
Abstract
Objectives
Telemedical applications are solutions to challenges in the healthcare system. However, it is unclear what intensive care unit healthcare professionals expect from such solutions. This study investigated the expectations and concerns of nurses and physicians when implementing telemedicine tools in intensive care units (tele-ICU).
Methods
The study was conducted in intensive care units in 2020 during the second wave of the COVID-19 pandemic. It used a mixed-methods approach targeted at physicians and nurses and involved 14 qualitative interviews and 63 quantitative questionnaires.
Results
The qualitative and quantitative data showed that both nurses and physicians were willing to use tele-ICU. Nurses recognised the advantages of real-time access to expertise offered by tele-ICU, but feared this would reduce physicians’ on-site patient time. Physicians, in turn, were concerned that they would be expected to be continuously on call. The majority in both groups agreed that any tele-ICU solution must be simple to use and integrate easily into existing organisational structures, networks, and work routines. Additionally, COVID-19 significantly influenced expectations: those who reported having more personal health concerns during the pandemic were more predisposed to favour the use of tele-ICU.
Conclusions
Overall, tele-ICU supports better care, but a successful implementation depends on its ease of use and context-sensitive approaches. Effectively integrating tele-ICU solutions into daily clinical routines requires input from nurses and physicians and their involvement in the implementation process from the outset, as well as consideration of existing organisational structures. Such measures will vastly increase the chance of acceptance and successful adoption of telemedical solutions in clinical practice.
Introduction
The COVID-19 pandemic revealed both the scale of the challenges posed by a global healthcare crisis and the fact that some national healthcare systems were ill-equipped and unprepared to handle them.1–3 These challenges were further exacerbated by the demands on healthcare systems caused by technical, staffing, and infrastructural limitations, which predated COVID-19.4–10 Although countermeasures were quickly taken to prevent healthcare systems from collapsing during the pandemic, COVID-19 showed that all over the world, and particularly in intensive care units (ICUs), healthcare systems were struggling with severe issues of resource scarcity. These included shortages of well-trained physicians and nurses and equipment.11,12 Telemedicine, including telemedical tools for ICUs, is seen as a potential solution to some of these difficulties.13–15
Telemedical tools allow healthcare to be delivered remotely. They enable a diverse array of applications, such as remote monitoring, transmission of medical data, and consultation with physicians.16–18 The value of telemedical tools in crisis situations makes them ideal for use in critical care settings (tele-ICU), where they connect off-site specialists with on-site staff (e.g. during medical emergencies).19–21 Tele-ICU typically involves the use of audio-visual technology and monitoring systems to assist physicians and nurses in the ICU, for example, by virtually connecting external specialists who can share their expertise during consultations on complicated cases.22–24
Ever since the publication of the study of Rosenfeld et al. 25 in 2000 and its positive findings on tele-ICU outcomes, the body of literature analysing its potential benefits as well as its barriers has grown considerably. Positive outcomes include a reduction in mortality, shortened length of stay (LOS), reduction of costs, and better adherence to best-practice protocols.26–30 Meta-analyses by Young et al. 31 and Chen et al. 32 supported these propositions. Other studies identified barriers, such as high costs or staff perceptions of telemedicine utility.33–35 Khurrum et al., for example, showed how ICU healthcare professionals sometimes viewed tele-ICU critically. 36 This highlights the need to identify and consider both enabling and inhibiting factors when implementing telemedicine in order to realise the potential benefits of this technology.37–39
Telemedicine access capabilities garnered increasing attention during the first phase of COVID-19 in 2020, when many medical wards, hospitals, and other medical services restricted in-person visits and consultations.40,41 A survey carried out by Peine et al. 42 showed that medical staff in Germany broadly accepted this measure during COVID-19. Telemedicine increasingly moved into the spotlight as a means of reducing contagion. 43 A subjectively perceived risk of contagion could, therefore, positively influence attitudes towards telemedicine.
Telemedicine is by no means the only technological driver for developments in ICUs. Particularly in recent years, due to rapid developments in artificial intelligence, robotics and the “Internet of things”, new models of intensive care units have emerged and called “intelligent care units” or “smart ICUs”. Many of these models are still based on the same fundamental consideration as telemedicine: obtaining information from experts who are not currently on site and acting accordingly.44,45
Technology acceptance of healthcare professionals is the key for the successful implementation of technological solutions like telemedicine or even more advanced technological solutions. Previous professional experience may strongly influence attitudes towards telemedicine. Generally, senior healthcare professionals rely more on their own expertise than on external input (e.g. via telemedicine46,47) and might, therefore, be more critical about its use. This is supported by Ahmed et al. 46 who identified more positive attitudes towards telemedicine among less experienced nurses than more senior nurses and supervisors.
Positive attitudes towards tele-ICU solutions could also be linked to more personal factors and attitudes. Some studies showed a greater willingness to use innovations like telemedicine, where job satisfaction is high, 48 although this relation could be more complex. 49 The willingness to implement tele-ICU solutions may also reflect a more general inclination to use technology. 50 Furthermore, nurses and physicians may view the same technology differently. Previous studies showed that different areas of expertise and working structures (e.g. due to profession) in the medical setting result in qualitatively different forms of use, motivation, and expectations of technological tools. This calls for a comparison of these two professional groups. 51
Critically, the above list of potentially influencing factors is not exhaustive and could be more heterogeneous. In order to achieve a more nuanced and in-depth overview of the influencing factors, we opted to conduct this research by triangulating methods and combining qualitative and quantitative research. The qualitative interviews bring detailed insights into daily routines, challenges, and individual insights. The quantitative data provide an overview of the expectations associated with tele-ICU and how these may be influenced by the factors outlined above. By approaching the expectations associated with the use of tele-ICU from multiple research angles, we can arrive at more comprehensive, reliable, and valid conclusions.52,53
Overall, using tele-ICU can bring positive health and economic outcomes and has great potential for alleviating some of the pressure in critical care settings. However, the expectations healthcare professionals have of the benefits and disadvantages of using these solutions are less clear. Consequently, the main aim of this study is to identify those expectations that encourage or inhibit the use of tele-ICU solutions. This is achieved by examining how these expectations are related to the level of professional experience, job satisfaction, areas of responsibility, and impact of COVID-19.
