, distinct from the other sub-categories in the overall framework. Coding was completed using NVivo Version 14 by the first author (MW). To enhance trustworthiness, reflexivity, credibility, transferability, and transparency were embedded in the planning and methodology of the study. 25
Reflexivity
The research team acknowledged that their own knowledge, experiences, characteristics, and biases were important to consider when undertaking qualitative research. The team considered and declared perceived, potential, and actual conflicts of interests at the beginning and throughout the research process. The project steering committee met monthly to discuss the progress of the research. These meetings allowed for reflection on the interpretation of findings and the incorporation of a range of perspectives. Additionally, the interviewer wrote a journal entry following each interview to consolidate the main ideas raised and observations that might be relevant to interpretation of the data.
Credibility
To aid credibility, three interview transcripts were randomly selected and coded by the third author (MD), a researcher with experience in qualitative methods external to the project steering committee. The double-coding was used to reflect on the understanding of the meaning of codes, consistency of coding, and refinement of the analysis. Further credibility measures were embedded in the research design where (a) the research steering committee brought diverse perspectives to early versions of the interview data analysis, and (b) workshop participants were provided an opportunity to learn about the findings of the study, provide feedback, and share additional ideas. Perspectives from these sources were considered in the final analysis and development of recommendations.
Transparency
Care was taken throughout the research process by reflective journaling, documenting minutes for steering committee meetings, maintaining an audit trail file of the coding rounds, saving versions of the NVivo file at different stages of the analysis, and sharing preliminary results for feedback during the workshop.
Transferability
The recruitment process and sample were described in detail to allow readers to make a determination about the relevance of the findings to other settings.
Results
Category 1: experiences of sharing and collaborating on goals
Nine sub-categories captured experiences of sharing and collaborating on goals. Table 1 provides a description of the Category 1 sub-categories and supporting quotes from interview participants. While a number of sub-categories revealed aspects of goal sharing that currently work well, challenges and barriers were also raised.
Category 1: experiences of sharing and collaborating on goals: sub-categories, descriptions and supporting quotes.

NDIS: National Disability Insurance Scheme.
The importance of the interactions and relationships between those involved in setting and sharing goals was highlighted by participants. Conversations and listening to the needs of families related to the conversations between service providers and families. Ongoing conversations are essential for identifying goals that meet the needs of young people and their families. Collaboration and building relationships captured experiences related to working in partnerships, both between service providers and between service providers and families. A Family-driven approach was described by participants, indicating that families of young people often come to service providers with goals, advocate for their child, and connect their care team. Participants expressed the importance of involving young people and their families in goals when possible.
Other sub-categories related to the processes involved in setting and management of goals. Participants explained that Goals need to be meaningful to the young person and relevant for their daily life. Goal setting often involves consideration of Big picture and specific goals, where broad goal areas are broken down into smaller, achievable steps. Goal setting is often supported by a framework and tools to measure progress (Using a structured approach). Experiences related to Communicating and documenting goals were described as well as the impact of the National Disability Insurance Scheme (NDIS) on goal setting, management, and sharing.
Participants shared Challenges and barriers that they have experienced when sharing and collaborating on goals including: difficulty with communication (particularly across organisational settings); limitations of existing platforms; difficulty collaborating with families; and limited funding or resources.
Category 2: views on using a digital platform for goal sharing
Participants shared their views on using a digital platform for collaborating on goals. The nine sub-categories related to Category 2 and supporting quotes from interview participants are shown in Table 2. Some ideas related to the specific features of the digital platform including Functionality and preferred features and Accessible and user friendly formats. These sub-categories contained views about what would make a platform useful (e.g. links to resources, capacity to upload videos), and the idea that the platform would need to be easy to navigate and accessible to all end users, including young people.
Category 2: using a digital platform for sharing goals of young people with a disability: sub-categories, descriptions and supporting quotes.

