
Abstract
Objective
Individuals who have experienced traumatic events often encounter a variety of changes in their lives and and may suffer from them. To help and alleviate these traumatic stress, we developed an evidence-based mobile application (app) for easy accessibility. This study aimed to test the effects of the mobile app for traumatic stress management using neurofeedback-based meditation and binaural beat music.
Method
Fifty-eight participants were enrolled in a pilot randomized controlled trial (Trial Registration Number: KCT007724) consisting of two groups: (a) experimental group (n = 28) and (b) control group (n = 30). Participants used the mobile app 3 days a week at home for 4 weeks, engaging in neurofeedback-based meditation and binaural beat music. Participants completed self-report measures (SCL-47-R, Psychological Well-Being Post-traumatic Changes questionnaire) and EEG test (emotional stability, anti-stress) at a pretreatment and 1-month follow-up.
Results
Participants in the experimental group demonstrated significant improvements in psychological well-being (F = 16.37, p < 0.001), emotional stability (F = 10.38; p = 0.002), and the anti-stress index (F = 11.37; p = 0.001).
Conclusion
The results of this pilot trial, involving a neurofeedback-based meditation and binaural beat-centered music intervention, provide preliminary support and a readily accessible option for individuals seeking to recover from the effects of traumatic events. Additionally, we have established the groundwork for subsequent research to study the efficacy of a neurofeedback-based meditation program and a binaural beat-centered music intervention for those who have experienced traumatic events.
Introduction
Post-traumatic stress disorder (PTSD) is a psychiatric disorder that can develop in individuals who have experienced or witnessed traumatic events, and it may significantly impact an individual's mental, physical, social, and spiritual well-being. 1 Experiencing traumatic events is a common occurrence worldwide and can have serious negative psychological effects on a large proportion of people, if not the majority. 2 The lifetime prevalence of PTSD among respondents exposed to trauma is 5.6%, with rates ranging from 0.5% to 14.5% across different countries. 3 The prevalence of traumatic stress symptoms may vary across countries; however, it has been confirmed to be higher in developed countries than in less developed regions. 4 The onset of symptoms commonly occurs immediately following a traumatic event, regardless of socioeconomic status. 3
Nevertheless, previous studies have indicated that the average delay in PTSD treatment has ranged from 3 to 30 years. 5 Additionally, although PTSD causes pain in various ways, many individuals with PTSD do not actively seek or receive treatment until they have experienced symptoms for an extended period. 6 While experiencing symptoms of PTSD, individuals may face delayed recovery owing to increasing social isolation, which can lead to greater depression and reduced well-being. 7
Over the previous few decades, there has been ongoing debate regarding effective strategies to support trauma survivors and prevent severe and prolonged PTSD. 8 General PTSD psychotherapy programs that involve exposure to traumatic memories have limitations due to high dropout rates, attributed to the extended duration and stringent structure of the therapy. 9 Additionally, existing psychopharmacological treatments do not entirely prevent the progression of the disease but rather alleviate specific symptoms. Moreover, limitations such as excessive side effects, limited efficacy, and low patient compliance can improve complex causes. 10 These therapeutic limitations highlight the rationale for further research on PTSD and the exploration of new treatment approaches. 11
Previous researchers have suggested that the first step in the basic stages of trauma recovery involves establishing stabilization. 12 Therefore, the most suitable topic for a self-management intervention for individuals exposed to traumatic events would be a method that enables self-stabilization. Self-regulation helps trauma survivors in their recovery by enabling them to control and manage their emotions and behaviors, engage in adaptive processes, utilize resources effectively, and prevent self-determination violations that can lead to persistent psychopathology such as PTSD. 13 Therefore, individuals who have experienced traumatic stress require a means of self-regulation and self-monitoring of their condition to progress in their recovery at their own pace.
