
Abstract
Objectives
Technology, mobile health (mHealth), and “eHealth” are broadly used in childhood overweight and obesity interventions. However, the impact of technology-based interventions where parents or caregivers are involved is unclear. Thus, the objective of this manuscript is to provide valuable insights about the development of a parent–child web-based tool to promote healthy eating among preadolescents.
Methods
The tool development was an iterative process and comprised of two phases. In Phase 1, formative research (focus groups and interviews) were conducted with parents of children around the topics of dietary behaviors, technology use, and proposed intervention components. In Phase 2, a brief survey, focus groups, interviews, and user-centered approaches were used to confirm/finalize content, assess the website wireframe, and conduct usability testing.
Results
From the Phase 1 formative research, parents preferred reading/looking up health-related information on larger laptop/tablet screens, but preferred smartphones when reading “on-the-go.” Suggestions for an online health tool included quick/easy/low-cost recipes, tips for healthy feeding and involving their children around healthy dietary-related behaviors, clear tool navigation, and using pictures/visuals. In Phase 2, when finalizing the tool wireframe and content, parents preferred a variety of motivational healthy feeding tips, local family-oriented community events, and a simple layout with minimal clicking to access links. During usability testing, parents responded positively to the content (healthy feeding tips, recipes, coupons, and free community events) and the clean layout.
Conclusions
Formative research and user-centered approaches with parents of preadolescents resulted in a web-based, mobile-friendly health promotion tool.
Introduction
Childhood obesity continues to be a serious public health challenge in the United States (US), particularly among low-income, minority populations—Latino and Black/African-American (AA) children have the highest obesity prevalence at 26.2% and 16.6%, respectively. 1 There are also alarming increases in prevalence between age groups, with prevalence rates highest among preadolescents and adolescents. 2 A strong body of evidence has linked childhood obesity trends to reduced years of life and other short- and long-term health, economic, physical, and psychosocial consequences. 3 Because the role of parenting, parental modeling, parental feeding practices, and the home environment all play important roles in childhood eating behaviors,4–6 effective prevention and treatment strategies are needed.
The use of technology, mobile health (mHealth), and “eHealth” more broadly in childhood overweight and obesity interventions are promising strategies.7–10 They offer an alternative to promoting healthy eating behaviors and have multiple advantages over face-to-face engagement interventions. For example technology-based interventions can be delivered remotely, reduce the need for additional childcare, eliminate the need for travel, and have high completion rates.11,12 Given that Latino and Black/AA parents are more likely to work nontraditional working hours and hold multiple jobs,13,14 technology-based interventions may address the noncompliance and dropout rates that have been reported to range between 50–75% in traditional face-to-face engagement nutrition interventions, particularly those that include low socioeconomic status and racially/ethnically diverse parents. 15 Further, studies using technology-based approaches, emphasizing the role of parents in supporting the initiation and maintenance of children's eating behaviors have reported changes in children's dietary, and/or physical activity outcomes.8,16 Additionally, Kouvari and colleagues conducted a systematic meta-analysis for weight management in children and adolescents. The study found that significance was lost in cases of no parental involvement (standardized mean difference, −0.36, 95% confidence interval [−0.83 to 0.11]; p = 0.14). 17 Hovadick and Cardoso noted that lasting changes in children's eating behaviors require parental involvement. 18 It is worth noting that while technology-based interventions to reduce overweight and obesity are on the rise, they often target adolescents and adults. 19
Therefore, this manuscript outlines the systematic design of a web-based, mobile-friendly parent tool. It involved formative research and the application of user-centered design, which grounds the characteristics of an innovation in information about the individuals who use that innovation, with a goal of maximizing usability in context. 20 Importantly, user-centered design also helps amplify the relevance, usability, and acceptability of the innovation or technology, increasing the likelihood of successful adoption by the intended population.21–24
Framework
In parent-involved childhood obesity interventions, theory-guided content (typically using the ecological framework, social cognitive theory (SCT), or parenting styles constructs) has aimed to increase parent knowledge, skills, and self-efficacy related to healthy eating and physical activity, and also promote parenting skills (e.g., motivation, effective communication, role modeling, child feeding practice).25–29 While a majority of these interventions have demonstrated improvement in child body massindex, few have included a diverse study population or were tailored to low-income or minority populations.28,30
This study is guided by the socioecological model (SEM), SCT, health belief model (HBM), and constructs from theories on parenting styles. The SEM, which describes five levels of influence, is a theoretical framework for understanding the influences of personal and environmental factors, and has been used extensively in childhood obesity research. 31 At the individual and interpersonal levels, parents and the home environment are central to the development of a child's attitudes, beliefs, knowledge and behavior, 32 highlighting the importance of intervening at these levels. The SCT lends explanation to ways in which improved parent behaviors and parent–child communication may influence child health behavior, particularly through role modeling of new behaviors. 33 Specifically, SCT constructs of behavioral capability and reciprocal determinism highlight the potential impact of resources and environmental contexts on parent health-related behaviors, which can in turn influence child health behavior, as well as child outcome expectancies, behavioral capability, and self-efficacy.34–36 The HBM construct of cues to action is important to consider when designing intervention approaches to activate readiness for change and stimulate behavior change. 37 Literature on general parenting styles 38 has identified dimensions of parental support behaviors (motivational, instrumental, and conditional) and their impact on child health-related behaviors such as physical activity, healthy eating, and screen time.39,40 Additional food parenting constructs focused on child dietary behaviors include structure (e.g., subconstructs of modeling, food availability, food accessibility) and autonomy support (e.g., subconstructs of child involvement, encouragement). 41 All in all, the SEM, SCT, HBM, and constructs from theories on parenting styles permit the design of a web-based tool that considers the multifaceted aspect of human behavior. For example, SEM provided the opportunity to customize content to improve health behavior in the home environment. The SCT supports self-regulatory behavior change procedures such as goal setting, self-monitoring, and problem solving through integrating interactive features of the web-tool. Cues to action from HBM can guide the structure and timing of the parent and child weekly messages to stimulate behavior changes.
