
Abstract
Objective
To evaluate the effect of intervention by Teach-back and Douyin platform short video health education on stigma, reproductive quality of life, family intimacy and family adaptability in women receiving infertility treatment.
Methods
This study is a quasi-experimental study. The intervention period is 6 weeks, and the study was implemented between January 2022 and August 2022. A total of 80 women (40 in the control group and 40 in the observation group) receiving infertility treatment were included in the study. The control group was given routine health education intervention, and the observation group was given Teach-back and Douyin platform short video health education on the basis of routine health education. The Chinese version of the Infertility Stigma Scale, the Infertility Quality of Life Questionnaire and the Family Intimacy and Adaptability Scale were used to evaluate the effects before and after the intervention.
Results
After the intervention, the total score of stigma in the observation group was significantly lower and lower than that of the control group (P < 0.05) and the total score of reproductive quality of life in the observation group was significantly higher than that of the control group (P < 0.05). The dissatisfaction score of family intimacy in the observation group was significantly lower than that of the control group (P < 0.05), and the dissatisfaction score of family adaptability in the observation group was significantly lower than that of the control group (P < 0.05).
Conclusion
Teach-back and Douyin platform short video health education can reduce the stigma in women receiving infertility treatment and improve their reproductive quality of life, family intimacy and family adaptability.
Keywords
Introduction
Infertility refers to the situation that couples live together for 1 year or more, have a normal sexual life, are not pregnant without contraception and can generally be divided into two types, primary infertility and secondary infertility. 1 Studies have shown that the prevalence of female infertility in the world is about 10% 2 and that in China is about 15.5%. 3 With the increase of the number of infertility patients year by year, the diagnosis and related treatment of infertility have brought different degrees of influence on patients’ body, mind and family, and infertility is considered as a major stressful event in life. 4
Infertility is a challenging medical condition that affects a significant number of women worldwide. Unfortunately, societal attitudes and perceptions surrounding infertility often contribute to the stigmatization of affected individuals. Stigmatization refers to the process of labelling and marginalizing individuals based on a particular characteristic, leading to social discrimination and negative stereotypes. 5
The stigma associated with infertility can manifest in various ways, including societal pressure to conceive, blame and guilt attributed to the woman and the perception of inadequacy or failure in fulfilling traditional gender roles. This stigma surrounding infertility can have profound effects on the well-being and mental health of women. It may impact their self-esteem, body image and overall quality of life. 6
Recognizing and addressing the stigmatization of infertile women are crucial for promoting empathy, understanding and support within society. By raising awareness, educating the public and fostering a supportive environment, we can work towards reducing the stigma associated with infertility and promoting inclusivity and compassion for those facing these challenges. 7
Douyin is a music creative short video social software hatched by Beijing ByteDance Technology Co. Ltd. 8 This software was launched in 2016, and it is a short video community platform for all ages. Users can shoot video works through this software to form their own works. 9 By December 2022, the number of users in Douyin had exceeded 800 million.
‘Teach-back’, also known as ‘feedback method’ and ‘feedback teaching’, is an interactive learning process between health care providers and recipients, and its implementation mainly includes four basic steps, interpretation–evaluation–clarification–understanding. 10 Studies have shown that Teach-back has great value and potential in increasing information understanding, improving health literacy, reducing readmission rate and promoting health behaviour. 11 At present, health educators have widely used Teach-back in the medical field, mainly including patients with chronic diseases, patients after surgery, pregnant women. 12
This study aims to evaluate the effect of Teach-back and Douyin platform short video health education on reducing the stigma in women receiving infertility treatment, improving their reproductive quality of life, family intimacy and family adaptability. The emergence of Internet and Douyin platform provides new possibilities for continuous health education for patients after discharge. During the hospitalization and after discharge, researchers provide health education through Teach-back and short videos on the Douyin platform in women receiving infertility treatment. Whole-process and all-round health education can maximize patients’ awareness of diseases and improve their emotions and behaviours.
