
Abstract
Background
Individuals increasingly turn to the Internet for health information, with YouTube being a prominent source. However, the quality and reliability of the health information vary widely, potentially affecting health literacy and behavioural intentions.
Methods
To analyse the impact of health information quality on health literacy and behavioural intention, we conducted a randomized controlled trial using a quality-controlled YouTube intervention. Health information quality on YouTube was evaluated using the Global Quality Score and DISCERN. We randomly allocated (1 : 1) to the intervention group to watch the highest quality-evaluated content and to the control group to watch the lowest quality-evaluated content. Health literacy and health behavioural intention were assessed before and after watching YouTube. The trial was set for two different topics: interpreting laboratory test results from health check-up and information about inflammatory bowel disease (IBD).
Results
From 8 April 2022 to 15 April 2022, 505 participants were randomly assigned to watch either high-quality content (intervention group, n = 255) or low-quality content (control group, n = 250). Health literacy significantly improved in the intervention group (28.1 before and 31.8 after; p < 0.01 for health check-up; 28.3 before and 31.3 after; p < 0.01 for IBD). Health behavioural intention significantly improved in the intervention group (3.5 before and 4.1 after; p < 0.01 for health check-up; 3.6 before and 4.0 after; p < 0.01 for IBD). Control groups had no such effect.
Conclusion
High-quality health information can enhance health literacy and behavioural intention in both healthy individuals and those with specific conditions like IBD. It stresses the significance of ensuring reliable health information online and calls for future efforts to curate and provide access to high-quality health content.
Keywords
Introduction
In the current medical system, patients often encounter challenges when seeking immediate answers to their health-related questions from medical experts. Traditional face-to-face healthcare service models may not be appropriate for patients to obtain timely and accessible information. Therefore, individuals frequently turn to alternative sources of information, particularly the vast array of health-related content available on the Internet. 1 In particular, YouTube is one of the most well-known social media platforms worldwide with 1.9 billion users and billions of views per day.2,3 Countless videos are being uploaded and viewed on YouTube at this very moment.
Widespread Internet connectivity and the proliferation of online platforms have empowered individuals to search for health information proactively. Reliance on online health information has become common practice, offering a potential solution to the difficulties faced in obtaining immediate answers within the current medical system. This shift in information-seeking behaviour reflects the growing trend of patients taking more control over their healthcare decisions. 4 By leveraging online health information, patients aim to gain a better understanding of their health concerns, diagnoses, and treatment options. Health literacy plays an important role in encompassing the degree to which individuals can acquire, process, understand, and communicate health information necessary for making informed decisions about their health. 5 Additionally, existing studies have shown that high digital health literacy is positively correlated with information-seeking and health behaviours.4,6 Therefore, it is crucial to understand the association between patients’ health literacy and the quality of the health information they might access. 7
However, reliance on online health information presents both opportunities and challenges. Because the Internet provides convenient and readily accessible resources, it has become increasingly important to ensure the reliability and accuracy of the information encountered. 8 Patients are at a high risk of encountering inaccurate, biased, and indiscriminately distributed health information, which can have serious health consequences. 9 Although several studies have been conducted to assess the quality of YouTube videos for specific diseases,10,11 there is a lack of research demonstrating the effect of quality-evaluated health information content on patients’ health-related outcomes.
To analyse the impact of the quality of online health information on health literacy and health behavioural intention, we conducted a randomized controlled trial with two different topics: a health check-up and inflammatory bowel disease (IBD). We aimed to demonstrate that health literacy and health behavioural intention are influenced by health information quality in various groups.
Materials and methods
Study design
This study was a two-armed, double-blind, age- and gender-stratified randomized controlled trial, and 505 participants were recruited from a domestic research company in Korea from 8 April 2022 to 15 April 2022; they were allocated 1 : 1 to the intervention and control groups. Once enrolled, participants were provided with a link to an online survey in which they completed their sociodemographic characteristics, such as age, gender, education, and occupation, baseline health literacy, and health behavioural intention. After the baseline survey, the participants were randomly assigned to watch either the highest quality YouTube content (intervention group) or the lowest quality YouTube content (control group). After the participants watched their assigned videos, they completed an online follow-up survey assessing information reliability, health literacy, and health behavioural intentions. The trial settings were restricted to environments where participants were able to fully focus on watching the video and answering the questionnaire alone. The study protocol and informed consent forms were approved by the Institutional Review Board of Seoul National University Hospital (SNUH) (approval no. H-2204–020–1313). This study was conducted in accordance with the principles of the Declaration of Helsinki.