Methods
Study overview
With an interdisciplinary design team and a partnership with a community-based organization (CBO), development of the parent tool comprised two phases. Of note, development of the parent tool was done in parallel with development of a child tool (an innovative web-based interactive comic tool) aimed at improving healthy eating behaviors to reduce childhood obesity risk among urban minority youth. 42 Together, the parent- and child-focused tools formed Intervention INC, a web-based intervention aimed at improving healthy eating behaviors, feeding behaviors, and the home food environment to reduce childhood obesity risk among urban, minority youth.
Figure 1 provides an overview of the data collection timeline and iterative parent tool development process, engaging both parent participants and the design team (see Interdisciplinary Design Team section in the Results). There were two phases to the development process. During Phase 1, focus groups and interviews were conducted with parents of low-income urban Latino and Black/AA children around the topics of dietary behaviors, technology use, and proposed intervention components. Phase 2 included iterative design activities (content confirmation, codesigning, and usability testing of prototypes) to ultimately produce web-based health newsletters to support healthy parental feeding behaviors and the home food environment. Written informed consent was obtained from all parent participants prior to the start of any study procedures.

Data collection summary and timeline.
Participants
Study participants were recruited from a child-focused CBO, whose mission is to help children in poverty succeed and thrive in high-needs New York City (NYC) neighborhoods. With permission and coordination with the CBO, research team members recruited, screened, and obtained written consent from eligible participants at tabling sessions at three different CBO sites in East Harlem/Upper Manhattan, NYC. CBO site directors also assisted with participant recruitment by making referrals/recommendations of potential participants who: (a) fit eligibility criteria provided to them, (b) were highly engaged within the CBO, and/or (c) could contribute unique perspectives.
Inclusion criteria consisted of a parent: with a child between the ages of 9 and 12 years, self-identifying as Latino and/or Black/AA, being English- or Spanish-speaking, having internet access via smartphone or tablet, and having an interest in talking about food and technology. Parents who participated in Phase 1 or provided written consent to have their child/children participate in a child-only focus group (as part of parallel research to develop the child component; manuscript under review) were invited back to participate in Phase 2. Individuals who did not meet the aforementioned inclusion criteria were excluded from the study.
During Phase 1, parents received a $10 gift card for participating in a one-time study session. During Phase 2, incentives ranged from $10 (participating in tool content confirmation or usability testing study session) to $15 (participating in codesigning study session). All participants also received a round-trip MetroCard ($5.50 value) to cover travel to and from the study site (either a CBO site or the main study site).
Data collection
Phase 1: Formative research
Technology, dietary behaviors, and health promotion
Data collection occurred in July and August 2016 at three CBO sites. Participants chose to participate in either a parent-only focus group or a parent–child dyad interview. Dyad interviews were included as an option for data collection, with the intent of identifying parent–child interactions relevant for intervention design. Once arriving at their scheduled study session, parents completed a paper survey focused on demographics, food purchasing/preparation roles, phone/tablet ownership, and technology use, followed by a focus group/interview session, moderated by a trained research team member. Bilingual team members moderated Spanish-speaking interviews. Semistructured guides were created to assist the moderator in discussing key topics with participants to inform intervention design and content. Three parent-only focus groups were conducted with a range of three to five participants each (n = 13 parents). On average, each parent focus group lasted 54 min (range: 50–56 min). Seven parent–child dyad interviews (n = 7 parents; n = 7 children) were conducted (two conducted with a bilingual moderator, speaking in English with the child and in Spanish with the parent). The sample sizes were based on the literature, the feasibility of conducting the study and reaching saturation.43,44
On average, each dyad interview lasted 35 min (range: 26–52 min). In addition to field notes taken by a trained note-taker, each session was audio-recorded. Concurrent with data collection, research team members met weekly to review study sessions and determined whether data saturation was reached (when data collection failed to elicit new information relevant to intervention design).
Phase 2: Tool development
Content prioritization
In October 2016, parents (accompanying their child/children participating in child-only data collection at the main study site in East Harlem, NYC to develop child tool) completed a brief paper survey to identify preferences for parent-focused health content delivered via a web-based health promotion tool (e.g., recipes, coupons, healthy eating tips, local sales, local farmer's markets, nutrition education, local/community events promoting health, and wellness), as well as assess preferred format and frequency of content delivery (n = 6).
In November 2016, parents (also accompanying their child/children participating in child-only data collection) were invited to participate in a study session at the main study site to discuss: (a) preferences for text or email messages to motivate them to click on a link to access parent-focused health information, (b) behaviors around food shopping, and (c) approaches to communicating/motivating their child. For each session, a trained team member moderated and audio-recorded each interview following a semistructured interview guide, and an additional team member was present to take notes. Two parent interviews were conducted (two other available parents declined to participate), one lasting 47 min (conducted in English) and the other lasting 43 min (conducted in Spanish).
