
Abstract
Objective
Digital health technologies offer a more equitable way of providing access to health education. This study engaged consumers and clinicians from two Australian regions with a high burden of oral disease to develop a digital oral health resource called “TOOTH” tailored for adults.
Methods
A total of three focus groups (one clinician and two consumers) were conducted to identify themes that were used to draft text message content. The study team reviewed, refined, and mapped these messages to behaviour change techniques and developed videos to support key concepts.
Results
Eight multidisciplinary clinicians (dentist, oral health therapist, dietician, cardiac nurse, and dental nurse), 75% female with a mean age of 48 ± 10 years, and seven consumers from a metropolitan and a regional area in New South Wales, 43% female with a mean age 62 ± 11.6 years participated in the focus groups. Key themes identified by clinicians included (1) limited support from medical and allied health teams for integrating oral health care into the healthcare system, (2) government-supported measures enable prevention, and (3) poor oral health of Australians. Consumers highlighted (1) barriers to accessing oral health care, (2) negative attitudes towards oral health, and (3) limited oral health-related knowledge. The final resource developed includes 81 text messages sequenced to ensure a gradual increase in knowledge and skill and five supporting videos.
Conclusions
The TOOTH resource has the potential to improve awareness and knowledge regarding oral disease prevention, enabling more equitable access to oral health education and better self-management of oral health.
Introduction
Oral diseases, including tooth decay, gum disease (periodontitis), edentulism (total tooth loss), and cancer of the lip and oral cavity, are largely preventable. However, over the last 30 years, these conditions have increased globally, affecting nearly 3.4 billion people. 1 The two most prevalent oral diseases, tooth decay, and periodontitis, can impact the individual throughout their lifetime. Dental decay affects the primary dentition in childhood and the permanent dentition from late adolescence to adulthood. 2 Periodontitis typically emerges later in life, peaking around age 60, while total tooth loss peaks around age 70. 1 Traditionally, oral health care has focused primarily on the intervention and treatment of oral diseases, with limited attention on managing their underlying causes. 2
Oral health is closely linked to general health; both periodontitis and tooth loss have been shown to be associated with increased risks of cardiovascular disease (CVD) and all-cause mortality. 3 Notably, periodontitis has a bidirectional relationship with type 2 diabetes mellitus (T2DM), serving as both a cause and consequence of T2DM. 4 Additionally, tooth loss has been linked to a higher risk of developing diabetes and its complications,5,6 increased frailty, 7 and cognitive decline. 8 Many adults, however, remain unaware of the significant impact oral disease can have on overall health. 9 Even for those who do understand the oral-systemic health connection, access to care can be challenging.
In many countries, including Australia, oral health care is predominantly delivered through the private sector leading to inequitable access. 10 Socially disadvantaged populations including those on low incomes, those experiencing homelessness, harmful drug and alcohol use, and those from culturally and linguistically diverse communities face significant economic barriers to accessing oral health care. 10 Consequently, those living in socio-economically disadvantaged areas often have a higher burden of oral disease 10 and poor oral health literacy. 11 The limited access to oral health care highlights the need to identify alternative strategies to provide oral health information and reduce disparities in oral health outcomes. Inequalities to care maybe reduced through the use of mobile phone text message support which have proven effective in changing various health behaviours, including smoking cessation, 12 increasing physical activity, 13 and improving lifestyle behaviours and medical adherence in CVD and diabetes.14,15 Text message-based oral health education has been shown to enhance oral hygiene in children,16,17 and adults.18,19 While some studies provide details on developing oral health-related text message content for children, 20 there is a lack of detail for the development of oral health-related text message content for adults. Therefore, this study aimed to engage both consumers and clinicians in creating a bank of text messages designed to motivate behaviour change and support good oral health practices in adults.
Methods
This qualitative study used focus groups to gather in-depth insights and perspectives on knowledge, beliefs, and experiences associated with oral health care along with feedback on sample text messages and video content from a diverse range of adults and healthcare staff in New South Wales (NSW) Australia. Ethical approval for the study was obtained from the Western Sydney Local Health District Human Research Ethics Committee (2023/ETH01673) and the Charles Sturt University Human Research Ethics Committee (H23882). The study was conducted following the Consolidated Criteria for Reporting Qualitative Studies (COREQ). 21
Setting and participants
Consumers were patients attending clinical services at the recruitment sites. Consumers and clinicians were recruited on-site using convenience sampling between November 2023 and March 2024 from Westmead Hospital which is a tertiary referral hospital in a metropolitan area in Western Sydney with a large culturally and linguistically diverse population 22 and from a university dental clinic in Orange, which is a regional area in Western NSW servicing a large regional and rural population. Inclusion criteria for consumers included adults aged 18 years and older able to read and understand English attending either the Westmead Centre for Oral Health or the cardiac rehabilitation clinic at Westmead Hospital or the dental clinic at Charles Sturt University in Orange. Any adults with a cognitive impairment that impacted their ability to read and understand written material were excluded. Inclusion criteria for clinicians included any clinicians employed by Westmead Hospital working in the oral health or cardiac rehabilitation clinics at Westmead Hospital.
