
Abstract
Background
Technology advancement along with the increase in the older adults’ population leads to the creation of health applications. The combination of exercise, nutrition, and cognition should be studied carefully in improving older adults’ health.
Objective
The purpose of this study is to develop a health application, WeFit contains these three components and to determine its content validity, acceptability, and usability.
Methodology
This study is a design and development study involving three phases. The first phase is the need analysis involving a review on 16 mobile applications available in Google play and iTunes App store as well as a review of six articles for identifying the perception of older adults in using mobile applications. Second phase is mobile application development and content validity. The content validity was determined using the Content Validity Index for Individual Items (I-CVI). Phase 3 evaluated the acceptance of the WeFit mobile application among older adults and health practitioners.
Results
Phase 1 indicated that half of the applications reviewed (50.0%) had physical activity component and the other half (50.0%) had a cognitive component, and none on nutrition. No application is reported to have all three components. In Phase 2, WeFit health application containing the three components was developed where users can view exercise and food recommendations and play cognitive games. WeFit had an I-CVI value of 0.98. With respect to acceptability, majority of the study participants (93.3%) understood the WeFit's content and the graphics used were appropriate. The usability study found that the majority of the older adults were satisfied with the interface and content. All health practitioners (100%) agreed WeFit is easy to use and agreed that it can guide them in giving medical advices.
Conclusion
WeFit mobile app has been successfully developed, validated, and tested for acceptance among the older adults and health practitioners.
Introduction
The world's older population continues to grow at a rapid pace. Today, there are 703 million people aged 65 years or over in the world.1,2 This number is projected to double to 1.5 billion in 2050 with the proportion of one in six people in the world will be aged 65 years or over. 1 Narrowing down to Malaysia's population, older adults are defined as those who are aged 60 years and above. 3 This subpopulation has increased gradually since the 1970s and expected to be tripled from 2.0 million today to more than 6.0 million by 2040. This phenomenon represents one of the remarkable achievements of mankind's history with respect to health, social, and economic improvements over time. The improvements in healthcare systems such as infections control, immunizations, and better access to healthcare are among the huge contributors to the sustained increases in life expectancy across the globe.1,4
However, this successful history of human life expectancy did not come with a proportionate increase in quality of life for older adults. As heavily discussed in the literature, increased life expectancy has increased the risk in developing chronic diseases, disability, and dementia prior to death.4–6 This explains a higher use of health services and greater demand for specialized services among the older adults.4–6 Consequently, this puts increasing pressure on the economy and social systems in most countries due to the complexity of health services required along with increased health expenditure.7–9
This rapid growth of technology, particularly in smartphones and internet use, has led to a surge of interest in using mobile applications as a tool to seek health information as well as to monitor and manage health (commonly known as mobile health or mHealth). To date, no standardized definition for mHealth has been established, but the WHO defines mHealth as “medical and public health practice supported by mobile devices, personal digital assistants and other wireless devices.” 10 There are more than 325,000 identified mHealth applications covering diverse health, fitness, and medical topics.11,12 There is clear evidence that mHealth applications are effective in improving self-care, self-management, self-efficacy, medication adherence, as well as in improving health behaviors such as quality of sleep, diet, physical activity, and mental health.13–16 There are numerous studies demonstrating the benefits of mHealth toward older adults. 17 This includes addressing existing barriers to treatment such as long waiting time at hospital, poor access to transportation, and increased cost of healthcare services.13–17
A multinational study involving 2299 older adults from both the urban and rural areas in Malaysia reported that majority of the respondents were deficient of both macro and micronutrients regardless of gender, socioeconomic status, and location of residence either urban or rural areas. 18 Thus, online nutrition education specifically tailored for older adults is essential to improve their health and well-being. mhealth applications are less expensive and efficient as compared to traditional system. 19 In addition, physical activity among older adults is one of the risk factors of various health issues such as cardiovascular diseases, stroke, type 2 diabetes, and breast and colon cancer. Despite the substantial benefits of physical activity for healthy aging, physical inactivity among the elderly in Malaysia is still a significant public health concern. 20 According to National Health and Morbidity Survey 2019, approximately 38.3% of older adults (aged 60 years and above) were physically inactive. 21 Physical inactivity among older adults is due to low education level, functional limitation, frailty, being depressed, and environmental factors such as lack of infrastructure or recreational facilities.20,22
Aging is associated with decline in cognitive function namely the executive function, processing speed, language, visuospatial ability, attention, and memory. 23 Multidomain intervention is vital for addressing the declining cognitive function among older adults. The use of a holistic intervention combing exercise, diet counseling, vascular risk management, social activity, and cognitive training in The Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER) was found to lower the risk of dementia. 24 Limited use of technologies has been reported to be associated with hippocampal atrophy among older adults from the Intelligent Systems for Assessing Aging Change longitudinal study. 25 Mohandis et al. developed a persuasive system design (PSD) which was well-accepted by older adults who performed vigorous intensity physical activity participating in this study, but not among sedentary older adults. 26 The PSD consisted of primary task support, dialogue support, credibility support, and social support.