Other sub-categories related to potential advantages of a goal sharing digital platform, including: the Potential to empower families, Collaboration and shared understanding, Everything in the same place, and Communication in your own time. Participants expressed views that demonstrated understanding that a digital platform may be able to help families by giving them more control over their own goals, offering a system for keeping all goal-related information together, and increasing collaboration.
Factors that might impact uptake and implementation were covered in the sub-categories of Workload, Some families might not engage with it, and Using new technology. Participants acknowledged that a digital platform could either reduce or increase workload for service providers and families, depending on how well it fits with existing systems and responsibilities. Participants expressed the view that some families might not engage with a digital platform for a range of reasons including feeling overwhelmed by existing responsibilities, level of engagement, or socio-economic disadvantage. Some participants felt that the introduction of new technology could be met with resistance (e.g. concerns about privacy and security) whereas others felt adopting a new platform would be relatively straightforward.
The categories outlined in Table 1 include features of goal setting and sharing that need to be supported by the introduction of a digital platform. These involve features that participants expressed were important or necessary for the provision of optimal care and elements that facilitated collaboration (e.g. listening to families and building relationships). There were also barriers and challenges currently experienced by services (e.g. limited communication across settings) that present opportunities that a digital platform could be designed to address. In Table 2, views on the feasibility of a digital platform highlighted specific advantages (e.g. flexibility and individualised care) relative to goal sharing within the confines of standard face-to-face appointments. While the potential advantages of a digital platform were prominent in the findings, it was clear that there would also barriers to overcome with the introduction of new technology, including uptake, privacy concerns, and the burden of additional work.
Workshop
The workshop participants reflected on the aggregated interview participants’ views on a goal sharing digital platform. Reflections that aligned with sub-categories were evident throughout the workshop discussion. Additional considerations, ideas, and explanations related to the design and implementation of a goal sharing digital platform were raised by workshop participants, including:
A goal sharing digital platform needs to support collaboration in a way that is easy to navigate, presents defined advantages, and has potential to improve the current process. The introduction and implementation of a new platform needs to be carefully planned to ensure uptake and sustainability, particularly considering the needs of those who may be disadvantaged. The platform needs to be individualised and tailorable. It is important to understand that families have different needs. A flexible approach is required for families to have autonomy in what information they would like to share, how they would like to share it, and who they would like to share it with. Innovative features of a digital platform (such as the capacity to share photos and videos securely) could support families in being able to share their story and service providers to be able to see the ‘whole picture’. These features may help to keep goals active, by embedding them into everyday life. Supporting families through a transition from paediatric to adult disability and health services is important to consider in the introduction of a new process. This has been identified as an area where continuity of care is compromised. A digital platform for sharing goals would need to meet the needs of all proposed stakeholders (e.g. families, young people, clinicians, and organisations).
Discussion
This study aimed to better understand how the goals of children with a disability are shared and to identify factors influencing the use of a digital platform across health and community care systems. Results of an inductive qualitative analysis were organised into two categories (experiences of sharing and collaborating on goals and views on a digital platform for goal sharing) and associated sub-categories.