Subjects and methods
Subjects and design
The convenience sampling method was used to select the women receiving infertility treatment who were admitted to the Obstetrics and Gynaecology Department of a tertiary hospital in Sichuan Province, China, from January to June 2022. The simple random method was adopted for research grouping. Our researchers recruited participants based on inclusion and exclusion criteria and divided them into a control group and an observation group according to the last digits of their hospital admission numbers. Patients with an odd admission number were assigned to the control group, while patients with an even number were assigned to the observation group. This study was conducted with single blindness, participants not knowing which group they belonged to. Our researchers inform participants that they will receive infertility-related health education, without disclosing that we are conducting a controlled study. The study design was approved by the College Ethics Committee (Approval Number: 2022-K011).
The inclusion criteria were as follows: (a) meeting the WHO diagnostic criteria for infertility, (b) female, (c) over 18 years old, and (d) possessing written reading and language communication skills. The exclusion criteria were as follows: (a) patients with serious diseases and tumours and (b) patients with a history of mental illness or consciousness disorder.
The sample size comprised of 70 women, with 35 allocated to the control group and 35 assigned to the observation group, who were undergoing infertility treatment. The power was set at 80%, confidence interval at 95% and significance level at 0.05. Considering the potential for dropouts or losses during the study, a total of 80 women (40 in the control group and 40 in the observation group) receiving infertility treatment were included in the study. There was no significant difference in the general data of the two groups (P > 0.05, Table 1).
Comparison of the general data between control and observation groups.

The participants in both groups completed questionnaires at two specific time points: T1 (before the intervention) and T2 (after the intervention). Notably, no participants withdrew from the study, resulting in a questionnaire return rate of 100%.
Methods
Control group
Patients received a conventional pre-hospitalization stage–hospitalization stage–discharge stage model of care. One (1) day before discharge, the responsible nurse will give discharge guidance, including medication, diet, psychological counselling, discharge procedures, follow-up visits and consultation methods. Responsible nurses orally preached, emphasizing the importance, principles and precautions of maintaining physical and mental health to patients, guiding patients to build confidence in overcoming the disease and informing patients of the time, frequency, duration and content and methods of follow-up visits to health education.
Observation group
