
Abstract
Objective
To delineate the characteristics of the work undertaken by general practitioners (GPs) and staff in implementing and utilising video consultation within their situated clinical contexts.
Methods
The data material comprises 33 semi-structured interviews with GPs and staff and 132 hours of ethnographic fieldwork across seven clinics in Denmark. The data collection period spanned from June 2021 to August 2022. Reflexive thematic analysis was employed to analyse the data, drawing inspiration from the concept of invisible work as proposed by Susan Leigh Star and Anselm Strauss.
Results
Four types of invisible work were identified through the analysis: (1) the work of introducing video consultations, (2) the work of stabilising video consultation use, (3) the work of coordinating users and systems, (4) the work of repair as a response to breakdowns.
Conclusions
The video consultation changes the organisational structure and leads to a reconfiguration of professional roles and existing work practices. Moreover, implementing and using video consultations demands articulation, inclusion and affective work by GPs and staff, and this work includes allocating time to coordinate tasks, do workarounds and repair breakdowns.
Introduction
Video consultation was introduced in 2020 in Danish general practice as an urgent response to the COVID-19 pandemic. It now constitutes a permanent offer to patients, providing them with the opportunity to consult their general practitioner (GP) through audio-visual communication technology. Different digital healthcare technologies, such as video consultation, are often mentioned in political strategies as means to improve the Danish healthcare system, with the aim of increasing efficiency and better utilising scarce healthcare resources.1,2 However, implementing and using technologies require work from the healthcare professionals involved. Scholars within the field of science and technology studies (STS) have emphasised how the implementation of technologies is not merely a technical, plug-and-play process, 3 as often portrayed in policy strategies and public discourse, but also a social and organisational process. 4 Other scholars point to the invisible work, barriers and unintended consequences associated with the implementation of digital healthcare technologies in general practice.5–7 This underscores the importance of examining in detail what occurs in practice, and the consequences for healthcare professionals, when a new digital healthcare technology, such as video consultation, is introduced.
Following this perspective, our study explores what the implementation and use of video consultations imply workwise from the perspective of GPs and staff in general practice. We specifically aim to delineate the characteristics of the work undertaken by GPs and staff in implementing and utilising video consultation within their specific clinical contexts. By doing this, we seek to shed light on the processes and actual resources demanded from the GPs and staff in general practice to make video consultation practices work as part of their daily work life. This endeavour sheds light on the conditions under which video consultation is implemented and used and how these conditions might also relate to the choice not to use video consultations. We draw on 33 interviews with GPs and staff and 132 hours of ethnographic fieldwork conducted in seven general practice clinics in Denmark. In our exploration, we adhere to the sociological perspective of symbolic interactionism and specifically draw on the seminal work of American sociologists Susan Leigh Star and Anselm Strauss who mainly focus on types of work and sociotechnical practices in everyday life. They introduced the concept of ‘invisible work’, 8 which will be elaborated below. As will be evident, ‘work’ in this framework is not primarily physical or mental labour. It is rather all the efforts going into aligning symbolic meanings in a social context. 8 Thus, work should be understood as a social phenomenon, referring to people's actions and interactions with each other and with objects and technologies.
Healthcare, technologies and invisible work
The concept of invisible work by Star and Strauss has been applied in studies of computer-supported cooperative work (CSCW) to illuminate the frequently overlooked and undervalued work associated with collaborative activities, particularly regarding the use of technologies.8–10 It has also proved useful in studies of technology implementation and use in healthcare settings, where scholars have pointed out the often invisible, cooperative work between different professions and technologies. This includes the work of medical secretaries caring for patients’ records in hospitals, 11 radiologists interpreting patient data, 12 home care workers implementing new technologies, 13 care coordination tasks performed by nurses14,15 and the work of patients in handling complex information. 16 In this regard, some healthcare technology researchers have applied and refined the concept of invisible work in ways which we find particularly useful to draw on in our study, as described below.
Even though the concept has not been applied to studies of video consultations, we find the concept of invisible work interesting because it concerns work that is often taken for granted but is essential, for instance, in implementation processes. Defining what type of work counts as visible or invisible will always depend on the specific context, 8 and we work with the concept as a continuum with some types of work being more or less (in)visible than other types of work. In this regard, the creation of a ‘non-person’ is one node on this scale. 8 Here, the work is visible but the person doing the work is rendered invisible. Star and Strauss 8 explain how invisible work is often relegated to the background. A subcategory of invisible work is termed articulation work, defined as ‘work that gets things back “on track” in the face of the unexpected, and it can modify action to accommodate unanticipated contingencies’. 9 (p275) Articulation work involves making different assumptions and procedures work when there are no set rules among the parties. It includes ‘assembling, scheduling, monitoring and coordinating all the steps necessary to complete a production task’. 17 (p266) We find the concept of articulation work especially helpful regarding the implementation of video consultations, in part due to the special circumstances under which video consultation was introduced, namely as an acute solution to the COVID-19 pandemic. Because of this, standards and procedures for use occurred later and are still under development and not yet aligned between clinics, supposedly leading to a significant amount of articulation work in the clinics.
In relation to articulation work, organisational scholar Ninna Meier 18 applied this concept to describe the coordination of clinical managerial practice compared to clinical standards in different hospital settings. She explains how articulation work resembles ‘ad hoc coordination work’ which contrasts ‘planned coordination’. Ad hoc coordination work ‘refers to the unscheduled, real-time interactions of actors within an organization’. 18 (p68) Planned coordination, on the other hand, ‘may take the shape of rules, templates for work practice such as scheduled meetings, or standards for best practice’. 18 (p68) Using these concepts, Meier has demonstrated how both types of coordination exist, but to varying degrees, in the four hospital units she examined. She found that clinical managers perform articulation work to meet clinical standards and make the standards work in practice, especially in settings with high unpredictability. Hence, in Meier's study, the concept of articulation work proved helpful in understanding the relationship between plans and structures and what occurs in practice. This purpose aligns with our aim of understanding which type of work is needed in implementing and utilising video consultation in general practice, and we thus draw inspiration from her focus on visible and invisible coordination tasks.