Surveys and focus groups
To recruit participants for the focus groups, flyers were placed in the relevant clinics at Westmead (clinicians and consumers), and at Orange for consumers only. The flyers outlined the aims and intent of the research and provided a brief description of the study procedures. Clinic staff directed interested participants to complete an expression of interest (Supplemental Material), once this was received a member of the research team (SK) contacted the participant using the preferred method of contact as specified on the expression of interest. The study aims and processes were explained to the participant and a link to the eConsent form 23 (Supplemental Material) was provided. Once a completed eConsent form was received, an online survey (Supplemental Material) delivered through the research electronic data capture (REDCap) platform hosted at the Western Sydney Local Health District 24 was sent to the participants so that they could review sample text message content, and provide demographic information prior to the focus group session. The consumer survey collected demographic information (age, country of birth, language other than English spoken at home, and educational level), number of teeth, and basic medical and oral health details; and included five sample text messages and two videos. The clinician survey collected demographic information (age and sex) and the professional background of participants in addition to a sample of ten text messages and three videos. The sample text messages used in the initial survey were generated using ChatGPT guided by Australia's public health messages. 25
Three 90-minute focus groups were conducted, one multidisciplinary clinician focus group, and two patient focus groups. The decision regarding the number of focus groups to conduct was based on pragmatic factors such as time and cost. 26 The focus groups were conducted on site and were facilitated by members of the research team with experience in focus group facilitation, EO a qualified physiotherapist conducted the clinician focus group and SK a qualified dentist conducted the consumer focus groups. Focus group guides specific for consumers or clinicians (Supplemental Material) were used to lead discussions and an additional member of the research team observed and recorded field notes during the session. Audio recordings of the focus groups were transcribed by a trained professional and verified by SK. To ensure participant confidentiality once the audio recordings were transcribed, they were deleted, and the transcribed interviews were not identifiable. Additionally, all identifying information was stored separately from the focus group transcripts and accessed only by authorised researchers. The purpose of the focus group interviews was to learn participants views on oral health, get feedback on sample texts and videos, and to obtain content for the text messages.
Thematic analysis
Data were analysed using a thematic analysis following the six-stage framework proposed by Braun and Clarke. 27 Investigators EO, DC, and SK familiarised themselves with the transcripts and then independently generated codes from the data using an inductive approach. All three investigators then collaboratively analysed the data to develop a deeper and more nuanced understanding of the content. This step was used to ensure a comprehensive interpretation of the data and enhance the validity of our analysis. Investigators then collaboratively combined and clustered codes to form themes and sub-themes. The themes were defined and named and presented with quotes abstracted from the focus group discussions. The quotes were then shared with study participants to obtain feedback and ensure that participants did not feel they were identifiable and that the quotes were interpreted correctly. Any feedback received was used to edit and refine the quotes.
Development of text message content
An initial collection of twenty text messages, focused on oral hygiene as well as oral and general health content, were developed by oral health clinicians LC and SK, based on identified themes and specific focus group recommendations. Messages relating to diet, and alcohol intake were developed by student dietitians AP and AC, under the supervision of AAG who is an accredited, practicing dietician. All the messages were interpreted in the context of established behaviour change techniques (BCTs) which are defined as observable, replicable, and irreducible components of an intervention designed to alter or redirect causal processes that regulate behaviours. 28 The messages were mapped to 11 specific techniques BCTs including the provision of information on consequences, encouragement, instruction, and the health link; prompting about intention formation, and barrier identification; monitoring self-behaviour, advice about setting graded tasks, strategies aimed at preventing relapse, teaching to use prompts or cues and time management. 29 The initial bank of 20 messages was then expanded to include messages representative of all 11 BCTs. The final bank of messages was sequenced to ensure gradual improvement in oral hygiene skills, and oral health knowledge including diet, as well as addressing misconceptions and attitudes about oral health with the goal of empowering individuals to better self-manage their oral health. The length of each message was limited to 150 characters and each message was assessed for ease of reading using the Sydney Health Literacy Lab (SHeLL) editor 30 which is an automated tool that facilitates the implementation of health literacy guidelines to ensure health information is easy to read and understand. The messages were positively framed, emojis were used and links to instructional videos developed by the research team were provided as appropriate (Figure 1). Customisation of the resource will be possible by asking participants to complete a brief survey prior to delivery (e.g. according to dietary preferences, oral health habits, or health status such as diabetes).

