
Abstract
Background
Clinical management of ventilator-assisted individuals (VAIs) was challenged by social distancing rules during the COVID-19 pandemic. In May 2020, the Long-Term In-Home Ventilator Engagement (LIVE) Program was launched in Ontario, Canada to provide intensive digital care case management to VAIs. The purpose of this qualitative study was to explore the acceptability of the LIVE Program hosted via a digital platform during the COVID-19 pandemic from diverse perspectives.
Methods
We conducted a qualitative descriptive study (May 2020–April 2021) comprising semi-structured interviews with participants from eight home ventilation specialty centers in Ontario, Canada. We purposively recruited patients, family caregivers, and providers enrolled in LIVE. Content analysis and the theoretical concepts of acceptability, feasibility, and appropriateness were used to interpret findings.
Results
A total of 40 individuals (2 VAIs, 18 family caregivers, 20 healthcare providers) participated. Participants described LIVE as acceptable as it addressed a longstanding imperative to improve care access, ease of use, and training provided; feasible for triaging problems and sharing information; and appropriate for timeliness of provider responses, workflows, and perceived value. Negative perceptions of acceptability among healthcare providers concerned digital workload and fit with existing clinical workflows. Perceived benefits accorded to LIVE included enhanced physical and psychological safety in the home, patient–provider relations, and VAI engagement in their own care.
Conclusions
Study findings identify factors influencing the LIVE Program's acceptability by patients, family caregivers, and healthcare providers during pandemic conditions including enhanced access to care, ease of case management triage, and VAI safety. Findings may inform the implementation of digital health services to VAIs in non-pandemic circumstances.
Keywords
Introduction
The COVID-19 pandemic significantly disrupted access to health services in Canada, leading to major impacts on required care for ventilator-assisted individuals (VAIs) living in the community. VAIs represent a growing population (12.9/100,000 in Canada) requiring complex and highly specialized ongoing clinical management, most often provided via specialized home mechanical ventilation (HMV) centers or clinics. 1 Prevalence of HMV is associated a wide range of conditions including neuromuscular disorders, parenchymal lung disease, sleep-disordered breathing, and chest wall deformities. 2 In March 2020, health care organizations and health care providers (HCPs) in the province of Ontario, Canada (population > 15,000,000) were directed by the government to substantially reduce or stop non-urgent out-patient clinic visits to prevent transmission of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and conserve scarce hospital resources. 3 This directive raised concerns about interrupted access to specialist outpatient care 4 and highlighted the considerable potential of digital (i.e. virtual) care. 5
Digital or virtual care is defined as any synchronous or asynchronous interaction between patients and HCPs using any form of communication or information technology. 6 Digital care has long been proposed to bridge the gap between home and hospital as it can allow more frequent and closer monitoring of VAIs and reduce the incidence of disease exacerbations or complications leading to unplanned healthcare utilization. Digital care may also reduce the burden of routine in-person hospital appointments, which is a particularly salient benefit for VAIs who need to bring a ventilator and other technology to specialty clinic visits. 7
In Ontario in May 2020, to maintain continuity of management of VAIs while preventing exposure to SARS-CoV-2, we developed and implemented the Long-Term In-Home Ventilator Engagement (LIVE) Program hosted via the digital health management platform (aTouchAway, Aetonix, Canada). 7 We onboarded 251 VAIs (both children and adults) from 8 home ventilation centers. The LIVE Program was codesigned by patients, families, HCPs and clinical scientists, in collaboration with our e-health partner (Aetonix, Ottawa, Canada) and the Ontario Ventilator Equipment Pool (VEP). Following installation and orientation to the aTouchAway application on the preferred device of the patient/family (e.g. smartphone, tablet, or computer), access to the LIVE Program provided secure digital home visits, customizable care plans, an educational resource library, and clinical workflows to report changes in respiratory symptoms to the hospital-based HMV team. LIVE also enabled remote telemonitoring of ventilator use and two-way communication through instant messaging among the circle of care which included the patient, family caregivers, and HCPs (Figure 1). Additional details about the program have been reported elsewhere. 7

Screen captures showing the features of the LIVE program.
Despite extensive use of digital care among patients with chronic conditions during the COVID-19 pandemic, 8 perceptions in relation to its acceptability remain uncertain in vulnerable, medically complex populations, including those requiring HMV. 9 Acceptability, a core concept in digital health, is a multi-faceted construct that reflects the extent to which people delivering or receiving a healthcare intervention consider it to be appropriate.10,11 If an intervention is considered acceptable, patients are more likely to engage with and benefit from it. Conversely, if an intervention has low acceptability as perceived by HCPs, the intervention may not be delivered as intended. 11
Qualitative research is well suited to answer complex questions such as how patients, family members, and HCPs experience an intervention and make decisions about its use. 12 Therefore, this study sought to qualitatively evaluate whether the LIVE Program was acceptable, appropriate, and feasible form the perspectives of diverse HMV stakeholders (VAIs, family members, and HCPs) during the COVID-19 pandemic and identify recommendations to enhance or improve the intervention.