On the basis of the control group, the observation group adopted the Teach-back and Douyin platform short video health education, as follows:
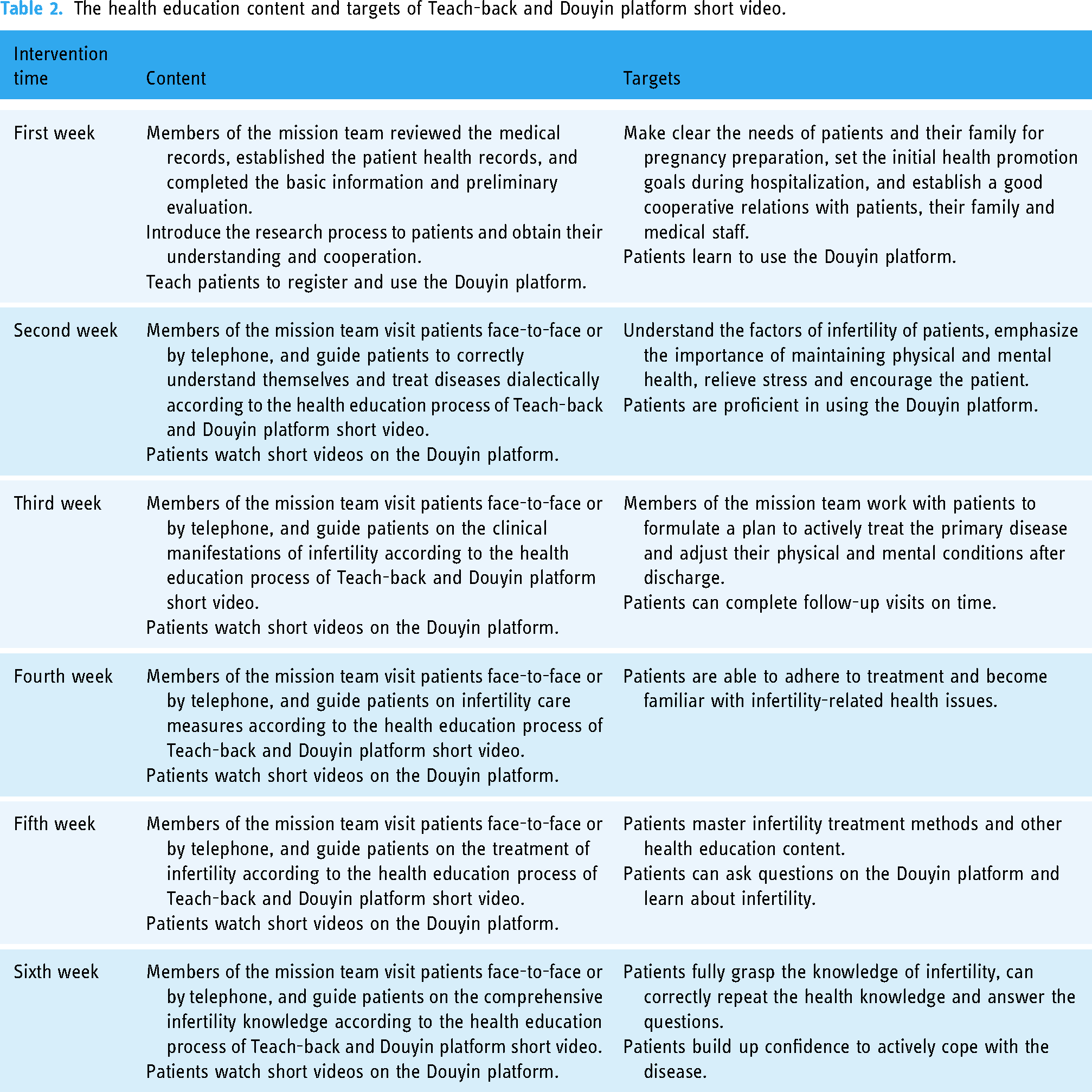
Set up a mission team. The selected candidates have a bachelor degree or above, more than 5 years of working experience in obstetrics and gynaecology, professional knowledge in obstetrics and gynaecology nursing, psychology, education, obstetrics and gynaecology, certain clinical judgment and comprehensive analysis ability, strong language expression ability, patience and good communication skills. After training and passing the examination, the above-mentioned personnel will become members of the mission team of this study, with a total of eight. Produce and publish short videos on the Douyin platform. The mission team writes video scripts. Each health mission video is recorded by four team members, with a trained nurse demonstrating the specific method, a nurse explaining the audio, a member recording the audio and a member editing the video. A total of six short videos were produced, each of which was about 3–5 minutes long, covering disease-related knowledge, medication care, diet care and psychological counselling. Register an account for mission team on the Douyin platform and publish a short video every week. Patients in the observation group can log in to the platform to watch, learn and ask questions at any time. Develop a Teach-back health education process. (a) Interpret information. Evaluate the patient's condition, explain and demonstrate the clinical manifestations, treatment methods and nursing measures in women receiving infertility treatment that patients need to master. Emphasize the significance of insisting on treatment and balancing physical and mental health to patients. (b) Evaluate information. Assess the patient's mastery and understanding of infertility-related knowledge, ask patients about infertility-related knowledge and ask patients to repeat the content of health education. (c) Clarify information. Assess the patient's mastery and understanding of the health education content and re-explain and guide the incomplete, inappropriate, and unclear content of the patient's retelling. (d) Understand information. Open-ended questions were asked again to assess the patient's understanding of the health education information. The frequency is once a week. Implement Teach-back and Douyin platform short video health education. According to the Teach-back health education process, members of the mission team regularly provide health education on infertility-related knowledge to patients and remind patients to watch short videos on the Douyin platform. The intervention period is 6 weeks, and the study was implemented between January 2022 and August 2022. The health education content and targets of Teach-back and Douyin platform short video, Table 2.
The health education content and targets of Teach-back and Douyin platform short video.