Participants
The inclusion criteria were as follows: (1) age 20–69 years, (2) for Group 1, participants who had undergone a health check-up within the past year, and (3) for Group 2, participants who had been diagnosed with IBD and were experiencing abdominal discomfort at the time of enrolment. Exclusion criteria were as follows: for both Group 1 and Group 2: (1) technically unable to watch the assigned YouTube content or (2) unable to complete the online survey. Participants who completed the trial received approximately $5 compensation, while those who withdrew received approximately $0.5 compensation.
Intervention
A two-step quality evaluation was conducted to select YouTube content on two health topics: interpreting laboratory test results from a health check-up (Group 1) and IBD (Group 2). The first quality evaluation consisted of four doctors watching the retrieved videos for each topic and scoring them using the Global Quality Score (GQS). 9 A total of 40 videos were preselected, 20 for each health topic that were assessed to be consistent and not significantly deviating from the topics chosen for the experiment. The second quality evaluation was performed by 62 nurses with DISCERN 12 on the 40 videos preselected in the first quality evaluation, with the highest and lowest quality selected as the average of the scores assessed for each video. Finally, two videos per topic selected as the highest or lowest quality, of four videos in total, were selected for the study.
The four experimental groups were formed as follows: one group that watched the highest quality content on interpreting laboratory test results in health check-ups (Group 1–1, intervention group), one that watched the lowest quality video on interpreting laboratory test results in health check-ups (Group 1–2, control group), one that watched the highest quality video on IBD (Group 2–1, intervention group), and one that watched the lowest quality video on IBD (Group 2–2, control group).
Outcomes and measures
To assess health literacy, we used the KeHEALS, 13 which is the Korean-translated version of the eHealth Literacy Scale (eHEALS). 14 The eHEALS consists of 10 items, with the first two questions asking about the usefulness and importance of online information in making health-related decisions to understand the interest of the subject in using online health information. The remaining eight questions that are included in the health literacy score calculation use a question-and-answer format based on subjective criteria such as knowledge, quality evaluation, and ability to use online health information. The Cronbach's alpha of health literacy in this study was 0.89 before and 0.93 after watching the quality-evaluated videos. Health behavioural intention was measured with the previously validated three-item instrument consisting of measurements that influence participants’ future health behaviour, such as detecting symptoms and involving active discussion with doctors to prevent or detect disease. 15 The Cronbach's alpha of health behavioural intention in this study was 0.85 before and 0.89 after watching the quality-evaluated videos. Information reliability included four items that identified how trustworthy the participants considered the provided information. 16 The reliability of the health information used in this study had a Cronbach's alpha of 0.86. All items used on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Higher scores indicate better levels of health literacy, health behavioural intention, and information reliability.
Sample size
The number of participants required for each group in this study was calculated using the G*Power analysis program version 3.1.9.7. At least 120 participants were required based on the correlation coefficient between e-health literacy and health behavioural intention (r = 0.32, p < 0.01, reported in a previous study 17 ). After excluding dropouts and participants who provided incomplete or inefficient responses, a minimum of 125 participants were recruited for each group (127, 125, 128, and 125, respectively); therefore, a total of 505 were included in this study.
Statistical analyses
The health literacy and health behavioural intentions of participants were tested twice: before and after they watched the randomly assigned content. Paired t-tests were performed to compare the effects of quality-controlled content within a group (Group 1–1, 1–2, 2–1, and 2–2, separately). Independent samples t-tests were performed to compare the effects of the quality of content between the groups (Group 1–1 and 1–2, Group 2–1 and 2–2).
Structural equation modelling (SEM) analysis with mediator variable regression was conducted to determine and validate whether changes in health literacy were a mediating factor in the relationship between information reliability and health behavioural intentions. Figure 1 presents the overall path diagram for this study expressed in the form of an SEM. All statistical analyses were performed using IBM SPSS Statistics version 26 (IBM Corporation, Armonk, NY, USA) and SAS version 9.4 (SAS Institute, Inc., NC, USA). All empirical findings were considered statistically significant at p < 0.05.