Methods
The study was conducted at the ICUs of the Medical University/General Hospital of Vienna (Allgemeines Krankenhaus: AKH). The AKH houses 140 systemised intensive care beds on 15 wards, representing the largest concentration of ICUs in Austria, and has not yet implemented any large-scale, standardised telemedicine solutions before the pandemic. 54 The study ran from October 2020–January 2021 and, therefore, included the second wave of the COVID-19 pandemic in Austria. The study was approved by the Ethics Committee and the Data Protection Commission of the Medical University of Vienna (ECS 1256/2020).
Both qualitative and quantitative studies focus on the expectations of telemedicine. We did not provide study participants with a set definition of “telemedicine” in the ICU. Given the exploratory nature of the study, we aimed to see telemedical application options the participants would or could envision both as providers and as recipients of telemedical support and supervision. All participants reported prior experiences with telemedicine, ranging from low-tech options like remote (phone) support to more high-tech support like expert boards with vitals or patient records shared.
Qualitative data collection and analysis
Participants
To obtain the qualitative data, we followed COREQ, the consolidated criteria for reporting qualitative research. 55 ME (PhD, female, extensive training in qualitative methods as a social scientist) conducted individual in-depth interviews until thematic saturation was successfully reached. 56 This resulted in a total of 14 interviews, seven with ICU physicians and seven with ICU nurses. The range of ages and years of professional experience were typical for AKH hospital staff: 30 to 60 years old, and 5 to over 30 years of experience. The interviews were held either in person or via Zoom, as chosen by the interviewee. Each interview lasted between 35 and 120 min and followed a predefined structure. Interviewees took part voluntarily following a general email request issued to ICU ward staff by the research team. Participants were assured that the data would be processed anonymously, and each signed a consent form prior to the interview.
Interview & analysis
The interviews were conducted using guided questions about current professional responsibilities, and expectations of and concerns about telemedicine. It intentionally allowed participants to describe the telemedicine solution that came to mind. All interviews were conducted, recorded, and transcribed in German. Selected quotes were translated into English for this article, with the accuracy of the translation checked by two native English speakers. We also followed the COREQ structure in the subsequent analysis. The coding was performed by a research team of three using printed versions of the transcribed interviews. In the first step, the researchers coded separately. The results were then compared and discussed. Where necessary, new codes and sub-codes were created following joint discussions between the three researchers. After familiarising ourselves with the data and obtaining a general overview, we established 44 final codes (10 main codes and 34 sub-codes, see Appendix (Table 1) to focus on the areas with the greatest impact on the research question. 57 Themes emerging from the codes and sub-codes were used to inform the section on qualitative results. The results of the interviews were structured into four overarching themes identified using the detailed coding process. Supporting quotations were directly marked. 55 We then discuss how these findings offer insights into issues requiring consideration when introducing tele-ICU.
With respect to the strategy of mixed-method analyses, we adopted a sequential approach and analysed the qualitative data first. 52 Following the theoretical considerations outlined in the introduction, this data then informed decisions about the statistical analyses of the quantitative data.
Quantitative data collection and analysis
Quantitative questionnaire
A questionnaire set consisting of psychometrically standardised and validated questionnaires,50,58 self-generated questions (tele-ICU expectations, personal health concerns, and distress), and socio-demographic questions was used to evaluate the expectations from tele-ICU and possible influencing factors.
The two standardised questionnaires were: 10 items from the Neyer et al. 50 short scale (Cronbach α=.791) to quantify willingness to use technology. Job satisfaction was measured using the short version of the Fischer and Lück 58 scale. Both used five-point Likert scales (1 = high, 5 = low).
Additionally, a panel of experts consisting of five researchers (psychologists, social scientists, physicians, and nurses) developed a questionnaire to capture the following four overarching aspects about telemedicine:
Expectations towards tele-ICU solutions: Expectations were measured using eight items on a five-point Likert scale (1 = low expectations, 5 = high expectations) and by computing an average score. Reliability was good (Cronbach α=.850). Effects of telemedicine on expected patient numbers: Respondents were additionally asked whether they expected tele-ICU to impact patient numbers (1 = significantly more, 2 = slightly more, 3 = about the same number, 4 = slightly less, 5 = significantly less). Benefits and concerns about telemedicine use: In two additional items, respondents indicated whether they considered tele-ICU solutions to be beneficial or whether they were giving rise to concerns, requiring responses in a binary format (yes/no). Questions related specifically to COVID-19: With respect to the impact of COVID-19, questions were included to report both pre-pandemic and pandemic-related levels of health concerns and general distress. Answers were given on a 10-point Likert scale (1 = low distress/low concern, 10 = high distress/high concern).
Overall, the questionnaire was pilot-tested with a physician and nurses from our research group.