As of 2020, there are no mobile apps that contain the three main components (exercise, nutrition, and cognitive function) identified in the literature, especially mobile app in Malay version.11,12 Therefore, this study aimed to develop and determine the validity, acceptability as well usability of the “Warga Emas Fit (WeFit)” mobile app as a self-monitoring tool among older adults. The WeFit mobile app with three main features namely nutrition, physical activity, and cognitive function will empower and engage older adults to manage and monitor their health.
Methods
Study design
This design and development study was divided into three phases comprising (1) need assessment (2) development of mobile application and content validation and (3) acceptance and usability testing among older adults. Ethical approval was obtained from the secretariat for human research ethics of Universiti Kebangsaan Malaysia (UKM PPI/111/8/JEP-2018-455). The study was conducted from August 2018 to August 2020. Prior to all studies, participants were given information about the study, and signed informed consents were obtained from individual participants.
Phase I: Need assessment
Prior to the development of the mobile application, need assessment was conducted by performing a scoping review on the available mobile applications in iTunes and Google Play (Figure 1). This was to determine the availability of mobile application which combined the three components namely exercise, nutrition, and cognition. The keywords used were “health older,” “healthy aging,” “healthy ageing,” “ageing,” “health elderly,” “frail,” and “elderly care.”

Mobile application search strategy and selection process.
Another scoping review was conducted to identify older adults’ readiness in using mobile application for managing their health, barriers in using mobile application for health management, and the possible motivating factors in using the mobile application. Search has been conducted using several databases such as PubMed, Excerpta Medica Database, Cumulative Index to Nursing and Allied Health Literature, Cochrane Library, Google Scholar, ScienceDirect, Journal of the American Medical Informatics Association, the Journal of Medical Internet Research, the International Journal of Digital Healthcare, Digital Health, and the Journal of mHealth. Besides that, search had been done in Grey Literature Report, OpenGrey, and Web of Science Conference Proceedings for identifying proceeding paper. The search terms that had been used were [mobile app or mhealth or mobile health or telehealth or mobile technology], [elderly or aging population, older population, aging, geriatric], [view or attitude or mindset or willingness or readiness or acceptability], [limitation or difficulty or restriction or drawback], and [motivate or promote or help, ease, and aid]. Search strategy was done using PRISMA guideline, as shown in Figure 2.

PRISMA flowchart for article selection strategy.
Phase II: Development
Prior to the development of WeFit, a literature review was conducted to identify current gaps in the literature regarding older adults’ willingness, perceived barriers, and motivators in adopting mobile applications for health-related interventions. This study had been published previously by the researcher’s team, 27 and the article discussed literature and prominent barriers, willingness, and motivators has been identified according to Theoretical Domain Framework. 28 Table 1 summarizing this information from study. 27
Willingness, perceived barriers, and motivators in adopting mobile applications for health-related interventions. 27

Next, several group discussions and meetings were conducted among the research team members (postgraduate students, principal investigator, and coresearchers) with the WeFit application developer, other experts in information technology, lectures from the various educational program namely nutrition, dietetics, and public health to identify the intended features, interface, and design to meet the functional needs of the older adults. After which, preparation of the proposed product features and design using international guidelines for ease of use and usability of graphic user interface for older persons (ISO/IEC 2001) was done. This guideline has been used to ensure and improve its usability among the older adults. The guideline includes the need to use high-contrast colors, larger text size, clear, and appropriate usage of words to describe the function of a particular button or icon, include a title and accurate description/explanation on the purpose of the system.
Prior to the use of WeFit, participants were shown an informed consent on data protection policy at the beginning of the app interface. Personal information or data were only saved in the user's device and could only be assessed by the user and researcher. It is also noteworthy that the information stored in WeFit will be handled in a similar way to hard copies of medical records, as declared in the Data Protection Disclaimer and Laws of Malaysia Act 709 and Personal Data Protection Act 2010. Since WeFit is a self-screening mobile app for identifying fall risk, and it does not provide any diagnosis or suggestion to change current medical dosages, it is not categorized as a medical device, which would require an approval from health authorities.
WeFit was developed by a freelance mobile software developer with more than five years’ experience in a related field, based on the proposed product features and design of the researcher team. The development of WeFit was conducted according to the waterfall software development process using agile principles for better quality, time, and cost-effective mobile app development.
Phase II content validation
Content validation was done among health professionals from Hospital Canselor Tuanku Mukhriz and Kuala Lumpur Hospital. Since this study was conducted during Covid-19 pandemic, an online approach via Google form had been administered to obtain the experts’ feedback. They were given one week to provide their feedback. Content validity is essential to ensure that the WeFit content is applicable and relevant before being used by the older adults. All the 10 health care professionals (HCPs) selected for this study met both the inclusion criteria of the study: (1) having more than five years of working experience, (2) is currently involved in professional related to nutrition, dietetics, exercise, physiotherapy, psychology, medical, and geriatrics. Purposive sampling approach had been employed for the selection of HCP. According to Lynn et al., at least three experts were required for content validation. 29 Thus, for this study ten professionals which consisted of one (10%) geriatrician, three (30%) dietitians, three (30%) physiotherapists, and three (30%) clinical psychologists were recruited to evaluate the domains of exercise, nutrition, and cognitive function, respectively.
