
Abstract
Background
Group psychotherapy is an effective treatment for postpartum depressive and anxiety symptoms, and interpersonal connection and support through the group process can aid recovery. Little is known about the implication of the delivery of interpersonally oriented group therapy in this population through videoconferencing.
Objective
To pragmatically evaluate the implementation of a conversationally-oriented postpartum videoconferencing psychotherapy group for depression and anxiety within the clinical setting.
Methods
Over 8 weeks, five to six patients and one therapist facilitator (closed group) meet weekly for 1 hour via a secure videoconferencing platform. We evaluated group adoption metrics for all postpartum videoconferencing psychotherapy groups offered during the evaluation period (October 2021–August 2022), and offered patients the opportunity to complete baseline and post-group quality improvement surveys to evaluate outcomes including acceptability (Satisfaction with Therapist and Therapy Scale-Revised, STTS-R), group process (Group Questionnaire, GQ), and effectiveness (Edinburgh Postnatal Depression Scale, EPDS).
Results
Of 153 patients (n = 26 groups), most (72.5%) attended >70% of group sessions. Of 137 patients (n = 24 groups) who were sent surveys, n = 50 (36.5%) completed both baseline and post-group surveys. Mean (SD) ratings were high for acceptability (STTS-R-therapy: 25.0/30 (3.1); STTS-R-therapist: 27.6/30 (2.3)) and group process with GQ ratings of 81.4/91 (7.8) (positive bond), 34.1/56 (3.8) (positive working relationship) and 23.5/63 (4.4) (negative relationship). Patients with probable depression (EPDS ≥ 13) significantly decreased from n = 23 (50%) to n = 19 (41.3%, p < .001), although the absolute score difference was minimal.
Discussion
Videoconferencing-based group therapy can be implemented with a robust group process and acceptability in the postpartum period. Impact on clinical outcomes should be further investigated.
Introduction
Symptoms of postpartum depression and anxiety affect 15–20% of new mothers and birthing parents.1,2 Effective treatments exist, yet as few as one in 10 of those in need of treatment are able to access them, 3 leaving mother and child vulnerable to the effects of untreated illness. Psychotherapy, with or without medication, is a first-line treatment option for depression in the postpartum period and can be effectively delivered individually or in a group setting.4,5 Participants in group therapy benefit from opportunities to engage in shared learning,6–8 modelling others’ behaviours, 7 normalizing experiences, 8 and improving social support. 6 In the postpartum context, an often isolated and lonely period, social and peer support from group therapy may have compounded benefits.9–12 Group therapy also offers health system advantages, including cost effectiveness6,7 and resource efficiency.13,14 Feasibility of in-person group therapy is limited by low attendance,8,15 with high attrition among new mothers attributed to barriers such as childcare,16–18 transportation,17,19 and scheduling constraints.16,18
Due in part to pandemic-related restrictions on in-person services, there has been a growing use of group therapy delivered via videoconferencing. The available literature on videoconferencing therapy groups shows that they trend towards improved clinical outcomes, both in the postpartum period20–23 and in others,24–27 and that there are acceptable levels of satisfaction and feasibility24,25,28,29 in varied populations. We also observe that there are knowledge gaps related to group process outcomes for therapy delivered through this modality. In the general population, the evidence on the positive and negative impacts of the videoconferencing modality on group processes is highly varied25,26,29 and to our knowledge this has not been specifically examined in the postpartum context. There is some evidence around the value of interpersonal support from peers in a videoconferencing context. 22 Given the importance of social support in the postpartum period, generating knowledge of how conversational and socially oriented group therapy programs can be delivered through videoconferencing may help us understand how they can be leveraged to address gaps in care in this population. Finally, most literature is focused on the use of videoconference-based group therapy as a scientific exercise or of its delivery as an immediate response to the pandemic; literature on the integration of such programs within a clinical care program beyond the immediate needs of the pandemic is lacking. 23 Exploring implementation outcomes related to postpartum group therapy delivered by videoconferencing can help us understand how and whether videoconferencing psychotherapy groups can be integrated into standard mental health care service delivery, and to inform future work into their optimization.
Our large, urban tertiary academic hospital has a strong vision and mandate to develop, implement and study virtual solutions to support the equitable delivery of high-quality, publicly funded healthcare services. We securely embedded Zoom® into the hospital's electronic medical record and patient-facing portal as part of an institutional-wide initiative to offer synchronous, videoconferencing-based group health interventions (‘videoconferencing groups’) to hospital patients during the pandemic and beyond; infrastructure sustainability was a core component of these efforts. 30 This enables secure access for patients and providers as well as complete clinical integration for documentation, care planning, and follow-up. A specialized reproductive mental health program within the Department of Psychiatry at the hospital continues to deliver interpersonally oriented group psychotherapy for postpartum depression and anxiety through this modality as standard of care due to patient request, even as restrictions to in-person therapy have lifted. As a major focus of this group when it was offered in person was the interpersonal (i.e. social) experience, ensuring that this aspect of the group (i.e. the ability to engage in conversation and socialization within the group setting) can be implemented in the transition to a virtual platform is paramount.