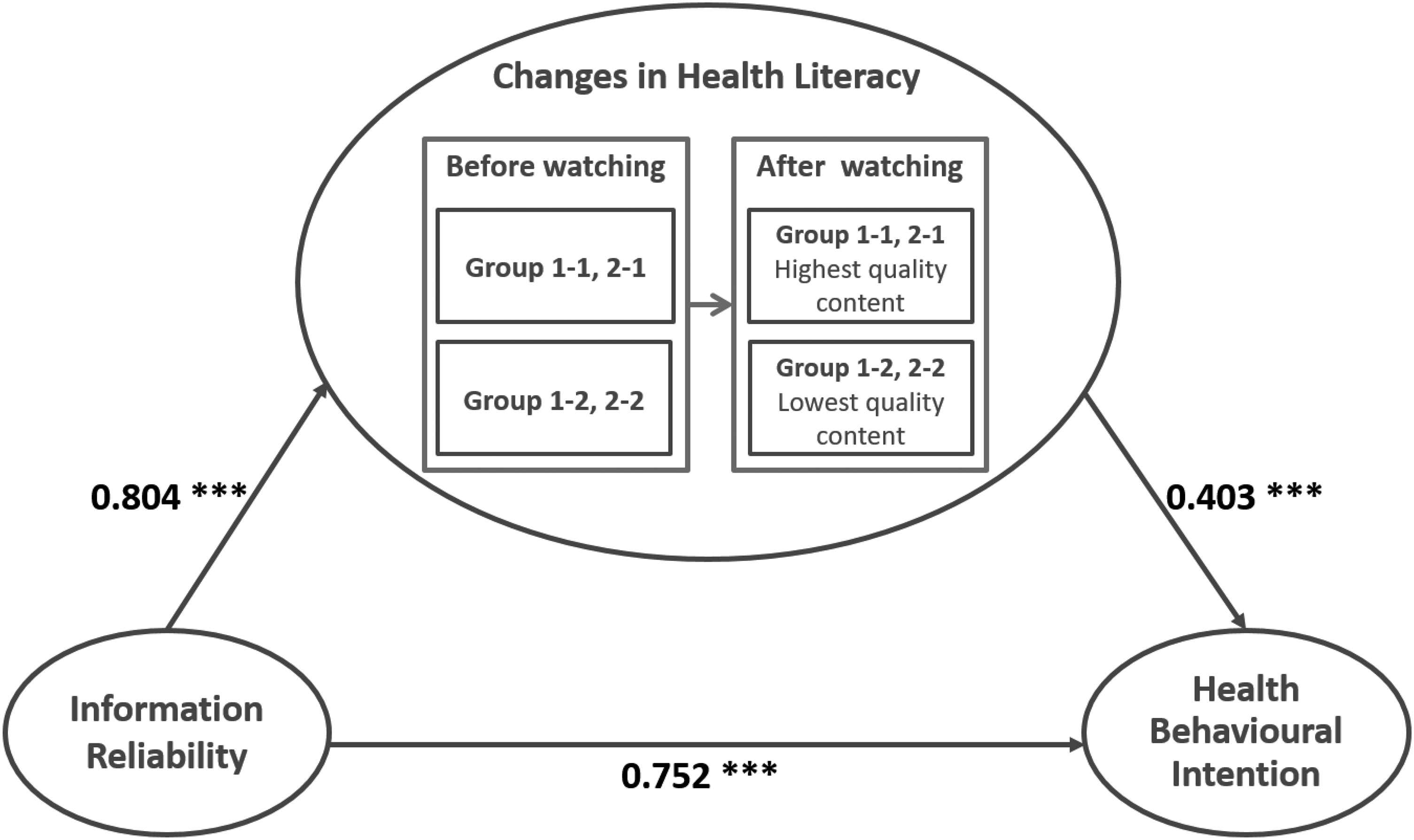
Structural equation model (SEM) among information reliability, changes in health literacy, and health behavioural intention. Note: β = Standardised coefficients, *** = Significant at p < 0.001.
Results
Demographic characteristics of participants
We recruited 505 eligible participants aged 20–69 years, with the distribution stratified by age and gender (Supplementary Table S1). A flow diagram of the study is shown in Figure 2.