The content validation questionnaire had been adapted from the previous study. 30 It had three sections with 19 items. Each item had options with 4-point Likert scale ranging from score 1 to 4. The first section was the sociodemographic information, while the second section was related to the use of smartphone Android, iOS, or both. In this section, user feedback of using smartphone was obtained. The final section was the WeFIT content validation item which consists of content, graphics, and color. Answer option of 3 and 4 was considered relevant while 1 and 2 were not relevant. Content validity index for individual items (I-CVI) were calculated to determine the relevance of an individual item in the feedback form. WeFIT application was considered relevant if it had I-CVI value of more than 0.78.
Phase III: User acceptance and usability testing
WeFit user acceptance testing (UAT) was tested 15 older adults.
Participant recruitment
A purposive sampling method was used to recruit the participants from two senior citizen clubs in Klang Valley, central of Malaysia via letters of invitation. Senior citizens activity center is a place for senior citizens to carry out daily activities within the community where it focuses on active, healthy, and productive aging. The older adults have the chance to participate in various activities as efforts toward a healthy lifestyle. Some of the activities include health talks, reflexology, and urban gardening. Participants were community-dwelling older persons aged 60 years and over and were from the main ethnicities in Malaysia (Malay, Chinese, and Indian). Inclusion criteria included being 60 years and above, able to comprehend the Malay or English language and can use a smartphone. Older adults with psychological and neurological problems (depression, dementia, and Parkinson's disease), who have physical disability problems (arthritis, amputation, spinal pain), and also those with various comorbidities or uncontrolled chronic diseases such as cardiovascular disease and cancer were excluded.
Procedure and instrumentation
Participants were given information regarding the procedures and consent to participate in this study. Participant level of smartphone proficiency was determined verbally before conducting the study. A phone call was conducted and among the questions asked were smartphone ownership, availability of smartphone application (WhatsApp), and the availability of registered e-mail. E-mail was required for logging in the WeFit application for data security purpose. A brief explanation about the study including the study flow, the aim of WeFit mobile application development as well as the 7-point Likert scale open-ended questionnaire that they received were provided. Any enquiries in the form of messages or calls from the participants were allowed within the study period.
Calculation on sample size was made using the priori power analysis method (Cohen, 1988) with the G*Power 3.1 software, a statistical correlation test: point biserial model was used with a priori. By using a coefficient of determination p2 = 0.5p^2 = 0.5p2 = 0.5, an effect size of 0.707 was obtained. 31 The information was entered into the input parameters for a two-tailed test with a power of 0.9. The output parameters were automatically calculated, indicating that a total sample size of 13 participants is required. WeFit UAT was tested among 15 older adults.
All 15 participants owning a smartphone have WhatsApp application installed and have their own personal registered e-mail. The older adults were invited to participate in this study online due to the study conducted during Covid-19 pandemic. A downloadable link for WeFit mobile app was given online along with the information sheet.
The older adults were invited internally online to participate in this study due to the study has been conducted during Covid-19 pandemic. A downloadable link for WeFit mobile app was given online along with the information sheet. They were given one week to utilize the WeFit app and required to answer the online feedback form. They will be given a questionnaire to explore their understanding of WeFit in relation to its features and design: (1) color contrast, (2) graphics or illustration, (3) font size, (4) presentation of instructional video, and (5) overall WeFit suitability. A modified version of a technology acceptance model (TAM) survey was also used. The TAM is rated on 7-point Likert scale and has a high internal reliability (Cronbach α = 0.96) and positive correlation between each determinant (perceived usefulness, perceived ease of use, intention, and attitude toward use of mobile technology). The determinants are four items of perceived usefulness, seven items of perceived ease of use, three items attitude toward the use, and two items in behavioral intention to use. 30
Results
From the 16 applications selected, eight applications had the physical activity components. These applications offered routine exercise guideline and encouraged users to perform physical activity. The eight applications were (1) Exercise plan for seniors, (2) Wysefit: Exercise App for 50+, (3) Moves4me, (4) Lori's Movin and Groovin, (5) Exercise tips for elderly, (6) Yoga Exercise for Seniors, (7) Senior Fitness Home Workout for Older Adults, and (8) Senior Beginner Workout. Another 50% of the applications had cognitive components especially brain games for stimulating cognitive function of older adults. The eight applications were (1) Mindmate: For a Healthy Brain, (2) Train your brain-Attention Games, (3) Train your brain-Memory Games, (4) Train your brain-Coordination Games, (5) Train your brain-Reasoning Games, (6) Memory Games for Elderly, (7) Brain Games for prevention of Dementia, and (8) Memory Exercise for Alzheimer's.