Experiences of sharing and collaborating on goals
Service providers and caregivers highlighted the importance of relational factors when setting and sharing goals. These factors included: collaboration and building relationships; conversations and listening to families’ needs; and adopting a family-driven approach, involving caregivers and young people. These interpersonal elements are central to family-centred practice. 2 Participants reflected that if a digital platform was introduced to improve goal sharing, it would be important for it to complement rather than attempt to replace the collaborative and relationship building interactions that currently occur during the goal setting process. While collaboration and communication were seen as essential to goal setting and sharing, challenges and barriers were experienced. Challenges involved limited communication (particularly across organisations), difficulty collaborating with families, limitations of existing platforms, and limited resources and funding. These findings suggest that there are areas where participants see potential for improvement in current goal sharing processes. The identification of challenges is consistent with extant research that has found that while family-centred practice is considered important, the implementation of these principles is not always achieved.2,3
Participants shared their experiences related to the setting and management of goals (e.g. big picture and specific goals, goals need to be meaningful, using a structured approach, communicating and documenting goals, and NDIS goals). Understanding how a new platform would fit with and add value to existing approaches and systems is important to consider, within the local context. Each service system presents unique strengths and challenges. For example, a recent Australian study 10 found reported that service providers experience challenges in achieving collaboration in early child intervention services under the NDIS, partly due to the transition from relationship-based early childhood intervention teams to individual therapy-focussed practitioners. A range of factors that could influence implementation, including the inner and outer settings (e.g. organisations and the community), processes, innovation characteristics, and the characteristics of the relevant stakeholders need to be understood.22,26
Views on a digital platform
Service providers and caregivers shared their views about using a digital platform that is secure, family-centred, and designed to share goals. The interview data indicated that participants could see potential for an improved process supported by a digital platform, reflected in the sub-categories collaboration and shared understanding; communication in your own time; potential to empower families; and everything in the same place. Previous research exploring what parents of children with disabilities want from their services has indicated a need for coordinated, individualised, and family-centred care. 3 There are specific and practical ways that digital innovations could support these needs and optimal outcomes through increased flexibility, coordination of teams and scheduling, information sharing, sharing of videos, and improved connections between therapy and home. 15
When introducing a digital platform, understanding what families are looking for from their services is critical. It is also important recognise that not every family has the same needs and may have different requirements and preferences. For example, Terwiel et al. (2017) found that parents of children with cerebral palsy varied in how they rated the importance of family-centred service elements. The authors highlighted that understanding what parents find important, and tailoring support, is essential for optimal service delivery. 27 From an implementation perspective, the construct of relative advantage or evaluation of whether a digital product leads to an improved process for all consumers should be considered.22,26
It was acknowledged by participants that there were known factors that could impact uptake and implementation of a digital platform, including workload, concerns about using new technology and recognition that some families might not engage with it. Barriers related to engagement and uptake of technology have been identified in digital health care implementation trials. 18 Barriers such as lack of motivation, privacy concerns, increased workload, and difficulty navigating new technology can be anticipated and considered in the introduction of a new platform. Participants expressed views on what they would like the platform to be able to do, including functionality and preferred features. It was identified as important that the platform would be accessible and user friendly. A feasibility investigation of an existing care planning digital innovation (PEM+) for children with disability found that while caregivers reported positive experiences (e.g. increased engagement in care planning) there were also concerns about the burden of using the tool. 14 The authors discussed the importance of exploring acceptability, usability, and optimising the design. 14 Similarly, for a goal sharing platform, feedback from end users (caregivers and service providers) will provide important information for design and implementation.
Recommendations
Analysis of qualitative interview data, the preliminary results workshop, and consultation with the project steering committee informed the general principles and proposed implementation steps presented in Figure 2.