Tool development
In January 2017, parents were invited to participate in a study session using codesigning approaches to develop and confirm aspects of the parent tool. Specifically, a presentation deck and interview guide was designed to walk parent participants through: (a) sample images of text messages parents would receive with a link to access parent-focused health information, (b) a wireframe of the parent tool homepage, and (c) sample content for each section of the parent homepage (i.e., healthy eating tips, tips for parent–child social interaction around healthy eating, recipes, coupons/sales, and resources/events). A trained team member moderated and audio-recorded each session with an additional team member present to take notes. Two parent focus groups were conducted in English (n = 4), one lasting 54 min and the other lasting 96 min.
Usability testing
In June and July 2017, parents were invited to participate in one-on-one usability testing of the web-based tool (n = 9; eight female; three Spanish-speaking). Usability testing is a critical step in development to ensure technology tools are understandable and useful for end-users.32,33 Different aspects of the tool were assessed (text/email messages, login process, and newsletter of week one, two, and three). At each study session, one trained team member moderated, while an additional team member took notes, recording nonverbal reactions and behaviors. Each session comprised a brief think-aloud training, audio-recorded usability testing of the web-based tool components with a think-aloud protocol and moderator guide (with examples of prompts to encourage verbalized feedback from participants throughout testing), and a paper survey to assess usability and acceptability questions using a 5-point Likert-type response scale (see Table 1 for usability survey statements and their usability domains). Examples of think-aloud prompts include, “What do you think of the text message? Is there anything you would change? What do you notice first? What would you change? Would you like to get a newsletter like this? Why or why not?”
Data analysis
Phase1: Formative research
Descriptive analyses were run on survey data to calculate frequencies and percentages. Audio files from focus groups and interviews were translated and/or transcribed verbatim and uploaded into Dedoose software (Version 7.6.6) to facilitate data analysis and coding. Inductive and deductive approaches were utilized in the analysis process. Deductive codes were generated based on the think-aloud moderator guide, which focused on assessing participant usability and feedback on specific aspects of the intervention (i.e., sample text/email message, login process, and sample healthy feeding tip, recipe, coupon). Inductive codes were developed based on reviewing a subset of transcripts, as well as field notes (JB, KFM, and MML). With this preliminary set of codes, one author (JB) coded each transcript, which was then reviewed by another author (MML). Final coded data and representative quotes were organized and summarized into matrices, and patterns were identified (KFM). Throughout this coding and analysis process, meetings were held regularly among all reviewers to resolve coding issues, update the codebook to reflect added, merged, or deleted codes, and discuss/refine emergent themes.
Phase 2: Tool development
Descriptive analyses were run on survey data to calculate frequencies and percentages. Audio files and field notes were systematically reviewed by two authors (KFM, SV). Participants’ comments from sessions conducted between October 2016 and January 2017 were extracted and organized into matrices to identify patterns (KFM). During usability testing in June and July 2017, participants’ utterances were extracted and coded as either positive comments in response to the tool or usability issues; similar comments were grouped into themes and subthemes (KFM, SV). Microsoft Excel code trees and matrices were used to assist with data organization and pattern/theme identification.
Results
Participants: Phase 1 and Phase 2
Twenty parents participated during Phase1, while 15 participated in Phase 2. All parents self-identified as Hispanic/Latino and/or Black/AA, and nearly all were female. Fifty percent of Phase 1 participants (n = 10) returned for Phase 2 content review an usability testing. The remaining Phase 2 participants (n = 5) comprised parents who did not participate during Phase 1 (but their child/children did), as well as participants from a previous study, all meeting eligibility criteria. Table 2 describes the demographic information and participation of parents in each phase.
Demographics of study participants and study participation by phase.

aTen parents from Phase 1 also participated in Phase 2 study sessions; one parent did not provide her age.
bParents could select multiple race/ethnicities.
cSome development phase participants took part in multiple study sessions.
Phase 1
Technology use
Parents reported that devices they used most often were smartphones (100%), followed by desktop/laptop computers (50%) and tablets (30%). In addition, most owned an Android smartphone (55%) compared to an iPhone smartphone (35%). When asked about which device they preferred to use, most parents preferred tablets or laptops/computers over smartphones due to the larger screen but acknowledged the convenience of using a smartphone to read “on-the-go” or quickly preview material before looking at it later on a larger device. When asked about their preferred reading platform, most parents expressed a preference for books or PDFs of printed content over digital print when viewing a lot of text or images. The only exception was with the Kindle, which some parents commented was a device optimized for reading. A few mentioned using voice-controlled devices (e.g., Amazon Echo) to read material to them.
Parents primarily used devices to communicate (e.g., calling, texting, email, Facetime, WhatsApp), access social media platforms (e.g., Facebook, Instagram), and look up information (e.g., calendar, weather, bus times, school-related, directions). Additionally, parents mentioned using devices for entertainment purposes, including playing games, listening to music (e.g., via Pandora), and watching videos/shows/movies (e.g., via YouTube, Netflix). A few parents mentioned using health-related apps, such as ones to track food intake or activity/exercise, ones that provide recipes and show cooking videos.