From the 16 applications, none had dietary or nutrition component. None of the applications combined physical and cognitive domains or had combination of all the three components. About 37.5% of the application content had been validated by the healthcare professionals and two of the applications offered personalized health consultation session.
The final articles selected for this study were published from year 2017 till 2020.32–37 Five articles were qualitative and only one study was quantitative. All the articles discussed about the barriers in using mobile application of which limited technology knowledge as well as not being tech-savvy. Some of the articles highlighted that using mobile application can be waste of time as older adults have difficulties to learn and explore.
However, there were several motivating factors highlighted in the articles namely positive thoughts about using mobile applications and important features embedded in the health applications such as medications intake alert, reminder for stocking medications, and medications interaction.
Phase II: WeFit final version
Figure 3 and 4 depict the screenshot of WeFit with English translation. On the first page of this WeFit application, there were two buttons namely “Login” and “Register” displayed. Users were required to sign in by pressing the “Register” button and entering their email to allow them to access the features of the WeFit application. A key button in the upper left corner was displayed on this page intended for users to access the entire content of the application. The keypad contained five options namely “Main,” “Profile,” “Exercise,” “Nutrition,” and “Cognitive.”

Home page of WeFit mobile application with English translation.
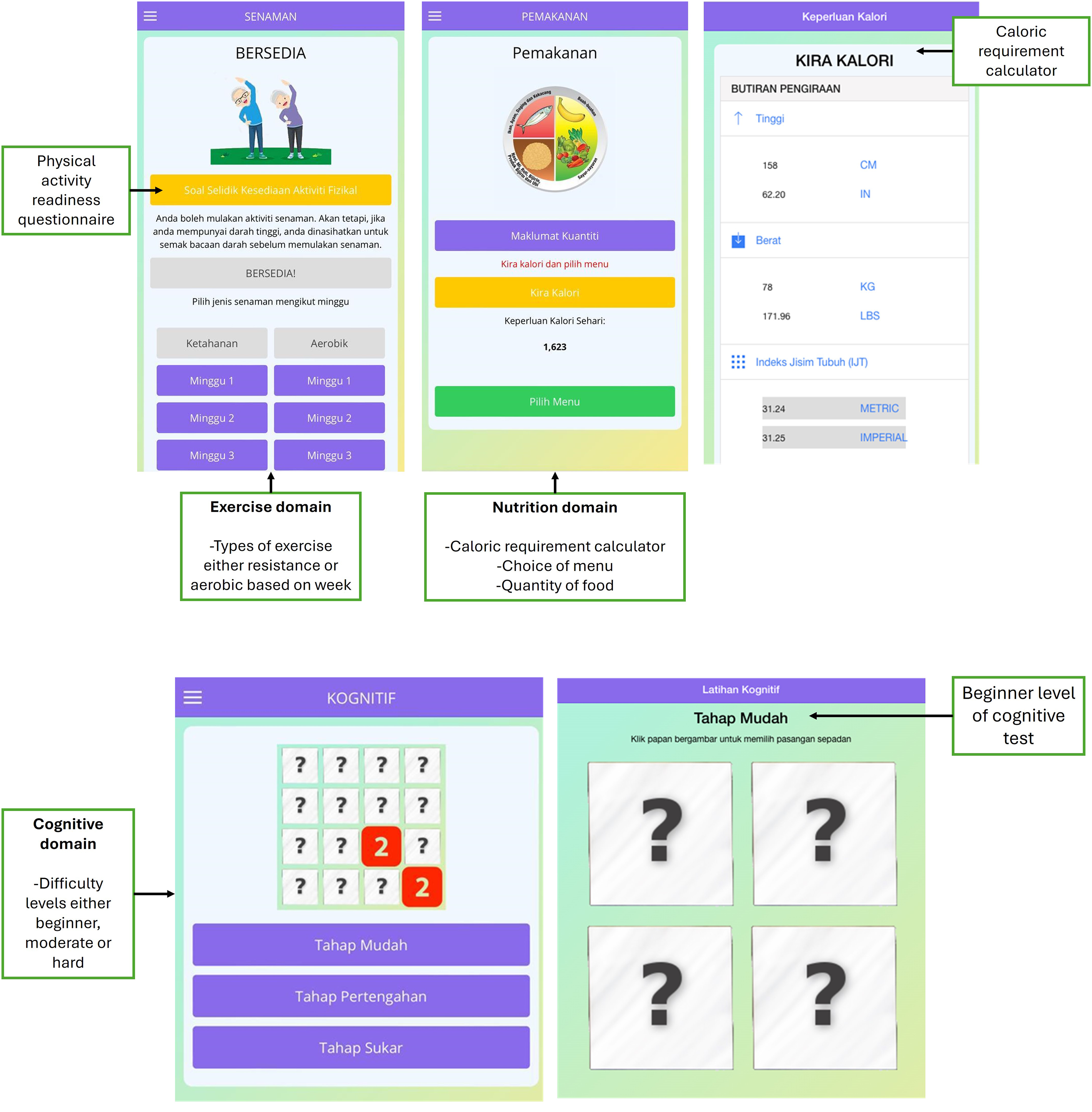
Exercise, nutrition, and cognitive page in WeFit mobile application with English translation.