The goal of the current study was to pragmatically evaluate the implementation of the postpartum videoconferencing psychotherapy group within the clinical setting.
Methods
Study design
The study design was informed by the Virtual Group Evaluation Framework 30 (VGEF), which spans implementation, quality and effectiveness domains; it was developed and used by our institution to guide the evaluation of videoconferencing groups. We primarily focused this evaluation on the implementation (i.e. its adoption, acceptability, appropriateness, and feasibility) of the videoconferencing group as it was most relevant to our research question and pragmatic in terms of data collection. Additionally, we looked at other outcomes related to group dynamics and development (‘group process’), given that the interaction between group members was a core element of the in-person group, as well as the group's efficiency, effectiveness, safety, and overall experience from the patient perspective. This study was part of a pragmatic, real-world quality improvement evaluation.
Setting and intervention
The psychotherapy group's content and approach loosely follow an interpersonal therapy (IPT) model, but it is not strictly an IPT group. 31 The interpersonally oriented basis of the group is the idea that improving relationships with others can buffer the effect of major stressors on a person's psychological health.32,33 Therapy focuses on relationship management in four areas: conflict in relationships, life changes, grief and loss, and difficulties in starting and maintaining relationships. 33 The interpersonally oriented approach is particularly appropriate for the postpartum period where people undergo significant life changes, manage new expectations of relationships, and when social isolation is a major risk factor for mental illness. During the first group session, the facilitator and patients collaboratively develop a list of specific topics of interest that are discussed over the remaining sessions. Over the course of the group, in addition to elements of traditional IPT (i.e. education and discussion on losses and gains, and the impact of transition and change), the facilitator and patients practice guided mindfulness and discuss the mutually agreed-upon topics relevant to the role transition to parenthood. Prior to this evaluation, patients often anecdotally indicated that they found the in-person group to provide validation and social connection at a time when they struggled with isolation due to their new baby and their mental health challenges. There were three primary individuals who facilitated the groups, each of whom was either a trained social worker therapist or a registered psychotherapist, and all of whom had a specialist background in perinatal mental health. One group was facilitated by a trainee under the supervision of one of the three primary facilitators.
Originally developed as an in-person psychotherapy group, it has been offered virtually since 2020 (originally due to pandemic-related restrictions) as standard of care. Our institution integrated the hospital's electronic medical record (Epic) with Zoom to facilitate ease and security of clinical care planning, documentation, and follow-up. 30 From the patient's perspective, it is accessed through the patient portal, which is accessible via desktop computers and laptops, and is mobile-friendly. Training materials on the use of the patient portal to access and participate in the videoconferencing group were developed by the hospital and can be accessed online. Specific changes were made to the group's structure when it was adapted from an in-person to a videoconferencing format. The duration of the group was reduced from 10 weeks to 8 weeks for practical reasons related to waitlist management during the pandemic and ensuring timely access to care. The composition of the group was reduced from 10–12 patients and two highly trained psychotherapists to 5–6 patients and one highly trained psychotherapist (either a social worker therapist or a registered psychologist) in the videoconferencing format as it was thought that a smaller group size would allow for greater social engagement among patients since this was a central aspect of the group.
Participants
Upon referral to the reproductive mental health program, patients are assessed by a perinatal psychiatrist. Together, the patient and perinatal psychiatrist collaboratively form a treatment plan that may include psychotherapy and/or medication. Group psychotherapy is the main therapeutic modality offered to patients 0–12 months postpartum with depressive or anxious symptoms. Postpartum people (anyone who delivered a baby within the past 1 year or who self-identifies as a mother of an infant <1 year of age, inclusive of cisgender and transgender individuals) with symptoms of depression and anxiety (based on the psychiatrist's assessment) are eligible to participate in the group. Patients would be excluded from the group and offered individual psychotherapy only if deemed clinically appropriate for the patient (e.g. due to diagnosis, illness severity). Referral to the postpartum videoconferencing psychotherapy group does not require a diagnosis of a major depressive or anxiety disorder, nor a specific symptom threshold. All patients of the clinical program who participated in the videoconferencing psychotherapy group as part of their clinical treatment plan were included in the quality improvement evaluation.
Data sources, collection and storage
Data on group adoption metrics (i.e. usage) was extracted from the electronic medical record for all patients registered in the postpartum videoconferencing psychotherapy group during the evaluation period (October 2021–August 2022). All patients in the postpartum videoconferencing psychotherapy groups during this period were asked to optionally complete a baseline survey before the group, and again at group completion to evaluate the self-reported outcomes of the videoconferencing group (Table 1). Sociodemographic variables were collected via self-report at baseline, and group facilitators completed a treatment log to describe the primary topics of discussion, education provided, and/or skills taught for each group session.
Overview of patient-reported experience measures and outcome measures.