Furthermore, professor of Science and Technology Studies, Nelly Oudshoorn applied the theory of invisible work in her study of patients’ use of an ambulatory ECG recorder, examining the work the patients had to do in producing a diagnosis at a distance. 19 Oudshoorn extended the concept of invisible work by introducing the subcategory of ‘inclusion work’ (originally described by Rommes 20 ) in her analysis. Inclusion work refers to the efforts done by healthcare professionals to turn patients into users of technology, such as video consultations. Additionally, Oudshoorn applied the subcategory of ‘affective work’ (originally described by Hardt 21 ), referring to emotional and relational dimensions of healthcare practices, for example, creating intimacy at a distance through video consultations. Whereas Oudshoorn focused mainly on the patients’ perspective, our focus lies on GPs and staff in the clinic. Nevertheless, we apply the terms inclusion work and affective work to the descriptions provided by GPs and staff regarding video consultations, because we find them helpful in deepening our understanding of the work characteristics and bringing forth the nuances of the work. By applying these terms and continuing these lines of thought, we aim at unravelling the complexity inherent in the work needed to implement video consultations in Danish general practice.
Study design and methods
Setting
In the Danish healthcare system, almost all services are financed by taxes. About 98% of Danish citizens are listed with a GP (often of their own choosing), and general practice is based on the ideal of continuity of care and a strong doctor–patient relationship.22,23 GPs own their clinics, either as single-handed GPs (27%) or in partnerships with other GPs (73%), 24 and in 2022 there were 3488 GPs organised in 1675 clinics in Denmark. 25 Besides the GP owners, the workforce in general practice consists mainly of employed physicians, GP residents, nurses, secretaries, social and healthcare assistants, biomedical analysts and medical students. As the Danish health authorities aim to move more healthcare tasks from hospitals to general practice, the need for more GPs and clinic staff has increased. While there is still a shortage of GPs, there has been a 20% rise in clinic staff since 2018, with nurses being the biggest staff group. 26 GPs work as private contractors and are remunerated by the public health authorities through a mixed capitation and fee-for-service system while staff are remunerated by the GPs with a monthly fixed salary determined according to their agreements. The system is based on a fee schedule covering each specific service. For example, a standard, in-clinic consultation is remunerated by the health authorities with DKK153.61 (per January 2023). 27
Video consultations were introduced in general practice in March 2020 because of the COVID-19 pandemic and the resulting societal lockdowns, hindering the majority of patients from attending general practice in-person. While a temporary reimbursement agreement was made between The Danish Organisation of General Practitioners (PLO) and the Danish health authorities in April 2020, the new collective agreement, which commenced in January 2022, confirmed video consultation to be a permanent offer in general practice. This means that general practices must offer video consultations to their patients by the end of 2024. The political reasoning behind this decision includes expectations of increased efficiency, optimised use of healthcare resources1,2 and wanting to meet patients’ wish of a more digital healthcare system. 28
The level of uptake of video consultation differs between clinics with some clinics using video consultation daily or weekly and others using it on rare occasions or not at all. As of December 2023, approximately 25% of the clinics do not use video consultations (personal correspondence with PLO). In some clinics, patients can book a video consultation through an online booking system while other clinics use the secretary as a coordinator for video consultation bookings. In 2022, video consultation accounted for 1% of all consultations in general practice. 29 Video consultation is accessed through the publicly developed and freely available software My Doctor. GPs and clinic staff access the software through a website, in most cases linked with their electronic patient record, and patients access the software through an application on their smartphone or through an SMS link sent by the clinic. As of April 2024, a video consultation is reimbursed with DKK160.72 equivalent to the fee for an in-person consultation. 30
Data sample
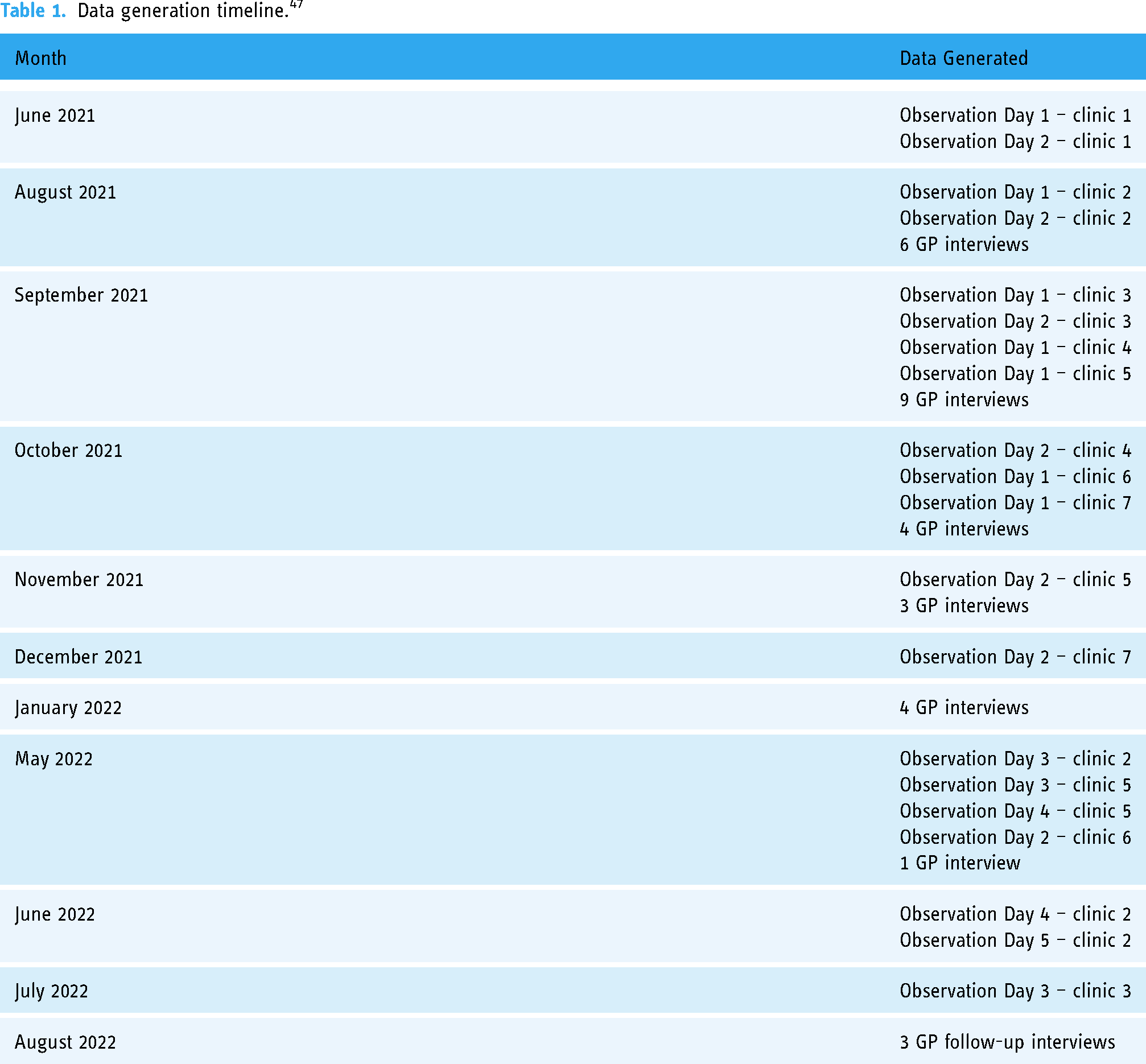
This is a qualitative, ethnographic study based on 33 semi-structured interviews with 27 GPs (including three follow-up interviews) and three clinic staff members. Additionally, 132 hours of multi-sited fieldwork was conducted across seven clinics and includes informal interviews with GPs and clinic staff. Data were generated between June 2021 and August 2022 (see Table 1) by female PhD student and MA in media studies ECL, who is trained in ethnographic methods and experienced in conducting interviews. Interviews and fieldwork were combined to the level of ‘information power’. 31 (p1754) This means we assessed the generation of data in the context of the study's aim and specificity, the quality of ECL's interactions with informants, data analysis methods and the application of theory. 31 Fieldwork and interviews were used to reciprocally contextualise the topic and inspire new interview questions and focus points during fieldwork.
