
Abstract
Objective
To evaluate the feasibility of a mobile health-supported intervention in patients with cardiovascular diseases after completion of a cardiac rehabilitation programme.
Methods
The feasibility study was performed in two hospitals and one municipality in Region Zealand, Denmark. Eligible participants were ≥18 years old, participated in a supervised cardiac rehabilitation programme, had access to a mobile phone, and could walk 3 m independently. Participants received a 12-week intervention utilizing behaviour change techniques, consisting of action planning, text messages, and phone support. Feasibility was assessed using pre-defined progression criteria, which included recruitment (≥75%), retention (≥80%), accelerometer data completeness (≥80%), coordinator (phone support) time (≤30 min), the response rate on patient-reported outcomes (≥90%), adherence (≥75% respond to ≥75% of messages), and acceptability (≥75%). The secondary outcome of objective physical activity was assessed with accelerometers.
Results
Ten women and 30 men with cardiovascular diseases aged 63.5 (±9.8 SD) participated. The progression criteria for retention (90%), accelerometer data completeness (83%), coordinator time (9.9 min), adherence (83%), and acceptability (82%) were at acceptable levels, exceptions were progression criteria for recruitment (35%) being below acceptable levels for recruitment, and response rate on patient-reported outcomes (75%). High satisfaction (92.6%) with the intervention was found. All objectively measured physical activity levels remained unchanged from baseline to follow-up. No serious adverse events related to the intervention were reported.
Conclusion
Mobile health-supported maintenance of physical activity after cardiac rehabilitation completion was feasible, safe, and acceptable. Yet, changes to improve recruitment and response rate are needed before conducting a large-scale effect evaluation.
Introduction
Background and rationale
Cardiovascular diseases (CVDs) are one of the leading causes of death globally, and with an increasing prevalence, CVD poses a substantial burden on healthcare systems around the world1,2 and accounts for a significant number of disability-adjusted life years. 3 Lifelong physical activity plays a crucial role in the management of CVD, significantly improving quality of life and physical and mental health and reducing cardiovascular mortality and hospitalizations.4–7 To stay healthy and reduce the risk of a cardiovascular event, international guidelines recommend that adults engage in either 150–300 min of moderate-intensity physical activity, 75–150 min of vigorous-intensity physical activity per week, or a combination of the two. 4 Thus, to aid recovery and reduce mortality and secondary cardiovascular events for patients with CVD, exercise-based cardiac rehabilitation (CR) is a recommended evidence-based class-1 treatment strategy implemented in most European countries.4–9 One of the main goals of exercise-based CR is to support healthy physical activity behaviour in patients after the supervised programme is completed. 10 Despite the demonstrated benefits of CR on health outcomes, it is difficult for patients to maintain physical activity without the supervision provided during CR. Hence, patients risk experiencing a decline in physical activity levels over time, missing out on the long-term benefits, thereby increasing the risk of a secondary cardiovascular event.11–18 Various intervention types to support people with CVD in maintaining physical activity levels in everyday life have been tested, including mobile health (mHealth) interventions. Yet, the evidence remains diverse and of low quality, calling for further investigation in well-designed randomized controlled trial (RCT) studies. 19
mHealth refers to the use of mobile devices to enhance healthcare and practice. 20 Text message-based mHealth interventions are commonly used in health promotion 21 and have shown effects in promoting physical activity.22,23 Studies on text message-based interventions during CR indicate an increase in physical activity and have been found to be cost-effective.22,23 Still, two systematic reviews19,24 only report three RCTs exploring mHealth interventions for maintaining physical activity after CR.25–27 These provide divergent results, and the RCTs had small sample sizes and suffer from quality concerns. A recent systematic review by Heimer et al. 28 found a small overall effect on physical activity of eHealth interventions versus usual care after CR. The included studies present a high risk of bias regarding details of the content of interventions and blinding but otherwise present a low risk of bias. Six of the studies were text message-based, and only three of these studies reported using behaviour change theory, although it is interpreted as strengthening the intervention. 28 This highlights the need for high-quality research investigating the effect of mHealth interventions using behaviour change theory and techniques aimed at maintaining physical activity after CR. Maintenance can be defined as “a period of at least six months where the goal is to keep the benefits gained and prevent relapse”. 29
Methodological guidelines state that to successfully promote and maintain health behaviour change, interventions must be based on solid behaviour change theory. Hence, the primary objective of this study was to evaluate the feasibility of a mHealth-supported intervention using behaviour change theory and techniques in patients with CVD for three months after completion of a CR programme. Feasibility was assessed, both in terms of study design and intervention, through pre-selected progression criteria on recruitment, retention, data completeness, intervention delivery and adherence, and acceptability. Furthermore, we assessed changes in physical activity level through accelerometer data, physical function, quality of life, self-efficacy, depression and anxiety, and potential harms of the intervention, as these are intended outcomes in a future RCT.