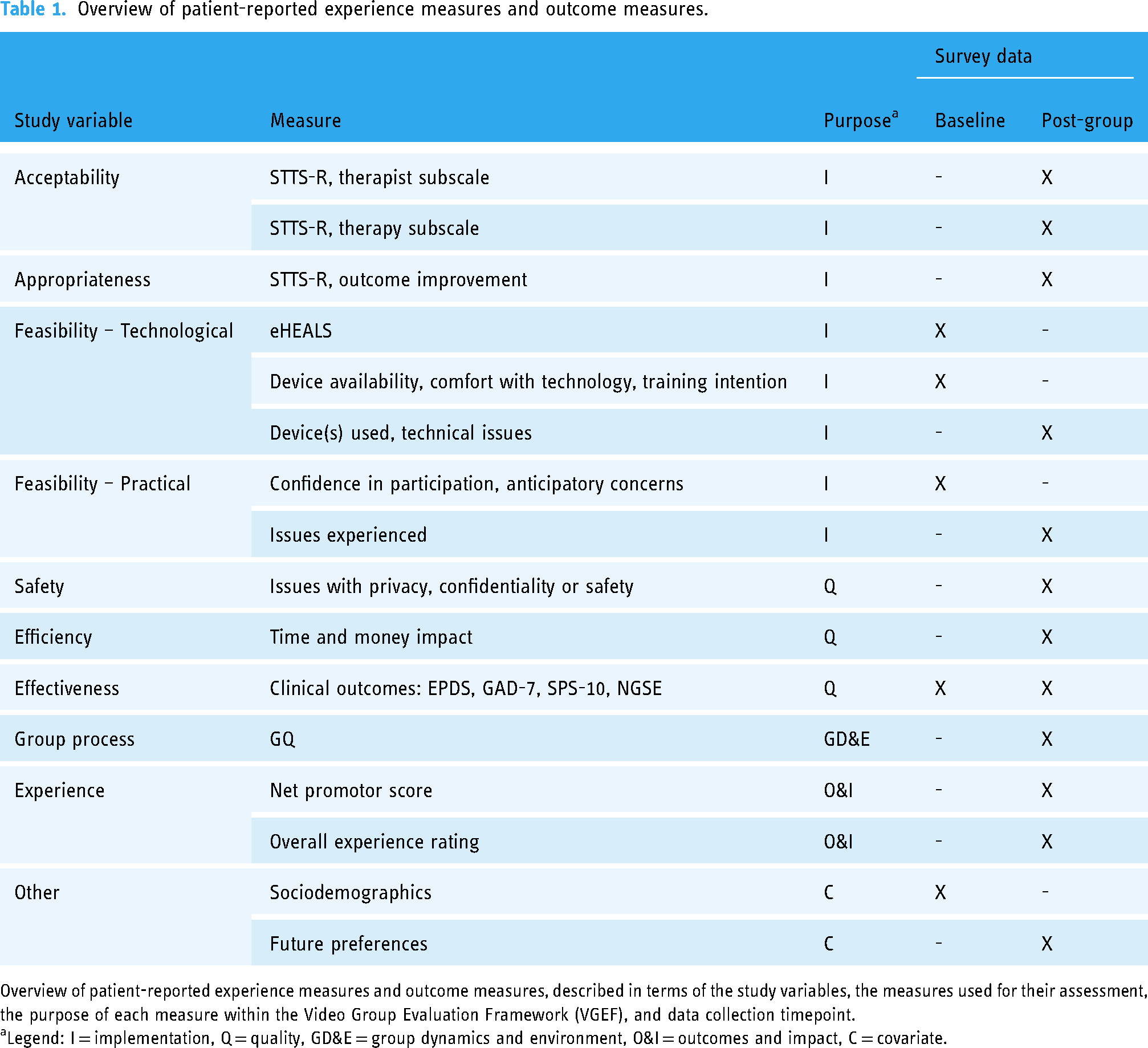
Overview of patient-reported experience measures and outcome measures, described in terms of the study variables, the measures used for their assessment, the purpose of each measure within the Video Group Evaluation Framework (VGEF), and data collection timepoint.
aLegend: I = implementation, Q = quality, GD&E = group dynamics and environment, O&I = outcomes and impact, C = covariate.
Surveys were digitally administered, and data were collected and managed using Research Electronic Data Capture (REDCap) hosted at our institution.34,35 REDCap is a secure, web-based software platform designed to support data capture for research studies, providing an intuitive interface for validated data capture, audit trails for tracking data manipulation and export procedures, automated export procedures for seamless data downloads to common statistical packages, and procedures for data integration and interoperability with external sources.
Outcomes
Implementation outcomes
The primary objective was to pragmatically evaluate the implementation of the interpersonally oriented postpartum videoconferencing psychotherapy group in the clinical setting using measures of implementation outcomes36,37 relevant to this work as per the VGEF. 30
Adoption (i.e. uptake of the videoconferencing group): Data on service use was extracted from hospital medical records for all groups provided during the evaluation period. We defined active participants as those who attended ≥70% of group sessions (i.e. at least 6/8 or 5/7 sessions, depending on group length), and drop-outs as not attending the last two sessions of the group series.