Important behaviors to promote health
When asked about important dietary habits to stay healthy, parents highlighted eating a variety of fruits and vegetables. Parents often emphasized the importance of “fresh” food and limiting foods with artificial ingredients, like store-bought seasonings and fast food. Importantly, many parents commented on the lack of fresh food in their communities and neighborhoods. Other common behaviors mentioned by parents included eating on a schedule or eating at the “right” times, eating small portions, and eating together—a practice influenced by their culture or traditions passed on from their own parents. Parents also mentioned common barriers to healthy eating including energy to cook/prepare meals (especially “fresh” meals), and cost to purchase healthy food/ingredients and feed a large family. Further some parents stated that having children that were “picky eaters” or had specific dietary preferences, and limited time were additional barriers. In particular, one parent stated: “We’re always on the run. We just grab something and run, or we eat something outside.”
When asked about how parents learned about health-related topics, nearly all parents mentioned looking up health/nutrition/disease information or recipes online (“Google everything!”). However, several noted having to read through a lot of information online before finding what they need or what is relevant. One parent highlighted that looking up health-related information online helped her learn how to replace ingredients in traditional dishes with healthier ones (e.g., beans instead of meat for a protein source). Another parent indicated that getting recipes from their children's school, the CBO (via their nutrition programs, cooking classes, nutrition educators), or YouTube (my whole refrigerator is full of recipes that are from [CBO] from my son!).
Health promotion tool
To inform development of a parent-focused tool, parents were asked to describe what they would want to see in a health-related app for parents and provide feedback on proposed components/aspects.
Family-friendly: Most parents indicated that the app should relate to their family, regardless of the specific content or component, specifically intimating “I would say to be like a family app like family plan where everyone is on the app.” The parents provided specific examples, which included information or resources to help plan dinners but take into account every family member's preferences, allergies, and dietary restrictions; an app that can be shared by the whole family and encourage improvement of healthy eating as a family; include advice on how to make recipes more appealing to the picky eaters of the family; discounts to make healthy eating affordable for their family.
Recipes: Nearly all parents agreed that they would want recipes, and especially ones that were affordable, easy to prepare, using ingredients that were easily accessible, stating “I would love an affordable healthy meal app.” A few also expressed interest in recipes with healthy alternatives to familiar/traditional recipes.
Health-related tips: Parents’ preference was for tips that encouraged their children to eat healthy. For example, they wanted tips on how to motivate their “picky eaters” to eat fruits/vegetables, how to hide vegetables in dishes, what is the recommended daily amount of different food groups for children, what is the evidence behind healthy foods so they can have discussions with their children. A parent intimated that they wanted information to support the information that they were sharing with their children, specifically indicating “I also would appreciate the benefits of certain foods but to the education it helps with me to solidify why I am saying this.” Parents also wanted broader dietary-related information, for example, understanding daily nutritional values, healthier alternatives to recipe ingredients, how to recognize which foods are “really” natural—and tips on how to incorporate healthy habits/behaviors into everyday life.
Discounts and coupons: Parents often spoke of how expensive healthy food and healthy eating was, specifically stating “with $20 you go to a healthy store to get broccoli and fish … you ain’t gonna make it with no $20. So that's why people chose McDonald's, Taco Bell's or something that's quick to make.” Building on these comments, some parents expressed wanting discounts or coupons for fruits, vegetables, and other healthy recipe ingredients. Several parents wanted coupons specific to places they frequently shop at or stores in their communities/neighborhoods.
Look and feel of the app: Parents emphasized that the app needed to be easy to access, understand, and maneuver around or they would lose motivation to use it. In addition, most parents preferred more visuals over text, and color themes that were bright, colorful, and engaging.
Phase 2: Tool development
Content prioritization (October 2016)
Survey data
Based on survey data, parents were most interested in receiving kid-friendly healthy recipes (five out of six), coupons for healthy food items (five out of six), and tips/education related to healthy eating and healthy lifestyles (four out of six). Additionally, some preferred information about sales or deals at local grocery stores (three out of six), local farmers markets (two out of six), and upcoming community events promoting health and wellness (two out of six). With regard to format and delivery of content, two parents preferred an emailed newsletter format, two parents preferred a brief email with a link to more information/full newsletter, and two parents preferred a text message with a link to more information/full newsletter. In terms of frequency, one parent preferred receiving this health information once a month, two preferred twice a month, and three preferred once a week.
Content prioritization (November 2016)
Preferences for messages
After briefly describing potential parent-focused components and content of the health promotion tool, the moderator showed participants different text messages aimed at motivating parents to click on a link to access more parent-focused health information. Both parents generally found all the messages to be motivating as they each offered interesting health-related information plus a clickable web link to find out more. While both agreed that the web link was clear in the message as the text was blue and underlined, they both highlighted their preference for the message that included the entire URL (web address). One parent explained that having the entire URL “lets you know it really is a link,” while the other parent highlighted that if clicking it does not work for some reason, she could always copy and paste it into a web browser and find it herself. When asked about their preference to receive these types of messages by text or email, both noted that they would see and respond to texts faster than emails. When asked about their opinions regarding automated messages, one parent explained that they were annoying if she didn’t know where it was coming from (e.g., spam messages) while the other parent noted that they were “impersonal.”
Food shopping practices
To inform parent-focused content related to coupons and sales for healthy food items, parents were asked questions about their food shopping practices. The parents lived in the East Harlem, NYC neighborhood and frequently did their food shopping at the nearby Costco, noting that it had a large selection and was generally cheaper. Other stores they mentioned included Target and Aldi's. Both preferred not to shop at local groceries or bodegas, indicating that “the things [bodegas] sell have been sitting around for a while.” Additionally, parents noted picky eating habits of their children and how it impacted food shopping and preparation. One parent shared that her child generally did not eat school lunch and as a result, she would buy quick but often unhealthy snacks or takeout food after school to give to her child.
