
Abstract
Introduction
Implementing Big Data Analytics (BDA) could enhance the efficiency and effectiveness of Community Health Centres (CHCs). This study focuses on improving healthcare service delivery in CHCs located in the Nkangala District through the adoption of BDA. It identifies a specific research gap and seeks to consolidate existing knowledge while revealing challenges and opportunities in BDA implementation.
Methods
This literature review was conducted using a systematic method that adheres to PRISMA principles. The review process involved the identification and selection of peer-reviewed publications in English up to 2024. The search was carried out among several major academic databases, including PubMed, Taylor & Francis Online, Google Scholar, IEEE Xplore, SpringerLink, ScienceDirect, and JSTOR. Specific search terms related to data-driven approaches and healthcare service delivery were used. The inclusion criteria focused on studies addressing the adoption and implementation of BDA in CHCs, while exclusion criteria eliminated studies not relevant to this context. The selected studies were analysed to assess the research state, identify key themes, and highlight gaps and challenges in BDA adoption within CHCs.
Results
A total of 31 studies met the inclusion criteria, demonstrating variability in study design, geographic location, and focus areas related to BDA adoption and implementation. The synthesis of results unveiled common challenges, best practices, and outcomes associated with BDA implementation, including technological, organizational, and human factors influencing successful integration.
Conclusion
The development and implementation of data-driven methodologies in healthcare service delivery present several challenges, including evidence limitations such as heterogeneity in study designs, restricted generalizability, and variability in study quality. Additionally, the short duration of many studies complicates the evaluation of their long-term impacts. Despite these challenges, the transformative potential of data-driven approaches highlights the necessity for further research to enhance adoption strategies and address existing research gaps.
Introduction
The healthcare delivery landscape is experiencing a profound transformation, with CHCs increasingly pivotal in delivering accessible and comprehensive services to diverse populations. As noted by Kvedar et al., the concept of “connected health” holds substantial promise for enhancing healthcare outcomes by employing technology to improve patient engagement and care coordination 1 . A significant facet of this technological integration is the adoption of advanced technologies such as big data analytics (BDA), which can vastly improve the efficiency and effectiveness of CHCs. Big data analytics serves as the technological backbone of data-driven healthcare, encompassing sophisticated data processing and modelling capabilities that interpret the extensive and intricate datasets inherent in the healthcare sector 2 . Raghupathi and Raghupathi underscore that BDA facilitates improved decision making, cost reduction, and enhanced patient outcomes, asserting that it can “improve decision making, reduce costs, and enhance patient outcomes” 3 . By utilizing the immense structured and unstructured data produced within the healthcare ecosystem, BDA provides essential insights that enhance decision making and optimize resource allocation, ultimately leading to improved healthcare outcomes.
Service delivery refers to the degree to which public services such as policing, defence, healthcare, and education meet or exceed the expectations of the beneficiaries, who are the public [86]. In the realm of healthcare, augmenting service delivery is vital to ensure that healthcare services meet or surpass public expectations. Despite the promising potential of BDA in CHCs, its implementation encounters several challenges. Issues concerning data interoperability, technological constraints, and resistance to change significantly hinder the successful adoption of BDA in these centres. Li et al. emphasize that “data interoperability is a major challenge in healthcare big data analytics” 4 . Nevertheless, the potential to improve service delivery and operational efficiency through data-driven approaches remains promising. This study aims to explore these complexities by synthesizing existing research, identifying key gaps, and highlighting opportunities afforded by BDA adoption in CHCs.
The impetus for this review stems from a notable gap in the literature regarding the specific context of CHCs. While numerous studies have investigated BDA within broader healthcare frameworks, there is a scarcity of focused research on the distinct characteristics and requirements of community-based healthcare settings. Singh and Singh highlight the necessity for increased research into BDA within community health, noting that “there is a dearth of studies on BDA in community health settings” 5 . This review seeks to address this gap by systematically cataloguing current knowledge and providing insights that can inform practice, policy, and future research.