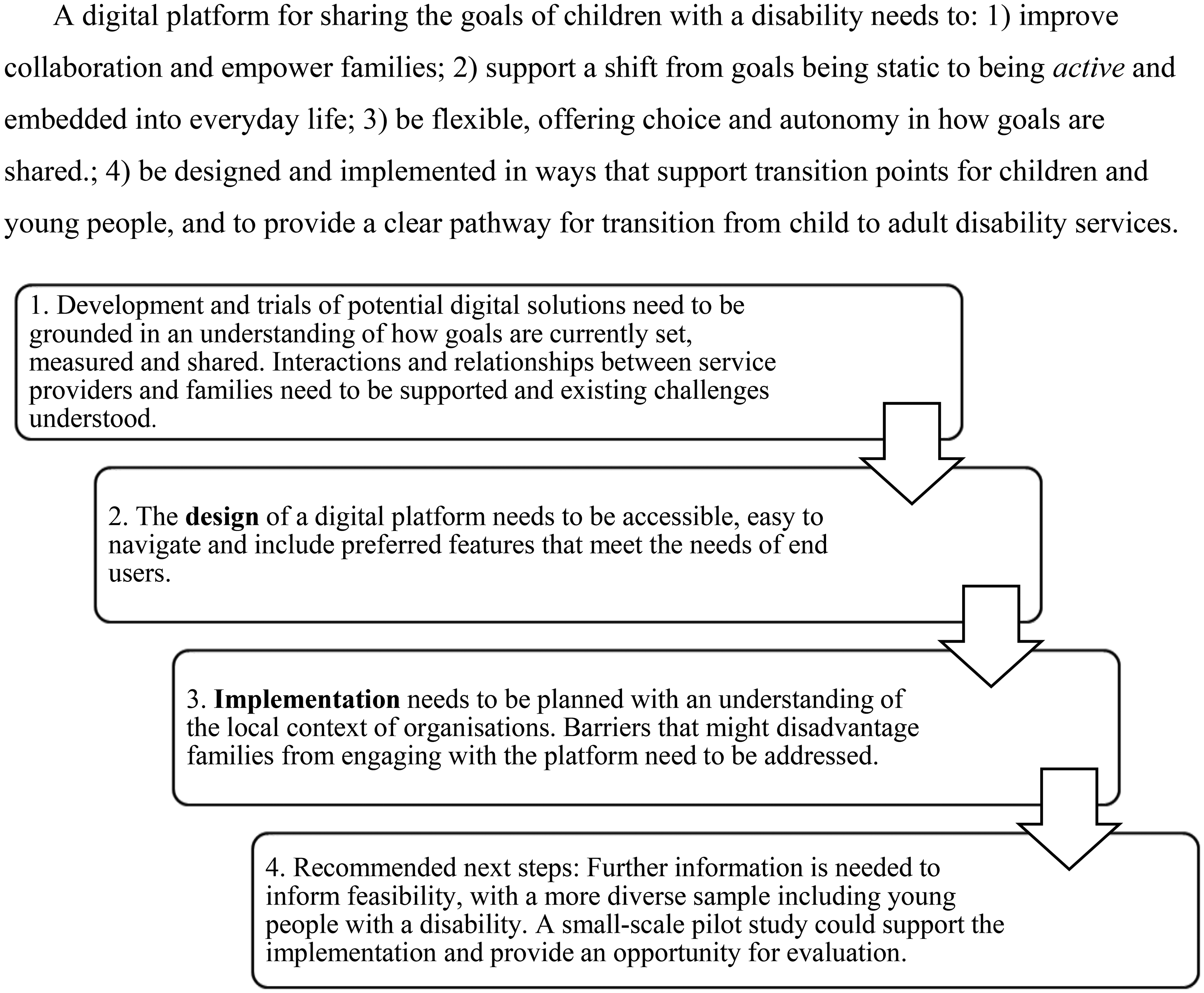
General principles and proposed implementation steps.
Strengths, limitations, and future directions
A strength of this study was the inclusion of the perspective of caregivers and service providers, at an early pre-implementation stage of the research process. Within the service provider subset, a range of professional disciplines were represented, including participants from three states of Australia and from public (hospital) and private organisations. This diversity of views was useful for identifying factors that are relevant to a range of stakeholders who may be users of a goal sharing digital platform. In other ways, the sample could have been more diverse. For example, all participants identified as female and Caucasian, Anglo-Saxon, and/or Australian. Since it was identified that some families may be at a disadvantage in engaging with a digital platform, investigating the views of caregivers and service providers from a variety of cultures will be an important future direction. Purposive sampling could be used to recruit participants from under-represented groups.