Data generation timeline. 47
We used a purposive sampling strategy with the aim of ensuring the inclusion of a diverse spectrum of GPs and clinic staff, considering factors such as age, sex, geographical distribution, clinic size and frequency of video consultation use, spanning from no use to daily use, to cover diverse experiences and perspectives. While the focus of this paper is on the work done in relation to the implementation and use of video consultations, we argue that including non-users makes it possible to examine if there is a relation between the work involved and the choice not to use video consultations. We recruited participants through our professional network and social media platforms. Thus, some of the GPs were known to the author group, but most were new acquaints to ECL. The GPs and staff, aged between 35 and 71, were geographically dispersed across Denmark, representing clinics of varying sizes. Recruitment for interviewees and fieldwork clinics was executed in parallel. Some GPs agreed to an initial clinic visit by ECL, while others agreed to an interview. A few agreed to a visit or proactively invited ECL at the end of the interview.
ECL aimed at doing fieldwork in clinics of varying sizes and located in the different regions of Denmark because there might be differences in how the Regions structure and support general practice, for example, the degree of technical support and delivery of video consultation equipment. Moreover, there are geographical variations within the country, such as the densely populated capital region versus more sparsely populated regions with greater geographical distances and possibly poorer GP coverage. Likewise, ECL aimed at interviewing GPs across the regions. However, a GP in the North Jutland Region cancelled the planned interview because of workload. Due to this and an assessment of our information power, we ultimately represented four out of five regions in the country. We ended up conducting fieldwork in seven clinics because we assessed that these clinics together provided us with comprehensive insights into video consultations in relation to our study purpose.
Fieldwork
The fieldwork in the seven clinics focused on understanding how GPs and staff integrated (or chose not to integrate) video consultation into their workflows. The first clinic visit served as a pilot where ECL could test her fieldwork strategy and reflect on her focus and questions. ECL followed a multi-sited fieldwork strategy, which is suitable for discovering dynamics within and across different clinics by following a topic, namely video consultation, in different locations for shorter periods 32 (see Table 2). Thus, multi-sited fieldwork allows researchers to gain a broader range of perspectives compared to traditional single-sited fieldwork. As ECL aimed to establish a field that encompassed diverse video consultation experiences and would reflect the diversity of Danish general practice, the multi-sited fieldwork strategy was found to be well-suited. ECL adjusted her focus while doing fieldwork, following GPs on some days and clinic staff on other days to make room for different perspectives. She observed in-person, telephone and video consultations with patients as well as the preparation and summarising of journal work for each patient. Moreover, ECL followed the secretaries in the back office and at the front desk, observing how they perform a wide range of booking and planning tasks related to video consultations. ECL wrote jottings by hand 33 and transferred these to field notes, using Microsoft Word, upon her return from each fieldwork day. Additionally, ECL took photos of the clinics’ calendars to capture the formal structure of their work.
Fieldwork clinics.

ECL approached the observations as negotiated and interactive, meaning that what ECL could gain access to always rely on her specific interactions with the GPs and staff and the relationships she formed with them. 34 For instance, as ECL has a background in media studies, she could not participate in the clinical jargon and discussions. However, she could for the same reason pose questions that might not have occurred to a healthcare professional. On the other hand, because of ECL's background and her knowledge of technologies and video consultations, many informants asked for her advice and assistance regarding video consultations. ECL aimed at balancing being helpful by answering questions and engaging in conversations about video consultations while also trying not to let her knowledge or opinions overshadow and affect those of her informants. Not least, as ECL became more acquainted with the work in the clinics, she assisted with practical tasks such as greeting patients in the reception and handling blood and urine samples, but always kept a distance to more complex tasks where the knowledge of a trained healthcare professional was needed. Thus, we acknowledge that knowledge production is situated 34 and dependent on the researcher's background and personality.
Interviews
Interviews (see Table 3) focused on how GPs and clinic staff experienced the introduction of video consultation, including how video consultations affected their organisational practices and work processes. The interview guide included questions such as: ‘What does it require of a GP [or other healthcare professional], in your opinion, to use video consultations?’, ‘Has the use of video consultations brought about changes in your clinic? If so, which?’ and ‘Who is involved in deciding or assessing in which situations you can use video consultations in your clinic?’ The interview guide was tested on a nurse colleague and a GP colleague. ECL conducted interviews either on video (n = 21), by telephone (n = 6) or face-to-face (n = 6). The video interviews allowed ECL to connect with the context of video consultations, with most GPs participating in interviews at the very location where they conduct video consultation. This fostered a shared, embodied understanding of the interview subject. To ECL's knowledge, other people were not present doing interviews. Interviews followed a semi-structured interview guide with room for adjustments during the data generation period. They lasted between 21 and 74 minutes and were audio- or video-recorded. Interviews were transcribed verbatim by ECL (n = 9) and a student assistant (n = 24). Transcripts were not returned to informants for comments or corrections but discussed in the author group, which also includes a GP, and with GP colleagues.