A sample of text messages including the introductory message.
Review of the final text message bank
The final text message bank was reviewed by the multidisciplinary study team (n = 6) using an online survey hosted on RedCap. Messages were rated on a scale of 1–10, where 1 indicated a poor-quality message and 10 indicated a high-quality message. Additionally, textboxes were provided for open comments for each topic area. Of the 81 messages, eight messages received a score of 6 or less, these messages were revised, and any additional open comments were used to refine content for other messages.
Results
The initial survey and focus groups included 15 people, eight clinicians, and seven consumers. The average age of clinicians was 48 ± 10 years, 75% female, and included a multidisciplinary team with the following professional backgrounds, dental practice, oral health therapy, dietetics, cardiac nursing, and dental nursing. All eight clinicians participated in the focus group discussion held at Westmead. The average age for consumers was 62 ± 11.6 years and 43% female. A total of 10 consumers completed the initial survey, four of whom participated in the focus group discussion held at Westmead. Of these four participants, three were born overseas and one was Australian born. The focus group held at Orange was attended by three participants, all of whom were Australian born. A further three participants did not attend the focus group discussions and were not contactable.
Themes
The major themes identified from the qualitative analysis will be presented in turn for clinicians and consumers (Table 1).
Major themes and subthemes for text message content.
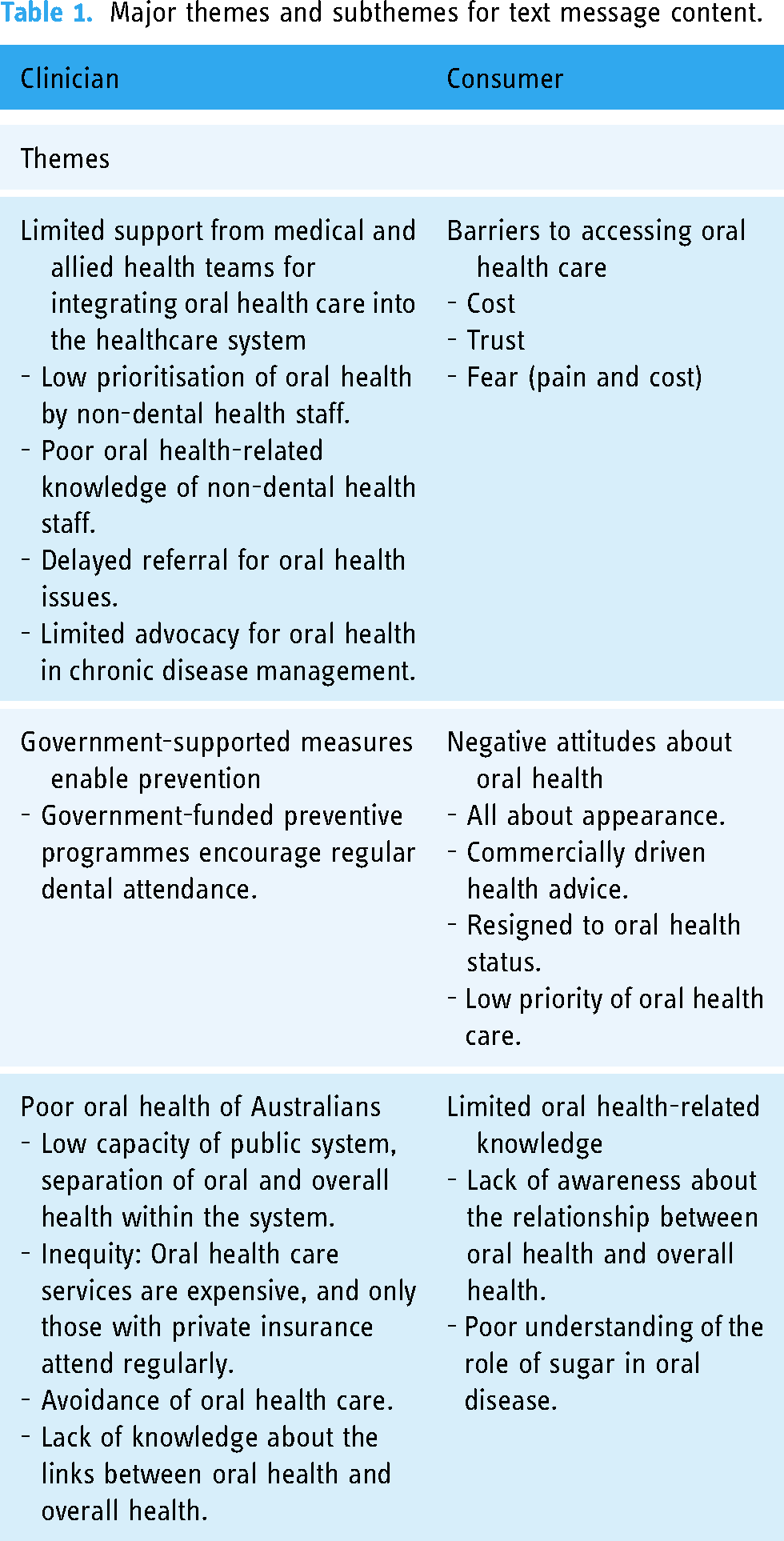
The themes identified from the clinician focus group discussions were (1) limited support from medical and allied health teams for integrating oral health care into the health care system, (2) government-supported measures that enable prevention, and (3) poor oral health of Australians. Each of the themes expanded into sub-themes as presented in Table 1.
Limited support from medical and allied health teams for integrating oral health care into the health care system.
Oral health clinicians reported a lack of support from allied and medical health for the integration of oral health care into the overall healthcare system which was reflected in low prioritisation and late referrals for oral health care (Textbox 1, quote 1). Poor oral health-related knowledge amongst non-dental clinicians was noted by the dietician as leading to a lack of consideration of oral health in management plans (Textbox 1, quote 2). Finally, the lack of advocacy regarding the links between oral and overall health was another factor noted by the oral health clinicians.
Clinician themes and quotes.

Government-supported measures enable prevention.
Specific government-funded programmes such as the child dental benefits scheme were identified by clinicians as measures that encouraged accessibility to prevention by encouraging parents to bring their children to their existing dental clinical appointments (Textbox 1, quote 4).