Furthermore, recent research has indicated that treatment for PTSD can be effective without directly processing traumatic memories. Various methods, including Internet-based cognitive therapy with psychoeducation, 14 mindfulness-based therapies, 15 and behavioral therapy interventions such as psychoeducation, breathing exercises, and relaxation training, 16 have shown promise. Additional techniques, like neurofeedback and music interventions,17,18 are effective in reducing PTSD-related symptoms. These findings suggest that both trauma exposure-based and nonexposure-based treatments can potentially alleviate PTSD symptoms. 19 Moreover, for those with PTSD to achieve long-term recovery, comprehensive interventions that enhance well-being are necessary, not merely those that focus on symptomatic relief. Such approaches aim to prevent relapse, address residual PTSD symptoms, and foster complete recovery. 20 Enhancing the well-being of individuals with PTSD is crucial, as it significantly influences treatment outcomes and overall quality of life. 21 Researchers also suggested that considering the symptom severity of PTSD and well-being when evaluating treatment response in PTSD individuals is crucial. 22 Focusing on well-being enhances treatment effectiveness and plays an important role in improving patients’ psychosocial functioning and quality of life. Furthermore, this approach has the potential to yield benefits by strengthening positive psychological factors in PTSD management. 23 In particular, mindfulness has been studied as a method to enhance the symptoms and psychological well-being of individuals with PTSD, especially when provided alongside various trauma treatments.24–26
Previous studies have demonstrated that the psychological symptoms of patients with PTSD can be improved, and neurophysiological changes can be induced by meditative interventions that affect EEG activity. As such, the neurophysiological changes associated with meditation have recently attracted scientific attention. Meditation has been demonstrated to regulate emotions by facilitating the integration of experiences through nonjudgmental concentration training, increasing positive emotions, and reducing negative emotions. 27
Neurofeedback, utilizing brain wave activity, is a technology that promotes the body's homeostasis. Positive brain wave patterns are generated through individuals’ willingness to improve their cognitive abilities and achieve a state where the body can independently regulate tension, anxiety, and excitement levels. Neurofeedback enhances the ability to regulate brain homeostasis while measuring one's brain waves. This enables individuals to create an optimal brain state through personalized efforts and training without the use of medication. 28 Neurofeedback is a noninvasive intervention that can be used continuously, regardless of time and location. It is also simple and effective and has no side effects.
Another therapeutic intervention involving brain waves is the use of binaural beat music, which has recently gained attention. Binaural beat music promotes psychological stability and reportedly alleviates pain, anxiety, and depression.29,30 This form of acoustic psychotherapy influences brain waves by delivering two different-frequency sounds to the left and right ears as auditory stimuli, which are then transmitted to the brainstem nuclei. 31 A study applying binaural beats to reduce anxiety and pain in psychiatric patients found that it effectively decreased anxiety levels. 32 Another study examining the impact of binaural beats on stress relief confirmed that the group listening to binaural beats exhibited reduced stress responses to acute psychological stressors compared to the control group. 33
The recent proliferation and widespread use of smartphones have spurred research into mental health management using mobile apps, including for the assessment and treatment of mental health issues.34–36 Through mobile mental health management apps, individuals can access medical information, receive exercise management and diet guidance, monitor biometric data, and manage their health daily at minimal cost and without constraints of time or location.36,37 However, studies demonstrating the effectiveness of mobile programs for traumatic stress management using brainwave interventions are still lacking, highlighting the need for further research in this area.
Based on this identified gap, our study aimed to facilitate the psychological recovery of individuals experiencing traumatic stress and support their reintegration into daily life by investigating the effects of a traumatic stress management mobile app utilizing neurofeedback-based meditation and binaural beat music. We verified the effectiveness of the developed app and formulated the following hypotheses regarding the statistical comparison of average values between the experimental and control groups:
Methods
Study design
This study was a pilot randomized controlled trial (RCT) aimed at evaluating the effectiveness of a mobile traumatic stress management app utilizing neurofeedback and binaural beat music for individuals who have experienced trauma.
