
Abstract
Objective
Healthcare delivery and research are moving increasingly towards digital engagement, which could inequitably exclude some populations due to differential technology access and uptake. We sought to evaluate study-related digital access, preferences, and use among parents of patients with Medicaid insurance enrolled in research in a pediatric emergency department (ED).
Methods
We conducted a secondary analysis within a randomized trial at an academic pediatric ED. Children with public insurance and a language of English or Spanish who were treated for asthma symptoms were enrolled; parents completed surveys regarding digital access, preferences and demographics. Associations were tested using Fisher's exact test.
Results
We enrolled 80 families, of whom 18% had a language for care of Spanish; 31% of children identified as Hispanic, and 25% as Black. All baseline survey respondents (n = 79) endorsed having an internet-connected computer (73%) or smartphone (99%); 85% of smartphone holders reported unlimited data. When given the choice, 73% of participants requested a physical gift card instead of an electronic gift card. Only 31% had patient portal access 6 months after study end. Parents who spoke Spanish or with a child identified as Hispanic or Black more often requested physical gift cards and less often had patient portal access, but these differences were not statistically significant.
Conclusion
Despite ubiquitous access to internet-connected digital devices among this Medicaid-insured population, patient portal use was low and many families preferred non-digital reimbursement. Efforts to enhance research inclusion should consider digital preferences in addition to digital access when planning study procedures.
Keywords
Introduction
Over the past few decades, the United States (US) has invested heavily and made significant improvements in its health information technology (HIT), including electronic health records (EHR) with embedded decision-support and patient portals, which provide online access for patients and families to view their EHR and communicate with their care team. 1 Expanding HIT presents the potential to expand access to healthcare and improve quality of care while allowing individuals to engage and participate in their own care. These changes in healthcare mirror the rapid expansion of new technology in society, adding momentum to the movement of healthcare access and engagement towards digital spaces. 2
With this increased adoption of technology in healthcare, however, concerns have arisen over the “digital divide,” which refers to differences in technological access and uptake among different individuals in ways that create barriers to accessing services or resources. Populations that have been found to have less access to technology include individuals from minoritized racial and ethnic groups, persons with disabilities, those with lower socio-economic status, and rural populations. 3 Several factors have been reported to contribute to the differential access including poverty, low literacy, structural barriers to accessing computers, smartphones, and broadband internet, and less interest in using available technology.2,4,5 Given that the digital divide affects those who may already be experiencing other types of marginalization, it may further exacerbate existing social and economic disparities for individuals who are unable to access healthcare information. 2 Some of these gaps are narrowing over time, while others persist. 2 With advances in healthcare technology, there is potential for worsening health disparities among structurally marginalized populations.
The movement towards digital engagement is occurring within patient-oriented research as well, with unclear effects on participant enrollment and retention. Knowing that the digital divide exists but may be narrowing, we sought to evaluate study-related digital access, preferences, and use for parents of children with public insurance enrolled in research in a pediatric emergency department (ED).
Methods
This study was a secondary data analysis from a pilot randomized control trial, Recordable Cards for Optimizing Outcomes and Reducing Disparities after ED Discharge (RECORD-ED), conducted at a high-volume freestanding academic pediatric Emergency Department (ED) with 50,000–60,000 patient encounters each year. 6 The RECORD-ED study is registered at clinicaltrials.gov under study ID NCT04676490. In the main study, families were randomly assigned to receive usual care or usual care plus audio-recorded discharge instructions, either on a physical greeting card or via the online patient portal. All participants were encouraged to set up patient portal access, but if assigned to usual care plus patient portal audio-recorded instructions, participants received additional, user-friendly instructions in English or Spanish. In this study we analyze participant survey responses related to digital access and preferences, which were collected at enrollment for the larger study.
Study enrollment
Study enrollment and initial data collection occurred in the ED between 12/15/2020 and 4/30/2022. Research coordinators screened an electronic tracking board of current ED patients to identify those who might be eligible. Patient eligibility criteria, determined by the overall study objectives, included age <10 years, Medicaid or no insurance (to identify a primarily low-income population), language for care of Spanish or English, and being discharged home from the ED following treatment for asthma or wheezing. Parents of potentially eligible patients were informed about the study and all legally authorized representatives of minors provided informed consent prior to study enrollment; a waiver of written documentation of consent was obtained from our IRB given the low-risk nature of the study.
Ethics approval
This study was approved by the Seattle Children's Institutional Review Board; study number 2727.