Flow diagram of participant inclusion of the randomized control group pre-test post-test study.
Table 1 presents the demographic and online health information behavioural characteristics of the participants for all groups (Groups 1–1, 1–2, 2–1, and 2–2). Hospitals, healthcare centres, and medical professionals were the most common sources of health information (30.09%), followed by online videos (24.95%) and websites (24.75%). The most searched and obtained health information was about disease (33.26%), followed by disease prevention (23.56%) and treatment (21.78%). Other health information included a healthy diet, dietary (nutritional) supplements, exercise videos, fitness training, and posture correction. The most difficult type of health information to search for and utilize was treatment (29.30%), followed by diagnosis (21.99%) and medication (16.24%). Another reported difficulty was that even when the disease information is detailed, applying it in real life is challenging.
Baseline characteristics of the participants.

Quality evaluation results of health information on YouTube
Based on the GQS, a total of 40 videos—20 videos on each of the two topics, one on interpreting laboratory test results in health check-ups (Group 1) and the other on symptoms and suggested treatments for IBD (Group 2)—were preselected for quality evaluation by medical experts. Sixty-two nurses rated the preselected YouTube content based on the DISCERN criteria and assessment manual. The average clinical experience of the nurses was 11 years 3 months. The results of the highest and lowest quality content evaluated with DISCERN are presented in Supplementary Table S2. Regarding the interpretation of laboratory test results from the health check-up (Group 1), a video uploaded by a medical association (The Korean Society of Nephrology) received the highest quality evaluation (intervention group, Group 1–1), whereas a video uploaded by an individual received the lowest quality evaluation (control group, Group 1–2). Regarding IBD (Group 2), a video uploaded by a university hospital (The Catholic University of Korea, Yeouido St Mary's Hospital) received the highest quality evaluation (intervention group, Group 2–1), whereas a video uploaded by a broadcasting company (Channel A) received the lowest quality evaluation (control group, Group 2–2). Supplementary Figure 1 illustrates the overall study flow and intervention delivery for each group.
Changes in health literacy via quality-controlled YouTube content
Table 2 presents the changes in health literacy before and after participants watched the quality-controlled YouTube content.
Changes in health literacy before and after watching the quality-controlled content.

Mean ± SD of KeHEALS
p-value
Note: Group 1 watched video about interpreting lab test results in health check-up and Group 2 watched video about Inflammatory Bowel Disease (IBD)
There were no significant differences in baseline health literacy measured by KeHEALS between Groups 1–1 and 1–2 (28.07 ± 4.67 and 28.02 ± 5.10, respectively, p = 0.93) and between Groups 2–1 and 2–2 (28.31 ± 4.56 and 28.66 ± 4.89, respectively, p = 0.56). However, there was a difference in health literacy after watching the quality-controlled YouTube content between Groups 1–1 and 1–2 (31.83 ± 4.40 and 27.54 ± 5.59, respectively, p < 0.01) and between Groups 2–1 and 2–2 (31.30 ± 3.71 and 27.63 ± 5.14, respectively, p < 0.01). For intervention groups, the health literacy improved after watching the highest quality-evaluated content both in Group 1–1 (28.07 ± 4.67 before and 31.83 ± 4.40 after, p < 0.01) and Group 2–1 (28.31 ± 4.56 before and 31.30 ± 3.71 after, p < 0.01). However, for control groups, there was no difference in health literacy after watching the lowest quality-evaluated content in Group 1–2 (28.02 ± 5.10 before and 27.54 ± 5.59 after, p = 0.31) and statistically significantly decreased in Group 2–2 (28.66 ± 4.89 before and 27.63 ± 5.14 after, p = 0.02).
Subgroup analyses results showed that the health literacy increased in all intervention groups, a significant decrease in health literacy among female in Group 1–2, male, ≤ College graduation and ≥ Graduation school in Group 2–2 (Supplementary Tables S3–S5).
Changes in health behavioural intention via quality-controlled YouTube content
Table 3 presents the changes in health behavioural intentions before and after watching the quality-controlled YouTube content.
Changes in health behavioural intention before and after watching the quality-controlled content.