Preferences for motivating/communicating with their child
To inform parent-focused content related to healthy eating and feeding, the moderator showed participants different examples of “tips,” reflecting different parenting/motivating approaches to supporting healthy feeding behaviors with their child (i.e., motivational, instrumental, regulatory, conditional, gain frame, loss frame, gamification). While both parents thought the “motivational” approach may work as it uses a famous person as a role model to encourage drinking more water, they noted that the person may not be influential to all children. One parent already practiced the “instrumental” approach with her child (i.e., packing a water bottle for child to bring to school), stating “you can’t ask, ‘Why didn’t you drink water today?’ if I didn’t give her water today. But if I have the water in my bag for her, she’ll drink it.” With regard to the “regulatory” approach (i.e., make a rule to drink one glass of water before leaving home), one parent did not like the approach of making a rule around drinking water, while the other parent liked the approach because it set a schedule for when to drink water. With the “conditional” approach (i.e., lead by example and drink water with your child during meals), one parent already practiced this noting the importance to lead children by example. While the other parent admitted this approach would be more difficult because she herself does not drink water often, she expressed a willingness to still try since it would benefit her as well to drink more water (i.e., to “get better skin”). Both parents liked the “gain frame” message (and preferred it over the “loss frame” message) as it highlighted the benefits of drinking water if involved in sports (as opposed to the negative effects on their sports performance if not drinking enough water). This approach was especially relevant as one parent's child played sports and the other parent's child took dance. Both parents were intrigued by the “gamification” approach as making water consumption competitive would involve the whole family and potentially work as an effective motivator.
Tool development
Messages
When parents were shown an example of the proposed message template to be used when sending the weekly link to the parent web-based tool homepage (i.e., “This week's parent newsletter is now available! Go check it out! https://www.incinc.org/parentweek1), parents noted they would only open messages from senders that they trusted. Most parents also agreed that they would more likely check messages quickly if sent by text rather than email. Specific suggestions made included writing the specific week number as opposed to simply saying “this week” and including a few details about what is in the newsletter (e.g., recipe ideas, coupons) to motivate them to open the link.
Homepage
When parents were shown a wireframe for the homepage with labeled areas for specific types of content (i.e., healthy tip, recipe, coupon), they generally liked the layout, one describing it as “straight to the point.” Parents had mixed reactions to the proposed background image (arrangement of health foods in the shape of a heart), with one suggesting to instead change the images (i.e., use smaller images and assign to each content section) or the color theme of the newsletter from week to week. A few parents noted that they liked the menu tab labeled “About Intervention INC” so that they could find out more information about the intervention.
Specific content and website design
Parents were then shown examples of content that would populate each specific content area (developed based on data from Phase 1). For content containing healthy eating tips, most parents preferred all the information in one place, as opposed to including a link to more information. For tips around “parent/child social interactions” around healthy eating (reflecting different parenting/motivating approaches behavior change, that is, motivational, instrumental, regulatory, conditional, gain frame, loss frame, gamification), parents reacted positively toward motivational, instrumental, and gamification approaches, and negatively toward the regulatory approach. Parents loved the sample recipe, noting the simple and clear layout of the directions, as well as the simple recipe itself and the inexpensive ingredients. For the coupon section, parents noted that all proposed words for the section title—that is, “coupon,” “sale,” “deals”—were all catchy, and similarly appreciated the clear and simple layout. Parents highlighted the importance of having coupons to places where they frequently shop. For the resources/events section, parents preferred a simple layout (e.g., a very brief description) with a link to more event details (as opposed to placing all the details in the newsletter itself). One parent noted that only events happening in the next 1–2 weeks should be shown.
Usability testing
During usability testing, a think-aloud protocol was used to elicit reactions and feedback from parents as they explored different aspects of the tool (i.e., text/email messages, login process, and web-based newsletter of weeks one, two and three). Afterwards, parents completed a paper usability survey (see Table 1). When parents were sent a text or email message that a new newsletter was available for them to view, some parents noted it did not specify the name of the newsletter. Parents suggested to include “health newsletter” or “Intervention INC newsletter” to provide some context to the nature of the newsletter or who it was from when they read the message. Once they accessed the web-based newsletter, parents expressed how they were attracted by the bright and the vibrant colors used.
Mean usability scores by domain and survey items.

In general, parents felt the healthy feeding tips from the three newsletters were doable and feasible with their children, and that the recipes were simple and easy to follow. They especially liked that the recipes were simple enough that children could help out, or even prepare them on their own. However, some Spanish-speaking parents noted that certain words in the Spanish version of the newsletters were not common to all Spanish-speakers and offered examples of more common words to use. In addition, as many parents did not notice that the recipe could be printed, some suggested making the “Print this Page” text larger or more obvious. In the coupon section and healthy community event section of the newsletters, it was unclear to some parents that they needed to click on the images to open a separate browser window for the actual coupon or more information about the event. To make it more obvious, parents suggested an arrow or some other symbol and/or text saying, “click here.” Despite this, parents reacted positively to these sections, particularly noting that the events were “family-friendly.” Overall, parents reacted very positively to the newsletter, most saying that if they were available, they would like to receive them and even share it with other parents.