Data collection and analysis
Data were collected via REDCap and included four surveys, one at enrollment and three follow-up surveys: at 3 days, 7 days, and 3 months post-ED visit. 7 The enrollment survey was self-administered, with help from the research coordinator as needed; follow-up surveys were administered over the phone or self-administered online. The enrollment survey included items related to current access to computers, smartphones, and the internet; preferred methods of contact by the research team; and the choice between digital and physical gift cards. Of note, the choice between payment options began part way through the study due to institutional policies that initially limited incentives but then changed, allowing for multiple incentive options. Detailed demographic data were collected as part of any follow-up survey that was completed, including parent income, education, and health literacy using the Single Item Literacy Screener. 8 We collected administrative data from hospital records, including activation of a MyChart patient portal account by 6 months after the end of the study, and hospital-collected demographic data (race and ethnicity, sex, and language for care). These hospital-collected data were parent-reported and collected during ED registration. Race and ethnicity categories reflected current US Census options. This analysis used data from the enrollment survey, demographic survey, and administrative data.
The analysis was primarily descriptive. Summary statistics were compiled for study participants, including means with standard deviations and percentages. We tested for associations between race and ethnicity and language, as predictors, and gift card preference and portal activation as outcomes, using Fisher's exact text.
Results
Between 12/15/2020 and 4/30/2022, we approached 177 and enrolled 83 (47%) English- or Spanish-speaking parents of children with Medicaid or no insurance being treated for wheezing or asthma in the ED; 3 were subsequently withdrawn following admission to the hospital, leaving a study sample of 80 parent-child dyads (Figure 1). Of those, 79 (99%) completed all digital access questions on the enrollment survey and 54 (68%) completed the detailed demographics survey at follow-up. Over half (49/80, 61%) were given the option of physical or electronic gift cards at enrollment. Hospital-based administrative data was available for all 80 enrolled patients, including patient portal account status 6 months after study end to allow ample time for account activation.
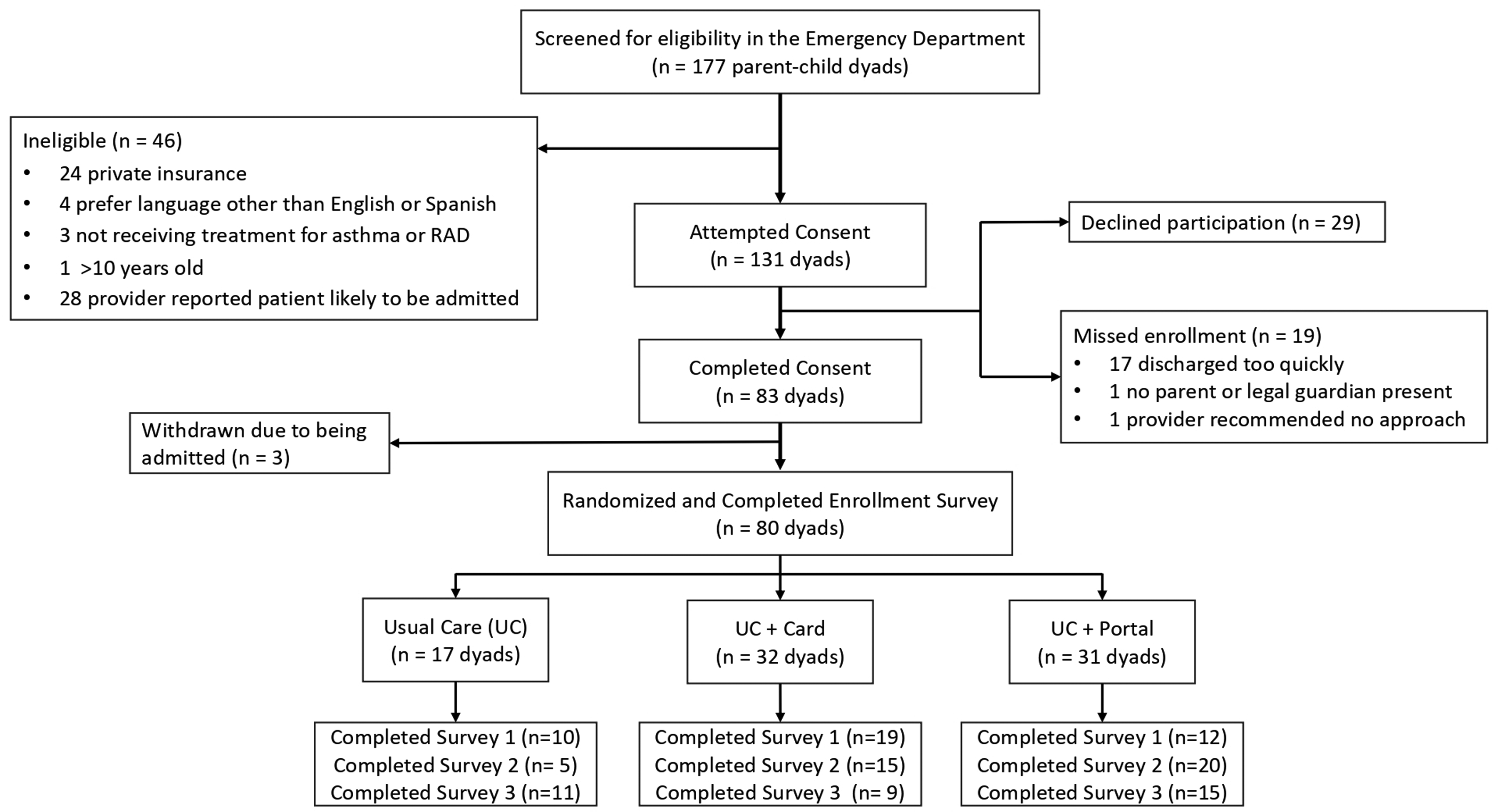
CONSORT diagram of study enrollment and retention.