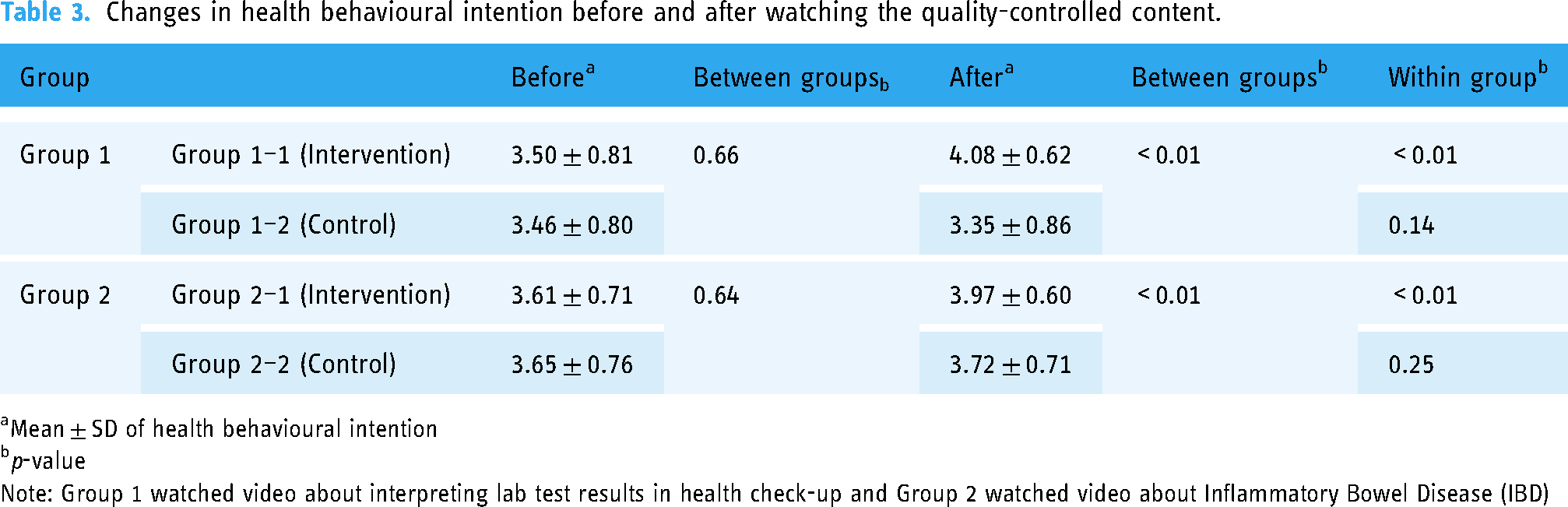
Mean ± SD of health behavioural intention
p-value
Note: Group 1 watched video about interpreting lab test results in health check-up and Group 2 watched video about Inflammatory Bowel Disease (IBD)
There were no significant differences in baseline health behavioural intentions between Groups 1–1 and 1–2 (3.50 ± 0.81 and 3.46 ± 0.80, respectively, p = 0.66) and between Groups 2–1 and 2–2 (3.61 ± 0.71 and 3.65 ± 0.76, respectively, p = 0.64). However, there was a difference in health behavioural intention after watching the quality-controlled YouTube content between Groups 1–1 and 1–2 (4.08 ± 0.62 and 3.35 ± 0.86, respectively, p < 0.01) and between Groups 2–1 and 2–2 (3.97 ± 0.60 and 3.72 ± 0.71, respectively, p < 0.01).
For intervention groups, health behavioural intention significantly increased after watching the highest quality YouTube content in Group 1–1 (3.50 ± 0.81 before and 4.08 ± 0.62 after, p < 0.01) and Group 2–1 (3.61 ± 0.71 before and 3.97 ± 0.60 after, p < 0.01), whereas for control groups, there were no changes in health behavioural intention in Group 1–2 (3.46 ± 0.80 before and 3.35 ± 0.86 after, p = 0.14) and Group 2–2 (3.65 ± 0.76 before and 3.72 ± 0.71 after, p = 0.25) after watching the lowest quality health information content.
All intervention groups from the subgroup analyses showed a statistically significant increase in health behavioural intention after watching the assigned content (Supplementary Tables S6–S8).