Phase II: WeFit validation
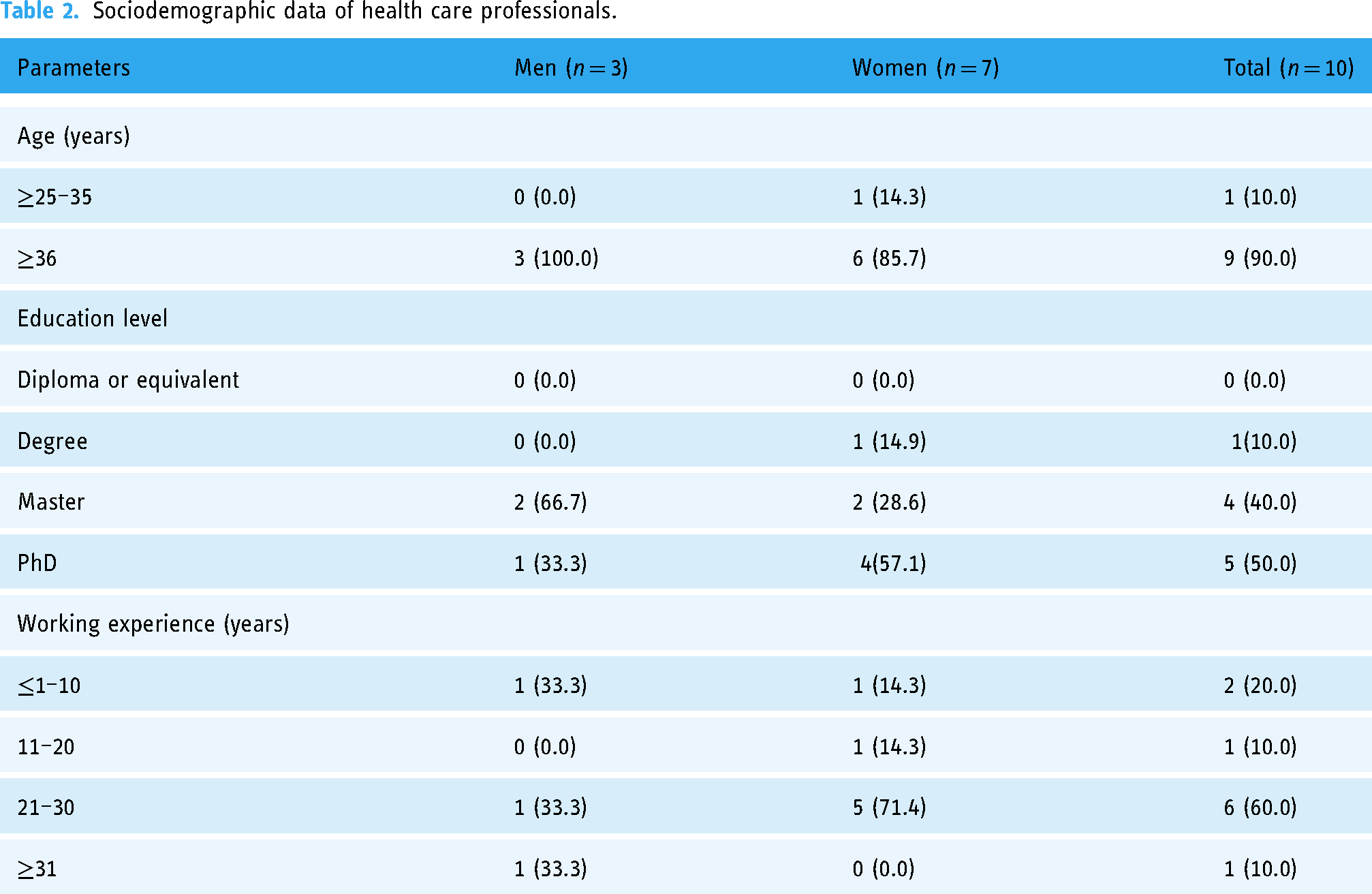
Ten experts were recruited which consisted of one (10%) geriatrician, three (30%) dietitian, three (30%) physiotherapist, and three (30%) of clinical psychologist. All the healthcare professionals were university graduates. Table 2 is the sociodemographic data of the healthcare professional who participated in the validation study.
Sociodemographic data of health care professionals.
The validation results showed that the content, graphics, and colors of WeFIT were suitable. All the health professionals chose score 3 or 4 as the options for all the questions for the main page, exercise, and dietary page, indicating good acceptance. On the other hand, for the cognitive page, there were few items such as use of graphics, types of games, and difficulty level of the games were that were given score 1 or 2. The WeFIT content was considered valid if the I-CVI value was above 0.78. The mean I-CVI value for WeFIT was 0.98. Table 3 shows the mean I-CVI values for all items in the questionnaire.