Enrolled children were 4.8 years old, on average (Table 1), and 65% were male. All had Medicaid insurance (80/80, 100%). Based on hospital-collected data, 25 (31%) were of Hispanic ethnicity with any race, 20 (25%) were non-Hispanic Black, and 12 (15%) were non-Hispanic White (Table 1). Eighteen percent (14/80) had a language for care of Spanish. Participating parents were 34 years old on average, and 91% identified as female. Of the 68% of participants that completed the follow-up demographic survey, 59% (32/54) had completed some college or more; 94% (51/54) had adequate or better health literacy based on the single item literacy screener. 8 Of those providing income data, 65% (17/26) had an annual household income below $40,000.
Participant characteristics.

Results are presented as Mean (SD, (Minimum-Maximum)) for continuous variables, or as n.
/ N (%) for dichotomous variables. Denominators vary for survey questions based on participant non-response.
With regards to digital access and preferences, notably, 100% (79/79) of individuals who responded endorsed access to a computer or smartphone (Table 2). Overall, three quarters (59/79) of individuals had a computer, and all but one had a smartphone (78/79); of the smartphone holders, 85% (66/78) reported unlimited data. Of those with a computer, all (58/58) had internet access. Despite ubiquitous access to technology, when given the choice, 73% (36/49) of participants requested a physical gift card instead of an electronic gift card (Table 2). Regarding digital communication, 32% (25/79) of participants requested follow-up contact via phone call, 23% (18/79) via text and 46% (36/79) via email (Table 2). Lastly, while 65% (51/79) of participants reported previous experience using a patient portal, only 31% (25/80) of patients had an activated MyChart patient portal account 6 months after the end of the study based on administrative records.
Digital access and preference and literacy.

Total enrollment was 80; denominators vary based on survey non-response.
This question was only asked of respondents who indicated that they used a computer at home, yielding a denominator of 58.
While gift card preference and portal activation did not differ significantly by language or race and ethnicity in our small sample (with significance defined as alpha < .05), apparent differences existed (Figure 2). For example, relative to English-speaking parents, parents who used Spanish for care more often requested a physical gift card (100% Spanish vs 68% English, p = 0.09) and less often had an active patient portal (14% Spanish vs 35% English, p = 0.2). Similarly, relative to other parents, parents of children identified as Hispanic or non-Hispanic Black more often requested a physical gift card (Hispanic 73%, non-Hispanic Black 100%, non-Hispanic White 56%, p = 0.2) and less often had an active patient portal (Hispanic 20%, non-Hispanic Black 20%, non-Hispanic White 58%, p = 0.051).

Gift card preference and activated patient portal by Race and Ethnicity.