Methods and analysis
Trial design
This single-armed multisite feasibility study was designed to evaluate research progression criteria. A protocol for this study describing its methodology was published prior to the completion of data collection and is available via open access. 30 Further, a qualitative investigation using participant interviews to provide information about the feasibility and acceptability of the intervention has been published elsewhere. 31 The reporting follows the CONSORT statement extension on randomized pilot and feasibility trials 32 (Supplemental file). The study was registered on ClinicalTrials.gov (NCT05011994), conducted according to the guidelines of the Declaration of Helsinki, and approved by the Research Ethics Committee of Region Zealand, Denmark (EMN-2021-00020).
Participants
Patients were recruited from hospital and municipality-based exercise-based CR programmes at Slagelse Hospital, Slagelse Municipality, and Holbæk Hospital from September 2021 to December 2022. Enrolled patients received the intervention for a duration of 3 months, starting from the completion of the CR programme. Following national clinical guidelines in Denmark, the standard phase II CR programme consists of a minimum of 8 weeks supervised exercise-based CR delivered either at the hospital or a local health centre (referred to as municipality).4,33 The supervised CR typically lasts an hour twice a week with an emphasis on aerobic exercise and resistance training. Patients’ education and risk factor management are offered during the CR period. In the present study, the supervised exercise-based CR was provided for outpatients at Slagelse or Holbæk Hospital and the Municipality of Slagelse. For patients at Holbæk Hospital six weeks of exercise-based CR was provided at the hospital and, if available, an additional 6 weeks of physical exercise in the municipality. For more information consult the study protocol. 30
Patients aged 18 years and older who took part in an exercise-based CR programme either in a hospital or municipality setting, had access to a personal mobile phone with a Danish telephone number, and were capable of walking 3 m independently, were included in the study. Exclusion criteria included insufficient Danish language ability to read and understand questionnaires and text messages, cognitive or mental inability to participate, and terminal patients with a life expectancy of fewer than 3 months.
Eligibility was assessed by the physiotherapists who conducted the CR programme at each site. These physiotherapists also provided eligible patients with written and brief information about the study. Oral information was then provided by either a researcher or a clinical staff member involved in the study. Informed consent was obtained prior to baseline assessments. All clinical assessment sessions in the study were conducted at the same location where the participants participated in the exercise-based CR programme. Based on the SPIRIT guideline, 34 a participant timeline was published in the protocol article. 30
Intervention
Immediately after completing the exercise-based CR programme, the participants received a mHealth-supported behavioural change intervention that consisted of individual action planning regarding physical activity, text messages to encourage and follow-up on planned physical activity, and the possibility of coordinator support via phone, e.g., when action plans were not met. The intervention did not replace any current treatment. Instead, it served as an addition to standard practice. Prior to the intervention, we sought input to enhance intervention design and setup from physiotherapists working in CR at hospitals and municipalities, patients, and representatives from the Danish Heart Foundation. 30
Theoretical framework
The Health Action Process Approach (HAPA) was chosen as the theoretical framework due to its frequent use in prior interventions promoting physical activity behaviour.35–39 HAPA consists of two phases, a motivational and a volitional, resulting in long-term behaviour change if both are successfully completed. This study focused on the volitional phase, in which intentions formed in the motivational phase are translated into action leading to actual behaviour.40–42
Behaviour change techniques
Recent advances in the design of behaviour change interventions have highlighted the value of categorizing intervention components (behaviour change techniques (BCTs)). 43 In this study, the intervention involved seven different BCTs as per the BCT taxonomy developed by Michie et al.. 43 The BCT components were: Action planning at the start of the intervention, social support from the coordinator to provide (a) guidance on physical activity and (b) establishment of contact with local activities. Further, four text messages addressing (a) prompt to do physical activity, (b) attention to action plans, (c) self-monitoring of behaviour, and (d) positive reinforcement. These BCT components were incorporated to promote and maintain physical activity behaviour. An overview of the BCTs is further described in the protocol article. 30
Action planning
A main BCT in the HAPA theoretical model is action planning. The purpose is to set specific plans for behaviours 44 in order to enhance the translation of formed intentions into action. 41 Assisted by a coordinator physiotherapist, participants created an individual action plan that specified types of physical activities, time and location of activities, and potential partners for each activity. The action plan was handwritten, and the participants brought it with them home, and kept it in a visible place e.g., hanging on the fridge. Further, the physiotherapist kept a copy. The action plan covered the 12-week intervention period and could be adjusted as needed by the participants themselves or with support from the coordinator physiotherapist through a phone conversation. The adjustments were for both parties registered by hand. A broad definition of physical activity was used. Thus, moderate-intensity activities included, e.g., gardening and playing with grandchildren.45–47
Text messages
Per the protocol article, 30 the 12-week intervention implemented auto-generated text messages consisting of two weekly messages. The first message prompted the participants to be physically active, drawing attention to the action plans, while the second facilitated self-monitoring of behaviour, asking if action plans for physical activity were achieved. A positive reinforcement automatic reply was produced for participants who responded ‘yes’, whereas those who responded ‘no’ received an automatic reply offering the participant a phone conversation with a coordinator physiotherapist for further guidance. The text messages addressed the participant by first name and used the researcher's name as the sender, making them personal despite being auto-generated.