Participants
The sample size of the study was calculated as 52 participants using G*power 3.1 program at a significance level of .05, power of .80, and effect size of .80. Participants included adults aged 18–45 years who reported experiencing trauma and stress. This age range was selected because brain wave background frequencies vary by age, and frequencies are consistent among individuals aged 15–45 years, which minimizes variations in measuring research effectiveness. Recruitment was continued based on the inclusion and exclusion criteria until 60 participants were included, taking into account dropout.
Inclusion criteria
Adults aged 18–45 years.
Individuals with moderate or higher severity (≥ 11 points) based on the PDS.
Experienced a traumatic event > 6 months prior to recruitment. Willing voluntary participation after receiving an explanation of the purpose and process of the clinical trial. Ability to use mobile phone applications without difficulty.
Exclusion criteria
Severe mental illness, recent or past delusions, or hallucinations.
Serious diseases affecting the central nervous system.
Participation in other clinical studies within the last month.
Participants were determined by the principal investigator to have significant difficulty in performing or understanding the clinical trial.
Randomization, allocation concealment, and blinding
An independent researcher generated a randomization table using a stratified randomization method in Excel. An independent researcher classified the participants into experimental and control groups based on the selection criteria, including age and willingness to participate among the general characteristics of the participants. Through this, we handled the classification to minimize any possible impact on the research outcomes, and the researcher responsible for the classification did not participate in the result analysis. Initially, 78 individuals expressed interest in the study; however, 14 did not meet inclusion criteria, and 4 declined consents after receiving study information. Thirty individuals were assigned to the experimental group, and 30 were assigned to the control group according to the allocation process, and the research was carried out. Twenty-eight individuals in the experimental group and 30 in the control group participated in the study. Two participants in the experimental group were excluded from the study because they were unable to regularly participate in the experimental intervention owing to personal scheduling conflicts (Figure 1).

Consort flow diagram.
Intervention
Experimental group
Participants in the experimental group received training to use the Mind Therapy app (Choi et al., 2023). 38 Figure 2 illustrates the Mind Therapy app. The app consists of (1) Information of Mind Therapy (trauma stress management information); (2) EEG/Stress Test; (3) Autonomic Nervous System Therapy (deep breathing/butter fly hug); (4) Brain Therapy (neurofeedback meditation/binaural beat music); and (5) Brain Games. In the figure, it is connected via Bluetooth to a two-channel EEG headset, employing neurofeedback meditation and binaural beat music available on the Google Play Store. 38

The Mind Therapy app using neurofeedback and binaural beat.
The intervention was conducted at home for 3 days or more per week for 4 weeks. Each training session lasted at least 50 min and consisted of neurofeedback-based meditation (30 min) and binaural beat music (20 min). During training, when participants focused on meditation and their alpha waves increased, a bell sounded to indicate heightened focus. The frequency of these bells corresponded to increases in alpha waves, signifying improved meditation focus. Experienced researchers, certified as brain counselors and involved in app development and EEG training, provided instructions on using the EEG device and app. Participants downloaded and utilized the “Mind Therapy” app on their smartphones, with experimental group log data accessible to researchers through Google Sheets, and the experiment was conducted. The log data, containing each participant's phone contact information (excluding personal identifiers), recorded connection dates, usage durations, and brain wave measurement results in a chronological order. This allowed researchers to verify participation and identify any missed sessions. Participants who did not engage in the experiment were reminded via phone calls or text messages to complete their assigned tasks.
The control group
Participants in the control group received a handout on traumatic stress management immediately following the pre-test and were scheduled for the post-test 4 weeks later. The handout contents included information on “healthy brain and brain waves,” “activities for a healthy brain,” and “traumatic stress management.” After completing the post-test, participants were wait-listed for treatment if desired.
Data collection
Data were collected between May 23, 2022, and February 28, 2023, using self-report questionnaires and EEG tests by the pre- and post-tests at Seoul Metropolitan area in Korea. Specific details regarding the measurement items and methods are outlined in the Measurements section.