Poor oral health of Australians.
System-level issues such as poor capacity of the public oral health system and the separation of oral health from overall health within the health system were identified as key drivers of poor oral health, by an oral health clinician (Textbox 1, quote 5). A dental nurse noted the inequity of the system (Textbox 1, quote 6) and additional individual-level issues related to the avoidance of dental care due to both the cost of care and the fear of dental treatment (Textbox 1, quote 7). Finally, a cardiac nurse identified the lack of knowledge about the relationship between oral health and overall health as another contributor to the poor oral health of Australians (Textbox 1, quote 8).
The major themes identified from the consumer focus groups included (1) barriers to accessing oral health care, (2) negative attitudes about oral health, and (3) limited oral health-related knowledge. These themes were expanded into sub-themes as outlined.
Barriers to accessing oral health care.
The main barrier to accessing care was cost. For this reason, one participant reported that they went overseas to access care (Textbox 2, quote 1). Another participant reported a lack of trust in oral health professionals (Textbox 2, quote 2). Finally, several participants reported that fear of dental treatment and also fear of the cost of treatment were major factors that limited access to oral health care (Textbox 2, quote 3).
Consumer themes and quotes.

Negative attitudes about oral health.
There was a general sense that oral health care was about appearance and that oral health information was often commercially driven (Textbox 2, quotes 4 and 5). Moreover, there was a sense of resignation about their own poor oral health status and a feeling that we should therefore focus on opportunities for the next generation (Textbox 2, quote 6). Another aspect noted by a participant was the low priority of oral health in relation to other household costs (Textbox 2, quote 7).
Limited oral health-related knowledge.
A participant from the cardiac rehabilitation programme felt that there was a general lack of awareness about the relationship between oral health and overall health (Textbox 2, quote 8). Similarly, the understanding about the role of sugar in oral disease was also thought to be superficial (Textbox 2, quote 9).
The digital oral health resource (TOOTH)
The final TOOTH resource consists of 81 text-messages, and five videos. The text-messages include one introductory message, and 80 messages categorised by the following topics, diet, tooth brushing, dentures, general oral health, interdental, bacteria, diabetes, and CVD (Supplemental Material). The videos support key concepts including, tooth brushing using manual or electric toothbrushes, cleaning between the teeth using floss or interdental brushes, advice on modifying toothbrush grip, and explanations on how to position the toothbrush correctly.
