
Abstract
Introduction
Digital health has the potential to support health care in rural areas by overcoming the problems of distance and poor infrastructure, however, rural areas have extremely low use of digital health because of the lack of interaction with technology. There is no existing tool to measure digital health literacy in rural China. This study aims to test and validate the digital health readiness questionnaire for assessing digital readiness among patients in rural China.
Methods
Due to the different Internet environments in China compared to Belgium, a cultural adaptation is needed to optimize the use of Digital Health Readiness Questionnaire in China. Then, a prospective single-center survey study was conducted in rural China among patients with hypertension. Confirmatory factor analysis was computed to test the measurement models.
Results
A total of 330 full questionnaires were selected and included in the analysis. The model-fit measures were used to assess the model's overall goodness of fit (Chi-square/degrees of freedom = 5.060, comparative fit index = 0.889, Tucker–Lewis index (TLI) = 0.869, root mean square error of approximation (RMSEA) = 0.111, standardized root mean square residual (SRMR) = 0.0880). TLI is a little bit lower than the borderline (more than 0.9) and RMSEA is higher than it (less than 0.08 means good model fit). We deleted two items 2 and 4 and the result shows a better goodness of fit (Chi-square/degrees of freedom = 4.897, comparative fit index = 0.914, TLI = 0.895, RMSEA = 0.109, SRMR = 0.0765)
Conclusion
To increase applicability and generalizability in rural areas, it should be considered to use the calculation of only the parts Digital skills, Digital literacy and Digital health literacy which are equally applicable in a Belgian population as in a rural Chinese population.
Keywords
Introduction
The lack of adequate medical resources in China's rural areas continues to be a key challenge, exacerbating the existing health disparities in settings with limited resources. 1 The spread of the internet and information technology, however, has the potential to support health care in rural areas by overcoming the problems of distance and poor infrastructure. 2 For example, He et al. proposed to build an internet-based hospital to address the maldistribution of healthcare resources in rural China. 3 However, rural areas have extremely low use of digital health, with only 0.67% (14/2101) participants using telemedicine services. 4 The greatest obstacle is a lack of knowledge and understanding, followed by a lack of trust, low self-efficacy and insufficient physical and social support. 4 The effectiveness of digital health interventions can be affected by inefficient interactions with technology. There is a need for digital health literacy training sessions to avoid the “digital divide.” Before expanding digital health services in rural China, it is imperative to assess and improve digital health literacy to prevent further inequalities in health resources.
Digital health literacy is defined as “the extension of health literacy, but in the context of technology.” 5 It is the use of digital technologies such as smartphones, laptops, and/or wearable devices to search, acquire, comprehend, appraise, communicate and apply health information in all contexts of health care. Studies on digital health literacy up until now have used the 8-item eHealth Literacy Scale (eHEALS), which has been translated and validated in Chinese. 6 However, with the increasingly updated technology, eHEALS lack the measure of digital health's dynamic and social nature. The Digital Health Readiness Questionnaire (DHRQ) is a state-of-the-art and easy-to-use tool that builds on other questionnaires developed by two physicians with extensive experience in digital health research based on a definition of readiness for digital health interventions and is designed to be used to capture digital usage, digital skills, digital literacy, digital health literacy, and digital learnability. Compared to eHEALS, (a) in the digital usage domain, DHRQ not only focused on the Internet but also included other digital tools such as computers, smartphones, and also wearable devices; (b) in the digital skills domain, DHRQ added the social nature of digital health, for example, “I use social media,” “I can take a photo and send it to another person”; (c) DHRQ added a new domain called digital learnability, which could identify those with low digital readiness but high learning ability and engage them in digital care programs by providing digital health educational program. DHRQ can be used to assess readiness for digital health interventions in routine clinical practice and has the potential to provide insights into patients treated in care pathways, to tailor digital care pathways for different patient populations, and to provide appropriate educational programs for those with low digital readiness but high learning ability to engage them in digital pathways. 7 This study aims to test and validate the DHRQ for assessing digital readiness among patients in rural China.
Methods
In this study, we hypothesized that the model fit evaluation indicators obtained from the confirmatory factor analysis (CFA) using AMOS were acceptable or desirable, the constructed model was well-fitted, and the sinicized DHRQ could be used to assess the digital health readiness of hypertensive patients in rural areas of China.