Methods
Study design and participants
We employed qualitative description methodology which is often used in healthcare studies for identifying participants’ direct experiences of an intervention and recommendations for how the intervention or its implementation might be improved. 13
We used purposive sampling to recruit VAI, family caregiver, and HCP participants (respiratory therapists, physicians, and nurse practitioners) enrolled in the LIVE Program during the study period (May 2020–April 2021). All adult and pediatric patients enrolled in the LIVE Program, living in a private home, and able to read and speak English were eligible for inclusion. There were no age restrictions for VAI participation. Inclusion criteria for family caregivers included being the most responsible person providing or coordinating the VAIs care without receiving financial compensation and able to read and speak English. HCPs involved in the LIVE Program to deliver care in one of the eight participating home mechanical ventilation centers were also eligible to participate. Potential participants were sent a recruitment message and link to a study flyer through the aTouchAway platform with instructions to contact the research team if interested. A research coordinator responded to patient, family caregiver, and HCP inquiries and organized an interview time following receipt of written informed consent.
Data collection
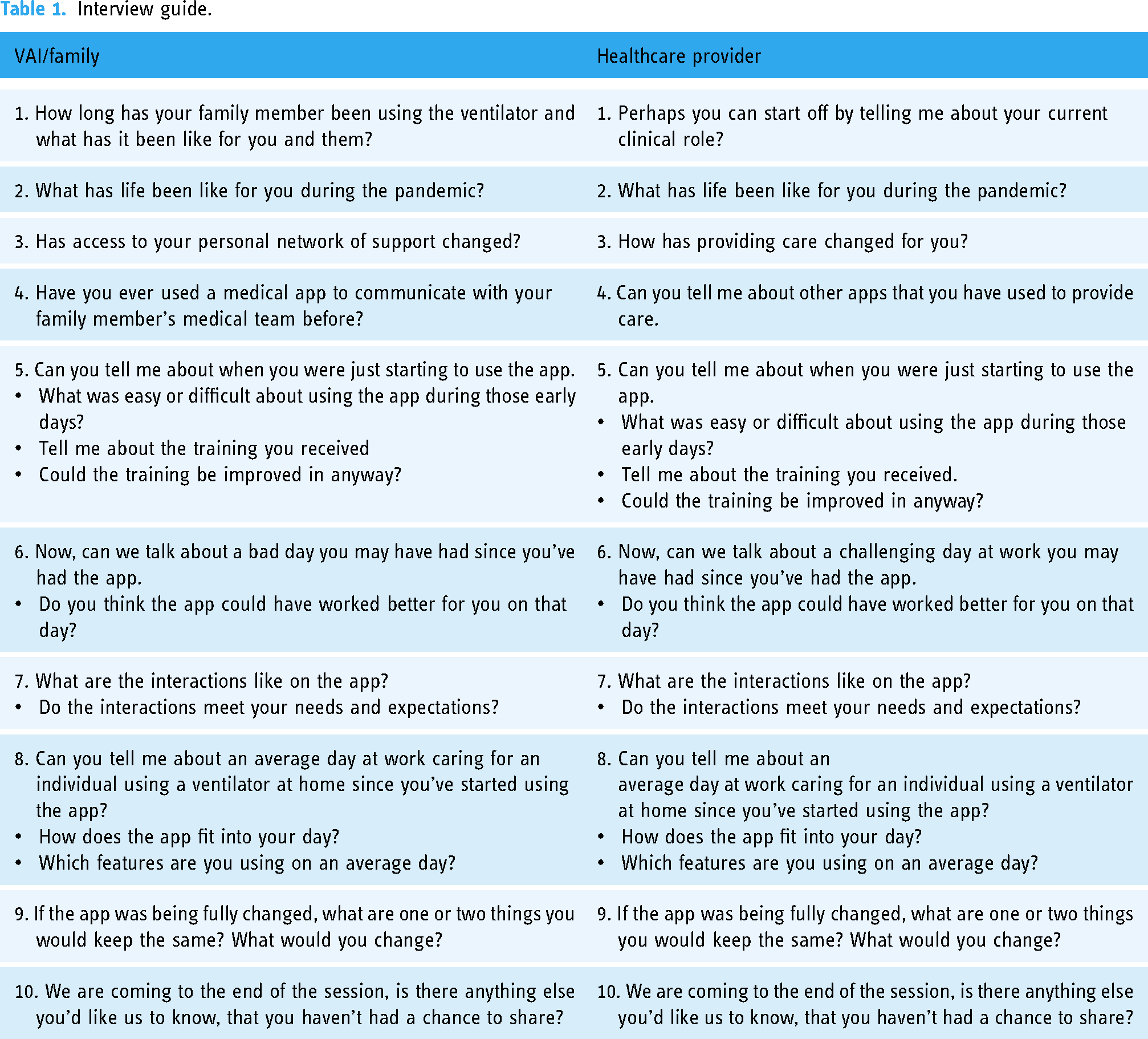
We conducted telephone and cloud-based video conferencing interviews (Zoom Video Communications Inc., San Jose, CA) using a semi-structured interview guide, developed using relevant evidence and an iterative consultation process with HMV experts. 14 The guide was pilot tested with the first three interviews with minor adjustments made to improve performance (Table 1). All interviews were conducted by two authors (MA, CD) who have health professional backgrounds and experience in qualitative interviewing. Interviews were digitally recorded, transcribed verbatim and identified with a unique code to maintain participant confidentiality. Notes were generated following each interview to document behaviors and initial impressions. 15 One interviewer was previously known to the participants through a respiratory care network. Data collection stopped at the point of conceptual saturation. 16
Interview guide.