Coordinator support
The study intervention included the possibility of being contacted by a coordinator physiotherapist throughout the 12-week intervention period. The coordinator's functions included calling participants who needed support, assisting the participants with adjustments to action plans, and offering general guidance for physical activity and contact with local activities. The coordinator physiotherapist contacted each participant only once in response to non-response to text messages but contacted them multiple times if requested by the participants.
Outcomes
Outcomes included pre-defined research progression criteria, objective measurements of physical activity and patient-reported outcomes of a range of health and quality of life parameters through questionnaires at baseline and follow-up. Data were obtained from baseline questionnaires and pre- and post-assessment sessions. A full list of outcomes is available in Supplemental Table 1 (supplementary file), corresponding to the supplementary table in the protocol article. 30 Further, a qualitative study exploring a sub-sample of eight participants’ lived experiences of participation in the intervention has been published elsewhere. 31
Primary outcomes
Pre-defined research progression criteria in order to evaluate the feasibility of the study design, the intervention and its readiness to be tested in a subsequent RCT design were set using a GREEN (proceed to RCT), AMBER (amend when proceeding to RCT), or RED (issue must be solved before proceeding to RCT) system 48 (Table 1). Recruitment of participants was evaluated by calculating the mean number of participants recruited per week per site and, subsequently, the total mean participant score per week. Retention was evaluated by calculating the percentage of participants who completed the follow-up assessment session out of the total number of participants who attended the baseline assessment. Accelerometer data completeness was evaluated by calculating the percentage of participants who provided valid accelerometer data from baseline and follow-up with the total number of participants who completed the intervention. The response rate to patient-reported outcomes was evaluated by calculating the percentage of participants who returned patient-reported outcomes of the total number of participants who attended both baseline and follow-up assessment sessions.
Progression criteria.
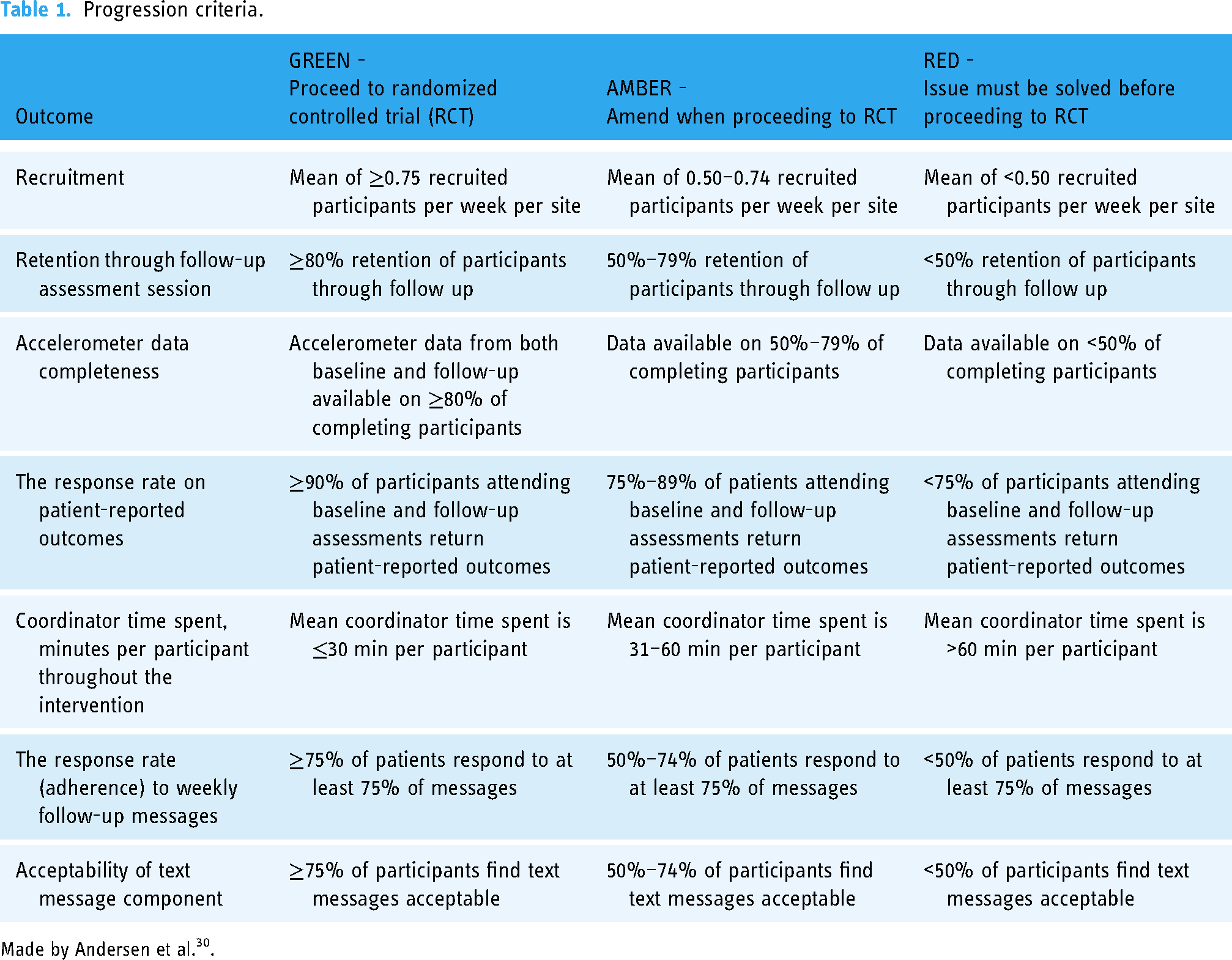
Made by Andersen et al.30.
Coordinator time spent was calculated as the mean of minutes spent per participant throughout the intervention. The response rate to weekly follow-up messages was evaluated by counting the number of responses divided by the 12 planned text messages. To evaluate the acceptability of the text message component, the participants were asked in the follow-up questionnaire whether they would participate in a project with weekly text messages again if given a chance to do it over, and the percentage of yes answers was calculated.
Secondary outcomes
Objective outcomes