The final questionnaire consisted of 48 items and was completed online (q-set.de), taking participants around 15 min to fill in. Informed consent was obtained from each participant prior to starting the questionnaire.
Participants
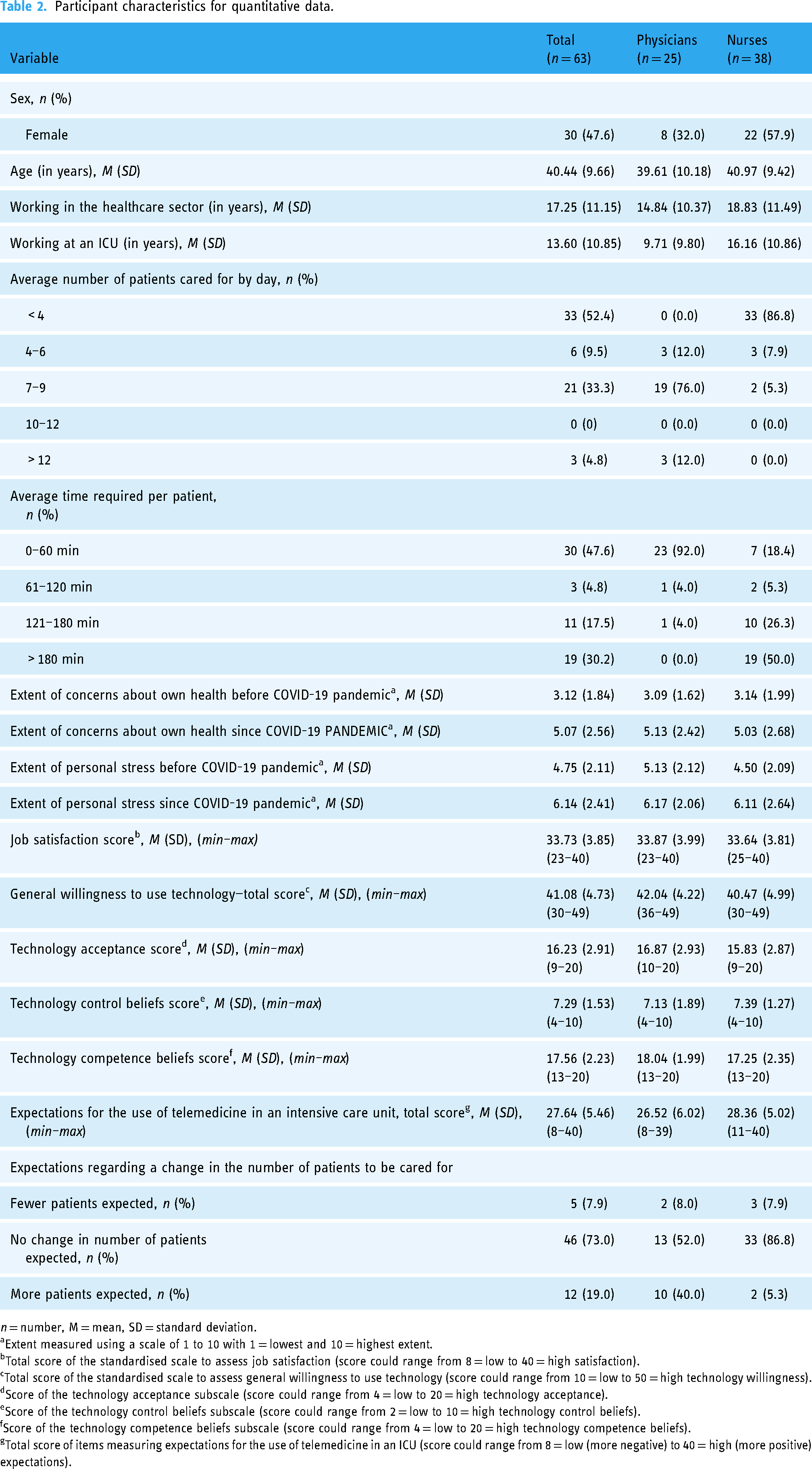
Emails were sent to 580 ICU healthcare professionals on an AKH management distribution list. A total of 63 health professionals completed the questionnaire in full, representing an estimated response rate of 11%: 38 (60.3%) were nurses, and 25 (39.7%) were physicians. The mean age of the respondents was 40.4 ± 9.7 years, and 47.6% (n = 30) was female. The mean number of years spent working in an ICU was 13.6 ± 10.8 years. Participant characteristics are displayed in the Appendix (Table 2).
Analysis strategy for quantitative data
The quantitative data are reported in three sections. The first two sections were informed by two topics that emerged as a result of the qualitative analyses and theoretical considerations outlined in the Introduction, namely, (1) the relation between age/professional experience and telemedicine and (2) group differences between physicians and nurses.
Firstly, with respect to the relation between age/professional experience and telemedicine expectations, Pearson correlations were calculated (see Results 1). Secondly, to assess group differences between physicians and nurses, we calculated the group comparisons (independent t-tests) for job satisfaction, willingness to use technology, and expectations of telemedicine. Furthermore, for the two binary outcome variables, namely, telemedicine seen as beneficial or causing concerns, we report group comparisons (physicians vs. nurses) based on Chi-squared tests (see Results 2: Differences due to profession).
Thirdly, in the last analysis step (Results 3: Effects of COVID-19) we considered the possible effects of the COVID-19 pandemic. These were measured using self-reported health concerns and general distress before and during COVID-19. We calculated dependent t-tests to test for changes resulting from COVID-19. Finally, we report Pearson correlations to analyse the effects of these variables on telemedical outcome variables (i.e. expectations of telemedicine, benefits of use, and concerns about use).