Data analysis
We employed a directed content analysis starting with a conceptual framework. 17 For our framework, we chose the theoretical concepts of acceptability, appropriateness, and feasibility based on their pragmatic nature, conceptual clarity, and centrality to understanding digital intervention development and evaluation. 18 Following an immersive reading of the transcripts, three researchers (MA, CD, SK) designed a formative coding matrix based on the three main theoretical concepts. This included the following definitions: acceptability as the perception among stakeholders that the innovation is agreeable, palatable, or satisfactory; appropriateness as the perceived fit of the innovation to address a particular issue or problem; and feasibility as the extent to which the innovation can be successfully used in a given setting. The three researchers then independently identified descriptions of barriers and facilitators to engaging in the LIVE Program aligning with the three theoretical concepts and generated novel codes to organize. We sought consensus in coding through discussion at biweekly team meetings over a six-month period. Peer debriefing with the larger research team expanded perspectives regarding our analysis, including key differences within and across participant groups. NVivo 12 software was used to apply codes across the dataset. The Consolidated Criteria for Reporting Qualitative Studies (COREQ) checklist was used to guide reporting (Supplemental File 1). 19
Findings
We recruited 40 participants (2 VAIs, 12 pediatric family caregivers, 6 adult family caregivers and 20 HCPs). Demographic details are presented in Tables 2 and 3. Findings below are organized into conceptual categories of intervention acceptability (digital imperative, ease of use, and training), feasibility (triage and information sharing), and appropriateness (timing, workflow, and value) for VAI-family (VAI or VF) and HCP participants, respectively (Table 4). We then report participant recommendations to improve the LIVE Program.
Patient and/or family care provider characteristics (N = 20).

All values are n (%).
Health care provider characteristics (N = 20).

All values are n (%).
Conceptual categories and participant quotes.

HCP: healthcare professional; PF: patient/family.
VAI–family acceptability
Digital imperative: VAIs and family caregiver participants described improved access to respiratory health services as a longstanding pre-existing priority. The LIVE Program was perceived to suitably respond to this imperative through ready access to respiratory health professionals whilst reducing the burden of attending in-person appointments: You know, travel and parking and if the weather's bad, pushing a wheelchair through the snow. So, it's been amazing for us. It's just getting ready to leave the house is an ordeal. (VF16)
VAIs and family caregivers expressed concern about the risk of SARS-CoV-2 exposure during in-person hospital appointments and more severe presentations of COVID-19 disease should they be infected. Access to the LIVE Program reduced these infection concerns: And even before COVID, we didn’t like bringing our daughter into [healthcare] environments, where she can catch a cold or flu because they’re particularly hard on her. And so, we’ve always asked, you know, to have remote appointments, and it's one of the positive outcomes of COVID. (VF1)
Beyond transportation and infection concerns, participants described how the LIVE Program fostered “more of a connection with the team members than we’ve ever really felt” (VF7). The opportunity to stay connected to their care team during the pandemic was perceived as enhancing access to care and strengthening patient–provider relations.
Training: Those identifying the LIVE Program as acceptable referred to themselves as being “comfortable” with the use of electronic tools. They described adapting quickly to using the LIVE application following onboarding, which comprised one-on-one training delivered using telephone methods: Yeah, I believe it was [a respiratory therapist who], walked me through it. Was simple. She just gave me a brief overview of it. I was able to fill in all the blanks myself. (VF10)
Most individuals found a single training session to be sufficient for immediate use of the LIVE Program. The few participants who characterized training as “overwhelming” were most often parents of pediatric VAIs, worked full-time, and spoke English as a second language: Well, the onboarding, just the cognitive load in the onboarding, was just overwhelming. (VF1)
These individuals concurrently reported high levels of pandemic-related stress which impacted their memory and the ability to incorporate new behaviors.