Instrument
The DHRQ was developed by Dr Martijn Scherrenberg and Dr Maarten Falter. This questionnaire was designed to assess patients’ digital health literacy and their willingness to learn new digital health tools in the future. The questionnaire includes five subscales (i.e. digital usage, digital skills, digital literacy, digital health literacy and digital learnability) measured by 20 items that are answered on a 5-point Likert scale ranging from 1 to 5. The sum of the scores of the first four subscales, that is, digital usage, digital skills, digital literacy and digital health literacy, was used to calculate the general DHRQ score. The minimum general DHRQ score was 15, and the maximum score was 75. The fifth subscale, that is, the scores of digital learnability, was used to calculate the digital learnability score; the minimum score of the digital learnability score was 5, and the maximum score was 25. Digital learnability was categorized into four groups according to the score scores: Group A (21–25), Group B (16–20), Group C (11–15) and Group D (5–10), and the higher the scores, the higher the willingness to learn the digital health tools. Scores on the DHRQ can be expressed as the general DHRQ score plus a grouping letter for digital learnability, for example, “40 + B.”
Translation, back translation and culture validation
First, the DHRQ was translated from English into Chinese by the first author (LX), who is a bilingual (Chinese/English) experienced researcher. Second, two other researchers (TY and XL) translated the Chinese version draft back into English separately. Then, a bilingual expert panel (LX, TY and XL) convened to discuss the differences between the translated version and the original version and review and correct the draft version of the DHRQ. Third, we sent the Chinese version 2 to three Chinese experts in the field of digital health to amend the questionnaire regarding culture adaptation. Then, feedback was discussed with the questionnaire's original writers (MS, MF and PD) so as not to significantly alter its original intent.
Due to the different Internet environments in China compared to Belgium, a cultural adaptation is needed to optimize the use of DHRQ in China.
Item 5 is “I am able to write and send an email independently” in the original questionnaire. However, the use of email is not common in China and many people are used to using timely communication software like WeChat. The authors therefore chose to email into “email and/or message” in the Chinese version. As the social media platforms used in China are also different compared to those in Western Europe where the questionnaire was developed, item 6 was changed from “I use social media such as Facebook, Instagram, other” into “I use social media such as WeChat, TikTok, Sina Weibo, Xiaohongshu, Kwai” which are the most popular social media platforms in China. The Chinese version of DHRQ was shown is Supplemental File 1.
Data collection
This prospective, single-center research study was conducted in Daxing Town, Liaoyuan City, Jilin Province, China, from August 15 to 19, 2022. It is a rural area in northern China. All participants with a hypertension diagnosis were eligible to participate. Hypertension is one of the major public health problems in China, especially in rural areas. However, recruiting patients from township hospitals (research centers) did not reach many patients. Patients do not take hypertension seriously and are not aware of self-management, nor do they have good compliance with medication, and villagers do not go to township hospitals specifically for hypertension. We, therefore, chose to conduct a field survey in 12 villages (total 8191 residents) to provide more comprehensive coverage. We used a convenience sampling method. A pen and paper method was used in the survey. For validated factor analyses, sample sizes greater than 500 are perfect, around 300 are good, and around 200 are acceptable. Considering the 20% invalid questionnaires, 586 translated and revised Chinese versions of the DHRQ were distributed, considering the actual hypertensive patients in the 12 villages of Daxing Town. A total of 586 translated and revised Chinese versions of the DHRQ were distributed. Only fully completed questionnaires were included in the analysis. In addition to filling out the questionnaire, participants were also asked to provide their age, gender, occupation, the level of education, monthly income, marital status and residence status.
Statistical analyses
Data analysis was performed using SPSS Statistics and SPSS Amos (version 26). Categorical data were described by number and percentage. Continuous data were described by mean ± standard deviation and median. CFA was computed using AMOS to test the measurement models. The model's fit was evaluated using the standardized root mean square residual (SRMR), the root mean square error of approximation (RMSEA), the comparative fit index (CFI), and the Tucker–Lewis fit index (TLI). The model's fit is ideal when the SRMR is less than 0.08, and the model's fit is acceptable when the SRMR is less than 0.1. The model's fit is ideal when the RMSEA is less than 0.05. The model's fit is acceptable when the RMSEA is less than 0.08. And when the CFI and TLI are more significant than 0.9, the model's fit is ideal. Cronbach's alpha and composite reliability (CR) were used to assess construct reliability. The recommended cut-off of Cronbach's alpha and CR are both 0.70. Construct validity is established through two forms of validity: convergent validity and discriminant validity. The average variance extracted (AVE) method was used to estimate the convergence validity of scale items. Discriminant validity in the study was assessed for subscales using the Fornell and Larcker Criterion and Heterotrait-Monotrait (HTMT) Ratio.