Evaluation method and study outcomes
Infertility patients’ stigma scale was used to evaluate the stigma in women receiving infertility treatment. 13 The scale includes 27 items in four (4) dimensions. There are seven (7) items on self-disparagement, five (5) on social withdrawal, nine (9) on humiliation of surrounding people and six (6) on family humiliation. Each item was scored on a Likert five-level scoring scale, and the score of each item was 1–5 points. The total score was the sum of the scores of the four dimensions. The higher the total score, the higher the level of infertility stigma. This scale is validated by the researchers, the content validity index is 0.92, representing good content validity, and the coefficients of Cronbach's α in total scale and four (4) dimensions were between 0.77 and 0.94. 14 This is primary outcome of the study.
The reproductive quality of life scale was used to evaluate the reproductive quality of life in women receiving infertility treatment. 15 The scale includes 36 items in six (6) dimensions, which are divided into two parts: core module and selective treatment module, and two independent items: living conditions and physical conditions. The core module of 24 items includes emotional response, physical and mental relationship, marital relationship and social relationship and the selective treatment module of 10 items including treatment tolerance and treatment environment. Each item was scored on a Likert five-level scoring scale, and the score of each item was 0–4 points. The original score was the sum of the scores of each item and then standardized into 100 points. The standard score is calculated by multiplying the original score by 25/item number. The higher the score, the higher the level of reproductive quality of life. Scholar Yang Xiaoping analysed the reliability and validity of this scale and found that the coefficients of Cronbach's α, the Chinese version of the Scale, was 0.93, with good reliability and validity. 16 This is a secondary outcome of the study.
The family intimacy and adaptability scale was used to evaluate the family intimacy and adaptability in women receiving infertility treatment. 17 The scale includes 30 items in two (2) subscales, family intimacy and adaptability. Family intimacy includes three (3) sub-dimensions: ideal intimacy, actual intimacy and dissatisfaction with intimacy. Family adaptability includes three (3) sub-dimensions: ideal adaptability, actual adaptability and dissatisfaction with adaptability. Each item was scored on a Likert five-level scoring scale, and the score of each item was 1–5 points. The scores of actual intimacy, ideal intimacy, actual adaptability and ideal adaptability are the sum of the scores of each item. The higher the score, the better the family intimacy and family adaptability. The absolute value of the difference between actual intimacy and ideal intimacy is the score of intimacy dissatisfaction, and the absolute value of the difference between actual adaptability and ideal adaptability is the score of adaptability dissatisfaction. The higher the absolute value, the higher the dissatisfaction. A study has verified that the coefficients of Cronbach's α of the scale is between 0.68 and 0.85, which has good reliability and validity. 18 This is secondary outcome of the study.
Statistical methods
All data were analysed using SPSS 22.0 statistical software. The measurement data were expressed as mean and standard deviation. The count data were expressed as frequency. The t-test, χ2 test, Fisher's exact test, and Wilcoxon test were used. P < 0.05 or α = 0.05 was regarded as a statistically significant.
Result
Primary outcome
A comparison of stigma in women receiving infertility treatment between control group and observation group before and after the intervention is shown in Table 3.
Comparison of stigma in women receiving infertility treatment between control group and observation group before and after the intervention.