To evaluate physical activity, all participants wore a thigh and a wrist accelerometer, Axivity AX3 (Axivity, Newcastle, UK), at baseline and follow-up. Per the protocol article, 30 the participants were required to wear both accelerometers at all times including during water activities and sleep for one consecutive week (thigh) and three consecutive weeks (wrist), respectively. The wrist accelerometer was worn for three weeks to obtain a reliable measurement of sedentary time and more long-term engagement with physical activity, requiring more than 5–7 days of measurement. Whereas, the thigh accelerometer provides a comprehensive description of activity types, which the wrist accelerometer is unable to do. Thus, this was worn for one week to minimize the inconvenience in regard to wearing the accelerometers.
At baseline, accelerometers were worn for the last week of CR, plus an additional 2 weeks for the wrist accelerometer. For follow-up measurements, a wrist accelerometer was worn for the last two weeks of the intervention plus an additional week. The thigh accelerometer was worn during the last week of the intervention for follow-up. The following activity intensity types were included: Light physical activity (LPA), moderate physical activity (MPA), vigorous physical activity (VPA), moderate to vigorous physical activity (MVPA), and sedentary behaviour (time spent sitting and lying) (SB). In order for accelerometer data to be considered valid, the participant had to have worn it for at least 22 of the 24 possible hours, and a measurement period was regarded as valid if the individual had three or more valid week-days and one valid weekend day.
Activity intensities were additionally used to assess whether participants adhered to the World Health Organization (WHO) recommendations for physical activity and SB (≥150 min. MVPA or ≥75 min. VPA weekly). 45
Moreover, clinically assessed outcomes regarding physical function were evaluated as a change in distance walked during the 6-min walking test (6MWT) from baseline to 12-week follow-up and as a change in number of sit-to-stand repetitions in the 30-s sit-to-stand test (30-STS) from baseline to 12-week follow-up. CR physiotherapists assessed the clinical tests.
Patient-reported outcomes
Patient-reported outcomes were collected via questionnaires in the electronic data capture system EasyTrial (easytrial.net, Aalborg, Denmark). The International Physical Activity Questionnaire (IPAQ) was used to assess self-reported physical activity, of respectively walking, moderate intensity, and vigorous intensity reported as MET-minutes/week and time spent sitting reported as min/day. 49 Further, physical function was assessed using the WHO Disability Assessment Schedule (WHODAS 2.0) 12-item version (0–100; higher scores indicating higher disability). 50 To assess health-related quality of life, HeartQoL was used with scores of 0–3, where a high score equals better HRQL. Anxiety and depression were assessed using the Hospital Anxiety and Depression Scale (HADS), where questions were scored from 0 to 3 and summarized to a total score for anxiety and depression, respectively (scores of 0–7 (normal), 8–10 (mild), 11–15 (moderate) 16–21 (severe)). 51 The Bayliss Burden of Illness Measure was used to gain information about the number of chronic conditions and to what extent the condition affected everyday life activities on a 5-point Likert scale (1 – not at all, to 5 – a lot). 52 See the protocol article for a full list of patient-reported outcomes 30 and Table 5.