Discussion
This study used a consultative process involving consumers and a multi-disciplinary panel of healthcare professionals to inform the development of oral health-related text message content. It is the first study to create co-designed oral health messages for adults, mapped to BCTs and sequenced into a digital oral health education resource (TOOTH).
Clinicians raised several systemic issues, including the need for improved oral health training for non-dental healthcare staff, the creation of referral pathways between dental and non-dental services, government-funded preventive programs, and addressing inequities in access to public oral health care. These issues are not new and have been echoed in a global call to action to address the high global burden of oral disease. 31 Although these concerns did not directly inform text message content, clinicians did make several recommendations including the need to prioritise gum disease as it was generally asymptomatic but highly prevalent. They also suggested keeping messages short, friendly, and positively framed. Importantly, they advised against focusing on the smile and instead suggested that the messages highlight the links between oral and overall health.
Consumers also identified systemic barriers such as the cost of private dental care and issues related to fear and a lack of trust in oral health providers and their advice. In terms of recommendations for text message content, consumers wanted to understand why good oral health was important, and advised that messages should be simple, friendly, and include visual content. Interestingly, despite recent interactions with the healthcare system (for oral or cardiac health), there was limited awareness of the connection between oral and general health. For example, although one participant mentioned headaches as a consequence of oral disease, none linked oral health with heart disease or diabetes. Likewise, although periodontitis affects about one in two people worldwide 32 consumers did not mention periodontitis (gum disease) at all, indicating minimal awareness within the community and highlighting the need for increased public education about the links between oral health and cardiometabolic diseases.
This limited awareness and knowledge help explain the low prioritisation of oral health reported by a number of consumers, aligning with a previous study that showed poor oral health literacy in a Western Sydney population. 11 Both the clinicians and the consumers recommended that the oral health messages should clearly explain the association between oral health and overall health. Clinicians specifically advised that the messaging should not focus on the aesthetics, such as having a nice smile, highlighting a consumer's concern that oral health care often seemed to centre on appearance. Messages that explain the link between oral and overall health could motivate adults with co-morbidities to better prioritise oral health care and improve their general health.
Behaviour change theory 29 has been used to underpin the design of the message content, which is expected to increase the likelihood of promoting better oral health behaviours. Oral diseases share common social determinants of health including economic, political and environmental factors and also common key modifiable risk factors for chronic disease including alcohol, tobacco and sugar consumption. 33 Although digital health education programmes for CVD, 34 T2DM, 35 and oral health17–19 have shown individual benefits, integrating these programmes based on the common risk factor approach could enhance non-communicable disease prevention efforts. The messages developed in this study could be adapted and incorporated into existing heart disease and diabetes prevention programmes.
A key strength of this study is that it is the first to develop a codesigned text message programme involving both consumers and clinicians. The programme focuses on broader health behaviours impacting oral health thereby highlighting the link between oral and overall health. Importantly, this study provides a detailed account of the development process for adult-oriented oral health-related text messages. A limitation of the study is that while the final messages have been reviewed by the multi-disciplinary team, they have not been pilot-tested with consumers and are currently only available in English. Furthermore, a large proportion of participants for the Western Sydney focus group (75%) were born overseas and whilst this suggests that diverse views have been included in the content development process it may also mean that the messaging needs to be customised to suit different demographic profiles. Future studies are therefore needed to validate this resource in different population groups including culturally and linguistically diverse populations, and in different age groups to identify the most impactful messages for each of these populations.