Ease of use: Ease of use was a key facilitator of the LIVE Program's acceptability. Participants reported use was supported by an intuitive application interface and ability to complete required tasks quickly, such as biweekly symptom reports for review by the HMV team: I found [the app] quite user-friendly […]. I found it quite easy to navigate. I found it easy to put information in and easy to get information out. (VF15)
Some participants shared how the LIVE Program application was preferentially deployed on their smartphone, which “doesn’t leave my side.” In these cases, proximity to their personal device increased opportunities to engage the program. In contrast, those with physical dexterity issues reported difficulty employing the LIVE Program application on their smartphone or computer: Well, with my mobility issues, the scrolling of the mouse is difficult. It's a I guess it's a bit of an issue. (VAI10)
Other factors impacting ease of use included disruptions to family function during the pandemic: Too many things have happened in the family during the past year with COVID. I’ve had, you know, illnesses in the family, my mom passed, and then my husband got sick and things like that. So, I kind of put [the app] aside for the last little while. (VF2)
Family lives characterized by social disruptions such as illness and death were described as time compressed, which negatively influenced ease of platform use.
VAI–family feasibility
Triage: The ability to use the LIVE Program application was described across a range of settings and problems. For example, participants described using the platform when seeking help for determining the nature of an unexpected respiratory symptom and the need of further medical evaluation: His O2 sats dropped, his heart rate was up, major changes from baseline […] And it was nice to know that even though we’re at the cottage, we could easily access the help that we would need. (VF4) Instead of going in person to a hospital or to the emergency, […] they can pass information and I can figure it out from home. So that's why it's very good. (VF13)
To triage their concerns, participants most often initiated help via the instant messaging feature, which was sometimes converted to a video or telephone call by the HMV team. A few participants reported the practicality of sharing photographs of their body or equipment with a HCP to communicate an unanticipated issue: So I was able to take a picture and send it immediately in, the next day they were able to get me into the hospital, so that was very helpful. (VAI2)
The ability to successfully triage issues through the LIVE Program application was positively described by one participant as “jumping the queue” for assistance. A few family caregivers, however, reported feeling overwhelmed by the number of patient-to-provider communication options (e.g. telephone, paging, email, messaging via the application, and patient portals such as MyChart) in the hospital setting.
Information sharing: In circumstances where an emergency room or urgent care visit was necessary, several participants reported the ability to access and share information stored on the LIVE Program application with these HCPs. Such information included medication lists, ventilator device settings, HMV provider contact details, and care plans: When somebody asks us what the [ventilator] settings are - and it's like I sometimes I just totally forget. And so it's really nice to have it there. (VF1)
In addition to overcoming problems of recall, the above participant explained how the LIVE Program application enhanced their ability to communicate confidently with HCPs and participate in shared decision-making.
VAI–family appropriateness
Timing: A key attribute of the LIVE Program's appropriateness were the perceptions of HMV provider responsiveness to their help seeking efforts, particularly when using the messaging function: I had messaged one of the [respiratory therapists] at probably 10:30 at night. I wasn’t really expecting an answer, I just thought she’ll see it first thing in the morning, and boom, she answered me right away. I thought, oh, wow, that's really neat. (VF16) It’s almost immediate results instead of going back and forth with an email. (VF2)
Participants identified a timely response by HMV providers to fit their expectations for appropriate care. Provider responses within a few hours or the same day was a particularly important issue for patients who had higher levels of perceived need or urgency
Workflow: Most participants reporting feeling positively engaged by the requirement to complete biweekly symptom reporting through the LIVE Program application. These symptom reports could trigger a “red flag” warranting a follow-up call by an HMV provider. In such instances, participants reported feeling deeply supported: [It] was so nice to get a phone call and say, “Is everything okay?” (VF23)
In contrast, some participants gradually disengaged with symptom reporting as they were uncertain their data were being monitored by the HMV team: So I really stopped providing that input, because I really didn’t feel anybody was directly paying attention to it. You know, if I’m going to go through the work of producing data, I want to know there's somebody's going through the work of consuming it. (VF15)
Value: A key benefit reported by participants was an enhanced perception of physical and psychological safety in the home. The ability to readily access HCP support, particularly when first transitioning to HMV, reduced early uncertainties about management of the technology in the home: It's helped make me feel safe at home, knowing that I could get [help] right away. And if I’m ever uncomfortable, or if I ever have questions like the team is always there to support you … it can be very scary coming home; [it] is scary coming home with all this equipment. (VF2)