Interviews with GPs and clinic staff. 47

Data analysis
In our analytical process, we employed Braun and Clarke's reflexive thematic analysis (2006; 2020) because it offers theoretical and interpretative flexibility, analytic reflexivity and depth, which are all characteristics we find suitable when working with our complex and rich ethnographic data. Following this approach, the transcripts were initially read and re-read by ECL and EAH, while ECL took notes along the way using the ‘annotations’ feature in CASDAQ software NVivo (version 14) and by hand. Afterwards, still using NVivo, ECL coded the data inductively and searched for ‘patterns of shared meaning’ 35 in an iterative and organic process that included discussions with EAH about minor and major potential themes, such as collaboration, the prioritisation of tasks, assisting patients and workload in the clinic. In this process, we were also inspired by abductive analysis, looking for surprising findings and going with ‘where the data is strongest’. 36 In this process, we sought theoretical frameworks within the field of science and technology studies and organisational studies that could refine the analytical focus and support our understanding of the details of the use and implementation of video consultations in relation to work processes and organisational practices. The concept of invisible work proved helpful in this pursuit because it offers a theoretical lens through which to gain a deep and nuanced understanding of the characteristics of the work needed to use video consultations. Consequently, we used this theoretical concept to further sort our data, and this analytical process resulted in four themes representing four types of invisible work: (1) the work of introducing video consultations, (2) the work of stabilising video consultation use, (3) the work of coordinating users and systems, and (4) the work of repair as a response to breakdowns. Informants did not provide feedback on the findings, but the findings were discussed in the author group. In line with reflexive thematic analysis, we acknowledge that our findings are our interpretive constructs and do not represent an objective reality. 35
Ethical considerations
The institutional board of the University of Southern Denmark, the Research and Innovation Organisation, approved the study (approval number 11.401). ECL introduced the research aim and procedure to participants before each interview or observation and presented her interest in the research topic as well as her professional background and employment affiliations. Participants were informed that participation in the study was voluntary, and all participants gave written consent.
Results
Below, we describe four types of work related to the use of video consultations. An overview of the findings is presented in Table 4.
Types of work related to video consultation use.

The work of introducing video consultations
In the following, we delineate the inclusion work performed by GPs who have taken on the role of IT-responsible in their clinic. Analytically, these GPs can be described as ‘implementation agents’ which refers to their roles as resource persons who support others in becoming good implementers of video consultations. 13 The work performed in this regard is crucial in turning colleagues into video consultation users.
In most clinics, one GP assumed the role of IT-responsible. The decision often rested with the group of GP clinic owners who selected the most suitable GP based on individual interests and competencies in handling IT. For example, one GP expressed curiosity about video consultations, stating, ‘I think it is fun, and I like general practice, so if there are different consultation forms, I believe you should try them out to see how they work’ (GP14). In many cases, the clinic already had an IT-responsible GP before introducing video consultation, making it a natural extension of their responsibilities. In other instances, clinics lacked a clearly defined role or designated IT-responsible person prior to video consultation implementation. However, they specifically appointed a GP to handle video consultations when they were introduced. Initiating video consultation use required a clinic owner with decision-making authority, i.e. a GP, to take on this responsibility. As one GP explained: ‘If you as a GP don’t take it upon yourself and say “we have to implement this” then it won’t happen’ (GP43). This sentiment resonated with staff members across various clinics, who relied on their IT-responsible GP for guidance and expertise in using the technology. Although colleagues and staff often witnessed the IT-responsible GP's efforts, they did not always fully grasp the extent of their work.
To conduct a video consultation, the IT-responsible GP needed to acquire and install video cameras, speakers and a microphone. These devices were often provided by the Region, unless already integrated into the clinic's computers. GPs and staff used their medical practice number to log in and access the video consultation software via a website. Most electronic health records included a built-in link to this website, allowing users to click a button and connect directly. Setting up the video consultation equipment and software primarily involved procedural and practical tasks. 19 The Regions and the PLO often provided ‘how to’ videos and guidelines, 37 turning the work into visible, planned coordination work. 18
In addition to planned coordination tasks, the IT-responsible GP actively worked on including relevant colleagues and staff in video consultation use. However, maintaining consistent video consultation usage over time posed challenges in many clinics. The IT-responsible GP had to repeatedly remind and encourage colleagues, staff and patients to book and use video consultation, ensuring their involvement in the implementation process and fostering confidence as competent video consultation users. Regular discussions during weekly or monthly meetings helped align everyone on the clinic's video consultation practices. Given changing rules in 2020, 2021 and 2022, the IT-responsible GP played a crucial role in keeping everyone informed and adjusting video consultation use as needed. A field note demonstrates this difficulty. Despite the IT-responsible GP's ambitious efforts, disagreements arose within the clinic regarding video consultation prioritisation when ECL visited them approximately 1.5 years after the initial introduction of the technology: The IT-responsible GP tells me he had asked the secretaries to offer patients video consultations whenever they find it suitable and as much as possible. However, when I talk to the secretaries later that day, they do not all agree on this fact. While one secretary still tries to book many video consultations, another secretary tells me how she has not been reminded to book them at all. Instead, she has been reminded by a different GP to book telephone consultations for all chronically ill patients. Thus, this – and not video consultations – is her focus now. Additionally, when following a GP resident who has been employed for a few months, he tells me that he has not been informed about the clinic's use of video consultations. Since he has no experience in using them nor any interest, he would never book a video consultation himself. (Excerpt from field notes, clinic 6)
This field note demonstrates how the IT-responsible GP believed he was fulfilling necessary tasks, but in reality, his efforts were ineffective. Viewpoints on video consultations sometimes diverged among clinic staff. Despite this, the IT-responsible GP remained a central figure during the initial implementation of video consultations, as acknowledge by colleagues. Nevertheless, this theme demonstrates how maintaining the clinic's use of video consultation demands continuous inclusion work that not all IT-responsible GPs succeed in. Furthermore, continued video consultation use relies on another type of work, performed by the secretary, as will be described in theme 2.
The work of stabilising video consultation use
In the following, we characterise the articulation-, inclusion- and affective work related to video consultation use that was delegated to the secretary.