Secondary outcomes
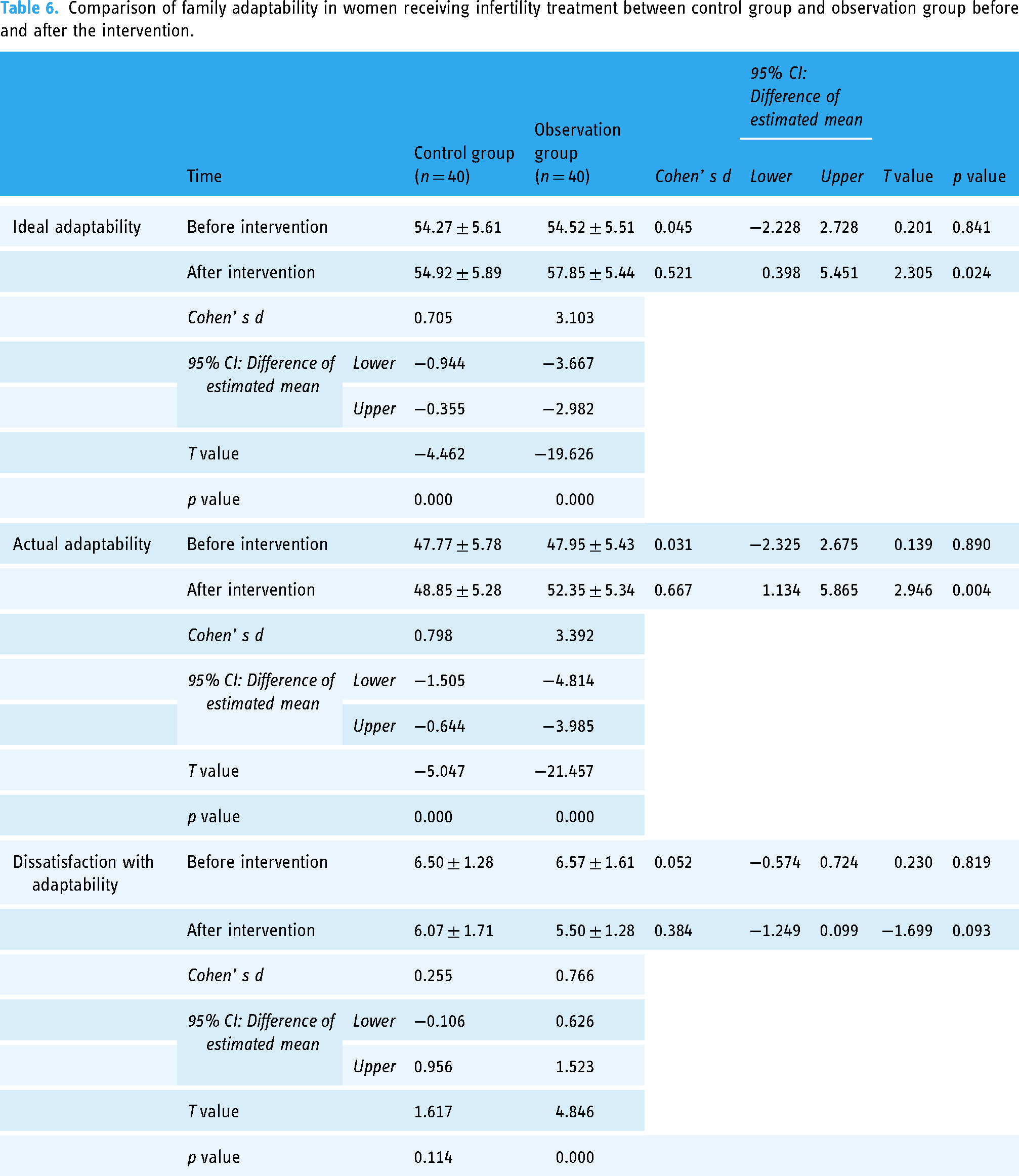
A comparison of reproductive quality of life in women receiving infertility treatment between the control group and observation group before and after the intervention is shown in Table 4. A comparison of family intimacy in women receiving infertility treatment between the control group and observation group before and after the intervention is shown in Table 5. A comparison of family adaptability in women receiving infertility treatment between the control group and observation group before and after the intervention is shown in Table 6.
Comparison of reproductive quality of life in women receiving infertility treatment between control group and observation group before and after the intervention.

Comparison of family intimacy in women receiving infertility treatment between control group and observation group before and after the intervention.

Comparison of family adaptability in women receiving infertility treatment between control group and observation group before and after the intervention.
Discussion
Infertility is a special reproductive health problem, which has become the third largest disease in the world after tumour and cardiovascular diseases. The treatment of infertility requires repeated invasive surgery, which has long treatment cycles and poor treatment effect. Certainly, it has brought great psychological pressure and physical and mental pain to infertile women. 19 As a new medical mode, mobile health refers to a time mode of supporting medical care and nursing through mobile devices, such as mobile phones, patient monitoring devices and personal digital assistant devices. 20 In recent years, mobile health technology has been widely used in health education and symptom management for patients with cancer, coronary heart disease and stroke and achieved good results. In this study, the Douyin platform is based on the Internet, with a simple user interface and strong applicability. Infertile women can watch health education short videos online, ask questions online and get feedback. In addition, infertile women can access the platform at any time to repeatedly learn short videos of health education, and if in doubt, they can also ask questions online to get health guidance, providing effective communication channels and interactive tools for patients’ post-discharge education.