The primary objective of this study is to evaluate existing research on the adoption of BDA in CHCs, specifically within the Nkangala District. By comprehending the crucial role of data analytics, the study aims to identify effective strategies for integrating BDA to enhance healthcare service delivery. Throughout the review process, stakeholders, including healthcare practitioners, policymakers, IT professionals, and community health workers, will be engaged to ensure that the findings are relevant and actionable. The approach involves developing tailored knowledge translation strategies for these stakeholders, fostering a collaborative environment that supports the effective implementation of BDA in CHCs.
In conclusion, this study seeks to synthesize current knowledge related to BDA in community health settings, offering a robust framework for understanding its potential impact on healthcare delivery. By addressing existing challenges and discovering new opportunities, the study aims to contribute meaningfully to the discourse on leveraging big data to improve the quality and effectiveness of healthcare services. Subsequent sections will outline the methodology used, key findings, and implications for practice and future research.
Methods
Inclusion and exclusion criteria
This review included studies that focused on both the adoption and implementation of Big Data Analytics (BDA) in Community Health Centres (CHCs). Eligible studies were those that examined strategies, interventions, or initiatives aimed at enhancing healthcare service delivery through data-driven approaches. Studies published in peer-reviewed journals were included. Non-peer-reviewed literature, such as conference abstracts or editorials, and studies unrelated to healthcare service delivery or BDA in CHCs were excluded.
Search strategy
A comprehensive search was conducted across several major academic databases, including PubMed, Taylor & Francis Online, Google Scholar, IEEE Xplore, SpringerLink, ScienceDirect, and JSTOR, to ensure a thorough review of relevant literature. The search was conducted up to the year 2024, with no language restrictions, although only English language publications were included. The date of the last search for each database is recorded in the search log.
The selection of studies followed stringent guidelines, as outlined in Table 1. This table presents the inclusion and exclusion criteria used to filter relevant studies. For instance, only empirical studies focusing on the adoption and implementation of BDA in CHCs were included, while non empirical studies or those unrelated to healthcare service delivery were excluded. Additionally, only peer-reviewed journal articles in English were considered, excluding non-peer reviewed literature and non-English publications. The criteria also emphasized studies that reported measurable outcomes related to BDA adoption and its impact on healthcare service delivery in CHCs.
Study selection guidelines.

Search terms and syntax
The search strategy utilized specific terms such as “big data analytics,” “healthcare service delivery,” and “community health centres.” Boolean operators and filters were applied to refine the results. Full search strategies, including filters and limits used, are detailed in Table 2.
Search strategies, filters, and limits are used across databases.

Study selection process
The study selection process involved a two-stage screening procedure. Initially, titles and abstracts were screened against predefined inclusion and exclusion criteria by multiple independent reviewers. Discrepancies were resolved through discussion. Subsequently, selected articles underwent a full-text review to confirm eligibility. Automation tools were not used in the screening process.
Data collection
Data items:
The data items collected during the present study consisted of various elements from the selected studies. These included:
▪ Authors and Year of Publication: Identification of the primary and secondary authors along with the year of publication. ▪ Title of the Study: Capturing the full title to understand the specific focus of the research. ▪ Study Design and Methodology: Documentation of the research design (qualitative, quantitative, mixed methods) and the methodologies employed in each article. ▪ Analytical Methods Used: A summary of analytical approaches adopted within the studies, such as descriptive statistics, inferential statistics, machine learning techniques, etc. ▪ Settings and Geographic Locations: The context of the studies regarding geographic regions and specific healthcare settings, especially focusing on Community Health Centres (CHCs). ▪ Target Population: Description of the populations studied, including any specific demographic information provided within each research article.
Outcomes:
The outcome measures extracted from the studies primarily focused on the effects of BDA on healthcare service delivery within CHCs. Key outcomes included:
▪ Improvements in Patient Care: Metrics related to changes in patient health outcomes, such as reduced hospital readmission rates, improved patient satisfaction, and enhanced care quality. ▪ Operational Efficiency: Outcomes measuring the effectiveness of BDA in streamlining processes, reducing costs, and increasing resource allocation efficiency within CHCs. ▪ Decision-Making Capabilities: The impact of BDA on the efficiency and effectiveness of healthcare decision-making processes, including evidence-based practice adoption.