The sample of the current study included more service providers than caregivers. We were particularly interested in the barriers that exist for service providers in organisational settings. While this was intentional, it should be noted that including a greater number of service providers resulted in data more representative of this perspective. To extend on these findings, it would be beneficial to explore the experiences and views of more community and private service providers, as most of the sample were service providers employed in public paediatric settings. It would also be useful for implementation pilot studies to evaluate the effectiveness and acceptability of a digital platform from different perspectives within organisations (e.g. managers, clinicians, and administrators).
A future direction will be to explore the views of a larger sample of caregivers, including families with younger children, who were not well represented in this study. The perspectives of parents with younger children who are newer to navigating and coordinating services for the children would likely contribute different insights important for the design and implementation of a platform.
Participants of the current study and previous research6,28 highlighted the importance of involving children and young people in their goal setting. Unfortunately, this phase of the research did not include the voice of young people with a disability. To complement the caregiver perspective, it will be important to explore how children and young people with a disability participate in their goal setting, sharing, and collaboration.
Conclusion
This study aimed to better understand experiences of sharing and collaborating on the goals of young people with a disability and views on using a goal sharing digital platform. The findings identified a range of factors related to experiences of goal sharing, preferred design features, possible advantages, and implementation considerations. These factors represent important considerations for the development and implementation of a digital goal sharing platform for children with disability in the health context.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251319827 - Supplemental material for Feasibility of a goal sharing digital platform designed to empower children with disability and their families: A qualitative, pre-implementation study
Supplemental material, sj-docx-1-dhj-10.1177_20552076251319827 for Feasibility of a goal sharing digital platform designed to empower children with disability and their families: A qualitative, pre-implementation study by Meghan Wilson, Bridget O’Connor, Marnie Drake, Adam Scheinberg, Christine Imms, Rose Babic, Danny Hui, George Charalambous and Sarah Knight in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251319827 - Supplemental material for Feasibility of a goal sharing digital platform designed to empower children with disability and their families: A qualitative, pre-implementation study
Supplemental material, sj-docx-2-dhj-10.1177_20552076251319827 for Feasibility of a goal sharing digital platform designed to empower children with disability and their families: A qualitative, pre-implementation study by Meghan Wilson, Bridget O’Connor, Marnie Drake, Adam Scheinberg, Christine Imms, Rose Babic, Danny Hui, George Charalambous and Sarah Knight in DIGITAL HEALTH
Footnotes
Acknowledgements
We are grateful to the caregiver and service provider participants of this study. We truly appreciate their willingness to give their time and share their valuable insights on this topic. We also acknowledge the Centre for Health Analytics (Royal Children's Hospital, Melbourne) for their consultation and guidance throughout the project.
Contributorship
MW was involved in conceptualisation, methodology, investigation, formal analysis, writing – original draft, and writing – review and editing. BO was involved in conceptualisation, methodology, investigation, formal analysis, and writing – review and editing. MD was involved in formal analysis and writing – review and editing. AS, CI, RB, and DH were involved in conceptualisation, methodology, formal analysis, writing – review and editing. GC was involved in conceptualisation and methodology. SK was involved in conceptualisation, methodology, formal analysis, writing – original draft, and writing – review and editing
Consent to participate
All participants provided informed verbal consent (recorded by researcher) prior to their participation in the research.
Declaration of conflicting interests
CI holds the position of Director of Healthy Trajectories (the funding body). Due to this role, CI was not involved in grant adjudication or management of the grant. Grant-related decisions were deferred to other funding body team members. BO held a position on the Health Trajectories grant team, however, was not involved in the assessment of this project, ranking of applications, or the management of this project. DH is the founder of Sameview (a digital platform that could be implemented in health care settings); however, this study was exploratory and focussed on views about digital platforms in general.
Ethical Approval
Ethical approval to conduct this study was granted by the Royal Children's Hospital, Melbourne, Human Research Ethics Committee (HREC94833).
Funding
This research was funded by SEED funding from Healthy Trajectories: A Child and Youth Disability Hub, an initiative of the Melbourne Children's Campus and The University of Melbourne.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.