While the IT-responsible GP initially introduced video consultations, the secretary coordinated and booked these appointments, taking on the role of what we analytically term a ‘stabilisation agent’. Moreover, the secretary repeatedly instructed and assisted patients in using the technology. Becoming a stabilisation agent was often a role assigned to a secretary who closely collaborated with the IT-responsible GP. In some cases, the role was formally delegated by one or more GPs. However, in most instances, the secretary assumed this role informally, taking on tasks related to video consultation use without explicit articulation of a formal new position.
The task of a secretary in managing video consultations was, roughly put, twofold: Firstly, they scheduled video appointments and coordinated everyone's calendars. This work involved, to some degree, visible, planned coordination tasks, 18 but also consisted of ad hoc articulation work. 18 Secondly, the secretary guided patients in using video consultations, which consisted of inclusion and affective work. 19 While several GPs acknowledged these tasks, the extent of the work did not seem to be visible to all GPs and colleagues, nor was it explicitly discussed within many clinics. In this way, the role of the secretary differed from the IT-responsible GP because the latter took on a more visible role in inspiring and leading the way for colleagues and staff. Nevertheless, the work performed by the secretary was crucial if the clinic was to succeed in transforming the initial implementation efforts to routinised, stable use of video consultation.
The role of the secretary was typically fulfilled by a trained medical secretary, a nurse or a health and social care (HSC) assistant. While some GPs, nurses and HSCs scheduled video consultations themselves, typically by the end of an in-person consultation, it was more common for secretaries to handle this task. In this regard, several GPs explained how implementing video consultation demanded more ‘bread-and-butter work’ (GP13) from the secretaries than from any other person in the clinic because booking video consultations and introducing them to the patient was a time-consuming task. This task increased the complexity of the coordination work done by the secretary because another option was added to the existing portfolio of consultation forms (primarily) managed by the secretary. Some secretaries considered the new responsibility a natural part of their duties and did not find it significantly time-consuming. Conversely, others felt confused and stressed, perceiving video consultations as an additional workload. The divergence in perception highlighted varying boundaries within the secretary role. Although most GPs acknowledged the secretaries’ increased workload, not all fully grasped the daily impact on them. For instance, a GP resident humorously remarked that ‘all the secretary does is pick up the phone’ (field note excerpt, clinic 7), while another GP commented that staff, including secretaries, were always ‘afraid of change’ and ‘fear that they have to do more for the same salary’ (GP4_P2). This could indicate that secretaries performed work that was not only invisible outside the clinic but also taken for granted by (some) colleagues in the clinic. While the results of their work were visible, in the form of a well-organised calendar, the secretaries were rendered more invisible even though they enabled these results.
Moreover, as with the IT-responsible GP, the work related to video consultation use was not compensated with tangible benefits such as additional pay or time set aside for this specific task. However, while the GPs at the time of the study received a higher reimbursement fee for each video consultation, compared to other consultation forms, the staff's monthly salary did not change. Hence, the conditions and motivation for spending time implementing and using video consultation differed for the staff compared to the GP clinic owners.
In clinic 5, the IT-responsible GP collaborated with a secretary to manage the clinic's use of video consultations. While the GP initially introduced video consultations, as explained in theme 1, the secretary led the ongoing coordination task, performing articulation work. For instance, every morning, the secretary logged into the virtual waiting room and reviewed everybody's schedules to identify consultations that could be converted to video appointments. If the secretary believed this was feasible, he contacted the GP or colleague, who had the patient in their schedule, and asked permission to inform the patient that the consultation had been converted to a video format (on the condition that the patient agreed). The secretary's assessment of when to convert a consultation to video was informed by his own experiences in using video consultations and his collaboration with the IT-responsible GP. This example illustrates how effective and continuous collaboration between the IT-responsible GP and the secretary facilitated the transition from initial implementation to habitual, routinised use of video consultations.
The work of making video consultations habitual and sustainable also included inclusion and affective work performed by the secretary who had to encourage the clinic's patients to become video consultation users. When proposing a video consultation to a patient, the secretary needed to consider if the consultation was appropriate for video consultation use (e.g. if a physical examination or specimen collection was needed), if it fitted the GP's preferences and if the patient could conduct a video consultation. On a fieldwork visit to clinic 4, ECL observed how a secretary tried to take these aspects into account, balancing the interests of the GP and the patient. The secretary took a call from a patient which ended with the secretary giving the patient a telephone appointment with a GP. After ending the call, the secretary shared some considerations with ECL: I hear S10 ask a patient on a telephone call: ‘What about a video consultation, would you be up for that?’ After a few seconds, the secretary tells the patient that she will ask the GP to call the patient by telephone, and I assume the patient turned down her video offer. When the secretary hangs up, she confirms my anticipation, and she explains how they are not allowed to book telephone consultations but must always try to book video consultations. However, this patient has earlier on experienced some problems and misunderstandings in their communication with the clinic. Because of these bad experiences, the secretary did not want to try to persuade the patient to use video consultations. In other cases, she would always try to make the patient agree to do a video consultation if it makes sense. However, many patients are upset about having to do video consultations for the first time. Typically, though, after completing their first video consultation, they realise that the consultation form is not that bad an idea and they become keen on using it again. S9 now interrupts our conversation. She explains how sometimes a telephone consultation is absolutely sufficient to meet the patient's need, but because the GPs are paid more for a video consultation, the secretaries have been asked to prioritise this consultation form when booking appointments. (Excerpt from field notes, clinic 4)
In this situation, the secretary considered the patient's prior experiences and decided not to challenge the patient after the patient declined a video consultation. Despite knowing that this decision contradicted the GPs’ preferences, she believed it would have a negative impact on the clinic–patient relationship. This highlights the affective dimension of managing video consultations, where secretaries navigate conflicting pressures based on varying intentions, needs and preferences. The secretary faced the challenge of handling patients who initially felt negatively about video consultations, often upset at having to use this technology. This affective work added to the existing burdening work of dealing with unsatisfied and frustrated patients due to long appointment wait times (regardless of consultation type). Across clinics, secretaries mentioned that this aspect of their work could be emotionally draining.
In another case, the secretary routinely prioritised video consultations as instructed by the GPs. During a telephone conversation with a patient, she initially offered a video consultation. However, upon reviewing the patient's record, she realised the patient needed to visit the clinic for new blood samples. She promptly adjusted the appointment to an in-person consultation and informed the patient. Such situations required the secretary to maintain an overview and assess the suitability of different consultation forms, especially when patients were unaware of specific requirements.