Other Variables:
Besides the primary outcomes, additional variables considered in the data collection process included:
▪ Barriers to BDA Implementation: Identification of challenges faced during the adoption of BDA in CHCs, such as technological limitations, organizational resistance, and training needs. ▪ Facilitators of BDA Adoption: Factors that promote the successful implementation of BDA, including stakeholder engagement, resource availability, and supportive policies. ▪ Study Quality Indicators: Assessment of the methodological quality of each study, focusing on biases, sample size, and overall rigor as determined using tools like the CASP checklist.
Quality appraisal using the critical appraisal skills program (CASP) checklist
The CASP Checklist is widely recognized as an effective instrument for assessing the quality of qualitative research, particularly in health-related studies. 6 Endorsed by the Cochrane Qualitative and Implementation Methods Group, this checklist is especially valuable for novice researchers engaging in qualitative evidence synthesis. The CASP Checklist provides a systematic approach for evaluating studies, with a focus on key aspects such as research design, data analysis, and the rigor of the findings. 6
In this study, the quality of the selected articles was appraised using the CASP Systematic Review Checklist. Both quantitative and qualitative studies were evaluated independently by two reviewers using the CASP checklist and other established tools. Any discrepancies between the reviewers were resolved through discussion. Importantly, automated tools were not used in the quality appraisal process.
Effect measures
The effect measures used in the synthesis included risk ratios, mean differences, and other relevant statistics, depending on the nature of the data reported in the studies.
Synthesis methods
Addressing risk of bias due to missing results
Risk of bias due to missing results was assessed by examining reporting biases and considering the completeness of outcome reporting across studies.
Certainty in the evidence
The certainty in the body of evidence for each outcome was assessed using established methods, considering factors such as study design, consistency of results, and directness of evidence.
Results
Study selection
Search and selection results
The search strategy identified a total of 929 records from various databases. After removing duplicates, 833 unique records were screened based on their titles and abstracts. This screening process led to the assessment of 104 full-text articles for eligibility. Ultimately, 31 studies met the inclusion criteria and were included in the systematic review. Reasons for exclusion included duplicate papers from different databases (96 studies), irrelevant topics, and inappropriate study designs.
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram (Figure 1) illustrates the search and selection process, showing the number of studies identified, screened, assessed for eligibility, and included in the final review, as well as the reasons for exclusions at each step.

PRISMA flow diagram.
Publication year of included studies
The timeline data presented in Table 3 illustrates significant trends in the publication of journal research papers utilized in the present study across various academic databases from 2019 to April 30, 2024. Overall, publishing activity has exhibited notable variability, marked by a peak in article output during 2019 and 2020. Specifically, the maximum number of publications occurred in 2019 with a total of 9 articles on Google Scholar, further underscored by contributions from other databases, particularly in 2020. However, there has been a dramatic decline in publication activity in 2023 and 2024, suggesting a potential decrease in research output or a shift in focus in the types of research being published during these years.
Sources searched for years 2019–2024 (including articles up to April 30, 2024).