Measurements
Post-traumatic diagnostic scale
The PDS was utilized to assess post-traumatic stress levels among participants. This scale was developed by Foa et al. 39 and standardized in Korean. 40 The PDS comprises 17 items rated on a 4-point Likert scale (0–3), addressing re-experiencing, avoidance, emotional numbness, and hyperarousal symptoms. Total scores range from 0 to 51 points, with three cutoff sections: (a) mild (under 10), (b) moderate (11 to 20), and (c) severe (over 20, the cutoff point for clinical diagnosis in Korea). Participants in this study were required to have a total score of ≥11 for inclusion criteria. The PDS encompasses all PTSD diagnostic criteria from the DSM-5 and is applicable to both male and female samples. Sample items include “If possible, I try to avoid activities, people, or places that remind me of the event,” “I have nightmares about that incident,” and “I feel distant or disconnected from the people around me.” Cronbach's alpha values for internal consistency have been reported between 0.90 and 0.94 in previous studies,40,41 and it was found to be 0.84 in this study.
Symptom Checklist-47-R
The Symptom Checklist-47-R (SCL-47-R) was employed to assess participants’ mental health status across various sub-categories, including depression, somatization, phobic anxiety, interpersonal sensitivity, anxiety, paranoia, obsessive–compulsive behavior, hostility, and psychoticism. Originally developed by Derogatis, 42 the SCL-47-R was translated and adapted into a concise Korean version.43,44 The SCL-47-R comprises 47 items rated on a 5-point Likert scale, with total scores ranging from 47 to 235 points. Sample items include “I feel nervous and anxious,” “I feel depressed,” and “I keep thinking useless thoughts.” Higher scores on the SCL-47-R indicate poorer mental health status across the assessed domains. The instrument has demonstrated high internal consistency, with Cronbach's α values ranging from 0.97 to 0.98 (Gwon & Park, 2016; Hyun & Cho, 2012).45,46
PWB-PTCQ
The PWB-PTCQ was utilized to measure participants’ psychological well-being. Developed by Joseph et al. 47 and translated into Korean, 48 this tool assesses two factors: (1) changes in outlook on life and interpersonal relationships (e.g. “I am a compassionate and giving person,” “I am grateful to have people in my life who care for me”) and (2) changes in oneself and the world (e.g. “I handle my responsibilities in life well,” “I have a sense of purpose in life”). The questionnaire consists of 16 items rated on a 5-point Likert scale. Total scores range from 16 to 80 points, with higher scores indicating better psychological well-being. The Cronbach's α coefficient for internal consistency ranges from .92 to .94,48,49 demonstrating the reliability of this instrument in assessing psychological well-being post-trauma.
EEG results: emotional stability and anti-stress index
The effects of the intervention on participants’ emotional stability and anti-stress index were assessed using the Neuroharmony program, which is approved by the Food and Drug Administration and measured by a two-channel EEG check device. Emotional stability was analyzed using the emotional quotient (EQ), which assesses the symmetry of alpha waves between the left and right sides of the brain. A higher EQ indicates more active emotional stability, while a lower EQ suggests darker or more depressed emotional stability. Generally, an EQ of 80 or higher is considered optimal; a range of 60–80 is considered active, 40–60 is considered normal, 20–40 is considered inactive, and ≤ 20 is considered extremely low. The anti-stress index measures stress resistance through the analysis of delta and high beta waves. A higher anti-stress index value indicates better resistance to stress-related conditions. Traumatic stress can hyper-arouse the right frontal lobe (the fear center of the brain) and increase high beta waves. This also affects the left brain, increasing high beta waves in the left brain and breaking the balance between the left and right brain. 50 Generally, a value of ≥80 is considered optimal, 60–80 is healthy, 40–60 is normal, 20–40 indicates fatigue, and <20 is considered pathological.51,52
Data analysis
The collected data were analyzed using SPSS version 25. Descriptive statistics were used to analyze participants’ general characteristics. Participant homogeneity was assessed using chi-square tests. Finally, differences between the experimental and control groups were analyzed using ANOVA.