Table 1 highlights the mean scores of the four usability domains (usability, usefulness, ease of use and satisfaction) that were assessed via paper survey after the think-aloud protocol. The overall mean score was high (mean = 4.5), with the highest mean for the satisfaction domain (mean = 4.8) and the lowest mean for ease of use domain (mean = 4.3). Table 3 summarizes formative and development phase themes and key findings, as well as their application to web-based tool development.
Summary of key findings from study sessions with parent participants and applications to web-based tool development.

Interdisciplinary design team
An interdisciplinary design team was formed to produce the web-based tool (primary production from October 2016 to September 2017), comprising a graphic designer, computer programmer, and academics (professors, researchers, and students) specializing in health communication, nutrition, psychology, and technology-based interventions. Newsletter content (messages, healthy tips, recipes, coupons, community events) and the overall design were developed using iterative feedback from parents throughout the development phase. After each set of data collection sessions with parents (see Figure 1), key findings were discussed among team members to guide development of content, wireframes, user interfaces, and the user experience. In cases where specific usability issues were raised (e.g., hard to read text, unclear when text was a clickable link, etc.), changes to the user interface were immediately implemented in alignment with universal design best practices. In the few cases where user feedback implied the need for customizations specific to urban, minority populations (e.g., preference for coupons to local groceries, use of more common Spanish words for recipe ingredients and directions), the team agreed that such changes were appropriate to make given the goal to develop and tailor an intervention tool for this population.
Software/hardware used by this team at various development stages included: Microsoft Suite, Google Drive Office Suite, drawing/graphics tablets, Adobe Photoshop, and Microsoft Visual Studio. Additional details and product examples are shown in Appendix A. Software/hardware used by this team at various development stages included: Microsoft Suite, Google Drive Office Suite, drawing/graphics tablets, Adobe Photoshop, and Microsoft Visual Studio. A detailed description of the web-based tool platform specifications is in Appendix B.
Final web-based tool
The final product was a theory-guided, user-centered web-based tool comprised of components aimed at improving parent feeding behaviors and the home food environment (see Figure 2). It consisted of six online newsletters with health content promoting either increased fruit/vegetable (F/V) or water intake of their child. Delivery of this tailored content is based on user (parent and child) responses to initial dietary screening questions, and thus focused on either F/V or water intake depending on the child's prioritized dietary needs and the parent's self-efficacy to support these needs. Newsletters were hosted on a mobile-friendly, web-based platform, with one newsletter released per week for six weeks.

Conceptual framework of the parent web-based tool.
Each newsletter (see Figure 3) contained a healthy feeding recommendation (e.g., “Encourage your child to drink water during every meal!”) with an actionable tip to involve their child (e.g., “Ask your child to fill a pitcher with water and set it on the table while you prepare dinner”), as well as a simple printable recipe, and clickable links to a weekly coupon/sale for a healthy food/drink item and a free/low-cost health-promoting event in the community. Of note, the final intervention will include both the parent and child tool (interactive web-based nutrition comic), thus, each parent newsletter will also have a link to the child tool. The comic has embedded interactive features to engage children around the storyline and its health content aimed at promoting either increased F/V or water intake (a more detailed description of the child comic is described elsewhere). The comic character profiles include “favorite recipes” of each character, which align with the recipes described in the parent newsletters.
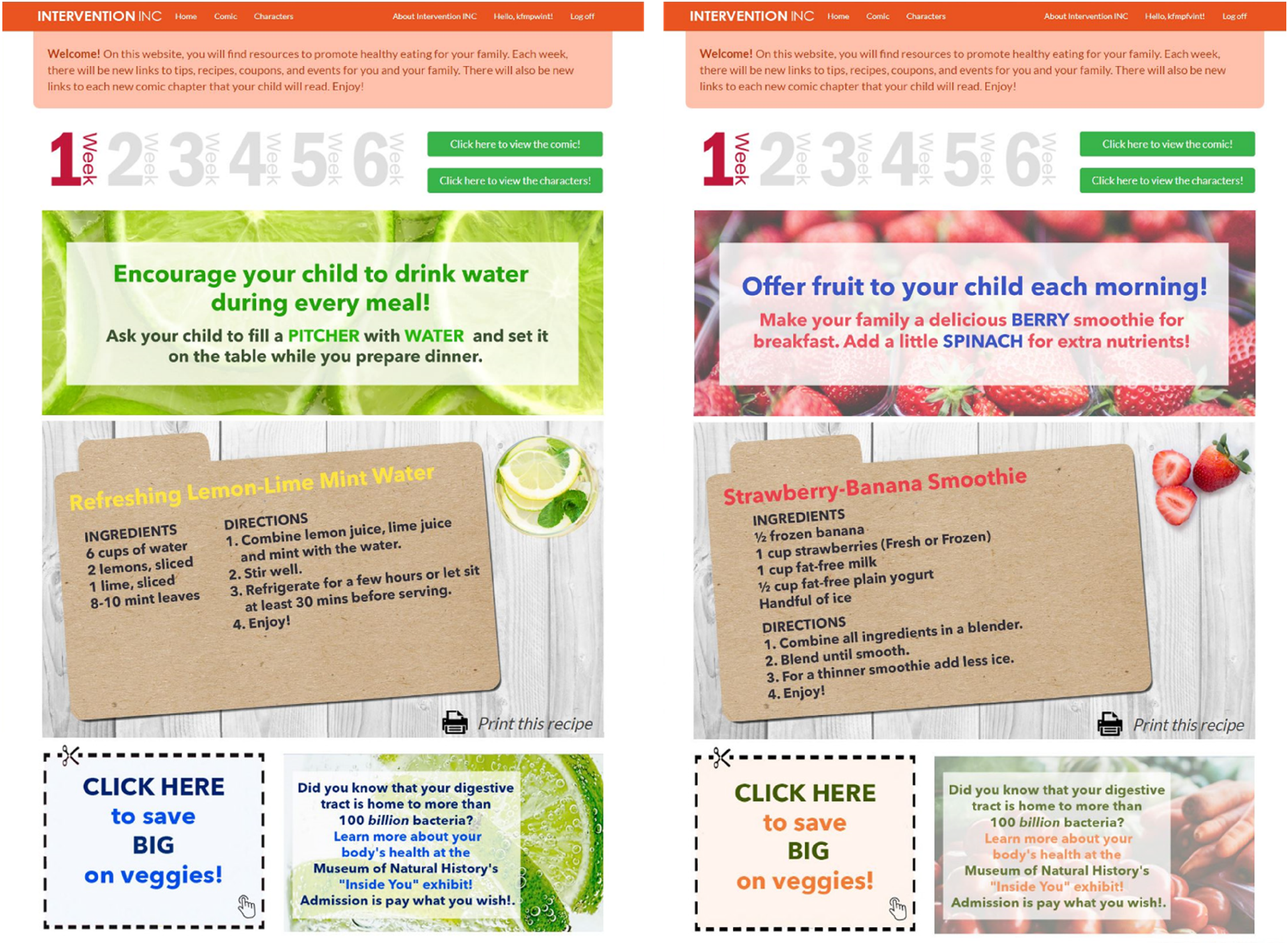
Screenshots of Week 1 parent newsletters (water-focused on left; fruit/vegetable-focused on right).
Discussion
Principal results