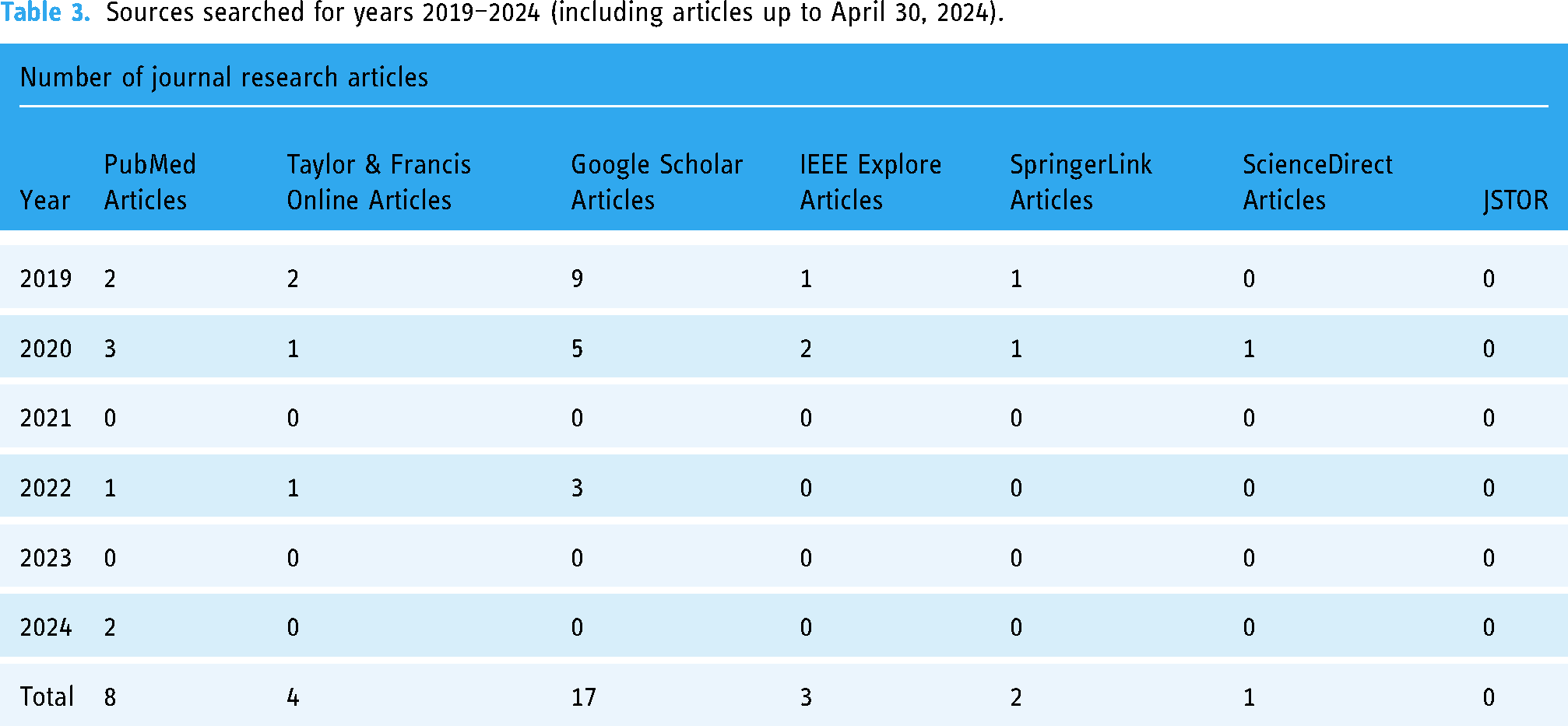
Examining database-specific trends reveals that certain platforms have been utilized more frequently than others. PubMed has demonstrated consistent, albeit minimal, publishing activity over the years, peaking in 2019 and 2020. Conversely, Taylor & Francis Online, SpringerLink, and JSTOR did not contribute any articles during this period, suggesting these databases may not have been primary sources for the study topic or were inadequately represented by the chosen search terms.
Google Scholar stands out as the most productive source, particularly in 2019 and 2020, with a noticeable drop in published articles, thereafter, highlighting a decline in activity with no publications in both 2023 and 2024. Similarly, IEEE Explore yielded only three articles throughout the years, all published in 2019 and 2020, with no further contributions since then. In contrast, ScienceDirect displayed erratic trends, contributing only five articles, primarily in the earlier years.
Overall, the data indicates a pronounced peak in research publications during 2019 and 2020, especially on Google Scholar, potentially reflecting heightened interest in specific research topics at that time. The subsequent decline in publications post-2022 could signal a shift in research priorities, decreased productivity, or changes in indexing practices across different databases. The absence of publications from certain databases further emphasizes the diversity in source utilization, suggesting that various research areas may depend on different platforms.
Tools and technologies identified
The systematic review identified several Big Data tools and platforms that have been employed in the studies to enhance healthcare service delivery, particularly in CHCs. These tools vary in their capabilities, ranging from data storage solutions to advanced analytics platforms. Table 4 provides a summary of the key tools identified in the reviewed literature.
Big Data Tools Identified in the Reviewed Studies.