All analyses were conducted in R and R-Studio.59,60 Figures were plotted using the ggstatsplot package, 61 which allows raw data to be shown together with visualisations of data centrality (e.g. mean, median, percentages) and data dispersion (e.g. combined box and violin plots). This package also directly performs statistical tests (e.g. Chi-squared test, t-tests, etc.). For reasons of parsimony, the statistical outcomes (i.e. significance tests and effect sizes) from this package are directly reported within the associated figures.
Findings
Results—qualitative analysis
The qualitative analyses identified four overarching themes: (1) age and professional experience in relation to technology acceptance; (2) professional differences (nurse vs. physician); (3) technical expectations; and (4) interpersonal and organisational networks.
Finding 1: technology acceptance related to age and professional experience
Our interviews reveal a complex matrix of expectations of tele-ICU solutions both between and within different age groups. Younger healthcare professionals often perceive opportunities, associating the use of tele-ICU tools with increased safety, both for themselves and their patients. The option to contact other possibly more experienced healthcare professionals would provide reassurance in their decision-making or help in choosing the best course of action. Older and more experienced healthcare professionals sometimes viewed tele-ICU measures more critically, for example, feeling obliged to use them and perceiving this as monitoring or control by superiors. Although a complex set of factors influences technology acceptance, of which age and professional experience are just one aspect, the interview data indicated that this must be considered as a highly relevant aspect. For example, one interviewee stated: “New employees would most likely be grateful (for telemedicine). But there will also be many who say that this is not necessary for them. It makes it appear as if they don’t know something, and they wouldn’t want others to think that.” (Interview three, physician)
Finding 2: professional differences
Although nurses and physicians in ICU units are similar in being highly qualified and skilled professionals in their respective fields, accustomed to the high-pressure working environment, and working closely within multidisciplinary structures and teams, our qualitative data indicated noticeable differences in their attitudes towards telemedicine.
In our interviews, physicians, even those generally in favour of introducing tele-ICU, expressed concerns about the effects of a new technology on their workload. Specifically, they expressed the fear of being expected to be always “on call”, even outside work and on-call hours, and that nursing staff and/or less experienced physicians would overuse the option to contact them when they needed reassurance or a second opinion: “Pushing the senior physician into the background, that he (sic!) will only be consulted in some cases as an expert and perhaps actually have more work, because the attitude is that, well, then we actually no longer need one physician for two ICUs, but he can do four at once because he will be able to sit in his room. This would be a little bit of a dangerous dynamic, so to speak.” (Interview seven, physician)
One interviewee added that for this cross-professional exchange to work, some changes in the current system might be necessary: “But you would also perhaps slightly flatten hierarchies, with more senior physicians willing to source expertise from nurses,” adding that, “respectful communication is a basic prerequisite for the successful use of telemedicine.” (Interview nine, nurse). “Fears regarding anything that is unclear need to be addressed, such as the possibility of an increased workload.” (Interview seven, physician) “If left unaddressed, differences in communication style could result in the use of telemedicine to access expertise being rejected, even where patients might benefit.” (Interview fourteen, physician)
Finding 3: technical expectations and requirements
Our data show that when new (telemedical) technologies have been introduced into intensive care units in the past, key factors influencing their acceptance, such as ease of use and suitability for clinical use (e.g. easy to disinfect), have often been overlooked, rendering the technology impracticable.
According to the interviews, specific technical requirements and criteria are crucial for telemedicine's acceptance in the ICU. They particularly stressed the importance of ease of use. Previous experience showed that new technologies introduced into the hospital setting were only used in daily routines if they were easy to log into, intuitive to use, and provided a clear benefit. Even tools that offered a medical benefit were often abandoned if the hardware or software was not easy to use. As one interviewee stressed: “If [the tool] is easy and people like using it. If the number of technologies just increases and the path to using them becomes more onerous, people will have difficulties accepting them. People need to say, ‘It used to be terrible, but now it's better’.” (Interview five, physician)
Regarding suitability for clinical use, ICUs house extremely vulnerable patients: “We treat patients with one or more non-functional organs.” (Interview three, physician)
Finding 4: interpersonal and organisational networks supporting technology
One central finding regarding the successful implementation of tele-ICU is that a perfect technological solution and ease of use are only a part of the equation. The related structures, regulations, and networks that support the use of telemedicine must be in place if tele-ICU is to be truly established.
As one participant said: “One would probably need to develop a certain framework, stating what the specific task of a telemedical practitioner is and what consequences a consultation or given advice has.” (Interview two, physician). “You have to prepare (the introduction of telemedicine) in such a way that it is not seen as failure or defeat to contact someone else.” (Interview four, nurse) “Creating clear structures, and addressing fears related to uncertainty” would be key steps in establishing any telemedical tool in an ICU (Interview seven, physician). “It could easily be accomplished within a year, at the very latest.” (Interview four, nurse) “A lot of organisational work will be needed behind the scenes. After all, one can’t just consult arbitrary people.” (Interview five, physician)
Results—quantitative analysis
Results 1: correlations—what variables influence expectations of telemedicine
Figure 1 shows the correlational results. Apart from substantive and significant correlations between years of professional experience (ICU and health system) and age, which are clearly dependent, the experience and age variable was barely related to expectations about telemedicine, benefits, concerns about telemedicine use, expectations of reductions in patient numbers caused by the use of telemedicine, or a general willingness to use technology. The only other significant correlations concerned general expectations about telemedicine, which went hand-in-hand with higher expected benefits and fewer concerns.