Results
In this study, 586 questionnaires were handed out, and 256 were removed because of missing or incomplete responses. We compared the demographic characteristics of the included and missing questionnaires in Table 1. Table 2 we found that those who were older, male, less educated, with lower incomes and less social support (marriage and occupation) were more inclined to not complete the questionnaire. Smartphone penetration is not high in rural China, so most of the questions in the DHRQ (e.g. I feel like I’m in control (others) when I search for information online) could not be answered because they did not use internet before, and we excluded questionnaires with incomplete data. Thus, 330 full questionnaires were selected and included in the analysis. The mean age is 61.7 ± 10.0, and 64.2% of participants are women. 83% of participants are farmers (People's main work is agricultural production, including farming, planting, breeding and fishing), and 84.5% have a low income (Less than 429 euros per month). More demographic details are shown in Table 2. The theoretical maximum score of DHRQ was 75; in our population, the score is 35.8 ± 15.3. The mean score of digital learnability is 14.7 ± 7.0. Specific scores for the subscales are presented in Table 3. Age, occupation, education and income are correlated with the score of DHRQ. Higher age was associated with a lower DHRQ score, and higher education level and income level were associated with a higher DHRQ score. More information about the correlation analysis can be found in Supplemental File 2.
Comparison of baseline characteristics of included and missing subjects.

Demographic.

The score of DHRQ.

Model fit
Figure 1 overviews the predefined 5-factor solution of the Chinese version of DHRQ. CFA was computed using AMOS to test the measurement models. The model-fit measures were used to assess the model's overall goodness of fit (CMIN/DF = 5.060, CFI = 0.889, TLI = 0.869, RMSEA = 0.111, SRMR = 0.0880).8–10 TLI is a little bit lower than the borderline(more than 0.9) and RMSEA is higher than it (less than 0.08 means good model fit).

Framework for CFA. e: error term.
Construct reliability
Construct reliability was assessed using Cronbach's alpha and CR. The general DHRQ score showed a high overall Cronbach's alpha with 0.916 for the first four subscales. The internal consistency for subscales of digital skills, digital literacy, digital health literacy and digital learnability is higher than the recommended cut-off of 0.70. 9 But the Cronbach's alpha of digital usage is low. Except for digital usage, composite reliabilities ranged from 0.877 to 0.952, above the 0.70 benchmark, 10 which means that construct reliability was established for these constructs in the study. All values are presented in Table 4.