Mean I-CVI.

Phase III: User acceptance and usability testing
The study participants consisted of six men participants and nine women participants. The average participants’ age was between 60 and 65 years old. Most of the participants who were involved in this study were Malay (73.3%). All the participants received tertiary education of diploma (46.7%), bachelor's degree (46.7%), and master's and doctoral degree (6.6%). Table 4 shows the sociodemographic data of the participants recruited in the user acceptance survey of WeFit.
Sociodemographic characteristics of participants of the acceptance study.

It was found that more than 90% (14/15) of the participants were able to comprehend the contents of WeFit and agreed with its suitability of the use of graphics and color combinations used. All participants (100%) understood the video exercises that have been included in the mobile application. However, 33.3% (5/15) of participants reported that the font size used in WeFit was not suitable. Overall, 80% (12/15) of participants found that WeFit is suitable as a self-manage health mobile app that can be used among Malaysian community-dwelling older adults. A total of 80.0% of older adults can accept this WeFit application as a whole. Technology Acceptance Model survey results showed the presence of a high correlation (0.70 and above) between all determinants (perceived usefulness, perceived ease of use, intention, and attitude toward usage of mobile technology). Table 5 shows the results of the acceptance study.
User's acceptance test result based on different domains of WeFit based on gender.

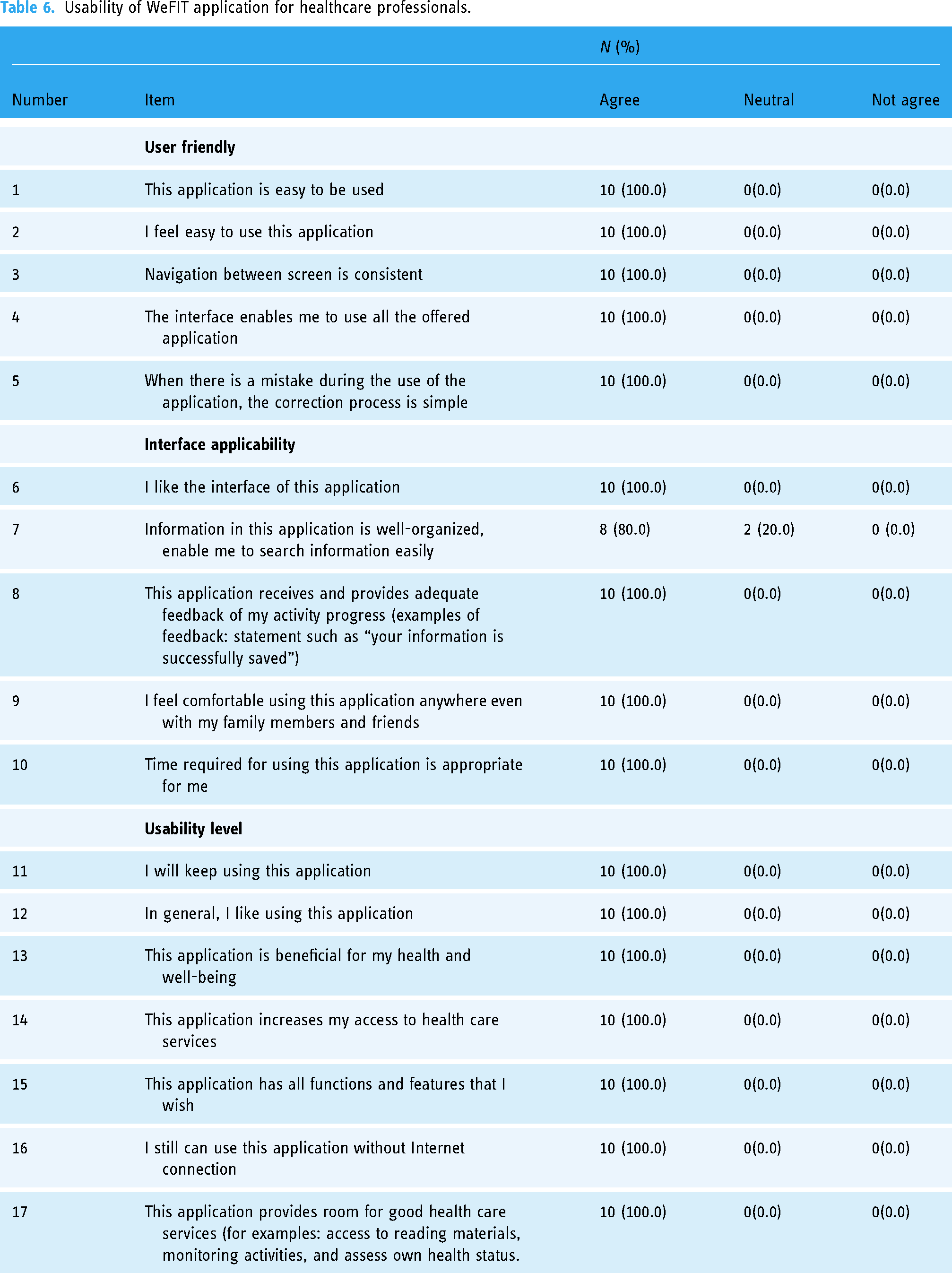
Findings revealed that 100% of the professionals agreed that the WeFIT application is useful and able to guide the professionals when treating their patients. Only 20% of the professionals chose neutral option for the item related to information arrangement. Findings are presented in Table 6.