Structural equation model
A significant direct pathway was found from the reliability of information to health behavioural intention, and changes in health literacy played a partial mediating role between information reliability and health behavioural intention (Figure 1). Information reliability was significantly, directly, and positively related with changes in health literacy (β = 0.80, p < 0.01), indicating that patients receiving more reliable information tend to have higher level of health literacy improvement. Information reliability had a positive effect on health behavioural intention (β = 0.75, p < 0.01). Changes in health literacy were significantly and positively associated with health behavioural intention (β = 0.40, p < 0.01), indicating that the higher the level of health literacy improvement, the higher the intention to engage in health behaviours. In addition, as the direct effect (β = 0.75) was greater than the indirect effect (β = 0.44) of information reliability on health behavioural intentions, it was found that changes in health literacy were a partial mediating factor (Supplementary Table S9). In other words, changes in health literacy partially explain the relationship between information reliability and health behavioural intentions.
Discussion
This study found that high-quality online health information enhanced health literacy and behavioural intentions in both healthy individuals and patients with IBD. The topics were selected based on a thorough literature review of existing research, suggesting that improving health literacy with active health information interventions can have a significant impact on improving health outcomes.17,18 Lee et al. 19 suggested that to increase regular health check-up attendance, it is necessary to improve communication with easy-to-understand explanations suitable for patients and develop health literacy interventions. Furthermore, the Internet as a major source of health-related information among patients with IBD 20 and health literacy-based interventions, such as patient-centered communication, can help prevent negative health outcomes. 21
As expected, participants who watched the high-quality content (Groups 1–1 and 2–1) showed an overall increase in health literacy and behavioural intentions. Given that videos convey information better than text and are more effective for learning,2,22 the results of this study demonstrate that high-quality YouTube content has an educational effect. As YouTube content might have a direct impact on patient health and good potential for use as a 24/7 freely accessible educational resource, 23 it is important to provide quality and reliable health information. This is also supported by our finding that higher information reliability is associated with greater improvements in health literacy and behavioural intentions.
The randomized controlled trial was conducted on two distinct topics: interpreting laboratory test results from health check-ups (Groups 1–1 and 1–2) and providing general information about IBD (Groups 2–1 and 2–2). Neither health literacy nor health behavioural intention changed in Group 1–2, a group that watched the low-quality content. A large proportion of patients often experience insufficient post-check-up follow-up, including inadequate explanations of health check-up results and a lack of advice or preventive care.24,25 Based on a previous finding that patients with higher health literacy are more likely to attend health check-ups and recognize the risk of illness, 26 it is hoped that YouTube will be used as a platform to improve health literacy and take further preventive action. Conversely, Group 2–2, which watched lower quality content, showed increase in health behavioural intention although it was not statistically significant (3.65 to 3.72, p = 0.253). Although the content provided for Group 2–2 was poorly rated by medical experts as providing relatively less medical information, the video shared the symptoms experienced by patients with IBD. This is consistent with previous research indicating that health information seeking and sharing among patients with rare diseases influence their health behaviours in everyday life. 20 Patients with IBD usually seek online information regarding the nature and cause of the disease, self-diagnosis, and treatment options. 27 It is difficult to obtain information from medical experts in busy clinical settings; therefore, the Internet may be the easiest way to obtain health information without encountering medical professionals. 27 In general, Group 2 had a higher mean baseline health behavioural intention than Group 1, suggesting that patients with IBD have a higher commitment to health behaviour. As IBD is sufficiently preventable and treatable through continuous lifestyle modifications and dietary management, 28 it is essential for patients to easily access detailed and high-quality clinical information that can guide them in managing their daily lives.
Information accuracy is always an issue when utilizing YouTube content as a health information source. Numerous medical institutions and associations upload various categories of health content on YouTube to provide health information, communicate with patients, and promote their services. 20 Furthermore, we found there were some videos with higher DISCERN scores had lower viewing ratios. As videos with high-quality informative content have a significantly lower number of views than videos with low-quality informative content, it would be helpful to properly combine the characteristics of videos that received the highest quality evaluations and the highest number of views in this study: patients’ questions based on real-world experience with answers or solutions from medical staff are a good example. Content created in this direction will attract public attention and serve as a good source of medical information to help improve health literacy and health.