Discussion
In this survey study of 80 parents of Medicaid-insured children in the pediatric ED, we found that despite universal access to the internet and/or smartphones, a large proportion of study participants still preferred non-digital compensation, with nearly three-quarters of participants choosing a physical gift card versus an e-gift card when given the choice. Additionally, despite 64% of participants reporting previous patient portal experience, at the end of the study period less than a third had patient portal access. Thus, access to technology and the internet does not necessarily increase HIT utilization or translate into preferences for digital engagement. This is important because as healthcare increasingly moves online, choosing methods to engage with patients and research participants that don’t work well for them will exclude patients from access and may create or worsen health care disparities that are already well documented in the literature. 9
Although not statistically significant, perhaps due to this pilot study's small sample size, these findings of non-digital preference and lack of portal access appeared to be more common among parents who use Spanish as their language for care, and among those with a child identified as Hispanic or non-Hispanic Black.
Disparities in access to technology on the basis of race, ethnicity and income are well-described. A recent report on Americans’ access to technology described how individuals who identify as Hispanic or Black were significantly less likely than the national average to own a computer, have Internet access, and access the Internet at home. 9 Another study by the Pew Research Center survey from 2021 reported that Black (69%) and Hispanic (67%) adults in the US remain less likely than White adults (80%) to own a desktop or laptop computer. With regard to income, almost 24% of adults with household incomes below $30,000 a year reported lack of a smartphone, and an estimated four-in-ten adults with lower incomes did not have home broadband services (43%) or a desktop or laptop computer (41%). On the other hand, households earning greater than $100,000 annually had nearly ubiquitous smartphone and tablet ownership. 9
In contrast to this previous research, in our study we found nearly ubiquitous access in our racially and ethnically diverse study population. That is especially notable given our goal to enroll a low-income population, with 65% of those reporting income making <$40,000 per year.
As some previous studies have suggested, access to technology alone may not be enough to overcome barriers to utilizing or preferring electronic technology, and access may not equate with preference. 10 This is of particular relevance as more institutions move to requiring use of trackable electronic gift cards for participant incentive payments, and more study procedures move to online-only options. If the goal among researchers is increasing equity and inclusion to improve representativeness and engagement of participants––which is critical for producing evidence that will apply to everyone and not exacerbate disparities by preferentially improving outcomes for those who were included in the studies—11,12 further attention should be paid to participant preferences while implementing interventions to decrease the digital divide. Failure to consider preference in addition to access may stymie well-intentioned efforts to improve the diversity and representativeness of research participants. Future research should also investigate what other barriers contribute to the limited patient portal uptakes, as this study suggests that technology access and prior experience may not be the primary barriers.
Limitations
This study had limitations. First, we enrolled a smaller sample than planned due to the COVID pandemic causing staffing shortages and abnormally low volumes of ED patients with respiratory illnesses. Additionally, the data were collected at one freestanding academic pediatric ED, so generalization to other hospitals or geographic areas may be limited. Self-reported demographics, including income and education, were available for only 68% of participants, so these results should be interpreted with caution. Finally, this study aimed to enroll a low-income population with limited health literacy; while all patients had Medicaid and many had low income, of those who provided demographic data very few had limited health literacy and education levels were high, suggesting that study participants may not be representative of the wider population of families with low-income.
Conclusion
In this survey study of parents of 80 low-income children in the ED, we found universal access to internet-connected digital devices. However, most participants preferred physical over electronic gift cards and contact via phone calls or texts over email, and less than a third activated a patient portal account, despite many reporting experience with them. Researchers should consider digital preferences in addition to digital access when planning their enrollment and retention procedures in order to improve the racial, ethnic, and socioeconomic diversity of research participants.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241302251 - Supplemental material for Digital divide: Differences between digital access, preference, and use among parents of pediatric research participants
Supplemental material, sj-docx-1-dhj-10.1177_20552076241302251 for Digital divide: Differences between digital access, preference, and use among parents of pediatric research participants by Lauren Smith, Cassandra Koid Jia Shin, Najma Abdi, Chuan Zhou, Julie C. Brown, Emily A. Hartford, Mahtab Danai and K. Casey Lion in DIGITAL HEALTH
Footnotes
Contributorship
Casey Lion, Julie Brown, Emily Hartford, and Mahtab Danai conceived the study. Casey Lion was involved in gaining IRB approval. Chuan Zhou led the statistical analysis. Cassandra Koid Jia Shin, Najma Abdi and Lauren Smith were involved in literature review and background research. Lauren Smith and Cassandra Koid Jia Shin wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Seattle Children's Institutional Review Board.
Funding
This study was funded by The National Institute of Nursing Research grant R21 NR018914 (PI Lion). The use of REDCap for this project was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1 TR002319. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders.
Guarantor
Lauren Smith
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.