The stigma in women receiving infertility treatment refers to the imaginary or actual fear of being rejected and humiliated by infertile women because of the fact of infertility, and then, it shows a negative psychological experience of self-humiliation and self-blame. 21 Women who receive infertility treatment generally have a high level of stigma, which brings negative emotions such as anxiety, depression and fear to patients. Researches have shown that the influencing factors of stigma among infertile women include social support, occupation and education level. 22 In this study, infertile women in the control group and the observation group had higher scores of stigma before the intervention. Routine nursing and follow-up were given to the infertile women in the control group; Teach-back and Douyin platform short video health education was given to the infertile women in the observation group, which effectively reduced the score of stigma of the two groups, and the stigma scores in women receiving infertility treatment in the observation group were lower than those in the control group (Table 3). After participating in this project, the reproductive needs in women receiving infertility treatment were understood, their physical and mental pressures were released, they gained more support from society, family and themselves, their awareness of self-affirmation increased and their level of stigma decreased.
In recent years, obtaining health information through social media platforms, such as WeChat and Douyin, has become the consensus of the public. Information technologies, such as the Internet and multimedia, have played a significant role in positively affecting the care of chronic diseases and other diseases. 23 Teach-back and Douyin platform short video health education can improve the reproductive quality of life in women receiving infertility treatment in the observation group, which is higher than that in the control group (Table 4). After participating in this project, infertile women can comprehensively learn and understand infertility-related knowledge, medication care, diet care and psychological counselling through the Douyin platform, ensuring continuous health education after discharge and improving the reproductive health level in women receiving infertility treatment. The implementation of this project has provided them with a platform and access to obtain correct health knowledge, enhanced their confidence in overcoming diseases and improved the reproductive quality of life.
After the diagnosis of infertility, the family should have a strong support in women receiving infertility treatment. However, the process of infertility treatment is complicated, the treatment period is long and medical expenses are high, which brings economic and psychological burdens to the family and infertile women. Therefore, the family intimacy and family adaptability in women receiving infertility treatment are affected, and there is a downward trend.24,25 In this study, Teach-back and Douyin platform short video health education was adopted, including four steps of interpreting information, evaluating information, clarifying information and understanding information, which can help infertile women correctly understand health information and improve the effect of health education. Providing Teach-back and Douyin platform short video health education for infertile women in the observation group can effectively improve their family intimacy and family adaptability, which are higher than those in the control group (Tables 5 and 6). During the process of participating in this project, infertile women can get more disease guidance and humanistic care from medical staff, which has a positive impact on their disease cognition, disease behaviour and disease belief and is conducive to enhancing their communication and understanding with society, family and friends and promoting their family harmony.
Study limitations
This study possesses certain limitations that warrant further discussion. Firstly, the sample size was restricted to a single region, and the utilization of convenience sampling method alongside a small sample size may not ensure equal access to sampling. Additionally, the adoption of a simple random grouping method may introduce sampling errors, consequently leading to potential biases in the obtained results. Furthermore, there is a need for more comprehensive consideration of the disparities between the samples and groups. Lastly, it is worth noting that the interventions implemented in the observation group differed significantly from the routine health education provided to the control group.
Conclusion
To sum up, Teach-back and Douyin platform short video health education can effectively reduce the stigma in women receiving infertility treatment, improve their reproductive quality of life and promote their family intimacy and family adaptability. Due to the limitations, the research protocol needs to be further optimized to improve the accuracy of the research results and provide a reference basis for clinical application.
Footnotes
Acknowledgements
Thanks to all patients who participated in this project.
Contributorship
LQ and FMX conceived the study design. WJJ, ZHY and LQ developed the sampling strategy. FMX, WJJ and ZHY conducted the intervention. LQ, NYP, FWW, LL and PL performed data analyses. LQ and CP drafted the manuscript. All authors contributed to the preparation of the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Patients who voluntarily participated in this study and signed the informed consent, at the same time, had the right to opt-out.
Guarantor
N/A.