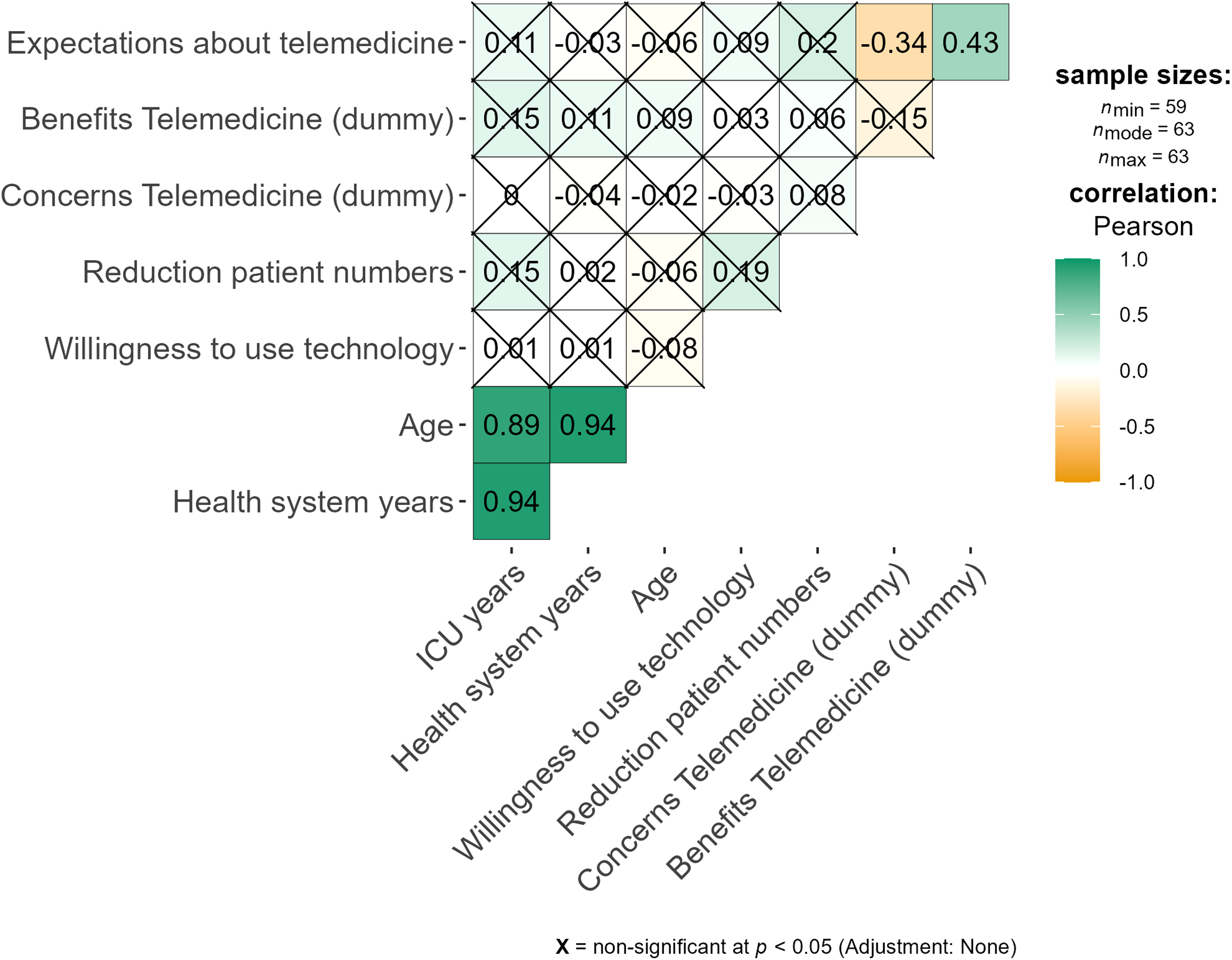
Correlations between professional experience/age and expectations of telemedicine and technology.
Results 2: differences due to profession: physicians vs. nurses
There was no significant difference between nurses and physicians (Figure 2, t-tests, Welch procedure to account for unequal variances) with respect to the reported levels of job satisfaction, willingness to use technology, or expectations of telemedicine. Generally, in terms of individual outcomes, on average, both physicians and nurses reported reasonably high levels of job satisfaction and willingness to use technology. The range of individual ratings only varied within the upper and mid-points of the scale. Overall, job satisfaction and general willingness to use technology were generally high among both physicians and nurses.

Differences in job satisfaction, willingness to use technology, and expectations of tele-ICU by profession.
Although the difference in expectations of telemedicine was not statistically significant, descriptively, nurses (mean = 2.50, median = 2.38) reported slightly higher expectations of telemedicine in ICU settings compared to physicians (mean = 2.71, median = 2.88). The range of individual ratings varied considerably from very high (1) to very low (5), suggesting highly idiosyncratic expectations.
When looking at general benefits and concerns related to telemedicine, overall, there were no significant differences between physicians and nurses in the rate of ‘yes’ and ‘no’ responses (Chi-squared test). For benefits, the rates within professions were very similar—almost all physicians (p < . 05) and almost all nurses (p < . 05) perceived benefits in using tele-ICU. For concerns, however, an interesting pattern emerged. The rates for physicians were at par (p = .84), whilst the majority of nurses reported no concerns (p < .05). See Figure 3.

Benefits and concerns of using tele-ICU by profession.