Acceptability and appropriateness: Acceptability (i.e. perception that the treatment and modality were satisfactory) and appropriateness (i.e. perceived fit of the videoconferencing group to address symptoms of postpartum depression and anxiety) were measured in the post-group survey by administering the Satisfaction with Therapist and Therapy Scale-Revised (STTS-R). 38 The STTS-R is used to evaluate satisfaction with a group therapy intervention and has been used for both in-person and online groups. 39 It is comprised of two, six-item subscales (satisfaction with therapy, and satisfaction with therapist), and one additional item on perceived outcome improvement (‘How much did this treatment help with the specific problem that led you to therapy?’). 38 Each item in the STTS-R is scored on a 5-point Likert scale, with higher scores indicating greater levels of satisfaction. Subscale items are summed to a maximum of 30 per subscale and the perceived outcome improvement question is analysed independently. A score of ≥21 has been used in the literature to indicate a reasonable level of satisfaction on each subscale. 40
Technical and practical feasibility (i.e. the extent to which the videoconferencing group can be successfully used): Technical feasibility was measured in the pre-group survey by administering the eHealth Literacy Scale (eHEALS)41,42 to assess readiness for successful engagement with health information technology. Each of the eight items on the eHEALS is scored on a Likert scale (from 1, strongly disagree to 5, strongly agree) and summed; higher scores (to maximum of 40) indicate higher levels of literacy. In the literature, the mean eHEALS score reported in adult populations ranges from 28 to 30. 43 Additionally, at baseline, we asked about the availability of technical devices in the home, comfort with technology in day-to-day life on a Likert scale (from 1, excellent to 5, poor), and plans to look at training materials. In the post-group survey, we ascertained which technical devices were used to access the group, whether there were technical issues that made participation difficult, and if they needed to contact technical support at the hospital to participate. Practical feasibility was measured at baseline by asking about confidence in participation on a 5-point Likert scale and anticipatory concerns related to participation. In the post-group survey, we asked if any practical issues were experienced using a binary question and provided patients the opportunity to expand on their experience in a free-text response.
Other outcomes
Group process: The group dynamic in a videoconferencing context was measured by looking at the group process using the Group Questionnaire (GQ) 44 in the post-group survey. Modifications were made so the questionnaire reflected the group overall, not singular sessions. Each of the 30 items on the GQ is scored on a 7-point Likert scale. 45 Scores are summed for each of three subscales on relational constructs: positive bonding relationship (out of 91), positive working relationship (out of 56), and negative relationship (out of 63). Each subscale construct is related to four key elements of group functioning (cohesion, alliance, empathy, and group climate) and are assessed from the perspective of members to each other, to the group, and to the facilitator. 44 We also asked whether patients felt it was easy to interact with the facilitator and other group members online, each on a 5-point Likert scale.
Efficiency: Efficiency was measured by asking patients in the post-group survey about whether their participation saved them time and/or money in comparison to an in-person group on a 5-point Likert scale and for their free-text perspectives on group benefits and drawbacks. Patients were asked about the comfort and ease of use of the videoconferencing group platform and the video group itself, and its impact on access to care, using Likert scale-based responses.
Effectiveness (i.e. clinical outcomes): To ascertain the effectiveness of the postpartum videoconferencing psychotherapy group, patients completed the Edinburgh Postnatal Depression Scale (EPDS), 46 seven-item screening tool for Generalized Anxiety Disorder (GAD-7), 47 Social Provisions Scale, Short Version (SPS-10), 48 and New General Self-Efficacy Scale (NGSE). 49 Each of the 10 items on the EPDS is scored 0–3; sum scores ≥13 indicate probable depression. Each item on the GAD-7 is scored on a 4-point Likert scale; a sum score >10 indicates probable moderate anxiety. The SPS-10 is scored on a 4-point Likert scale; a sum score of ≥30 indicates high levels of support. Each of the eight items on the NGSE is scored on a 5-point Likert scale and an average overall score is calculated.
Safety: It was assessed by asking patients a binary question in the post-group survey about whether they experienced anything that made them worried for their privacy, confidentiality or safety during the group along with the opportunity to elaborate. They were also asked about their general comfort with participation on a Likert scale.
Experience: Overall experience was measured by calculating a Net Promotor Score (NPS), which is used to provide an overall benchmark of performance within a comprehensive feedback process. 50 To calculate the videoconferencing group's NPS, each patient rated their willingness to recommend the group on a scale of 1–10, and each rating was categorized into detractors (rating 0–6), passives (rating 7–8), and promotors (rating 9–10). The NPS is calculated by determining the difference between the percentage of promotors and the percentage of detractors, for a possible range from −100 to +100. Additionally, patients were asked to rate their experience with the technology and with the videoconferencing group overall, each on a scale of 1–10.
Future preferences: Future preferences regarding videoconferencing groups were collected in the post-group survey.