Hence, this theme demonstrates how the secretary plays a vital role in video consultation use and often serves as the gatekeeper, controlling the use of different consultation forms in the consultation ecology and turning patients into video consultation users.
The work of coordinating users and systems
In this theme, we delineate the articulation work carried out by GPs and staff in the clinic to be able to use the video consultation software.
When implementing and using video consultations, coordination was essential not only between GPs and staff but also between users and specific systems – the virtual waiting room and the clinic's appointment and scheduling system (integrated with the electronic patient record (EPR)). Analytically, these systems can be described as ‘boundary objects’
38
because they serve as central artefacts through which GPs, nurses, secretaries, etc. coordinate their use of video consultations. All GPs and staff needed clear visibility when an appointment was booked as a video consultation to avoid mistakes and misunderstandings with patients and colleagues, so-called ‘breakdowns’.
39
Thus, the boundary objects support what in organisational studies is termed the ‘distributed work’ of GPs and staff, meaning these objects allow them to continuously coordinate their work even though they are not always physically together (as they are often attending to their respective patients in separate consultation rooms).
40
However, our findings revealed diverse approaches to working with these systems, with users often inventing ‘workarounds’ to overcome perceived barriers in the workflow.
41
These workarounds, akin to ‘user appropriation’,
42
reflect users’ active adaptation of technology to meet their needs. In summary, significant articulation work occurred in managing video consultations. For instance, ECL observed how an HSC settled a video consultation after the patient left the surgery: HSC10 starts by using a shortcut and a list of billing codes appears on his screen in the electronic patient record. A billing code for a video consultation does not appear on the screen. HSC10 clicks on the billing code for ‘telephone consultation’. Subsequently, he clicks on the box again and overwrites the telephone consultation billing code by manually writing the billing code for a video consultation in a small input field. A pop-up box appears, asking if he is sure he wants to overwrite the billing code. He clicks ‘yes’, and the pop-up box disappears. I ask HSC10 why he is doing it this way. He replies that there are no other ways of using the software when wanting to settle a video consultation. He hasn’t given it much thought, but now that I point it out, it makes him consider if he should notify the software provider of this missing shortcut. Maybe they can add it to the next system update, HSC10 considers aloud. (Excerpt from field notes, clinic 5)
This field note excerpt demonstrates how staff routinely employed workarounds and adjusted their system usage for video consultations. These adaptations became ingrained in their daily workflows, often going unnoticed. Consequently, these actions constituted a form of invisible work – so subtle that even the individuals performing them rarely acknowledged their significance until ECL brought it to their attention.
In other instances, missing software functionalities led to confusion among the GPs and staff because they used the software in various ways which could ultimately lead to misunderstandings and mistakes affecting their patients. For example, a secretary in Clinic 6 explained how there were different ways of booking and registering a video consultation in their appointment and scheduling system: N5 shows me their calendar, and we sit together and look at how many video consultations are currently on the calendar across the various GPs and nurses. N5 shows me that the blue fields indicate video consultations. She clicks on a video consultation and shows me the pop-up box with further information. ‘You can book a video consultation in different ways’, N5 explains, and she continues ‘I usually start by writing VC in the comment field here, so I'm sure it won't be overlooked. But really, it should be enough to paint it blue. And otherwise, you can mark with a V here’, says N5 and points to a small box with the text ‘video consultation’ next to it that you can tick off. She explains that this box has not always been there and that this may be why she continues to write VC in the comment field. N5 closes the box and scrolls through the calendar, while we both look for video consultations in the daily programs. N5 stops clicking, points to the screen and says ‘look, here is a video consultation, because it says V. But it is not made blue. Indeed, it should be’. I tell N5 how I am surprised by the many ways they can register a video consultation. To this she nods and answers ‘yes’ and adds that ‘so many things happen all the time, making it difficult to keep track of everything’. (Excerpt from field notes, clinic 6)
This field note illustrates how GPs and staff had to coordinate and interact with each other using the appointment and scheduling system, serving as a boundary object that, despite local adaptions and workarounds, supported collaboration between GPs and staff. However, to avoid misunderstandings and breakdowns, GPs and staff had to adapt to the system's design and reach a consensus on the symbols used to indicate video consultations. Given that both the appointment and scheduling system and the rules governing video consultation use have undergone multiple changes since their introduction in 2020, there was ongoing articulation work to align the distributed work of users and their interactions with and through the appointment and scheduling system.
The work of repair as a response to breakdowns
In this theme, we characterise the articulation and inclusion work performed by GPs and staff when their attempts to include patients (as described in theme 2) and coordinate users and systems (as described in theme 3), were unsuccessful, resulting in breakdowns.
Across various clinics with differing levels of video consultation usage, instances of unsuccessful video consultations occurred. When a video consultation did not proceed as intended, GPs, staff and patients collaborated to find alternative ways to complete the consultation. This necessitated invisible articulation and inclusion work.
19
For instance, in Clinic 2, a GP had five scheduled video consultations one morning when ECL visited. Unfortunately, none of these video consultations unfolded as planned: At 9 o’clock, I meet GP4 in his surgery. Today, he has five video consultations scheduled. Before the first video consultation, a mother with a young child has booked a physical appointment. To ensure the virtual waiting room appears open on patients’ applications, making it possible for them to log in and be ready for the video consultation in due time, GP4 logs in before commencing the physical appointment. Moreover, he sends an SMS to the first video consultation patient, indicating that he will soon be ready for the consultation. We then proceed to fetch the mother and child from the physical waiting room. Despite calling the patient's name twice, there is no response. GP4 speculates that the child may have recovered and therefore not turned up. Back at his computer, he opens the calendar and clicks on the second video consultation. As with the first video consultation patient, the GP also sends an SMS to this patient. After waiting for a couple of minutes, still no patients appear in the virtual waiting room. GP4 sends similar SMS messages to the next two patients, yet no one shows up. When he sends an SMS, he marks the patient with a green colour so that his colleagues can see that he is doing this consultation. If he doesn't mark the consultation, it might be that a colleague thinks he is behind schedule, and wanting to help him, the colleague moves the patient to their calendar. Suspecting a software issue, GP4 now logs out and back in, but the waiting room remains empty. He then calls the first video consultation patient, who had forgotten the appointment. GP4 suggests rescheduling for next week as too much time has now passed for the GP to do the consultation instantaneously. When the next patient doesn’t answer the phone, GP4 emails them instead. GP4 tells me that he assesses if and how it makes sense to contact the patient and when to not make more of it. In this case, it was a patient with some mental problems, and GP4 says: ‘I'm just writing to him to let him know he's not completely alone in the world’. (Excerpt from field notes, Clinic 2)
This field note demonstrates the breakdown of the working infrastructure, that is, the human organisation of the GPs, staff and patients. 39 In response to this breakdown, the GP engaged in repair work, referring to the subtle acts of care to restore order and fit the circumstances of the system and the patients. Thus, repair work constitutes a facet of articulation work. 43 The GP's approach involved addressing both patients physically present in the waiting room and those in the virtual waiting room. Simultaneously, the GP considered potential software bugs and individual patient needs. When the planned video consultations could not proceed as intended, the GP turned to alternative communication channels, such as telephone and e-mail consultations, to reach the patients. This ad hoc plan B was based on a situational assessment of what would be most suitable. In managing these five video consultations and the physical appointment, the GP weighted emotional, practical, technical and organisational consequences. The GP's actions illustrate the adaptability, tolerance and mental surplus required to integrate video consultations into their schedule effectively. While mistakes and misunderstandings are common, the strategies needed to handle them often remained invisible and were rarely discussed in the clinics.