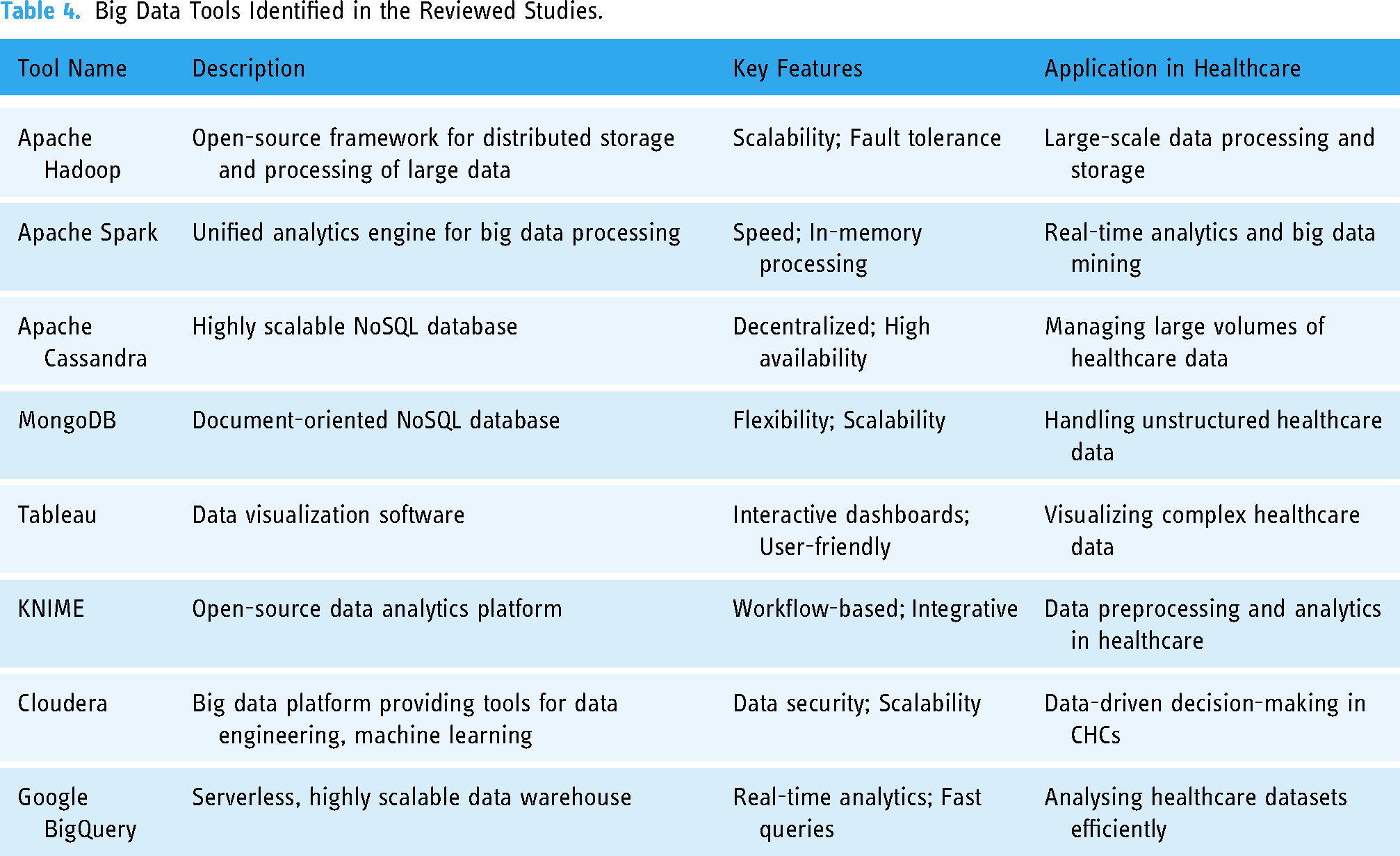
These tools have been applied across different levels of healthcare service delivery, including data integration, predictive analytics, and real-time monitoring, contributing significantly to improving patient outcomes and operational efficiency in CHCs. The diversity of tools highlights the various approaches taken by researchers to leverage Big Data in healthcare.