The use of technology-based approaches to prevent obesity is rapidly increasing and programs involving parents have shown some efficacy.7,45–48 However, recent literature has revealed that there is a knowledge gap on the effectiveness of mobile health technologies that promote healthy behavior change to prevent childhood obesity in preadolescents (8 to 12 years). 49 According to Yau and colleagues, most involved adolescents or a mix of pediatric and adult populations. 49 Since our web-based tool targets parents with children between the ages of 9 and 12 years, this points to important opportunities to develop parent-involved childhood obesity interventions with tailored content/designs (to increase relevance and engagement), high acceptability and broad dissemination potential (e.g., by using digital platforms as opposed to face-to-face engagement), and targeted implementation efforts to reach diverse, minority populations. In fact, a 2021 systematic review and meta-analysis of web-based interventions designed to change parent feeding practices in support of promoting children's healthy eating concluded that while promising, these interventions were still largely scarce. 50 Further, the authors asserted that while important to design such interventions based on a theoretical framework and including various behavior change techniques and multicomponent strategies, more regular inclusion of self-regulatory strategies could be relevant, and in particular, taking advantage of technological resources.
Specifically, in this manuscript, we describe a two-phase study to iteratively develop and conduct user-testing of a theory-informed, web-based health promotion tool that aims to improve parent feeding practices and the home food environment. This tool was designed to be the parental component of a child–parent intervention aimed at reducing childhood obesity risk in urban Latino and Black/AA preadolescents. 51 We have previously published on the development and usability testing of the primarily child-focused tool, 42 as well as the protocol for the pilot randomized control trial testing the combined child–parent intervention. 51 To the best of our knowledge, this is one of the few studies to date that describes the development and early-testing of a parent-focused childhood obesity tool using user-centered, with none tailored to parents of at-risk minority youth. Furthermore, a user-centered design approach, which aims to incorporate target users at every stage of the design and development process of applications, was used to guide development and testing of our parent tool.19,52,53 User-centered design approaches help to assess and maximize functionality, usability, acceptability, and feasibility, thus increasing the likelihood of successful adoption by end-users, as well as promotion and impact on intended health outcomes.
In this study, through formative phase focus groups and parent–child interviews, we prioritized the development of a web-based, mobile-friendly tool as opposed to a native smartphone application to ensure ease of use across preferred devices (e.g., smartphones, laptops/computers, tablets). Doing so also utilized a health-information seeking pathway already commonly used by parents (i.e., seeking online information and resources). 54 Indeed, literature highlights that parents seek easy-to-access and user-friendly program websites and resources that includes healthy recipes, 55 and information to promote healthy nutrition among children. 54 This was also highlighted in our formative research, as parents desired a tool that supported healthy dietary-related behaviors (i.e., increasing fruit/vegetable and water intake) by providing child-/family-friendly health promotion content.
Throughout development, we designed components of the parent tool to support these identified preferences—that is, feeding practice tips that also encourage child involvement in behaviors around healthy eating, easy/low-cost recipes, coupons, free-/low-cost health-promoting community events—and simultaneously address their most commonly cited barriers to healthy feeding practices (time, energy, cost). In addition, we also included existing resources that parents expressed interest in accessing but may not have been able to easily/typically find on their own (i.e., manufacturer coupons, upcoming free-/low-cost family-friendly events in their local communities). It is important to note that these components of the developed parent tool focused primarily on the delivery of information/content to cue improved parent feeding behaviors, improve behavioral capability to modify the home food environment, and support food parenting styles (as per our Conceptual Framework—see Figure 2). However, it is well-established that there are many other behavioral change techniques (BCTs) and strategies that can be used to support similar outcomes which were not incorporated into the parent tool—that is, goals and planning, feedback and monitoring, reward and threat, social support, etc. 50 While these other BCTs were not included in the design of the parent tool (not meant to be a standalone intervention tool), many were incorporated into the child intervention tool (the main intervention being developed, which the parent tool was meant to only support).