Data analysis
Descriptive analyses were conducted for each measure. Standardized scales (STTS-R, eHEALS, GQ, EPDS, GAD-7, SPS-10, NGSE, and NPS) were scored as described above. Pre- and post-group scores for the EPDS, GAD-7, SPS-10, and NGSE were compared using a paired samples t-test. For each of these four scales, each patient's score was also dichotomized based on its cut-off score, and differences between the baseline and post-group scores were compared using a Pearson chi-square test of association. Quantitative analyses were conducted using SPSS 29.0. Free-text responses and content from treatment logs were thematically coded 51 by NHS in NVIVO 12.0.
Ethical considerations
This initiative was reviewed and approved under the Assessment Process for Quality Improvement Projects program (File #2021-0059-E). As the postpartum videoconferencing psychotherapy group is a standard-of-care clinical program and this was a quality improvement evaluation, patients were not required to consent to the collection of EMR data (which was anonymized) to participate in the group, nor did we withhold group participation from anyone who declined to complete the surveys, which were optional. Clinical care providers were blinded to whether patients had completed the surveys. Before completing their surveys, patients reviewed an informed consent page, which outlined that completing the survey signified their implied consent to self-reported data collection. There were no benefits to patients for completing the surveys.
Results
Data on group attendance was available for all 153 patients (26 groups) during the study period; all but two groups were 8 weeks long (Figure 1). Of 137 patients (24 groups) who were sent e-surveys, 50 patients (36.5%) completed both the pre- and post-group surveys and are included in the analysis. Surveys were not sent to patients (n = 12) in two groups due to facilitator workload capacity. Sociodemographic data for patients included in the analysis are outlined in Table 2. Facilitators completed treatment logs for 24 out of 26 groups (two groups did not have treatment logs completed due to facilitator workload capacity). Details of topics covered are in Appendix 1.
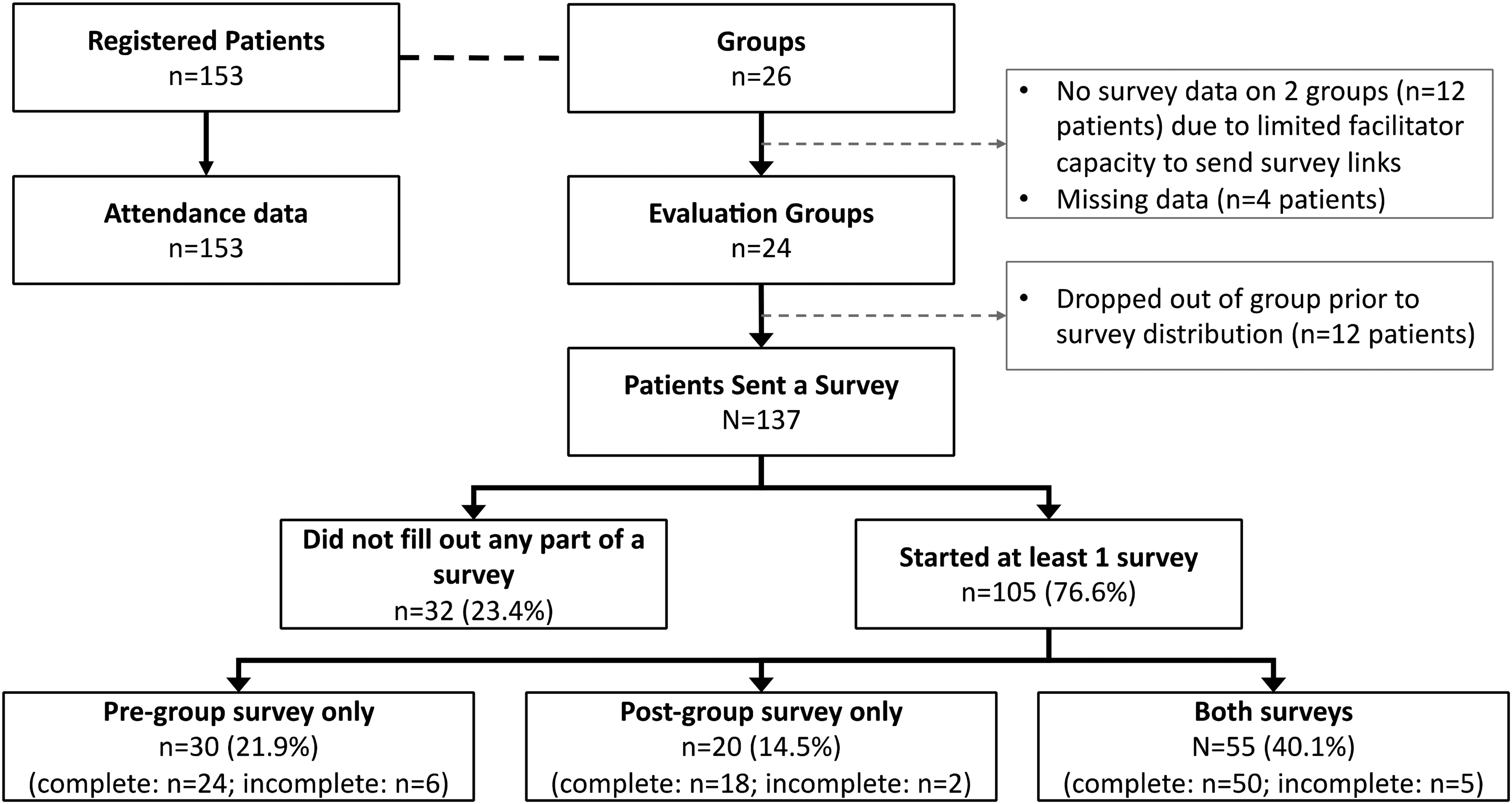
Patient flow.