Sample size
Our progression criteria for evaluating the feasibility specify a proportion of our sample that must meet these criteria (see Table 1). From our sample size estimation (published in the protocol article 30 ), a sample of 40 participants were considered to reach an acceptable level of certainty for evaluating the pre-selected progression criteria.
Statistical methods
The proportions outlined in Table 2, including 95% confidence intervals (CIs), were calculated to evaluate the progression criteria. For additional outcomes, we analyzed the change from baseline to follow-up. Continuous outcomes are reported as mean change with 95% CIs or as median and interquartile range calculated in STATA statistical software (StataCorp, version 18, College Station, Texas, USA). In addition, we calculated Cohen's d with thresholds for interpretation of the effect size of small (0.20–0.49), medium (0.50–0.79), and large (>0.80). 53
Baseline characteristics of participants.
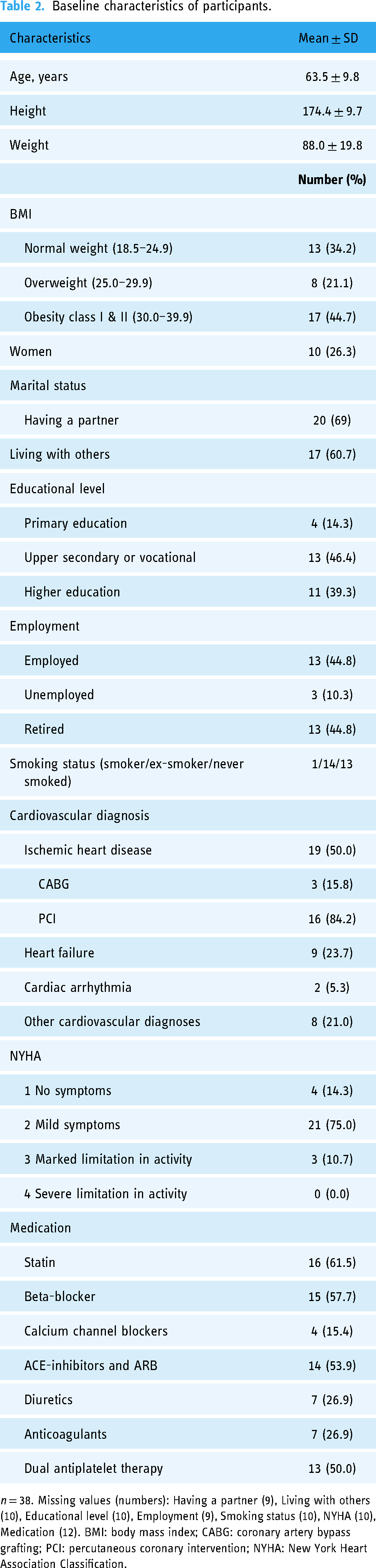
n = 38. Missing values (numbers): Having a partner (9), Living with others (10), Educational level (10), Employment (9), Smoking status (10), NYHA (10), Medication (12). BMI: body mass index; CABG: coronary artery bypass grafting; PCI: percutaneous coronary intervention; NYHA: New York Heart Association Classification.
Results
A total of 40 participants were included in the study, with follow-up data available from 36 participants for the final analyses (Figure 1) as four participants withdrew. Secondary outcomes on physical activity included 30 participants due to missing accelerometer data. Missing data from the follow-up measurement was caused by non-compliance (one participant), and loss of accelerometers (five participants) in the process of return by mail.

Flowchart of participant enrolment, follow-up, and analysis of primary outcomes.
The included participants were 10 females and 30 males. However, two participants dropped out during the time from inclusion to baseline assessment. The 38 participants with assessed baseline data were aged 63.5 ± 9.8 SD and diagnosed with CVD, predominantly ischemic heart disease (52.6%).
See Table 2 for more baseline characteristics.
Primary outcomes
The progression criteria (Table 3) for retention, accelerometer data completeness, coordinator time spent, adherence to text messages, and acceptability of text message components reached a level of acceptance (i.e., green, proceed to RCT). In contrast, progression criteria related to participant recruitment and response rate on patient-reported outcomes were red and amber, respectively.
Progression criteria evaluation.

* Both data from baseline and follow-up. Worn for at least 22 out of 24 h, for a period of at least three week-days and one weekend day. **Both data from baseline and follow-up. Data are presented as number (proportion), means (± standard deviation).
Secondary outcomes
All physical activity outcomes are displayed in Table 4. All objectively measured physical activity and physical function outcomes remained unchanged from baseline to follow-up (interpreted as Cohen's d < 0.20).