Results 3: Did COVID-19 affect expectations?
Comparing COVID and pre-COVID levels, participants reported greater health concerns, t(62) = −6.5, p < .01, and a higher general level of distress, t(62) = −5.7, p < .01. The greater health concerns during COVID-19 were indeed correlated with higher expectations of telemedicine (Figure 4, r = −0.33, p < .05). There were no substantive correlations between telemedicine expectations and concerns before COVID (r = −0.13, n.s), distress before COVID (r = 0.15, n.s.), or distress during COVID (r = −0.15, n.s) and the variable of telemedicine expectations.
Discussion and recommendations
The main aim of the study was to identify favourable and inhibiting factors for tele-ICU solutions. By triangulating qualitative and quantitative data, our study identified a complex set of factors influencing expectations of the use of tele-ICU. The findings highlight factors relevant to decision-making processes and change management, which go beyond the technological solution of implementing tele-ICU. We discuss these findings and conclusions in detail.
Age and professional experience
In the first topic discussed in our study—the influence of age and professional experience on willingness to use tele-ICU solutions—qualitative and quantitative data showed some differences, showcasing the benefits of a mixed-methods approach. We did not find any substantial correlations between age/professional experience and willingness to use tele-ICU in the quantitative data, although previous studies have found this link. 62 However, the qualitative data offer a more detailed and layered view as it allowed participants to factor in aspects of teamwork and organisational culture. Specifically, age and experience-related factors influence the use of telemedicine. This may be because more experienced employees strategically choose technology that will truly add value rather than using it merely due to its availability. 63 Similarly, our study found that a connection between age and willingness to use telemedicine is based on factors, which are not necessarily only related to technology use itself, but also to social structures, hierarchies within the team, and attitudes towards making mistakes. Our interview data showed that possible concerns about older individuals and the use of telemedicine do not necessarily stem from them being less willing or able to adapt to the use of new technology, but rather due to concerns about how using telemedicine might negatively reflect on their abilities. Hence, whilst younger and less experienced employees particularly see tele-ICU as a means of increasing patient safety and improving professional skills, older and more experienced employees see their expertise and professional independence threatened by unsolicited, external interference.
Commonalities and differences between professions—nurses and physicians
Our data show that professional differences—being a nurse or a physician—is an important aspect of expectations of tele-ICU. In general, both groups reported similarly high levels of job satisfaction and a high degree of willingness to employ technologies, such as telemedicine. This is not unexpected as using complex technological solutions are an inherent aspect of working in ICUs. Consequently, both professional groups were open to tele-ICU solutions and valued the option to contact other readily available or possibly more experienced healthcare professionals using tele-ICU, as indicated by both the qualitative and quantitative data.
However, there were also some notable differences. Overall, nurses adopted a slightly more positive attitude towards tele-ICU solutions. According to our data, nurses tend to see more benefit from sharing, whilst physicians, especially more experienced ones, tend to be more wary of interference. One repeatedly stated concern was having to be constantly available for (ad-hoc) consultations. This was also reflected in the quantitative data. These examples indicate the potential for disagreement between the two groups when negotiating the use of new technologies. Ideally, a successful implementation of telemedicine would involve a discussion of underlying professional differences, with possible solutions explored.
When asked about the benefits, both groups unequivocally recognised the benefits of tele-ICU solutions. However, with respect to concerns, the majority of nurses reported having no concerns, but this was the case only for roughly half of the physicians. This finding qualifies the study by Avdalovic and Marcin, 64 which showed that whilst some healthcare professionals see their expertise and professional independence threatened by unsolicited outside interference, and others see it as an opportunity to enhance patient safety and improve their professional skills, these differences can be primarily attributed to the professional group. The ambiguities described above—benefits of sharing, fear of interference, increased workload—also map well to the systematic literature review by Ramnath et al.: in their review, the perceptions of telemedicine ranged from improved teamwork and additional night-time support to poor communication and interruptions. 28
Technology acceptance and organisational structures
Throughout our qualitative interviews, three central topics emerged: ease of use; established organisational structures; and options for involvement in the implementation process. The interviewees stated that a new telemedicine application should be uniformly integrated into existing IT systems, show a clear advantage over existing technologies, and “appropriate organisational infrastructure needs to be provided”. 65 These are in accordance with previous studies (e.g. Gagnon et al. 65 and Deisz et al.) 66 It is important to involve various professional groups and ascertain specific expectations and views prior to purchasing and implementing solutions. Additionally, implementation processes need to be based on a functioning network and internal structures. Our data show that the necessary systems and network(s) should be prepared and established in advance to guarantee a smooth implementation process and long-term, successful use of the chosen tool. The importance of additional steps taken prior to implementation has already been addressed in several studies underlining the necessity of early-stage training and support systems.31,64 Involving ICU employees at an early stage in deciding which telemedical tools to purchase can help ensure that the tools will be used. Existing organisational networks can also be leveraged during the implementation of new telemedicine processes to gain input on robust communication and familiarity with workflows, 13 as found in our qualitative study. Consequently, clear structures and workflows are essential, with both nurses and physicians involved as early as possible, together with other relevant professions, in implementing tele-ICU solutions.
Significant work needs to be done by the management to connect the right people via telemedicine to create a robust telemedical network of experts. After all, telemedical tools are only of value when the relevant people can be reached with ease when needed. This could take different forms depending on the ICU setting in question, such as connecting several ICUs or linking ICU employees to experts working in other hospital departments or to experts outside the hospital. Assessing the type of expertise that would bring the most benefit to the ICU in question and building a suitable network of people to provide this expertise are perhaps the most important steps in establishing tele-ICU.