Similarly, the LIVE Program reduced feelings of social isolation from the health professional team: You didn’t feel like you’re all alone because that's sometimes how it feels. It's like, you’ve got all these specialists, but no, no connection other than your appointment every so many months, whereas this is, it helps you feel like [you’re] okay. (VAI18)
HCP perception of acceptability
Digital imperative: Like VAI and family caregiver participants, HCPs described how the LIVE Program was acceptable as it removed longstanding barriers to care delivery. For example, digital clinic appointments via the LIVE Program application removed the need for VAIs and their family caregivers to travel up to 100 km to the hospital, which was perceived as an undue burden: And so COVID has done some awful things but one [good] thing it has done is allowed for virtual appointments, which is I think long overdue. (HCP14)
The expansion of digital care also aligned with an evolution in the way HCPs worked with patient information in the hospital setting: A lot of what I do even before the pandemic was already based on patient report and downloads and virtual data. So, I saw this app as a further opportunity, but I was headed in that direction anyway. (HCP9)
One challenge to acceptability, however, was the cumulative burden of digital care in the hospital setting: So for example, I listed before, phone calls, and then I’ve pagers that result in phone calls, I have email, I have MyChart, and then the app. That's like five different ways that families can contact us. (HCP5)
Some HCP worried about their growing accountabilities for responding to patient concerns and documenting care delivered through multiple applications. This concern included the potential to inadvertently neglect communication, thereby inhibiting safe and efficient patient care.
Training: HCP participants described “hands-on” training as the best way of them learning how to use the LIVE Program application. This included ample time to practice with colleagues before engaging patients: I think it was hands-on and the best learning tool. (HCP19) I tend to learn things by just using them and trying them out. So, I sent lots of text messages and did lots of kind of practicing with colleagues, before we went to the patients with it. (HCP9)
The ability to request additional one-on-one training and the provision of a team “tip sheet” were other training strategies deemed helpful. HCPs responsible for orienting VAIs/families to the LIVE Program application noted how this accountability was “time-consuming” and sometimes required follow-up to ensure comprehension.
Ease of use: Most HCPs reported the LIVE Program application to be user friendly as it was easy to navigate on one or more devices including a desktop computer, tablet, or smartphone: How it's laid out is pretty straightforward. In my opinion, it's easy to use, easy to navigate, it works on several different devices. (HCP10)
Notwithstanding ease of use, several HCPs described challenges pivoting to digital modes of working during the pandemic. Challenges included “anxiety” about mastering new technology and making inadvertent errors. For example, some participants worried about accidentally “erasing” data such as biweekly symptom reports and forgetting passwords.
HCP perceptions of feasibility
Triage: Like VAIs and family caregivers, HCPs described an ability to successfully triage issues reported directly by a VAI through the LIVE Program application. Some participants credited provision of downloaded ventilator data into the LIVE Program application as helpful for sorting problems that could lead to a “disaster” (i.e. adverse event): We actually found this was probably a “good save”, [as we] learned that the parents were making setting changes [on the ventilator] that were not prescribed. (HCP2)
This HCP explained how correction of ventilator settings prevented patient harm and unplanned healthcare utilization.
A few participants noted challenges triaging patient concerns or “red flags” due to variable staffing or acuity in the hospital setting. Certain “red flag” alerts issued through the LIVE Program application were perceived as false alarms for patients with advanced disease states such as those with amyotrophic lateral sclerosis (ALS). In such cases, HCPs described additional time and work verifying such alerts through telephone outreach to the patient.
Information sharing: In reference to the above process of triage, most HCPs described an efficiency in communicating patient issues and treatment changes among the local HMV team through the LIVE Program application messaging function: Troubleshooting technological issues [is] one of the things that we put on a group chat. […]. So we’re always all in the know. (HCP4) [A] huge benefit, as I mentioned before, is like having everything all in kind of one place and consolidated into one interface. (HCP13)
Benefits of information sharing via the application included a reduction in “back and forth” email messaging regarding a problem and its solution. In addition to being a central repository of information about device settings, prescriptions, and care plans accessible to both HCPs, the VAI and their family caregivers, the LIVE Program application served as a convenient record of changes to the treatment plan. Therefore, the LIVE Program application conferred efficiencies and safety benefits.