Construct reliability and convergent validity.
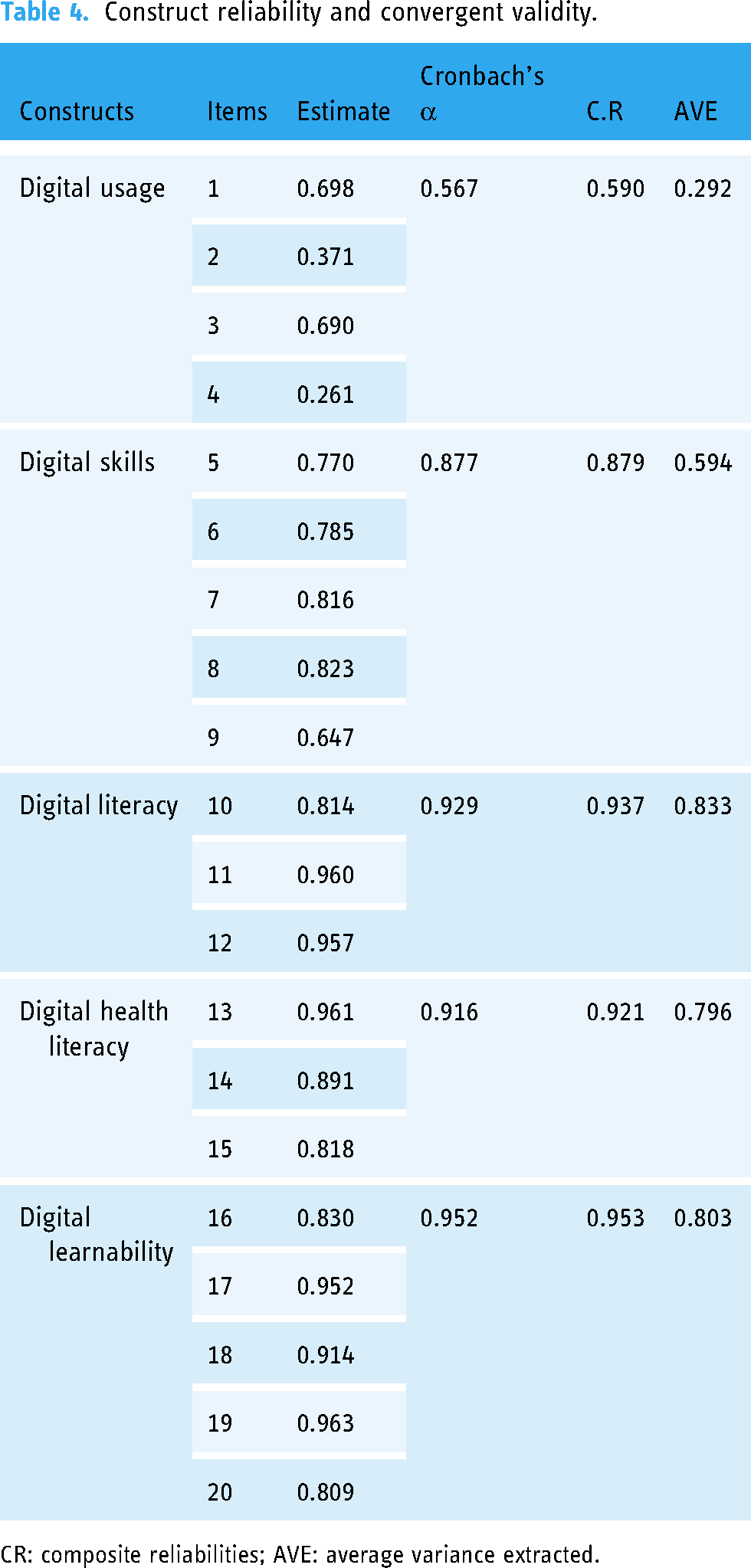
CR: composite reliabilities; AVE: average variance extracted.
Construct validity
As shown in Table 4, construct validity is established through two forms of validities: convergent validity and discriminant validity. Convergent validity of scale items was estimated using AVE. 11 The AVE values were above the threshold value of 0.50. 11 Therefore, except for digital usage, the scales used for the present study have the required convergent validity. More details about discriminant validity are in Supplemental File 3.
Modified model
As shown in Figure 2, we deleted two items 2 and 4 and did a CFA using AMOS to test the modified models. The result shows a better goodness of fit (CMIN/DF = 4.897, CFI = 0.914, TLI = 0.895, RMSEA = 0.109, SRMR = 0.0765).

Modified CFA framework. e: error term.
Discussion
Digital health interventions have the potential to partially address the gap in scarce healthcare services in rural China. However, it is essential to assess digital health readiness and provide relevant support to avoid a “digital divide.” DHRQ is a short and easy-to-use instrument suitable for use in rural areas. It identifies potential people who lack digital skills but are willing to learn new technology.
Principal findings
In this study, we translated the questionnaire DHRQ into Chinese and validated it in rural China. Our study showed that digital skills, digital literacy, digital health literacy and digital learnability have acceptable construct reliability and construct validity.
Two items in the domain of digital usage have low factor loadings. After we deleted these two items, the model showed better fit. Firstly, for item 2 “I use a computer and/or laptop,” the authors hypothesize that the low factor loading can be explained as follows: in many rural areas worldwide, including in China, the uptake of smartphones and mobile technology are often higher than computers or laptops that are connected to cable-based network connections. This is an interesting finding that could be used to optimize the DHRQ when expanding the use from the Western European setting to worldwide usage.
For item 4, “I use a wearable (fitness tracker, smartwatch, other),” distorted the results in are a growing technology and the question could grow more appropriate in coming years. Future investigations will point out if this is indeed the case.
Digital health tools are used by people in different ways, but this does not mean they are illiterate about digital health. We suggest separating the domain “digital usage” from other domains in the Chinese and possibly worldwide version of DHRQ. Using this approach, we could better understand digital literacy, digital learnability, and digital usage.