Ethical considerations
This study was conducted with the approval of the Institutional Review Board at a university in Seoul, South Korea (No. 1041078-20230331-HR- 081). Following an explanation of the study's purpose and methodology, participants were provided with a consent form to read and sign. The researchers clarified that participants had the option to withdraw from the study at any time without facing adverse consequences. Additionally, participants were assured that their personal information would be used solely for research purposes and would be discarded upon completion of the study.
Results
Regarding the participant demographics, there were 8 men (13.8%) and 50 women (86.2%) in the study. In terms of age distribution, 25 participants were in their 20s (43.1%), 21 in their 30s (36.2%), and 12 in their 40s (20.7%). Analysis of homogeneity between the experimental and control groups revealed no significant differences in sex, age, education level, or occupation (Table 1).
General characteristics and homogeneity of participants.
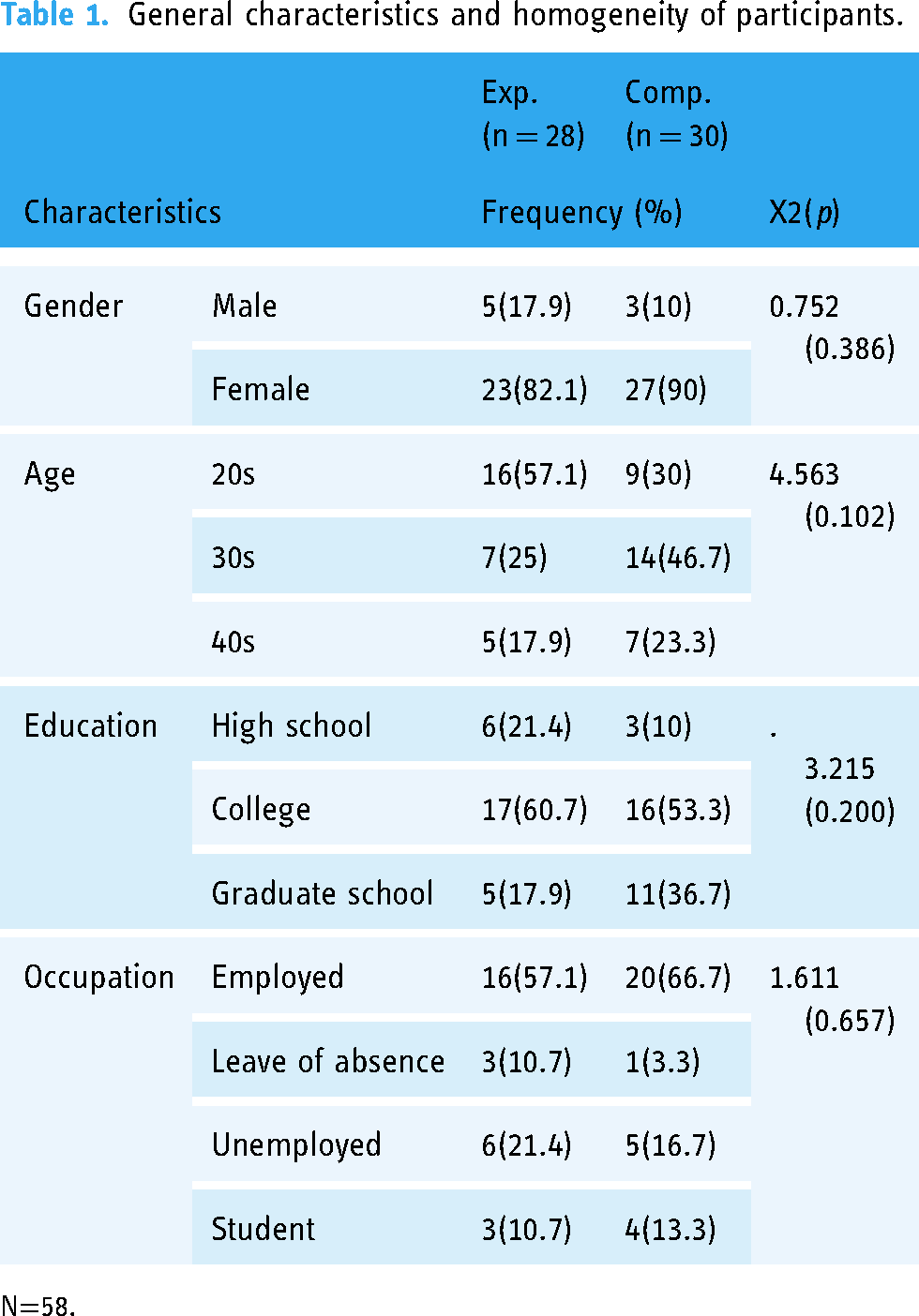
N=58.