Secondary outcomes on physical activity.

*n = 30 (participants with valid accelerometer data from baseline to post-intervention. Worn for at least 22 out of 24 h, for a period of at least three week-days and one weekend day).
Data are presented as medians and IQR (25th and 75th quartile) or n and proportion (%). SB: sedentary behaviour (hours/day); LPA: light physical activity (min/day); MPA: moderate physical activity (min/day); VPA: vigorous physical activity (min/day); MVPA: moderate to vigorous physical activity (min/day); IPAQ: International Physical Activity Questionnaire; WHO; World Health Organization; CI: 95% confidence intervals.
Paired t-test presented as mean and 95% CI.
Cohen's d effect size of small (0.20–0.49), medium (0.50–0.79), and large (>0.80), presented with CI.
Adherence to recommendations on weekly physical activity according to WHO. Following recommendations for weekly physical activity: ≥ 150 min MVPA or ≥75 min VPA weekly or an equivalent combination.
All patient-reported secondary outcomes are displayed in Table 5. Most patient-reported outcomes remained unchanged from baseline to follow-up. However, small positive changes (interpreted as Cohen's d > 0.20) were presented in HeartQoL, HADS depression, and WHODAS.
Patient-reported secondary outcomes.

n = 27. Data are presented as medians and IQR (25th and 75th quartile).
CI 95%: 95% confidence intervals; IQR: interquartile range; EQ-5D-5L: The EuroQol 5 Dimension 5 Level Questionnaire (EQ-5D-5L Index: −0.624 to 1; worst to best); EQ-5D VAS: (0–100; a low score indicating a bad health state); HeartQoL: (Scores of 0–3, where a high score equals better HRQL); HADS: Hospital Anxiety and Depression Scale (Scores of 0–7 (Normal), 8–10 (Mild), 11–15 (Moderate) 16–21 (Severe)); WHODAS 2.0: The World Health Organization Disability Assessment Schedule, (0–100; higher scores indicating higher disability); Self-Efficacy 6-item Scale: Self-Efficacy for Managing Chronic Disease 6-Item Scale (1–10; a higher score indicates a higher level of self-efficacy.
Non-parametric data, presented as medians and IQR (25th and 75th quartile).
Cohen's d effect size of small (0.20–0.49), medium (0.50–0.79), and large (>0.80), presented with CI.
Patient-reported acceptability of the intervention, self-rated physical fitness, and physical activity modalities
The study showed a high degree of acceptability and adherence, as all but two participants were very satisfied (37%) or, for the most part, satisfied (55.6%) with the intervention, and all participants (100%) reported reading all the messages they received as part of the research project.
Of the 27 participants responding to the follow-up questionnaire, 7 (25.9%) rated their physical fitness as good, 9 (33.3%) as tolerable, and 11 (40.7%) as less good. Six participants (22.2%) reported coronavirus disease 2019 (COVID-19) having limited their possibilities of being physically active in the intervention period to a moderate extent (11.1%), to a great (11.1%) extent, and eight participants (29.6%) to a small extent. Moreover, 13 participants (48.2%) reported ‘not at all’. Further, 20 participants (74.1%) reported that they wished to be more physically active. The predominant types of physical activities that the participants performed during the 12-week intervention period were gardening, biking, walking, group-based exercise, badminton, and golf.
Safety during the intervention
Of the 27 participants responding to the follow-up questionnaire, three (11.1%) reported adverse events during the 12-week intervention period: tiredness, extreme dizziness, and an arm strain, not related to the intervention. Sixteen (59.3%) reported hospital visits during the intervention period, most of which were scheduled visits as part of their treatment plan. Two (12.5%) of these sixteen hospital visits resulted in participants being hospitalized; none were cardiac-related or serious adverse events related to the intervention. 54
Discussion
This study investigated the feasibility of a post-CR text message-based intervention for patients with CVD. Outcomes for the progression criteria for retention, accelerometer data completeness, coordinator time spent, adherence to text messages, and acceptability of the text message component were found feasible. Participant recruitment and response rate on patient-reported outcomes indicated that some amendments to the design are needed before investigating its effectiveness in a future RCT.