Excluded studies
Several studies that appeared to meet the inclusion criteria were excluded. Reasons for exclusion included:
▪ ▪ ▪
Characteristics of included studies
The methodological diversity evident among the studies included in the present study is significant, encompassing approaches that range from qualitative interviews to quantitative surveys. Each study contributes unique theoretical frameworks and empirical insights into the application of BDA in healthcare settings. The characteristics of these studies, including identified gaps, methodologies, assessment criteria, and theories employed, are summarized in Table 5.
Characteristics of Included Studies

Table 5 illustrates the variety of research frameworks and findings, highlighting how different studies have approached common challenges such as data integration, privacy concerns, and the application of big data in improving patient care. The table provides a comprehensive overview of the studies, facilitating a clear understanding of how BDA intersects with healthcare delivery and outcomes.
Identified research gaps and challenges in included studies
The literature review reveals several research gaps and challenges that hinder the effective utilization of Big Data Analytics (BDA) in healthcare. Notably, the integration of structured and unstructured data poses a significant challenge, necessitating the development of improved data management frameworks and standards.32,35–37 Additionally, pervasive concerns regarding data privacy and security substantially impede the implementation of BDA.8,17,23,27,37
There is an urgent need for more empirical research, particularly in developing countries, to comprehensively understand the adoption of BDA and its implications for healthcare.29,35,38,39 The literature also highlights the lack of standardized analytical frameworks as well as managerial and organizational limitations that must be addressed to align BDA with broader business strategies.39–43 Furthermore, resistance to change among healthcare employees presents a significant barrier to successful BDA adoption.38,39
Moreover, the need for clearer ethical guidelines and legislative frameworks concerning data usage and patient privacy is evident.16,23 Limited community engagement in data processes and a general deficiency in technological capabilities and training within healthcare organizations are also critical gaps needing attention.22,41 Lastly, the literature emphasizes the necessity for systematic evaluations of BDA applications to assess their effectiveness in improving patient outcomes and operational efficiencies. 42
Bias assessment of included studies
The assessment of bias risk was conducted using the Critical Appraisal Skills Programme (CASP) checklist, revealing a moderate to high risk of bias in several studies included in the present study. Key issues contributing to this risk included inadequate sample sizes and selective reporting, both of which are critical for assessing the validity of reported outcomes (Table 6).
Risk of Bias in the Included Studies.

Identified risk of bias in included studies
The assessment of risk of bias conducted in this systematic review reveals a range of potential biases within the included studies, highlighting important considerations for interpreting the findings. Overall, several studies demonstrated a moderate to high risk of bias due to various factors. Common issues contributing to this risk included inadequate sample sizes, which limit the generalizability of the results, and selective reporting practices that can distort the validity of outcomes. A significant number of studies utilized cross-sectional designs, thereby restricting the ability to evaluate longitudinal effects and potentially overlooking important causal relationships. The reliance on self-reported data in some studies raised concerns regarding response bias, further complicating the evaluation of findings. Moreover, the inherent subjectivity in qualitative analyses introduces additional risks related to interpretation bias. Additionally, potential publication bias was noted, as the review may not fully represent the landscape of research on Big Data Analytics due to the exclusion of unpublished and non-peer-reviewed studies. This limitation underscores the need for caution when drawing conclusions from the existing literature.
Results of syntheses
The synthesis revealed converging themes highlighting enhanced patient care, improved operational efficiency, and streamlined administrative processes due to BDA implementation. However, significant barriers such as technical challenges and organizational resistance were also identified.
Statistical syntheses
Given the heterogeneity of study designs, statistical meta-analysis was deemed inappropriate. Thus, qualitative synthesis was employed to extract and analyse common patterns, emphasizing the vital role of BDA in transforming healthcare delivery models.
Investigation of heterogeneity
Subgroup analyses indicated contextual dependencies in the effectiveness of BDA, with studies from urban CHCs generally reporting more favourable outcomes than those situated in rural areas.
Sensitivity analyses
Sensitivity analysis, which excluded higher-risk studies, affirmed the positive impacts of BDA on patient care improvements and underscored the need for methodological rigor in future research.
Certainty in the body of evidence
The certainty of evidence regarding BDA implementation in CHCs was classified using GRADE criteria. While some benefits are observed, the limitations inherent to study designs necessitate caution and the encouragement of longitudinal studies for more robust evidence.