Additionally, development of this parent intervention tool did not consider alternative or enhanced implementation mechanisms beyond direct intervention delivery via mobile-friendly, web-based platform. Dissemination and implementation (D&I) science is one lens in particular that offers concepts and frameworks that are useful in designing implementing, and evaluating parent feeding interventions, especially since parents/families are the primary food socialization agent for children. 56 Further, there are other environmental settings that play a role in food socialization for children including schools, sports, after-school programs that were not incorporated to increase reach.
In several rounds of user-testing of early design and web-based prototypes in the development phase, key parent preferences and facilitators to use and adoption were identified (i.e., “action” words or identifiable icons to prompt users to click on hyperlinks/images, clear and colorful newsletter designs, simple navigation), which were then incorporated into design interfaces to increase engagement and acceptability of tool content. Other usability studies have found similar usability preferences for digital health content that were incorporated such as avoiding lengthy text, limiting use of popups, limiting colors in the design and using one font type.42,57 Feedback from Spanish-speaking parents also helped to identify more commonly used terms/phrasing in Spanish newsletters, making them more acceptable and meaningful to Spanish-speaking users.
Limitations
While this study has many strengths, including an interdisciplinary design team, the use of user-centered approaches with parents of urban, minority children at-risk for childhood obesity, and the integration of evidence-based and theory-guided health promotion content, there are several limitations that should be noted. As the tool was developed specifically as a parental component of a childhood obesity intervention tailored to urban, low-income Black/AA and Latino preadolescents, it has limited generalizability. However, a similar approach to the one described in this study can be used to develop comparable tools among other parent/adult race/ethnic populations. With some data collection conducted in group settings and/or with discussion moderators, key findings could have been biased by social desirability, social norms, and peer groups dynamics. Although early development phase study sessions included a small size, subsequent data collection sessions with more participants confirmed initial findings. The use of some formative phase participants throughout the development phase may have also resulted in biases regarding preconceived ideas for how the web-based tool should look. However, engaging the same participants throughout study phases builds on prior knowledge, which may have contributed to more relevant/informed feedback. Importantly, as user-centered approaches are time- and resource-intensive, development of this tool occurred over a year, although it should be noted that development and user-testing of the primary and more complex child component of the intervention (an interactive, tablet-optimized, six-chapter nutrition comic with integrated goal setting/assessment and tailored messaging) occurred in parallel to the development and user-testing of the parent newsletters.
Conclusions
A systematic design and development process was utilized to create a mobile-friendly, web-based health promotion tool for parents of urban minority children at risk of childhood obesity, focused on providing strategies and resources to improve parent feeding practices and the home food environment. By incorporating user-centered methods throughout the formative and development phases, the needs, priorities, and preferences of the target audience of this tool were able to be voiced through our study participants and integrated into the tool content and user interface design. A two-group pilot randomized study was recently completed (May 2018), primarily testing the tool's feasibility and acceptability, as well as measuring outcomes related to changes in parent feeding practices and the home food environment. If found to be acceptable and effective, it could be disseminated as a publicly available online health promotion tool for parents and implemented in various settings, such as healthcare clinics, and community-based health organizations, highlighting its potential for broad reach.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241298433 - Supplemental material for User-centered design and development of a web-based tool to support healthy feeding practices by parents of urban minority youth at risk for childhood obesity
Supplemental material, sj-docx-1-dhj-10.1177_20552076241298433 for User-centered design and development of a web-based tool to support healthy feeding practices by parents of urban minority youth at risk for childhood obesity by Katrina F Mateo, Helene Vilme, Sandra Verdaguer, Abigail Fuqua, Kris Hoyt, Jacquelyn Davis and May May Leung in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241298433 - Supplemental material for User-centered design and development of a web-based tool to support healthy feeding practices by parents of urban minority youth at risk for childhood obesity
Supplemental material, sj-docx-2-dhj-10.1177_20552076241298433 for User-centered design and development of a web-based tool to support healthy feeding practices by parents of urban minority youth at risk for childhood obesity by Katrina F Mateo, Helene Vilme, Sandra Verdaguer, Abigail Fuqua, Kris Hoyt, Jacquelyn Davis and May May Leung in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors would like to acknowledge the larger team of research assistants and other collaborators involved in participant recruitment, data collection, and tool content/design development and internal testing.
Contributorship
KFM and MML conceived the study design and protocols. KFM, SV, and JB were responsible for data collection and analysis. AF and KH were the user interface designer and software developer of the intervention tool. KFM and HV were primarily responsible for manuscript preparation, with support from SV and MML. All authors reviewed and approved this manuscript for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All study procedures were approved by the Hunter College Institutional Review Board (#2015-0547) and is registered with the Clinical Trials Registry (NCT03165474).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grant number R21H5024117 from the Agency for Healthcare Research and Quality (AHRQ). The content is solely the responsibility of the authors and do not necessarily represent the official views of AHRQ.
Guarantor
MML.
Supplemental material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.