This study justifies the importance of providing health information, the accuracy of which has been verified through an expert quality evaluation. While health literacy increased in Groups 1–1 and 2–1 after watching YouTube content, it decreased in Groups 1–2 and 2–2 even though the provided content had been quality checked once and preselected based on the GQS. Considering that the GQS was not conducted by medical professionals, this could be evidence that quality evaluation by medical professionals is important because it is directly related to the improvement of patient health literacy and health-related behaviours. Furthermore, information reliability positively affects both health literacy improvement and health behavioural intention. This suggests that the reliability of the video, which has been verified by experts, is likely to lead patients to acquire more health information and link it to their health behaviour. Therefore, while expert quality evaluation is important, it is also necessary for experts to conduct health information quality evaluations with greater responsibility and a sense of duty. Owing to the nature of the video platform, which is easily accessed by both medical and non-medical professionals, there is a possibility that the average quality of YouTube videos as a medical information source might be relatively low. 29 Although patient access to misinformation cannot be restricted, they can be guided by providing high-quality videos with evaluation rates. 20 Therefore, it may be worth considering building more automated quality assessment algorithms to help patients curate and access high-quality health information.
Given the increasing attention garnered by medical and health information content, the systematic exploration of health literacy and health behaviour has become crucial. We sought to provide evidence to protect patients who may have been exposed to substantial amounts of unverified or quality-controlled medical and health information online. To the best of our knowledge, this is the first randomized controlled trial to assess the efficacy of quality-controlled YouTube content in enhancing health literacy and behavioural intention. Through our comprehensive analysis, we aimed to investigate the importance of ensuring the quality and reliability of health information available on online platforms and provide insights that can be used to improve patients’ health literacy and informed decision-making. However, this study has some limitations. First, even for the same health information content, the quality score may be evaluated differently depending on which expert evaluates the content. 30 Second, 7 out of 16 evaluation items of DISCERN enquired about treatment options; therefore, videos that did not discuss treatment may have been poorly evaluated, even though clinical aspects, risk factors, diagnosis, prognosis, and prevention were sufficiently provided. Third, the study was conducted with those who were able to watch the designated YouTube content and complete an online survey. As baseline digital literacy of this group may be higher than that of the general population, it might be difficult to generalize the study results. Finally, this study did not examine the relationship between watching quality-controlled content and health outcomes. Thus, further studies on various health-related outcomes should be conducted.
Existing studies have primarily focused on evaluating and interpreting the quality of online health information; this study is noteworthy in that currently distributed and easily accessible YouTube videos were thoroughly evaluated to determine whether high-quality online health information can aid in improving the health literacy and health behavioural intentions of participants. In the future, the results of this study can be used as a cornerstone for various health-related environments that require quality evaluations. It is necessary to provide continuous opportunities for patients to access high-quality health information that can have a decisive effect on their health.
Conclusion
In conclusion, our randomized controlled study demonstrates the pivotal role of high-quality online health content in improving health literacy and fostering health behavioural intentions among diverse groups, including those seeking health check-up information and individuals grappling with conditions like IBD. This research underscores the importance of ensuring the reliability and accuracy of online health information, particularly on platforms like YouTube. Our findings emphasize the potential of such content as an accessible and educational resource for individuals navigating health-related decisions. Moreover, this study highlights the need for expert quality evaluation of online health information and its positive impact on users’ health literacy and health-related intentions. As the digital landscape continues to evolve, these insights serve as a foundation for developing strategies to enhance patients’ health literacy, promote informed decision-making, and ultimately contribute to improved health outcomes. However, we acknowledge the limitations of our study and suggest further research exploring the relationships between online health information, health literacy, and health outcomes to better inform healthcare practices and patient education in the digital age.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241263691 - Supplemental material for Quality controlled YouTube content intervention for enhancing health literacy and health behavioural intention: A randomized controlled study
Supplemental material, sj-docx-1-dhj-10.1177_20552076241263691 for Quality controlled YouTube content intervention for enhancing health literacy and health behavioural intention: A randomized controlled study by Yujin Park, Su Hwan Kim and Hyung-Jin Yoon in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank all the study investors and research coordinators.
Contributorship
YP contributed to the conception and design of the study, acquisition of data, analysis and interpretation of data, and drafting the article. SHK revised the article for important intellectual content, and HJY made final approval of the version to be submitted.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant of the Korea Health Promotion R&D Project, funded by the Ministry of Health & Welfare, Republic of Korea (grant number : HS22C0061).
Guarantor
YP and HJY.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.