Comparison to prior work
The total score of the DHRQ is low in rural China (47.3%, 35.8/75.0) compared to the score in Belgium. 7 Digital health literacy is correlated with telehealth utilization, which explains why only 0.67% (14/2101) of people in rural areas use telemedicine services, whereas 10% of the population in urban areas use web-based healthcare communication or management. 8 Improving digital health literacy in rural areas is, therefore, essential for expanding the use of digital health interventions. Moreover, the total score of the DHRQ is lower compared to the score in Belgium (35.8 ± 15.3 vs 54.1 ± 18.6), this could be explained by the education level. The educational attainment of the Belgian sample is higher than that of the Chinese rural sample. It might also be because of the economy, as 80.9% of the Belgian population owns a smartphone, compared to 56.3% in rural China. In addition, China's rural areas have insufficient medical resources and poor network accessibility. In the future, we could provide digital health training programs to improve the digital health readiness of people willing to learn in rural areas so that they can engage in digital pathways in the future.
Limitations
There are limitations in this study. First, we only included the complete 330 questionnaires out of the 586 questionnaires issued in the analysis. The sample size is much reduced according to the pre-calculated, but 300 is also suitable for the validated factor analysis. Second, since we excluded incomplete questionnaires, and most of the incomplete questionnaires were due to not having a smartphone or not having access to the internet, this may have caused selective bias. Third, although we included all 12 villages in Daxing Township, this was a single-center survey as it was only within Liaoyuan City.
Conclusion
The DHRQ is a new tool to assess digital health literacy and digital health readiness in patient groups to assess the potential to participate in novel and evolving digital health interventions. To increase applicability and generalizability in rural areas, it should be considered to use the calculation of only the parts Digital skills, Digital literacy and Digital health literacy which are equally applicable in a Belgian population as in a rural Chinese population.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231216604 - Supplemental material for Validity and reliability of the Chinese version of digital health readiness questionnaire among hypertension patients in rural areas of China
Supplemental material, sj-docx-1-dhj-10.1177_20552076231216604 for Validity and reliability of the Chinese version of digital health readiness questionnaire among hypertension patients in rural areas of China by Linqi Xu, Tianzhuo Yu, Xin Leng, Tianyue Yu, Martijn Scherrenberg, Maarten Falter, Toshiki Kaihara, Sevda Ece Kizilkilic, Hanne Van Erum, Hanne Kindermans, Paul Dendale, Qian Tong and Feng Li in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076231216604 - Supplemental material for Validity and reliability of the Chinese version of digital health readiness questionnaire among hypertension patients in rural areas of China
Supplemental material, sj-docx-2-dhj-10.1177_20552076231216604 for Validity and reliability of the Chinese version of digital health readiness questionnaire among hypertension patients in rural areas of China by Linqi Xu, Tianzhuo Yu, Xin Leng, Tianyue Yu, Martijn Scherrenberg, Maarten Falter, Toshiki Kaihara, Sevda Ece Kizilkilic, Hanne Van Erum, Hanne Kindermans, Paul Dendale, Qian Tong and Feng Li in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076231216604 - Supplemental material for Validity and reliability of the Chinese version of digital health readiness questionnaire among hypertension patients in rural areas of China
Supplemental material, sj-docx-3-dhj-10.1177_20552076231216604 for Validity and reliability of the Chinese version of digital health readiness questionnaire among hypertension patients in rural areas of China by Linqi Xu, Tianzhuo Yu, Xin Leng, Tianyue Yu, Martijn Scherrenberg, Maarten Falter, Toshiki Kaihara, Sevda Ece Kizilkilic, Hanne Van Erum, Hanne Kindermans, Paul Dendale, Qian Tong and Feng Li in DIGITAL HEALTH
Footnotes
Acknowledgements
We thank Dr Meidi Shen and Dr Lirong Guo for their review and value feedback on the questionnaire.
Contributorship
LX contributed to conceptualization, study design, questionnaire translation, data analysis, writing of the article and project administration. TY contributed to questionnaire translation, recruitment management, data collection, data analysis and critically revised the article. XL contributed to questionnaire revision and data collection. TY contributed to questionnaire revision and data collection. MF contributed to conceptualization, study design and critically revised the article. MS contributed to conceptualization, study design, and critically revised the article. TK contributed to conceptualization and study design. SK contributed to critically revised the article. HE critically revised the article. HK contributed to conceptualization, study design and critically revised the article. PD conceptualization, study design and critically revised the article. QT conceptualization, study design, and critically revised the article. FL conceptualization, study design, critically revised the article and funding acquisition.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study has been approved by the Human Research Ethics Committee of the School of Nursing, Jilin University (HREC 2022081201). Informed consent was obtained from all participants and the research team maintained the confidentiality of participant information involved.
Funding
This study is funded by Remote Management of Cardiovascular and Peripheral Vascular Diseases Technology and Intelligent System Development (2022YFC3601300).
Guarantor
FL.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.