Sociodemographics.

Sociodemographic data of survey respondents as reported in the pre-group survey, reported as n (%), unless otherwise specified (N = 50).
Implementation outcomes
Adoption: There were n = 8 (5.2%) registered patients who did not attend any group sessions, and over one-third (35.5%, n = 54) had perfect attendance. Patients in groups that were 8 weeks in length (n = 24 groups, n = 142 patients), attended a median of 7 (interquartile range, IQR: 6–8) group sessions. Overall, 72.5% (n = 111) were active participants and only 13.7% (n = 21) dropped-out (Table 3).
Video group implementation outcomes.

Indicators of implementation, as recorded in the hospital electronic medical record (N = 153) for adoption, and as self-reported by patients in the pre- and post-group surveys (N = 50), for other domains, as n (%) unless otherwise specified.
aBased on 24 groups that were 8 weeks in length; two groups were 7 weeks long.
bDefined as attending at least 6 of 8, or 5 of 7 group sessions, depending on group length.
cDefined as not attending the final two sessions of the group.
dEach of the six items in each subscale is scored on a Likert scale from 1 to 5 and summed to a maximum score of 30.
eSelect all that apply format, answers do not add up to 100%.
Acceptability and appropriateness: The mean scores on the STTS-R Therapy Subscale and Therapist Subscale were 25.0 (SD: 3.1) and 27.6 (SD: 2.3) out of 30, respectively (Table 3). When asked about the perceived impact of participating in the video therapy group, most patients felt it made their problem at least somewhat (n = 37, 74.0%) better.
Technical and practical feasibility: The mean (SD) eHEALS score in our sample was 25.8 (4.1). Patients had access to a range of devices that would be appropriate for accessing the video group and most accessed it using a laptop (n = 40, 80.0%) and/or smartphone (n = 14, 28.0%) (Table 3). Few patients planned to look at the video group training materials (n = 13, 28.0%). Technical issues that made it difficult to participate were uncommon and no patients contacted the hospital's technical support to participate. Before the start of the group, most felt confident in their ability to participate in a videoconferencing group (very confident: n = 31, 62.0%). Anticipatory concerns were reported by 22.0% (n = 11) and mostly related to practical issues (e.g. childcare, technology-related concerns, and general concerns about interacting with others online). Issues that were experienced were similar (e.g. Internet connection, problems logging in to portal, childcare, having a private space) but experienced by fewer in proportion (n = 8, 16.0%).
Other outcomes
Group process: Patients reported a mean positive bond score of 81.4/91 (SD: 7.8), a mean Positive Working Relationship score of 34.1/56 (SD: 3.8) and a mean negative relationship score of 23.5/63 (SD: 4.4) (Table 4). Most felt it was easy to interact online with other group members (agree: n = 20, 40.0%) and the facilitator (agree: n = 24, 48.0%).
Additional videoconferencing group outcome measures.

Additional outcome measures for the videoconferencing group, as self-reported by patients (N = 50), as n (%) unless otherwise specified.
Efficiency: Patients agreed that participating in the video group compared to an in-person group saved them time (strongly agree: n = 35, 70.0%) and money (strongly agree: n = 28, 56.0%) (Table 4). In free-text responses, patients reported that the benefits of the group included having the flexibility to participate from home, being able to maintain their infant's schedule, reduced exposure to communicable illness, not having to commute (e.g. costs of driving and parking, avoiding travel on public transit, avoiding weather-related concerns, etc.), ease of childcare (e.g. either self or a partner at home), and less pressure to appear ‘presentable’ to others. Drawbacks of participating in the videoconferencing group included difficulty reading and responding to body language, trouble with conversational flow, distractions at home, loss of incidental interactions with fellow group members, and the lack of excuse to leave the house. Nearly all patients reported that the videoconferencing platform was easy to use and that they felt comfortable using it to participate in the group; they agreed that having the videoconferencing platform improved their ability to access care (Table 4).