The study outcomes indicated that Hypothesis 1 was not supported, whereas Hypotheses 2 and 3 were supported, with Hypothesis 4 partially supported (Table 2). The specifics are outlined below:
Effects of the program.

N = 58.
*p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
This study was conducted to evaluate the effectiveness of a developed traumatic stress management program utilizing neurofeedback-based meditation and binaural beat-centered music intervention and to propose an effective research design for future follow-up studies.
In this study, the effects of meditation align with findings from a RCT, 53 which demonstrated that participants experienced improvements in stress and well-being following a mobile meditation intervention. Previous research has indicated that meditation can effectively address various mental health challenges, such as PTSD, anxiety, and depression, 54 and is an activity that increases alpha waves. 55 The meditation provided in this study focused on improving alpha waves using neurofeedback technology, providing an environment that allows users to become more immersed in meditation activities. Therefore, it can be assumed that the participant's mental health and well-being scale improved as a result of this study. Therefore, providing alpha wave neurofeedback training through meditation, which is an activity that increases alpha wave, is suggested to be an efficient method for people experiencing mental health difficulties. As the number of mobile meditation apps is gradually increasing, studies on their effects and qualitative research on the positive experiences of app users are being reported. 56 In the future, qualitative studies on the experience of using mobile neurofeedback-based meditation apps are required to ensure their continuous quality and alignment with user needs.
The results of this study confirmed significant differences in other evaluation scales, but this was not the case with the PTSD scale (PDS). When reviewing the duration of neurofeedback intervention for PTSD participants from previous research, the measurement interval at which significant changes in PTSD were observed (a) not at 4 weeks and (b) others were taken at 3-month, 6-month, or 8-week intervals. 57 Another study demonstrated a significant reduction in PTSD symptoms after 40 intervention sessions conducted twice a week over 4 months, with improvements in emotional regulation observed beforehand. 58 Furthermore, studies involving the general population, not limited to those with PTSD, have shown sufficient stress reduction effects even within a 4-week research period. 59 These findings from previous studies partly align with the results of this study. In this study, the emotional control and mental health indicators of the participants were improved, including significant enhancement in the mental health status and well-being scale of the experimental group and brain emotional indicators in the EEG test. Due to the limited intervention period of 4 weeks, we speculate that there was no significant difference in the improvement of direct PTSD symptoms, which follows a complex and varied course. Therefore, to directly address PTSD symptoms, it is deemed necessary to conduct follow-up research by applying various “periods” within the intervention conditions.
In this study, to assess the improvement of PTSD-related symptoms, emotional stability was measured by evaluating the left–right balance of alpha waves in the brain. Previous research has indicated that PTSD may be linked to the imbalance of alpha waves between the left and right hemispheres, leading to emotional instability.60–62 Following the 4-week intervention, it was observed that the emotional stability of the experimental group increased. It is assumed that our intervention had a significant impact on the balance of alpha waves between the hemispheres, which may have positively influenced the mental health status scale. These findings are consistent with prior research suggesting that emotional symptoms may improve before the symptoms of PTSD.