Discussion
This systematic review contributes to the growing body of evidence supporting the transformative potential of Big Data Analytics (BDA) in enhancing healthcare delivery within Community Health Centres (CHCs). Our findings, demonstrating enhanced patient care, improved operational efficiency, and streamlined administrative processes through BDA implementation, align with several previous systematic reviews.2,43 These studies, like ours, underscore the crucial role of effective data integration in optimizing healthcare services. However, our review extends this understanding by providing a more granular analysis of the challenges specific to the CHC context, particularly within the resource-constrained environment of the Nkangala District.
In contrast to some broader reviews that focus on BDA across various healthcare settings,32,36,44 this review specifically targets the unique challenges and opportunities presented by CHCs. This targeted approach reveals nuances not captured in broader analyses. For example, while prior research has identified technological limitations as a major barrier to BDA adoption,39,40 our review highlights the amplification of these challenges in resource-limited CHC settings, particularly evident in rural areas as shown by our subgroup analyses. Furthermore, the heterogeneity in study designs, a limitation acknowledged in other reviews, 40 underscores the critical need for more robust methodological consistency and, importantly, longitudinal studies to comprehensively evaluate the long-term impacts of BDA implementation. The dearth of longitudinal data is a significant limitation hindering a definitive assessment of sustained benefits.
A comparison with Al-Sai et al.'s 44 review, which explores BDA applications and opportunities, reveals a complementary focus. While Al-Sai et al. provide a broad overview, our review delves deeper into the CHC-specific context, offering insights into the practical challenges and facilitators of implementation within these settings. Similarly, while studies like Liang et al.'s 45 systematic review on BDA adoption in healthcare organizations provide valuable contextual information, our study offers a more focused examination of the challenges within the unique operational realities of CHCs, particularly in under-resourced environments. This contributes to a more nuanced understanding of the practical considerations needed for successful implementation.
This review also acknowledges limitations. The potential for publication bias, resulting from the exclusion of grey literature, warrants careful consideration. This limitation, coupled with the inherent methodological limitations of many included studies (e.g., predominantly cross-sectional designs, 46 reliance on self-reported data]), necessitates a cautious interpretation of the findings. The moderate to high risk of bias identified in several studies using the CASP checklist further emphasizes the need for future research utilizing more robust methodologies to minimize these limitations and enhance the certainty of the evidence.
Conclusion
This systematic review provides strong evidence of the potential benefits of BDA implementation in CHCs, offering improved patient care and operational efficiency. However, successful adoption and integration face considerable challenges, including technological limitations, data privacy concerns, organizational resistance to change, and the need for enhanced training. The current evidence, while suggestive of BDA's potential, is characterized by moderate certainty and significant risks of bias. Future research should prioritize longitudinal studies with rigorous methodologies and diverse CHC representations to strengthen the evidence base and to guide effective implementation strategies. Policy changes should address the resource allocation for training, infrastructure development, and ethical guidelines. Collaborative efforts among healthcare practitioners, policymakers, and technology specialists are vital to overcoming existing barriers and fully realizing BDA's transformational potential of BDA in improving healthcare service delivery within CHCs.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251314548 - Supplemental material for Improving community health centres with big data analytics: A systematic literature review on adoption
Supplemental material, sj-docx-1-dhj-10.1177_20552076251314548 for Improving community health centres with big data analytics: A systematic literature review on adoption by Pascal Ndikuyeze and Phahlane Mampilo in DIGITAL HEALTH
Footnotes
Acknowledgements
Thank you to Tebogo Lejaka from the University of South Africa for his ongoing research contributions and Ayanda Sithole for their ongoing encouragement.
Contributorship
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this systematic review was deemed unnecessary, as the research relied solely on the analysis of secondary data published in peer-reviewed journals.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Pascal Ndikuyeze
Patient consent
In conducting the present study, no primary data collection involving human participants was undertaken. Therefore, obtaining individual patient consent was not applicable. The studies included in this review utilized existing literature and data that were publicly accessible and did not involve direct interaction with patients or identifiable individual data.
Systematic review registration
This review is registered with PROSPERO (ID: CRD42024580100), any changes to the published record will be reported.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.