Conclusion
This study outlined the process of developing content for an oral health-related text-message-based digital resource for adults by engaging both consumers and clinicians. Our study identified key oral health issues affecting adults, and developed messages based on behaviour change theory. This resource could be integrated into broader non-communicable disease management to promote oral health care as part of chronic disease care plans however, the effect on oral health awareness and knowledge needs to be evaluated in a randomised controlled trial.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076241311730 - Supplemental material for Developing a codesigned text message-based digital oral health education resource (TOOTH)
Supplemental material, sj-pdf-1-dhj-10.1177_20552076241311730 for Developing a codesigned text message-based digital oral health education resource (TOOTH) by Shalinie King, Lauren Adriel Church, Edel O’Hagan, Dion Candelaria, Aboli Pawar, Ashley Cooper, Rebecca Chen and Alice Gibson in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076241311730 - Supplemental material for Developing a codesigned text message-based digital oral health education resource (TOOTH)
Supplemental material, sj-pdf-2-dhj-10.1177_20552076241311730 for Developing a codesigned text message-based digital oral health education resource (TOOTH) by Shalinie King, Lauren Adriel Church, Edel O’Hagan, Dion Candelaria, Aboli Pawar, Ashley Cooper, Rebecca Chen and Alice Gibson in DIGITAL HEALTH
Supplemental Material
sj-pdf-3-dhj-10.1177_20552076241311730 - Supplemental material for Developing a codesigned text message-based digital oral health education resource (TOOTH)
Supplemental material, sj-pdf-3-dhj-10.1177_20552076241311730 for Developing a codesigned text message-based digital oral health education resource (TOOTH) by Shalinie King, Lauren Adriel Church, Edel O’Hagan, Dion Candelaria, Aboli Pawar, Ashley Cooper, Rebecca Chen and Alice Gibson in DIGITAL HEALTH
Supplemental Material
sj-pdf-4-dhj-10.1177_20552076241311730 - Supplemental material for Developing a codesigned text message-based digital oral health education resource (TOOTH)
Supplemental material, sj-pdf-4-dhj-10.1177_20552076241311730 for Developing a codesigned text message-based digital oral health education resource (TOOTH) by Shalinie King, Lauren Adriel Church, Edel O’Hagan, Dion Candelaria, Aboli Pawar, Ashley Cooper, Rebecca Chen and Alice Gibson in DIGITAL HEALTH
Supplemental Material
sj-pdf-5-dhj-10.1177_20552076241311730 - Supplemental material for Developing a codesigned text message-based digital oral health education resource (TOOTH)
Supplemental material, sj-pdf-5-dhj-10.1177_20552076241311730 for Developing a codesigned text message-based digital oral health education resource (TOOTH) by Shalinie King, Lauren Adriel Church, Edel O’Hagan, Dion Candelaria, Aboli Pawar, Ashley Cooper, Rebecca Chen and Alice Gibson in DIGITAL HEALTH
Supplemental Material
sj-docx-6-dhj-10.1177_20552076241311730 - Supplemental material for Developing a codesigned text message-based digital oral health education resource (TOOTH)
Supplemental material, sj-docx-6-dhj-10.1177_20552076241311730 for Developing a codesigned text message-based digital oral health education resource (TOOTH) by Shalinie King, Lauren Adriel Church, Edel O’Hagan, Dion Candelaria, Aboli Pawar, Ashley Cooper, Rebecca Chen and Alice Gibson in DIGITAL HEALTH
Supplemental Material
sj-xlsx-7-dhj-10.1177_20552076241311730 - Supplemental material for Developing a codesigned text message-based digital oral health education resource (TOOTH)
Supplemental material, sj-xlsx-7-dhj-10.1177_20552076241311730 for Developing a codesigned text message-based digital oral health education resource (TOOTH) by Shalinie King, Lauren Adriel Church, Edel O’Hagan, Dion Candelaria, Aboli Pawar, Ashley Cooper, Rebecca Chen and Alice Gibson in DIGITAL HEALTH
Supplemental Material
sj-docx-8-dhj-10.1177_20552076241311730 - Supplemental material for Developing a codesigned text message-based digital oral health education resource (TOOTH)
Supplemental material, sj-docx-8-dhj-10.1177_20552076241311730 for Developing a codesigned text message-based digital oral health education resource (TOOTH) by Shalinie King, Lauren Adriel Church, Edel O’Hagan, Dion Candelaria, Aboli Pawar, Ashley Cooper, Rebecca Chen and Alice Gibson in DIGITAL HEALTH
Footnotes
Acknowledgements
Dr Carina Baptiston-Tanaka and Dr Smitha Sukumar for their operational support for the study.
Contributorship
In accordance with the guidelines provided by the International Committee of Medical Journal Editors (ICMJE), we hereby declare the contributions of each author to the article: SK: study design; SK, EO, LC, AAP, AC, and AG: study conduct; SK, EO, and DC: data analysis; SK: drafting of the article; and AAG, RC, EO, and DC: review and final approval of the article.
Data availability
The data underlying this article will be share on reasonable request to the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Western Sydney Local Health District Human Research Ethics Committee (protocol number: 2023/ETH01673). All participants provided written informed consent prior to any data collection. All methods were performed in accordance with the relevant guidelines and regulations.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a research grant from the Charles Perkins Centre, The University of Sydney.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.