Additionally, our data highlighted the need to create an environment of trust when following the therapeutical recommendations provided via telemedicine. Accordingly, hospital policies need to be explicitly communicated and employees ensured of their validity. Clear communication of the policies for tele-ICU is a crucial step towards achieving broad acceptance and use of the chosen tool. What is also required is a greater willingness to ask for help.
There must be a network of experts with whom there is either an established relationship and/or an agreement for the exchange of expertise through telemedicine. If these relationships are in place, and it is clear when particular experts can be reached through on-call lists, for example, then there is a much higher chance that the telemedical technology will be used in the ICU. If these factors are considered, a well-established telemedical expert network could have multifold benefits to ICUs and beyond.
Effects of COVID-19
The study was conducted during the second wave of the COVID-19 pandemic in Austria. The hospital used in the study served as a primary location for COVID-19 intensive care patients, with two of the six ICUs dedicated to ICU COVID-19 care. Presumably, this increased awareness of the possible benefits of telemedical solutions. Indeed, in our study, a greater concern for personal health during this testing period was statistically related to higher expectations of telemedicine, as other studies have also shown. 67 This relation was not significant when participants were asked to consider their pre-COVID-19 health concerns. In the qualitative interviews, participants arrived at similar conclusions. Additionally, ICU employees were acutely aware that hospitals are in dire need of new strategies to foster resilience during (future) crises. Telemedicine may be one, although not the only solution for accessing external expertise when ICU employees are unavailable (sickness, quarantined during COVID-19, etc.). Thus, a functional telemedical system can help access expertise, potentially from a global network, to provide optimal treatment for complex medical cases, which are common in ICUs.
Limitations
This study has several limitations. The study was carried out in Austria's largest university hospital, which is known for its specialised centres and high patient volume. This setting ensured consistency in work practices, organisational structures, and allowed for easy access to numerous ICU healthcare professionals. This is necessary as return rates for (quantitative) online studies are generally low. Our study had an 11% return rate (63 participants for the quantitative analyses), which is within the range of similar studies. 68 The variation in ratings for expectations of telemedicine (Figure 2) extended across the entire possible range, with a higher density around the mean, as might be expected by random selection. The qualitative interviews also showed that opinions of tele-ICU among ICU healthcare professionals were diverse and differentiated. This suggests that our data were free of a bias that attracts primarily people with intrinsic interest in telemedicine. Another caveat is that the hospital is a university hospital; hence, a disproportionately high level of curiosity about innovation and an affinity for technology might be assumed. Furthermore, the study was conducted in a multi-centre, city-based hospital. In smaller, less specialised, or more rural hospitals with less patient throughput, different sets of background factors might influence attitudes towards tele-ICU. Consequently, our study findings and conclusions should be not uncritically extrapolated to other hospitals or clinical environments. Nonetheless, some identified factors, such as the need to incorporate solutions on an organisational and personal level, can be considered valid in a broad range of settings.
In order to maintain anonymity, we did not explicitly ask whether or not the participants had taken part in both sections of the study. Some participants mentioned that they had. We do not believe this influenced the outcomes as the quantitative and qualitative studies were not conducted in direct succession. Finally, whilst most interviews were conducted in person at the hospital (10 interviews), due to interviewee preferences, four of the interviews were conducted remotely via ZOOM. Although it was slightly easier to establish a personal connection during in-person interviews, interviewers did not feel this affected the outcome.
Conclusions
The main findings of our study can help aid future strategies for implementing telemedicine in intensive care settings. We found that the value of even the best potential telemedical ICU technology is highly dependent on the organisational network and structures in which it is embedded. Furthermore, an organisational shift is needed, which reframes requests for support and external opinions as a means of ensuring excellent patient care and perhaps fostering continuous professional development. Assuming these “soft” factors of organisational culture and human networks are in place, the telemedical technology must be integrated into existing processes and structures as seamlessly as possible, be easy to use, and simple to keep sterile. Our findings also highlight the importance of considering the different groups of ICU employees (and hospital employees more generally), and showing which implementation measures could be tailored to more hesitant groups. This will allow for targeted measures to support individual employees during the implementation phase of telemedicine, rather than providing a one-size-fits-all training for all employees. This might include voluntary measures, such as training, in technology use for those wishing to participate. Not only does this give employees agency, it also saves personnel resources in often-overworked ICU settings by not requiring the participation of employees already comfortable using telemedicine. Adopting these changes will make the health system more resilient to future labour shortages and health crises.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241257042 - Supplemental material for Focusing on experts: Expectations of healthcare professionals regarding the use of telemedicine in intensive care units
Supplemental material, sj-docx-1-dhj-10.1177_20552076241257042 for Focusing on experts: Expectations of healthcare professionals regarding the use of telemedicine in intensive care units by Magdalena Eitenberger, Gernot Gerger, Sophie Klomfar, Marcus Alexander Gabriel, Maria Kletecka-Pulker, Eva Schaden, Atanas G Atanasov, Mathias Maleczek, Sabine Völkl-Kernstock and Elisabeth Klager in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241257042 - Supplemental material for Focusing on experts: Expectations of healthcare professionals regarding the use of telemedicine in intensive care units
Supplemental material, sj-docx-2-dhj-10.1177_20552076241257042 for Focusing on experts: Expectations of healthcare professionals regarding the use of telemedicine in intensive care units by Magdalena Eitenberger, Gernot Gerger, Sophie Klomfar, Marcus Alexander Gabriel, Maria Kletecka-Pulker, Eva Schaden, Atanas G Atanasov, Mathias Maleczek, Sabine Völkl-Kernstock and Elisabeth Klager in DIGITAL HEALTH
Footnotes
Acknowledgements
We would like to thank all participants for taking time to contribute to our research amidst the COVID-19 pandemic.