Similar to the effect of binaural beat music used with mobile neurofeedback meditation in this study, previous studies have reported reductions in acute psychological stress among intervention groups exposed to binaural beats. 33 A research demonstrated that a single application of binaural beats improved the alpha levels of the right hemisphere—more involved in processing negative emotions—compared to the alpha level of the left hemisphere. 63 However, one study included a meditation group, a binaural beat group, a meditation and binaural beat group, and a control group. The greatest improvement in sleep, stress, depression, anger, and overall mood was reported for the meditation and binaural beat groups. 64 These findings are consistent with the results of our study, which utilized mobile neurofeedback-based meditation and binaural beat music to achieve significant improvements in participants’ mental health status, psychological well-being, emotional stability, and anti-stress index. Therefore, this study is valuable as it offers a convenient program for users by making neurofeedback meditation and binaural beat music available via a mobile app.
Finally, the limitation of this study is the inability to fully control all exogenous variables occurring in participants’ daily lives during the 4-week intervention period, which may affect the generalizability of the research results. Future studies should aim to explore these phenomena among diverse populations to address this limitation. This study used the PDS cut point to select participants with a history of trauma, which may result in a lack of specificity in the population. Therefore, caution is needed when interpreting or generalizing the results of this study. In addition, when selecting participants, the brain measurement was considered to be in a normal state, so it could be difficult to determine the extent of change after intervention. The possibility cannot be ruled out because the EEG test results can be affected by external factors such as individual conditions and measurement time, temperature, sound, etc. The handouts provided to the control group may raise issues due to treatment as usual. In future studies, it is necessary to ensure that more stringent treatment is provided to the control group. In this study, binaural beat-centered music intervention and alpha wave-centered neurofeedback meditation intervention were structurally separate in the application; however, they were combined in parallel during the experiment. The potential mutual effects of these interventions cannot be completely ruled out. Therefore, future research should investigate each intervention separately to understand their individual effects in follow-up studies better.
Despite these limitations, this study holds significant importance. It conducted an RCT on a new smartphone app offering binaural beats and meditation treatment for trauma, laying the foundation for future intervention research targeting individuals with PTSD. The exposure therapy of trauma, which has been the mainstay of PTSD treatment to date, has been highly effective; however, it has a high dropout rate, which has its limitations. The mobile neurofeedback-based meditation intervention developed in this study presents a promising alternative to trauma exposure therapy, aligning with the advantages of neurofeedback interventions suggested in previous research. 50 Furthermore, the mobile neurofeedback-based meditation and binaural beat-centered music intervention program introduced in this study offers user-friendly convenience and can serve as a routine and safe intervention that individuals with PTSD can utilize at their discretion. Discovering cost-effective and time-flexible treatments for PTSD and other mental health disorders is particularly critical given the limitations of existing therapies and the need for continuous care. Our research is meaningful as it contributes to advancing public mental health by providing free development content and conducting the development in consideration of convenience and cost-effectiveness.
Conclusion
The mobile neurofeedback-based meditation and binaural beats-centered music program developed in this study holds promise for effectively managing evidence-based traumatic stress. By prioritizing emotional stability and enhancing individual well-being and mental health status, this program is expected to impact the future recovery of individuals with PTSD positively. It is crucial to undertake ongoing long-term evaluation using systematic research design and long-term effectiveness analysis to assess the program's benefits and outcomes further. This cost-effective and time-efficient treatment intervention can be disseminated widely to individuals, families, and communities experiencing disaster and mental stress in a more accessible way and without side effects. We hope that this program will effectively promote mental health within communities.
Footnotes
Acknowledgements
We would like to thank everyone who agreed and offered to take part in this study.
Contributorship
YC: conceptualization, methodology, writing—original draft. DC: data analysis, project administration, writing—review. NL: data curation.
Consent to participate
Participants provided written informed consent prior to participation.
Data availability
The data of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was conducted with the approval of the Institutional Review Board at a university in Seoul, South Korea (No. 1041078-20230331-HR-081).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Ministry of Science and ICT, Republic of Korea (NRF-2020R1A2B5B0100208 and NRF-2023R1A2C2003043).
Guarantor
Y. Choi.