Usability of WeFIT application for healthcare professionals.
Discussion
The study has successfully developed a smartphone application, WeFit targeting older population. WeFit has three main components which are exercise, nutrition, and cognitive function; based on need assessment, validation, acceptance, and usability evaluation.
This WeFit application has been developed based on the graphical user interface guidelines (GUI) for older adults (ISO/IEC Guide 71: 2001 (E)). WeFit is a senior friendly application as it has less navigation, more icons, and suitable colors and has organized navigation buttons. One study has found that critical limiting factors for usage of mHealth applications among older adults are small font size, font type, button type keys, QWERTY keyboard size, icon size, and navigation options that are too complex to understand. 28 This highlights the importance of adhering to the GUI guidelines for the older adults (ISO/IEC 2001) to aid any mobile health application development. This guideline explains the importance of using high-contrast colors, large font sizes, and suitable font type when designing smartphone-based application for older adults. Older adults who use the Internet have higher likelihood to browse information online, however, not all the available online applications are senior-friendly. Hong et al. had developed a special application to promote physical activity among older cancer survivors. The app is known as iCanFit web application which has four important features namely goals of physical activity, community for creating network, tips on healthy living, and reliable health information resources. Almost 56% of the study participants agreed to continue using this application. 38
In addition, WeFit has good content validation index (I-CVI) of 0.94. An I-CVI (Item Content Validity Index) of 0.78 or higher is often considered reliable based on the method for assessing content validity developed by Lynn and later refined by Polit, Beck, and Owen (2007).29,39 The I-CVI is used to determine the extent to which individual items on a scale are relevant and representative of the construct being measured, based on the judgment of experts. Lynn suggested that an item should be retained if the I-CVI is 0.78 or higher when the number of experts reviewing the item is five or more. This threshold ensures that the item is generally agreed upon as valid by a significant majority of the experts. Polit et al. conducted further research to support this threshold, indicating that an I-CVI of 0.78 or above is acceptable when using a small number of experts. Content Validity Index for Individual Item above 0.78 reflects reasonable level of agreement among experts, which indicates good content validity. 39
Our findings showed that 80% of the participants agreed that WeFit is suitable for use as a self-monitoring tool among Malaysian community-dwelling older person. Through UAT, it was found that the use of graphics, color combinations, and font size application in WeFit is acceptable. The large font size used in this study is in line with another previous study which reported that large font sizes can increase the acceptance and use of technology among older adults. 26 This is because the large font size can help the older adults to read clearly, quickly, and enable positive effect on the usability of a health application. The results of the study from acceptance test, found more than 90% of the study participants understood the contents of the WeFit application and it was easy to use. The current study participants also reported that they understood the content of the exercise videos that has been embedded in WeFit. Exercise videos serve as a platform for delivering information especially among the older adults. 40 Usage of nonclinical or technical words (layman terms) in the exercise video subtitles are one of the attractive factors among the study participants. This is supported by previous study reporting that older adults are motivated to participate in exercise or play video games if a simple design and easy-to-understand word choice are used. 41 Another personalized hologram coach platform aimed for coaching and empowering older adults with poor balance known as HOLOBALANCE received positive responses from its users. 42 Mehra et al. developed a tablet-based mHealth intervention known as VITAMIN for supporting older adults to exercise at home. This app had five features namely the exercises (library with 16 functional exercise), profile (setting personal goals with appropriate exercises), weekly schedule (exercise icons planned for each day of the week), today (exercise planned for the day), and video calling (call for consulting a personal coach for advising on exercise). Although some respondents had difficulties using tablets, majority gave positive responses toward the application. 43
WeFit application incorporates three elements which are diet/nutrition, physical activity, and cognitive training. Combining these three elements in a single mHealth application offers a synergistic and holistic approach to improving the health and well-being of older adults. Ngandu et al. found that a multidomain intervention (including diet, physical activity, and cognitive training) delivered through an mHealth app improved cognitive function, physical health, and reduced the risk of dementia in older adults over two years. 44 To add, mHealth applications that integrate multiple components into one platform are more likely to engage users consistently. This comprehensive approach reduces the need for multiple apps, simplifying the user experience and promoting sustained engagement. Lam et al. (2021) reported that older adults using a multicomponent mHealth app were more likely to adhere to lifestyle interventions and showed better health outcomes, including improved physical and cognitive function, compared to those using separate apps for each component. 45 Another study by Mavros et al. found that older adults using an integrated mHealth app for diet, exercise, and cognitive training had a lower incidence of falls, improved cognitive function, and better overall physical health over a 12-month period. 46
Limitations and strengths
One of the limitations of the study is the acceptance testing of WeFit application was conducted among senior citizens who lived in cities where all of them have good access to the internet and are also capable of having a smartphone. Therefore, the findings may not cover the various layers of different socioeconomic background. However, note that our study comprised older persons from Peninsular Malaysia and all three main ethnicities (Malays, Chinese, and Indians), and the results can be generalized to the entire community-dwelling older population. Another limitation is the small sample sizes. Small sample sizes limit the ability to conduct meaningful subgroup analyses. This is particularly important in mHealth research where different subgroups (e.g., by age, health status, or baseline activity levels) may respond differently to interventions. Finally, this study only involved single institution used for selection of health professionals in Phase 3 study.