The feasibility of text messages as a simple mHealth intervention is supported by our results. We found high adherence to the intervention, with a patient-reported response rate of 100% who had read all the text messages. Furthermore, most participants experienced the intervention to be acceptable, as 92.6% of the participants were satisfied with the intervention and 82% would participate in a similar intervention, if provided again. The satisfaction with the intervention is supported by the findings from the qualitative study, showing that participants experience the intervention as someone holding their hand in a vulnerable situation and as reasonable support in reaching their weekly goals for physical activities. 31 This resembles previous studies,21,55,56 where participants found text messages acceptable and that they helped them engage in regular physical activity. 55 Further, the high retention rate in our study can be considered a result of the active engagement of participants through the individual action plans for physical activity and the 2-way text messaging highlighted in other studies.57,58 These findings add valuable contributions to the literature, as maintenance of physical activity during this critical period can be considered an important predictor of future health outcomes and behaviour. 59
Despite the satisfaction of the patients, our intervention setup reveals challenges that need to be addressed before proceeding to an RCT. In terms of recruitment, the progression criterion for recruitment was set to a mean of ≥0.75 recruited participants per week per site. However, this was not reached for any sites (mean of 0.50, 0.30, and 0.25). The study was conducted during the COVID-19 pandemic. The pandemic had a huge impact on everyday clinical practice, reducing the number of patients with CVD in the hospital departments, causing a reduced patient flow in the rehabilitation pathway, and further increasing other COVID-19-related work tasks in the municipalities. 60 Precisely how much this affected our study is unknown due to the complex changes in services during COVID-19. Nevertheless, the pandemic alone does not explain the low recruitment rate. The study was designed to be simple and easy to implement in everyday clinical practice, which is why the recruitment was conducted with minimal influence from the researchers. 60 However, a low recruitment rate is a commonly seen problem in research studies. 61 A Cochrane Methodology Review presents strategies designed to ease the recruitment of participants to research. 61 Following these strategies, possible amendments to a future recruitment strategy could be a better preparation of the physiotherapists, allowing them to build a daily work routine and the possibility of implementing the tasks well in the daily clinical work. Moreover, the sites could benefit from a screening and registration tool and allocation of time to secure a systematic and transparent screening process. Appointing one physiotherapist per site as the primary recruiter could ease the recruitment process and thus minimize unintentional gatekeeping arising due to a lack of time and routine in the study procedures. 61
For the response rate on patient-reported outcomes, the progression criterion was set to ≥90% of participants. This limit was not met, as only 75% of participants who attended both baseline and follow-up assessment sessions completed the questionnaires, and some of those only partly. According to the study protocol, 30 only email reminders were sent. Allocating resources to secure in-person follow-up on participants to obtain sufficient data seems central before proceeding to an RCT. 62 Further, the questionnaires took on average 30 min to complete, which might have led to fewer responses at follow-up. A revision of the questionnaire and prioritization and shortening of the questionnaire, may also positively impact the response rate. 63 Moreover, according to the MRC framework, feasibility of study design components can be improved by engaging potential users in the refinements. 64 Hence, user-involvement could be relevant to help focus the questionnaires and ensure higher participation.
The study was not powered to investigate the intervention effects, 30 and also lacked a control group. Only trends in changes in the outcome measures were explored. The results of the secondary outcomes on physical activity (LPA, MPA, MVPA, 6MWT, and 30-STS) indicate that the intervention facilitated the maintenance of the post-CR effects. However, this needs validation in a well-powered RCT using physical activity as a primary outcome. Other studies addressing the maintenance of physical activity after CR report similar results regarding unaffected levels of physical activity from baseline to follow-up.19,24,65,66 This suggests that maintaining the same level of physical activity over time in people with CVD, instead of improving, could be a more realistic and appropriate outcome in future studies.
Moreover, this study showed small positive changes for HeartQoL, HADS depression, and WHODAS. Combined with our qualitative investigation, 31 this mHealth intervention may potentially support people with CVD and improve the quality of life. This needs careful evaluation in a large, well-powered RCT, as increasing quality of life and well-being are the central outcomes in rehabilitation care. 67
Limitations and strengths
This feasibility study had some limitations. First of all, the study design is without a control group and power to investigate effectiveness, which precludes drawing any conclusions about the effectiveness of the intervention and specific elements.
Further, we limited our population to patients with CVD who had completed an exercise-based CR programme, and the included participants were primarily males. Thus, conclusions from this feasibility study cannot be generalized to all people with CVD. Further, the conclusions are based on all types of CVD, and particular trends within this large group cannot be drawn. We only included a 3-month follow-up period. According to the definition of maintenance: ‘a period of at least six months where the goal is to keep the gained benefits and prevent relapse’, 29 a longer period would be beneficial in a future RCT, in order to determine a long-term effect on maintenance. Furthermore, concluded by the systematic review by Heimer et al. 28 due to a limited number of studies exploring the long-term effects of eHealth after the completion of CR.
As per the study protocol, 30 CR physiotherapists conducting the phase II CR programme at each site had to screen for eligibility among the participants and then approach eligible participants. At the sites, all participants attending the phase II CR programme were informed about the project during the CR programme and handed an information leaflet. There is however inconsistency as to whether the CR physiotherapists systematically screened and approached the participants or if they volunteered to participate, and the total number of eligible patients was unfortunately not registered during this procedure. The number of participants completing CR during the trial period was n = 47 for Slagelse Hospital, n = 208 for Holbæk Hospital but is unknown for Slagelse Municipality, because of a new IT system implemented during the same period. A thorough standard procedure for eligibility registration and a standard registration form are to be developed prior to a future RCT.