Additionally, patients sometimes felt uncertain about their appointments and required assistance from the GP or staff to successfully navigate future video consultations. This led the GP or (typically) staff to continue the inclusion work they had initiated during the initial introduction of video consultations to the patient. Occasionally, patients forgot or misunderstood that their appointment was scheduled as a video consultation, resulting in their arrival at the clinic. While GPs and staff generally explained that this was not a problem, they often spent additional time doing inclusion work at the end of the in-person consultation, addressing any misunderstandings or insecurities the patient might have had, preparing them for the next video consultation. In some cases, the GP or staff proactively planned for contingencies. For example, an HSC noted in the EPR that the planned video consultation might need to be converted to a telephone consultation if the patient encountered difficulties with the video consultation software (fieldwork, clinic 5). In another case, the HSC agreed with a patient that she could call the clinic if she changed her mind and preferred an in-person visit instead of the planned video consultation (fieldwork, clinic 5). In such situations, the staff aimed to encourage patients to use video consultations while ensuring their comfort and safety, taking into account their feelings and the patient-clinic relationship. They drew on their knowledge of the patient, including their consultation preferences, technological proficiency and whether they had relatives who could assist them with the video consultation application.
Considering these factors, a one-size-fits-all approach for a plan B is not feasible faced with uncertainty or deviations from the original plan. While the telephone is commonly suggested as an alternative to video, the reality is more nuanced. The work described in this theme emphasises the importance of individualised assessments for each patient, necessitating a mix of articulation, inclusion and affective work. This approach, which includes knowledge of the patient's unique situation, supports the relationship-based model of care in general practice. 44
Discussion
In this study, we have illuminated some of the ‘black box’45,46 elements tied to work processes that emerge in connection with video consultation implementation in general practice in Denmark. Using Star and Strauss’ concept of work, we delineated four types of work each of which was embedded alongside existing organisation activities: (1) the work of introducing video consultations, (2) the work of stabilising video consultation use, (3) the work of coordinating users and systems, and (4) the work of repair as a response to breakdowns. These different types of work all demonstrate how implementing and (especially) securing sustained and, to some extent, stable use of new technologies presuppose and entail single efforts from individual members within the organisation in question that, if successfully coordinated, lead to uptake and continued use of the technology. Our findings thus show that video consultation is implicated in relational networks of human and non-human actors, in our case of GPs, staff and technology carrying out work that is crucial in making video consultation come into being. In that sense, our study exemplifies and supports a sociomaterial approach to studying technologies as phenomena ‘emerging within a densely interconnected assemblage of actors, actions, and relationships’. 45 In our study, we have provided examples of how these assemblages have affected use of video consultation. However, and as described elsewhere,45,47,48 the alignment between people and technologies might fail somewhere in the process towards stabilisation, and in some instances even before initial implementation. In a recent study, 47 we have described how, in these clinics, the work needed to succeed in using video consultation is not performed and, consequently, the GPs and staff become non-users. Taken together, our findings on processes effecting use and non-use of video consultation demonstrate that implementation of video consultation is a porous context since technologies, following Nicolini, 45 ‘…are in fact a (more or less) stable assemblage of a variety of material and human elements’.
Our results also align with existing sociomaterial research that emphasises how implementing new technologies leads to a reconfiguration and transformation of professional roles and existing work practices.13,45,49 For instance, the GP's role as a medical doctor is reconfigured into additionally comprising the role of an implementation agent (theme 1). Moreover, the role of a stabilisation agent (theme 2) is being embedded within the secretary's professional work tasks and role. Hence, the technology is not merely integrated into existing workflows but changes the organisational structure, a theme that has been dealt with at length in organisational studies of technology implementation under the notion of ‘boundary work’, signifying how individuals and groups engage in a process of continuously defining what does and does not belong to their areas of expertise and responsibilities. 50 Regarding the secretary becoming a stabilisation agent, other healthcare technology scholars11,51,52 have challenged the widespread anticipation that the medical secretary performs simple routine work, similar to our example of a GP resident believing that a secretary's job is only to answer phone calls. Their empirical studies of the implementation of an electronic health record at two hospital departments in Denmark have shown how not acknowledging the importance of the secretaries’ (invisible) work led to replacing the secretaries with a new IT system, which ultimately led to critical breakdowns in the hospital's work arrangements. Our study adds to this knowledge by describing the crucial – but to some degree invisible – role of the secretary concerning the general practice clinics’ successes in video consultation use.
As is especially evident in our themes 3 and 4, the movement towards stable use of video consultation is far from a linear trajectory from introduction, diffusion and uptake, a narrative that is too often associated with technology implementation. 13 Besides articulation work, the work performed by GPs and staff who are experienced and competent video consultation users also consists of inclusion and affective work when they try to motivate colleagues and patients to use video consultation and make them feel secure and competent in their use. These findings support Ertner's 13 point that implementation of technology includes affective work, pampering and motivating, directing our attention to how crisis (e.g. pandemics) and political pressure only work as motivational factors for technology implementation to a certain degree. Located incentives and efforts in the clinic are needed to make video consultation use successful. Moreover, the work required towards implementation of video consultation also includes allocating time to do workarounds and repair breakdowns. Related to this, Ziebland, Hyde and Powell6 describe how awareness of unintended consequences of the use of digital health technologies ‘can help to balance a promissory discourse of digital health’. Similar to our findings about some staff members’ feelings of increasing stress due to the introduction of video consultation (theme 2), Ziebland, Hyde and Powell describe how staff can develop a pessimism about digital innovations when they experience technology failure. Not least, they argue that accounts of unintended consequences can be used for reflection and learning in organisations. Based on our findings, we agree that elucidating the work carried out by GPs and staff is helpful in developing future approaches to the implementation and use of healthcare technologies such as video consultations.