The main strength of this study is that it is a smartphone health application development study targeting the older adults which includes three main components which are exercise, nutrition, and cognitive function. This WeFit application is equipped with a data saving system as it saves data such as the number of repetitions, time, and intensity when doing the suggested exercise and the users can review all this data at any time desired. By no means directly, it can help the older adults in getting a more accurate and precise health consultation from their HCPs. Health data that are kept digitally are much safer as it can prevent any unwanted data leakage as well as breached of privacy. Health applications have greatly helped HCPs in performing their duties, especially with regard to their time management and access to health records. This has given improved patient care in relation to clinical decision making.
Clinically, WeFit has the potential to be used as a self-monitoring tool, caregiver administered, or at primary health care settings as it can aid clinical decision making among the HCPs. This will assist in the efficiency of delivering tailored and personalized health consultation between older adults and their HCP. Packaged as a mobile app, WeFit is accessible anywhere, anytime, and is simple, fast, and easy to administer. However, WeFit could be improved by incorporating food calorie trackers to help older adults to monitor their daily nutrition intake. And, developing it in few other languages (English, Tamil, and Chinese) to promote better engagements with the users in Malaysia and even other countries.
Conclusion
In this study, the mobile application, WeFit was successfully developed, validated, and tested for acceptance and usability. To the best of our knowledge, WeFit is the only mobile health app that is in Malay language version that includes three components namely exercise, nutrition, and cognitive function for the use of monitoring and managing health among the older adults. However, there is a need to determine the cost-effectiveness of the application for its ability to empower health among older adults. The integration of diet/nutrition, physical activity, and cognitive training in mobile health (mHealth) applications for older adults has significant implications for future research. As this approach becomes more prevalent, several key areas of focus can be identified to maximize the effectiveness and reach of these interventions. Future research should explore how to tailor mHealth interventions to the unique needs, preferences, and health conditions of individual users. Personalization could involve adapting the content based on factors such as age, gender, baseline health status, and cultural background. Future studies could investigate the development and efficacy of algorithms that use data from wearable devices, user input, and health records to customize recommendations for diet, exercise, and cognitive training. While short-term benefits of integrated mHealth interventions are well-documented, long-term effects, and sustainability remain areas for further exploration. Understanding how these interventions impact health over extended periods is crucial for establishing their role in aging populations. Future studies could include longitudinal studies could examine the sustained effects of using mHealth apps over several years, assessing outcomes such as cognitive decline, physical frailty, and quality of life. Researchers could also investigate factors that influence long-term adherence and engagement. Social and environmental factors, such as social support, living environment, and access to resources, can significantly influence the effectiveness of mHealth interventions. Understanding these factors can help in designing more comprehensive and effective programs. Future studies could examine how social and environmental factors interact with mHealth interventions to influence health outcomes. Research could also explore ways to incorporate social support features, such as peer networks or community engagement, into mHealth apps to enhance their effectiveness.
Footnotes
Acknowledgements
The authors are grateful to Universiti Kebangsaan Malaysia for supporting the conduct of this study. The authors would like to thank the participants and staff who contributed to this study.
Contributorship
NAA: data analysis, literature review, drafting of manuscript, approving final version of manuscript. AFML: conceptualization, methodology, editing manuscript, supervision, project administration, funding acquisition, approving final version of manuscript. DV: drafting of manuscript, editing manuscript, approving final version of manuscript. NLT: conceptualization, methodology, editing manuscript, supervision, approving final version of manuscript. ZAM: conceptualization, methodology, editing manuscript, supervision, approving final version of manuscript. SS: conceptualization, methodology, editing manuscript, supervision, project administration, approving final version of manuscript. SAMN: conceptualization, methodology, editing manuscript, supervision, project administration, approving final version of manuscript
Data availability
The data of this study is available upon request from the corresponding author
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The secretariat for human research ethics of Universiti Kebangsaan Malaysia (UKM PPI/111/8/JEP-2018-455).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received funding from the Ministry of Higher Education via the Dana Cabaran Perdana (DCP-2017-002/3).
Guarantor
All subjects included in this study have provided consent to participate and publish their data anonymously.