Despite its limitations, the study was designed and conducted according to recommended guidelines.34,64 Further, the feasibility was evaluated based on pre-defined progression criteria and published together with the overall design of the study in a peer-reviewed protocol. 30 This has been advocated as an important strategy for improving transparency in the conduct and reporting of feasibility trials. 68 Moreover, in order to promote successful long-term health behaviour change, the study included the use of BCTs and behaviour change theory to support the participants regulate their behaviour during the transition to everyday life, which is also highlighted as a strength in a systematic review by Heimer et al.. 28
A focus in a future RCT study will be blinding, as this is often a challenge to achieve in trials reflected in the quality assessments, which is also shown in the systematic review by Heimer et al. 28 In this single-arm feasibility study the assessor of the primary physical activity outcome was blinded to patient characteristics, blinding of participants and physiotherapists was not obtained.
The study also included a qualitative exploration of the feasibility and acceptability of the intervention. 31 A further strength of the study is its generalizability to clinical practice, as the study was conducted in clinical practice in multiple settings, which in general reflects the organizational CR setup in Denmark. 69 Here, the standardized procedure for facilitating maintenance is a conversation upon CR completion, addressing patients’ opportunities to engage in an active and healthy lifestyle on their own. 69 Therefore, it would be the natural choice for a control intervention in a future RCT.
Conclusion
A mHealth-supported intervention, including BCTs such as action planning, prompting and positive reinforcement via text messages, and coordinator support via phone to maintain physical activity after completing an exercise-based CR programme, was feasible, safe, and acceptable for individuals with CVD. Hence, the intervention is a promising solution to support the transition from CR to everyday life with the small sample size and one-armed study design in mind. However, as the progression criteria for participant recruitment and response rate on patient-reported outcomes did not reach a level of acceptance, changes to improve these are needed before continuing to a full-scale RCT.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241239243 - Supplemental material for mHealth intervention including text messaging and behaviour change techniques to support maintenance of physical activity after cardiac rehabilitation: A single-arm feasibility study
Supplemental material, sj-docx-1-dhj-10.1177_20552076241239243 for mHealth intervention including text messaging and behaviour change techniques to support maintenance of physical activity after cardiac rehabilitation: A single-arm feasibility study by Trine G Hamborg, Rune M Andersen, Søren T Skou and Mikkel B Clausen, Madalina Jäger, Graziella Zangger, Charlotte Simonÿ, Anders Grøntved, Jan C Brønd, Anne M B Soja, Lars H Tang in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors thank the Department of Physiotherapy and Occupational Therapy at Holbæk Hospital, the rehabilitation unit in the Municipality of Slagelse, and the Department of Physiotherapy and Occupational Therapy at Slagelse Hospital and the participants for their participation in this study. Furthermore, we would like to thank Sofie Rath Mortensen for statistical advice, and Ida Marie Marcussen, Ida Ulriksen, and Mette Nyberg from The Research and Implementation Unit PROgrez, Department of Physiotherapy and Occupational Therapy, Næstved-Slagelse-Ringsted Hospitals for their contribution to the study.
Access to data
Data will be made available on reasonable request and within the terms of the study approvals. Data cannot be reused unless a collaboration agreement has been signed by both parties.
Contributorship
TGH drafted the article and finalized it with input from all authors. RMA, STS and LHT were involved in generating the idea for the study and in all sections of the protocol. MBC provided overall input and specific input on text messages and the Interventions section. MJ and GZ provided input on BCTs. AG and JCB provided overall input and specific input to measuring physical activity and feasibility evaluation. AMBS provided overall input, cardiology expertise, and specific input on the patient population. CS provided overall input, and rehabilitation expertise, and guided the qualitative study, thus, the patients’ lived experiences in the intervention. All authors were involved in the interpretation of results and reviewed and approved the manuscript prior to publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The project is approved by the Research Ethics Committee of Region Zealand, Denmark (EMN-2021-00020).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Region Zealand (Exercise First) and Næstved-Slagelse-Ringsted Hospitals (A841 & A1290) funded the project but were not involved in designing, conducting or reporting of the study. Dr. Tang is further funded by grants from The Danish Health Confederation through the Development and Research Fund (project no. 2703) and Næstved-Slagelse-Ringsted Hospitals research fund, Denmark (project no. A1277). Dr. Skou is currently funded by a programme grant from Region Zealand (Exercise First) and two grants from the European Union's Horizon 2020 research and innovation programme, one from the European Research Council grant agreement no. 801790 (MOBILIZE), and the other under grant agreement no. 945377 (ESCAPE).
Guarantor
TGH
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.