Effectiveness: Self-reported mental health symptoms improved for patients (Table 5). The mean EPDS score (n = 46) fell from 12.7 (SD: 4.1) to 11.2 (SD: 4.3) in the post-group survey (p = .004). The number of patients with probable depression (EPDS ≥13) significantly decreased from n = 23 (50%) to n = 19 (41.3%) patients (p < .001). The mean GAD-7 score (n = 49) fell from 9.0 (SD: 4.4) to 8.3 (SD: 4.6) in the post-group survey, a non-statistically significant difference (p = .223); the number of patients with probable anxiety (GAD-7 ≥ 10) significantly decreased from n = 22 (44.9%) to n = 15 (30.6%; p = 0.04). Patients (n = 48) reported high mean levels of social support on the SPS-10 in the pre-group survey (34.2, SD: 4.8) which significantly improved post-group (35.7, SD: 4.5; p = .002). The proportion of those reporting high levels of social support (SPS-10 ≥ 30) significantly increased from n = 38 (79.2%) to n = 42 (87.5%; p < .001). Similarly, self-efficacy increased from a mean NGSE score of 3.7 (SD: 0.7) to 3.9 (SD: 0.7; p < .001) and the number of patients reporting high levels of self-efficacy (NGSE ≥3.8) increased from n = 25 (50.0%) to n = 29 (58.0%; p < .001).
Effectiveness scales.

Self-reported outcome scales, comparing pre- and post-group scores (N = 50) using paired samples t-tests for raw scores and Pearson chi-square to compare cut-off scores. Statistical significance was defined as p < .05 and is indicated by an asterisk (*).
Safety: Few patients reported anticipatory safety concerns (n = 2, 4.0%) or actually experiencing any issues (n = 2, 4.0%) related to privacy, confidentiality, or safety during their group. All reported having felt at least somewhat comfortable participating in the videoconferencing group (Table 4).
Experience: Patients gave a mean NPS rating of 9.2 (SD: 1.2) out of 10; based on their NPS, most patients (n = 36, 72.0%) were classified as promotors. The overall NPS for the videoconferencing psychotherapy group was +70. The mean scores for the experience with the technology specifically and the videoconferencing group overall were, respectively, 8.7 (SD: 1.1) and 8.9 (SD:1.1), each out of 10.
Future preferences: Patients noted they would be happy to participate in a videoconferencing group again (agree and strongly agree: n = 45, 90.0%) yet leaned towards attending an in-person group had the virtual option not been available (agree and strongly agree: n = 26, 52.0%) (Table 4). However, if given the option of a videoconferencing or in-person group in the future, patients leaned towards choosing the videoconferencing group (agree and strongly agree: n = 27, 54.0%). Patients would like the option of participating in a videoconferencing group in the future (agree and strongly agree: n = 44, 88.0%).
Discussion
In our evaluation, we demonstrate that an interpersonally oriented therapy group for symptoms of postpartum depression and anxiety can be delivered via videoconferencing and implemented successfully, with positive and strong group processes. Overall our key findings include high levels of acceptability and appropriateness and a robust group process alongside a highly rated experience among those who participated in a psychotherapy group delivered by videoconferencing as standard of care within a clinical setting. This suggests that the interpersonal and social nature of group therapy in the postpartum period can be translated into and implemented in the virtual world.
As its primary objective, our study is unique in its examination of the implementation of an interpersonally oriented and conversationally based videoconferencing group therapy for symptoms of postpartum depression and anxiety within a clinical setting. Our drop-out rate of 13.7% was lower than that reported among videoconferencing groups elsewhere in the literature in studies on varied populations including veterans (18% 29 ), adults with anxiety disorders (15.3% 52 ), and perinatal groups (20% 20 ), although the definition of drop-out varied between studies. Studies that compared attendance to an in-person group found higher attendance in the videoconferencing format,29,52 implying it may reduce barriers to care and support higher attendance. Many barriers to care often noted in the literature as contributing factors to treatment attrition in this population are, in part, addressed by this modality, noted by patients as benefits of the videoconferencing group. In our qualitative evaluation based on patient interviews (reported separately), patients note the tensions between finding childcare during the videoconferencing group or caregiving while participating and the added value of presenting oneself in a more authentic manner when participating online. Of critical importance, it was feasible for patients to access the group from a technical and practical standpoint and our group was highly acceptable to patients. This is particularly evident when noting that our scores on the STTS-R Therapy subscale were comparable to those found in a range of in-person studies.53–56
There are significant challenges with the creation of strong group processes in a virtual context. The group evaluated in this study was conversational and social in nature, and our data demonstrated that a therapy group of this nature can be successfully implemented virtually. Encouragingly, our study found scores on the GQ that were comparable to those measured among in-person groups. A meta-analysis of in-person studies that used the GQ 57 determined aggregate subscale scores for positive bonding (mean: 72.91, SD: 12.37), positive working (mean: 38.11, SD: 10.52), and negative relationship (mean: 23.54, SD: 8.74), which are all comparable to our data. Based on our data, strong group processes were achieved across multiple groups with different facilitators, suggesting that the development of a strong group environment can be created through videoconferencing. Our qualitative study validates this and highlights the important role played by the facilitator in developing a sense of cohesion among group members in an online environment. The facilitator 58 and homogeneity among the group (related to either the presenting issue or identity-related factors) 59 are both associated with the cohesion of in-person groups. Inherent commonalities between group members (i.e. postpartum people with depressive and anxious symptoms) and the smaller group size (compared to the original in-person format) may have contributed to the highly rated group process and, in turn, may also explain the high levels of satisfaction observed.