HCP perceptions of appropriateness
Timing: Most HCPs reported that encounters via the LIVE Program application with VAIs were more efficient in the sense that it saved time and increased their perception of productivity. For example, messaging encounters initiated by VAIs or family caregivers often took less time to address than in-person visits. These encounters were often less complex as they were more in the moment, making it possible to provide consultation and rapidly resolve most VAI concerns: I think that's the one very big benefit of aTouchAway is that I do feel as though issues are addressed faster. So more in real time. (HCP13)
The ability to quickly resolve VAI concerns was described as a source of professional satisfaction. HCPs explained how the notification feature on the LIVE Program application enabled a prompt visual and auditory notification of a new message and the ability to respond without significant delay. Where appropriate, VAI or family caregiver messaging encounters could be converted to a video encounter without the need to generate and share a video-conferencing link.
Workflow: Important differences were detected across sites and teams with respect to LIVE Program workflow integration. Larger HMV teams of three or more HCPs reported the ability to rotate accountability for responding to messages and “red flags” during the week: So how we have divvied it up amongst our team members is we have a schedule of who responds to the messages every single day. (HCP17) It's truly been a well-integrated part of our day-to-day care […] So every day of the week, one of us is accountable for addressing flags on the app. (HCP4)
Shared accountability enhanced integration of the LIVE Program into outpatient care and reduced the perceptions of interruption for other in-patient care responsibilities that comprised their normal workload. Smaller HMV teams of less than three HCPs, in contrast, more often reported assignment of the LIVE Program to one clinician and greater difficulty integrating it into workflow routines: Whereas if it's more like an inpatient sort of related issue, or concern, then [the app] does kind of go to the background, because I’m dealing with a lot of the inpatient stuff at the hospital first. (HCP14)
Lack of shared accountability for the LIVE Program resulted in lower reported integration success into local workflows including within in-patient and outpatient clinic care.
Value: Most HCPs cited the value of the LIVE Program as its ability to engage VAIs in their own care. Digital reporting of biweekly symptoms, for instance, was perceived to help VAIs self-monitor, enhance learning, encourage behavior change, and foster closer relations with the HMV team. Some participants reported the LIVE Program being optimally suited to VAIs and family caregivers newly transitioning to HMV: I think for new users of ventilation it's different. This would enhance, you know, their learning. And, you know, it's a part of the therapy; it will supplement their education, it provides them with resources. You know, I think it's a totally different approach. And I think we would get better buy in. (HCP2)
The above HCP described the LIVE Program as a positive innovation and low-resource solution to help new VAIs s take ownership of their healthcare journey. In contrast, some HCPs noted lower engagement with longstanding and medically stable VAIs: For patients who were already managed and ventilated? You know, why fix [something when] there's no problem. What is there to fix? So that buy in was really challenging. (HCP3)
HCPs described greater difficulty initially engaging these VAIs in the LIVE Program. They expressed uncertainty about methods of encouraging its use for this stable group during and beyond the pandemic.
Recommendations
The major recommendation to improve the performance of the LIVE Program made by HCPs was its integration with the hospital's electronic medical record: All of our documentation in the outpatient setting is in an electronic health record, and we do have a process for that. So one of the challenges is, as you mentioned, all that kind of communication in the app has to be shifted to our formal record, if we want it to be formally documented and available to other kinds of clinics and providers. (HCP9)
Integrated record keeping was recommended to reduce workload due to the need for duplication of documentation across systems, to ensure accessibility of documentation, and to minimize information loss. HCPs described how the demands of clinical documentation were associated with an increased cognitive load and often competed with their focus on the VAI.
While HCPs found the LIVE Program application interface easy to navigate, some VAIs and family caregivers recommended the interface be further simplified: Last word of advice, simplify it a little bit. And gear it. It's geared towards the people that are more technology oriented. (VF11)
Simplification was deemed important for those with low digital literacy, lack of motivation to use technology, and physical limitations. To address these issues, the incorporation of interactive voice response technology was recommended. This would allow VAIs to access and send messages, in addition to other content, through a simple user interface that requires only their voice. This function was deemed important for greater inclusivity and equity; making the LIVE Program more accessible to VAIs with physical disability but also limited literacy or those unable to read or write.
Discussion
In this qualitative descriptive study comprising interviews with 40 participants from eight home ventilation specialty centers in Ontario, we found the introduction during the COVID-19 pandemic of an innovative digital intervention (the LIVE Program) specifically designed to address the needs of VAIs and family caregivers to be acceptable, feasible and appropriate to end-users. Key factors positively influencing acceptability were the digital imperative, ease of use, and access to training; influencing feasibility were problem triage and information sharing, and influencing appropriateness were timing, workflow, and perceived value.