Generally, we wish to challenge the political habit of setting quantitative targets for the use of video consultations (as seen in some hospital settings, e.g. 53 ) and, as also emphasised by Marent and Henwood, 46 promoting digital health per se. We are sceptical of this approach because our findings demonstrate how the use of video consultation evolves dynamically in each individual clinic and is situated in everyday settings where different practicalities, agendas, priorities and goals influence how video consultation is used. Our findings, enabled by our ethnographic fieldwork, support the argument that to better understand digital transformations in general practice, as well as in other healthcare settings, research is needed that elucidates technologies-in-use and connected hereto, the actual non-linear work performed by healthcare professionals in local practice settings. This will at the same time give an insight into the collaborative and organisational consequences and time spent on implementing and using new technology which might lead to a more nuanced and reality-checked dialogue about the ‘promises’ of new digital technologies in healthcare. We suggest that political stakeholders as well as GPs and staff consider and accept the fact that it takes time to implement and integrate video consultation into (new) routines and workflows. Regressions are part of the process and should not be perceived negatively but rather as valuable learning experiences. In this regard, continuous evaluations of video consultation use from ‘real-world’ contexts would be helpful in further developing the technology and the political goals regarding video consultation spread and scale-up.
Strengths and limitations
This study is, to our knowledge, the first ever to examine the characteristics of the work undertaken by GPs and staff to implement and use video consultations. This study was conducted at an interesting time with increasing focus on the use of digital technologies, moving towards the point where all clinics must offer video consultations. Our qualitative method, consisting of interviews and ethnographic fieldwork, led to novel insights into what actually happens in the clinics when video consultations are introduced and applied. It sheds light on the ad hoc work often invisible and hence not taken into account or articulated by political decision makers. Moreover, bearing in mind the 20% increase in clinic staff in general practice, as mentioned earlier, we see it as a strength that the various staff positions have been included in the study. We believe it to be a strength of the study that we have included a diverse range of clinics, representing both large clinics with more than 20 employees, solo clinics and clinics in between.
While the period of the data collection was interesting, things could potentially have changed since, considering the fast technological developments. Thus, follow-up studies would be useful. However, looking at the level of video consultation use there are no clear signs that clinics have changed their way of using video consultations. Likewise, the technology has not changed significantly, but there might be relevant changes in the future to consider in new studies. Not least, this study only represents GPs and clinic staff. Of course, patients play a crucial part in understanding how video consultations are used. Specifically, our results show how video consultations sometimes go wrong, triggering more articulation, inclusion and affective work. In relation to this, it would be valuable in future studies to include the perspective of the patients (and perhaps their relatives), sitting at ‘the other end’ of the video consultation.
Implications for practice
By making the invisible work visible and demonstrating the division of tasks, as done in this study, it might be possible for GPs and staff to critically evaluate and adjust workflows and strengthen coordination. We believe acknowledging each other's (invisible) work can strengthen the collaboration and coordination of video consultation use in the clinics. In this regard, our findings demonstrate how training across all functions in the clinic would be valuable, and we specifically suggest paying more attention to the secretaries’ tasks. We have emphasised the need for more training before, 47 and other researchers similarly highlight the vital role of training, including whole-team training. 54 Moreover, this study can provide feedback to developers of software related to video consultations, helping to improve their user-friendliness . Moreover, stakeholders involved in policies and collective agreements can use our findings to qualify their assessments of whether GPs’ and staff's work efforts are reflected in reimbursement schemes and match political goals related to video consultations. Finally, this study highlights the importance of patient education, and it can be used to discuss alternative approaches beyond relying on clinic secretaries to manage patient expectations and insecurities concerning video consultation use. The affective aspect of the work, as our study also demonstrates, shows that it is important to adopt a respectful approach towards patients when they are learning to use video consultations. This should also include a consideration of why some patients might be reluctant to use video consultations. Similarly, this study contributes to a greater understanding of human–technology relations and emphasises that the implementation and use of video consultations require a significant amount of work.
Conclusion
In this study, we departed from Star and Strauss’ sociological concept of work to delineate the characteristics of the work undertaken by GPs and staff to implement and use video consultation in their specific clinical contexts. We demonstrated that video consultation is implicated in relational networks of human and non-human actors, in our case of GPs, staff and technology, carrying out work that is crucial in making video consultation come into being. The video consultation changes the organisational structure and leads to a reconfiguration and transformation of professional roles and existing work practices. This becomes especially evident in our description of an implementation agent and a stabilisation agent. Moreover, implementing and using video consultation demands articulation, inclusion and affective work by GPs and staff, and this work includes allocating time to do workarounds, solve misunderstandings and repair breakdowns. Our findings demonstrate how the video consultation is situated in everyday settings where different practicalities, agendas and goals influence how the video consultation is used. Even though GPs and staff might have the best intentions of using the technology, their use might be slowed down or stopped because of these everyday circumstances and disruptions. Thus, the video consultation must show its worth among other systems, tasks and priorities for providing good care for the patients in the busy clinics. Following this, our findings support the argument that implementing technologies, such as video consultation, is a non-linear process which can best be understood by exploring the technology as a social phenomenon unfolding in the real-world situated settings of Danish general practice.
Footnotes
Acknowledgements
We wish to thank all participants in the study. We also wish to thank student assistant Emely Ravn for transcribing interviews.
Contributorship
ECL generated all data material and researched literature. ECL and EAH conceived the manuscript design. ECL wrote the first draft of the manuscript with help from EAH. All authors contributed iteratively with adjustments and supplements to the manuscript, discussed the theoretical approach and the findings, and reviewed and approved the final version.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The institutional board of the University of Southern Denmark, the Research and Innovation Organisation, approved the study (approval no. 11.401).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by University of Southern Denmark, Sygeforsikringen Danmark (2020-0117) and the Research Fund for General Practice (1398791).
Guarantor
ECL.