Although our data shows improvement in mental health symptom scores, the small changes in absolute scores on the EPDS in our evaluation (a difference of 1.5 points from baseline to post-group) do not meet the 2-point minimum threshold for a clinically important difference. 60 This may be related to the fact that entry to the group is based on the presence of symptoms and not a symptom threshold nor formal diagnosis. Additionally, this evaluation did not focus on the impact of the group of clinical outcomes and was not powered to do so. Understanding the group's impact on clinical outcomes and well-being, particularly given that 94% of patients reported feeling that the group made their problem at least ‘somewhat better’, should be the focus of future work.
There are few studies to our knowledge that specifically examine the implementation of videoconferencing therapy groups that focus on interpersonal and social interactions within a virtual setting. Limitations of this study should be noted. There was a low response rate for completion of both surveys and we only included data from patients who completed both of the optional baseline and post-group surveys, representing approximately one-third of all of those who were registered in the group. This may have introduced bias in that feedback was not received from all of those who participated in the group and may therefore limit the generalizability of our results. With the lack of external incentives for quality improvement surveys, response and completion are a challenge; response rates to quality improvement studies (such as this one) of 50% are considered to be ‘quite high’. 61 Our study achieved a response rate of only 36.5% for those who completed both the baseline and post-group surveys, although more than three-quarters of patients started at least one of the two quality improvement surveys. While we included several validated scales in our surveys, the use of questions that were not validated, and the lack of pilot testing the survey is an additional limitation. In addition, in the post-group survey we did not ask patients if they looked at the training materials, which may have better helped to understand their influence on outcomes, particularly related to the technical feasibility of the videoconferencing group. In line with the institutional approach to the development and implementation of videoconferencing groups as a treatment modality, the use of a systematic institutional-level approach to group evaluation, such as one centred on the principles of a Learning Health System, 62 may be warranted to improve survey response rates, with the added benefit of relieving facilitator administrative burden related to sending out survey links to patients. Without a direct comparison to an in-person group, it is not possible to say with certainty how our outcomes compare to traditional in-person groups, and the homogeneity of our survey sample population may limit the generalizability of findings, particularly among marginalized groups as our sample is skewed towards a higher income group.
In conclusion, interpersonally oriented group therapy for symptoms of postpartum depression and anxiety, delivered through videoconferencing, can be implemented with robust group processes that maintain social interactivity and with general acceptability. Future work should consider an evaluation of efficacy, equity, and comparison of differing delivery modalities, to determine who might be best served from accessing care through various approaches to delivery. Based on our evidence, there is a case for maintaining its place in the ongoing delivery of standard care at our hospital. Group psychotherapy, delivered through videoconferencing can be a way through which to deliver care to postpartum people who may otherwise experience barriers to access important mental health treatment that is vital to their well-being.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241269630 - Supplemental material for Implementation of a conversational, videoconferencing-based therapy group for postpartum depression and anxiety symptoms: A pragmatic evaluation
Supplemental material, sj-docx-1-dhj-10.1177_20552076241269630 for Implementation of a conversational, videoconferencing-based therapy group for postpartum depression and anxiety symptoms: A pragmatic evaluation by Neesha Hussain-Shamsy, Lori Wasserman, Greer Slyfield Cook, Kaeli Macdonald, Keisha Greene, Lucy C. Barker, Juveria Zaheer, Geetha Mukerji, Simone N. Vigod and Emily Seto in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076241269630 - Supplemental material for Implementation of a conversational, videoconferencing-based therapy group for postpartum depression and anxiety symptoms: A pragmatic evaluation
Supplemental material, sj-pdf-2-dhj-10.1177_20552076241269630 for Implementation of a conversational, videoconferencing-based therapy group for postpartum depression and anxiety symptoms: A pragmatic evaluation by Neesha Hussain-Shamsy, Lori Wasserman, Greer Slyfield Cook, Kaeli Macdonald, Keisha Greene, Lucy C. Barker, Juveria Zaheer, Geetha Mukerji, Simone N. Vigod and Emily Seto in DIGITAL HEALTH
Footnotes
Contributorship
NHS reviewed the literature, conceived of, and designed the study under the guidance and supervision of ES, SV, GM and JZ as part of her doctoral work. LW, GSC, KM and KG provided input into the design of the study and the processes for data acquisition. GSC, KM and KG facilitated data collection. NHS, ES, SV, GM and JZ interpreted the data. LB assisted with the interpretation of the data and provided critical revisions to the manuscript. All authors reviewed, edited, and approved the final version of the manuscript.
Declaration of conflicting interests
SV reports royalties from UpToDate Inc. for authorship of materials on depression and pregnancy.
Ethical approval
This initiative was formally reviewed by institutional authorities at Women's College Hospital and was approved under the Assessment Process for Quality Improvement Projects program (File #2021-0059-E).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Women's College Hospital (grant number AFP Innovation Fund WCH-22-005).
Guarantor
NHS.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.