A key facilitator of the LIVE Program's acceptability in our study was its ability to overcome existing care access barriers related to distance, time, and costs associated with travel to specialty outpatient clinics. Moreover, LIVE mitigated both systemic and personal difficulties associated with accessing services during the pandemic, that is, risk of nosocomial infection.20,21 The digital imperative identified in our findings affirms that VAIs and family caregivers perceive virtual care as a needed and desired improvement to service delivery. 7 The requirement for travel to specialty HMV clinics can impose significant individual and family burden that may detrimentally impact upon health-related quality of life. 22 Similar to research engaging other Canadian patient populations, most report satisfaction with virtual care; up to one-half identify virtual care as their preferred mode of contact following the pandemic. 23 We found the LIVE Program's acceptability among VAIs and HCPs to be further influenced by ease of use of the LIVE Program application interface and hands-on training opportunities. LIVE Program acceptability and its potential in complementing conventional in-person services supports recent calls for the expansion of digital care beyond the pandemic. 24
We identified that the LIVE Program introduced further elements of feasibility of care delivery in respect to triage of VAI- and family caregiver-identified concerns regarding changes in respiratory status or challenges related to ventilator or other device use. Similar to other research in digital care, 25 we found that most concerns were conveyed using asynchronous, secure text messaging with HCPs able to resolve concerns in a short amount of time. In addition, we identified the ability of HCPs to prioritize contact with VAIs following review of ventilator download data and prescription non-compliance. HMV requires overcoming multiple discomforts including those related to the delivery interface and positive airway pressures. 22 Monitoring of HMV prescription adherence and symptom changes are important to potentially avoid complications and disease exacerbations requiring emergency healthcare utilization. HCPs noted how the need for an in-person hospital assessment could be preliminarily determined using the LIVE Program application. However, this could add to a perceived increase in workload to complete further assessments remotely. Another perceived benefit was that changes made to the treatment plan were easily shared among the local HMV team, thereby offering an efficient method of clinical communication.
Appropriateness of the LIVE Program for virtual management of VAIs was supported by perceptions of a timely response by HCPs to VAI or family caregiver messages and the completion of biweekly symptom reports that could alert the HMV to changes that needed further assessment. An important condition of symptom reporting appropriateness was VAI or family caregiver perception of HCP review of these data and understanding of its contribution to their health management. These findings align with expert review of digital patient communication being accompanied by an expectation for the same day if not almost immediate review and/or response from HCPs. 26 VAI or family caregiver’s lack of understanding of the process of HCP review of data or the clinical relevance of data collected and submitted may negatively impact their motivation to remain engaged in digital care. 27 A potentially unique finding in our data pertains to lower ability among smaller HMV teams (i.e. three or fewer providers) to integrate the LIVE Program into their routine workflows and share accountability for the related workload. Challenges associated with balancing digital health workload with other workload by HCPs may preclude known patient-oriented benefits including accessibility, compliance, and timely intervention. 28
Value attributed to the LIVE Program included a unique opportunity for VAI engagement in their own care, enhanced VAI/family caregiver–provider relationships, and individual/team satisfaction with services delivered. The potential for VAI/family caregiver-initiated outreach and reporting may have fostered greater self-reflection and accountability for health outcomes. The LIVE Program may, therefore, offer a unique mechanism to increase VAI engagement and empowerment in care. Our VAI and family caregiver participants reported feelings of physical and psychological safety associated with participating in the LIVE Program which may have been due to perceived greater surveillance by HCPs. Feelings of safety may be especially important for those with mobility issues or living in a rural location. HCP reports of adverse event detection or prevention may explain individual and team satisfaction with the LIVE Program.
We identified differences concerning LIVE Program engagement by VAIs recently transitioning to HMV in comparison to those well-established. Practice guidelines recommend comprehensive initial and ongoing VAI/family caregiver training in ventilator use and early follow-up of ventilator effectiveness by HMV specialty teams. 29 Issues commonly addressed in clinic visits for those newly transitioning to HMV include collaborative goal setting, communication of a shared care plan, emergency preparation, and coordination of in-home visits by respiratory and allied health therapists. In our earlier work, we identified that VAIs and family caregivers newly transitioning to HMV recommended greater access to specialized respiratory support in the community. 2 These cumulative findings support consideration of the integration of digital care into HMV transition services. Incorporating the LIVE Program into existing and ongoing clinical services is an important adjunct to extend education, address unanticipated problems, titrate ventilator settings, and support compliance.
Our findings may offer guidance for the implementation of digital health interventions beyond the COVID-19 pandemic. Participant insights suggest the need for careful planning of technical and human resources when implementing a digital health management strategy such as the LIVE Program. Consideration should be given to the integration of digital health interventions into the electronic medical record to reduce the workload resulting from duplication of clinical documentation. Future research should focus on the quality and effectiveness of care delivered through digital platforms among new and established HMV users outside of pandemic conditions. Close attention should be paid to patient subgroups and HMV team size to appraise the impact on HCP workflows and patient outcomes.