Contributorship
ME: Conceptualization, Methodology, Data collection, Data analysis, Writing Original Draft, Project Management; EK: Conceptualization, Methodology, Data analysis, Writing Original Draft; MG: Research, Data analysis, Writing Original Draft; SK: Methodology, Data collection, Data analysis, Writing Original Draft; GG: Data analysis, Writing Original Draft; MK-P: Supervision, Review of Draft; ES: Supervision, Distribution of Online-survey, Review of Draft; AGA: Review of Draft; MM: Review of Draft; SV-K: Data collection, Supervision
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was confirmed by the Ethics Committee and the Data Protection Commission of the Medical University of Vienna (ECS 1256/2020).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
ME
Supplemental material
Supplemental material for this article is available online.
Appendix
Participant characteristics for quantitative data.
| Variable | Total |
Physicians |
Nurses |
|---|---|---|---|
| Sex, n (%) | |||
| Female | 30 (47.6) | 8 (32.0) | 22 (57.9) |
| Age (in years), M (SD) | 40.44 (9.66) | 39.61 (10.18) | 40.97 (9.42) |
| Working in the healthcare sector (in years), M (SD) | 17.25 (11.15) | 14.84 (10.37) | 18.83 (11.49) |
| Working at an ICU (in years), M (SD) | 13.60 (10.85) | 9.71 (9.80) | 16.16 (10.86) |
| Average number of patients cared for by day, n (%) | |||
| < 4 | 33 (52.4) | 0 (0.0) | 33 (86.8) |
| 4–6 | 6 (9.5) | 3 (12.0) | 3 (7.9) |
| 7–9 | 21 (33.3) | 19 (76.0) | 2 (5.3) |
| 10–12 | 0 (0) | 0 (0.0) | 0 (0.0) |
| > 12 | 3 (4.8) | 3 (12.0) | 0 (0.0) |
| Average time required per patient, n (%) |
|||
| 0–60 min | 30 (47.6) | 23 (92.0) | 7 (18.4) |
| 61–120 min | 3 (4.8) | 1 (4.0) | 2 (5.3) |
| 121–180 min | 11 (17.5) | 1 (4.0) | 10 (26.3) |
| > 180 min | 19 (30.2) | 0 (0.0) | 19 (50.0) |
| Extent of concerns about own health before COVID-19 pandemic a , M (SD) | 3.12 (1.84) | 3.09 (1.62) | 3.14 (1.99) |
| Extent of concerns about own health since COVID-19 PANDEMIC a , M (SD) | 5.07 (2.56) | 5.13 (2.42) | 5.03 (2.68) |
| Extent of personal stress before COVID-19 pandemic a , M (SD) | 4.75 (2.11) | 5.13 (2.12) | 4.50 (2.09) |
| Extent of personal stress since COVID-19 pandemic a , M (SD) | 6.14 (2.41) | 6.17 (2.06) | 6.11 (2.64) |
| Job satisfaction score b , M (SD), (min–max) | 33.73 (3.85) (23–40) |
33.87 (3.99) (23–40) |
33.64 (3.81) (25–40) |
| General willingness to use technology—total score c , M (SD), (min–max) | 41.08 (4.73) (30–49) |
42.04 (4.22) (36–49) |
40.47 (4.99) (30–49) |
| Technology acceptance score d , M (SD), (min–max) | 16.23 (2.91) (9–20) |
16.87 (2.93) (10–20) |
15.83 (2.87) (9–20) |
| Technology control beliefs score e , M (SD), (min–max) | 7.29 (1.53) (4–10) |
7.13 (1.89) (4–10) |
7.39 (1.27) (4–10) |
| Technology competence beliefs score f , M (SD), (min–max) | 17.56 (2.23) (13–20) |
18.04 (1.99) (13–20) |
17.25 (2.35) (13–20) |
| Expectations for the use of telemedicine in an intensive care unit, total score g , M (SD), (min–max) | 27.64 (5.46) (8–40) |
26.52 (6.02) (8–39) |
28.36 (5.02) (11–40) |
| Expectations regarding a change in the number of patients to be cared for | |||
| Fewer patients expected, n (%) | 5 (7.9) | 2 (8.0) | 3 (7.9) |
| No change in number of patients expected, n (%) |
46 (73.0) | 13 (52.0) | 33 (86.8) |
| More patients expected, n (%) | 12 (19.0) | 10 (40.0) | 2 (5.3) |
n = number, M = mean, SD = standard deviation.
Extent measured using a scale of 1 to 10 with 1 = lowest and 10 = highest extent.
Total score of the standardised scale to assess job satisfaction (score could range from 8 = low to 40 = high satisfaction).
Total score of the standardised scale to assess general willingness to use technology (score could range from 10 = low to 50 = high technology willingness).
Score of the technology acceptance subscale (score could range from 4 = low to 20 = high technology acceptance).
Score of the technology control beliefs subscale (score could range from 2 = low to 10 = high technology control beliefs).
Score of the technology competence beliefs subscale (score could range from 4 = low to 20 = high technology competence beliefs).
Total score of items measuring expectations for the use of telemedicine in an ICU (score could range from 8 = low (more negative) to 40 = high (more positive) expectations).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.