Strengths and limitations
Strengths of this study include diverse participant perspectives, recruitment from multiple sites, use of theoretical concepts important to digital care, and an interprofessional team of analysts. The present study also has several limitations. Interviews with VAIs were fewer than anticipated potentially due to cognitive, physical, and verbal incapacities. However, we recruited pediatric and adult family caregivers intimately engaged with HMV care and specialist providers. Participants were recruited from one province (Ontario), suggesting the findings may not be transferrable to other jurisdictions, particularly those that do not have universal coverage of physician and hospital services. Digital care acceptability may change over time due to evolving social norms, socioeconomic status, ethnicity, or geographic region. The burden of COVID-19 in Canada has been modest compared to other countries. Accordingly, the acceptability of a digital health management intervention such as the LIVE Program may be experienced and described differently in other pandemic settings. Finally, it is recognized that one interviewer was previously known to a few participants, however, recruitment was automated through the platform, thereby mitigating selection and social desirability bias.
Conclusion
In this qualitative study, we found the use of the LIVE Program digital health management intervention developed by our group for VAIs and their family caregiver and implemented during the COVID-19 pandemic to be acceptable, feasible, and appropriate. Factors positively influencing acceptability were digital imperative, ease of use, and training; influencing feasibility were triage and information sharing; and influencing appropriateness were timing, workflow, and perceived value. Future research should focus on the assessment of the effectiveness of digital care interventions for improving outcomes for this patient population and ways to tailor the intervention to suit the needs of smaller HCP teams and across the continuum of care, that is, new as well as established HMV users.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241228417 - Supplemental material for Acceptability of the Long-Term In-Home Ventilator Engagement virtual intervention for home mechanical ventilation patients during the COVID-19 pandemic: A qualitative evaluation
Supplemental material, sj-docx-1-dhj-10.1177_20552076241228417 for Acceptability of the Long-Term In-Home Ventilator Engagement virtual intervention for home mechanical ventilation patients during the COVID-19 pandemic: A qualitative evaluation by Craig M. Dale, Munazzah Ambreen, Sohee Kang, Francine Buchanan, Regina Pizzuti, Andrea S. Gershon, Louise Rose and Reshma Amin in DIGITAL HEALTH
Footnotes
Acknowledgements
We are grateful to the participation of VAIs, family caregivers, and dedicated clinical teams at LIVE centres. This work was conducted on behalf of the Long-Term In-Home Ventilation Engagement (LIVE) Program group: Reshma Amin, The Hospital for Sick Children; Ms. Regina Pizzuti, Ontario Ventilator Equipment Pool (VEP); Andrea Gershon, Sunnybrook Health Sciences Centre; Francine Buchanan, University of Toronto; Michel Paquet, Aetonix; Jackie Chiang, SickKids; Roger Goldstein, West Park Healthcare Centre; Sherri Katz, Children's Hospital of Eastern Ontario; David Leasa, London Health Sciences Centre; Audrey Lim, McMaster Children's Hospital; Doug McKim, The Ottawa Hospital; Anu Tandon, Sunnybrook Health Sciences Centre; Aaron St Laurent, London Health Sciences Centre; Louise Rose, Kings College London. We wish to acknowledge the contributions of the LIVE Allied Health team: Paula Abelha, Adele Baker, Ashley Benett, Sacha Bhatia, Cindy Brennan, Julia Bokhaut, Ronald Butler, Paul Cameron, Jackie Chiang, Nisha Cithiravel, Jana Collins, Leah Costa, Refika Ersu, Erin Fleischer, Sandy Foley, Janet Hyatt, Ashley Inman, Mary Irven, Joanna Janevski, Raj Kohli, Wilma Koopman, Sarah Kuyntjes, Audrey Lim, Paty Sala Lopez, Denise Martins, Cathy Mawdsley, Sandra McKay, Ramsay McNay, Kevan Mehta, Myla Moretti, Riley Moss, Jodee Naylor, Michelle Overholt, William Reisman, Josee Roy, Madan Roy, Christen Shoesmith, Joanne Smith, Lisa Spooner, Aaron St-Laurent, Faiza Syed, Anu Tandon, Mark Thompson, Tuyen Tran, Melissa Trinh, Robert Varadi, Shannon Venace, and Allison Zweerink.
Contributorship
Conception and design of the study by RA, LR, and CMD; data acquisition by MA and CMD; analysis and interpretation of data by CMD, MA, and SK; drafting the article or revising it critically for important intellectual content by all authors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Research Ethics Boards (REB) from The Hospital for Sick Children approved this study (1000073189).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Ontario Ventilator Equipment Pool, operated by the Kingston Health Sciences Centre, funded by the Ontario Ministry of Health Assistive Devices Program.
Guarantor
CMD.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.