
Abstract
Objective
To analyse general practitioner–patient consultations about type 2 diabetes mellitus or cardiovascular diseases and describe (i) the nature of self-management discussions; (ii) actions required from patients during and after consultation regarding self-management; and (iii) implications for digital health to support patients during (and after) consultation.
Method
This study screened 281 general practitioner consultations conducted in 2017 within the UK general practice setting from an existing dataset containing videos and transcripts of consultations between GPs and patients. Secondary analysis was conducted using a multi-method approach, including descriptive, content, and visualisation analysis, to inform the nature of self-management discussions, what actions are required from patients, and whether digital technology was mentioned during the consultation to support self-management.
Results
Analysis of eligible 19 consultations revealed a discord between what self-management actions are required of patients during and after consultations. Lifestyle discussions are often discussed in depth, but these discussions rely heavily on subjective inquiry and recall. Some patients in these cohorts are overwhelmed by self-management, to the detriment of their personal health. Digital support for self-management was not a major topic of discussion, however, we identified a number of emergent gaps where digital technology can support self-management concerns.
Conclusion
There is potential for digital technology to reconcile what actions are required of patients during and after consultations. Furthermore, a number of emergent themes around self-management have implications for digitalisation.
Keywords
Introduction
Increasingly, patients are expected to take care of their health outside of medical settings (i.e. self-management). 1 Self-management includes the actions taken by individuals to lead a healthy lifestyle, manage their long-term condition and prevent further illness, both individually and with support from healthcare professionals. 2 It is widely promoted to empower patients, improve health outcomes, and reduce constraints on overstretched health systems. 3 However, many individuals living with chronic conditions struggle to practise self-management effectively.4–6 Yet, few studies have focused on how self-management is discussed in general practitioner (GP)–patient consultations, specifically using a patient-centred analysis.
When self-management is poorly integrated, it can lead to treatment non-compliance, negatively impacting on health outcomes.7,8 GP consultations often present a major milestone for patients to stop and reflect on making changes that are actionable and sustainable for their health and wellbeing. However, GP consultations also present a missed opportunity to help patients in that regard. Limited studies have explored what ‘work’ is required from patients during and after the consultation regarding self-management.9,10 In some circumstances, self-management is discussed hastily due to time pressures in a consultation; 11 and some self-management recommendations, whilst given with goodwill, may fail to acknowledge the specificities of the individual, such as daily routine, physical environment, social obligations, as well as beliefs and attitudes.12–15 As a result, some patients leave the consultation feeling unsupported, not knowing what to do or how to start. Over time, a patient's will and momentum to make changes diminish, and the patient returns to living in the status quo with no changes attempted, made or maintained to improve their health and wellbeing.
In parallel, well-evidenced interventions are not routinely introduced to patients during consultations. Specifically, digital health interventions hold the promise to improve self-management. However, numerous studies evaluating digital self-management interventions showed a high participant dropout rate, with some studies having retention rates of 1% by the end of the study period.12,15–17 In particular, participants reported the lack of ‘fit’ of the intervention, 18 the lack of helpful advice received from the intervention, 18 or the inconsistency between GPs’ advice and the digital intervention as major reasons for discontinuation of use. 18
Understanding whether there is dissonance between GP advice, patient circumstances and the work involved in self-management is important to overcome barriers and challenges. Past studies reporting on challenges to self-management have focused on the difficulty in self-management, 5 time invested and required, 19 competing priorities,20,21 support sources required 22 and how self-management differs between patients’ and healthcare professionals’ perspectives. 11 These previous approaches relied on self-report methods (interviews, focus groups and questionnaires), medical records, or direct observation (researchers being present), which are subject to levels of reliability in self-report data, lack of meaningful data in medical records, and the degree of discomfort participants experience during direct observation. No studies have examined what actually happens inside a GP–patient consultation regarding self-management.
To our knowledge, this is the first study that examines how self-management is discussed in GP consultations. It also addresses three major gaps in the literature, namely the lack of studies reporting: (1) what happens inside a GP–patient consultation regarding self-management; (2) patient-centred analysis on the work required in self-management (during and after the consultation); and (3) implications for digital health to support patients during (and after) consultation.
Materials and methods
Study design and setting
This study is a secondary multi-method analysis, including descriptive, content and visualisation analysis. The dataset originates from a large qualitative mixed-methods study titled ‘Harnessing Resources from the Internet to maximize outcomes for GP consultations’ (HaRI): A mixed qualitative methods study to investigate internet use in GP. 23 The HaRI archive contains 281 GP consultations video-recorded during 2017 by 10 GPs, working at eight different GP clinics. These clinics are distributed across a wide range of urban, suburban and rural areas and counties in Southeast England. For details on how patient and GP participants were selected and recruited in the original HaRI study, please refer to Seguin et al. 23
Ethics approval was obtained for the original collection of these consultations (HaRI) from National Health Services (16/LO/1029; IRAS project ID: 197875), and secondary use of the HaRI archive from NHS (REC reference: 19/LO/0364 Protocol number: 120807 IRAS project ID: 257924) and in Australia from Macquarie University Human Research Ethics Committee for Medical Sciences (reference number: 52020558018892), where written consent has been given by participants for their data to be used for secondary data analysis (including this study).
Data screening
We categorised the HaRI data according to the primary reason the patient saw the GP according to ICPC-2 (International Classification of Primary Care). 24 We searched the accompanying SPSS metadata file that comes with the HaRI archive for all cases where the primary reasons for seeing the GP were coded as ‘Endocrine’ or ‘Cardiovascular to identify potentially relevant consultations. We eliminated duplication of any consultations from the HaRI archive. Three researchers (JR, UR and AL) read the transcripts of these extracted consultations, where 32 consultations met the inclusion criteria, and 19 consultations remained after meeting the exclusion criteria. Out of 19 consultations that met eligibility criteria, 11 discussed type 2 diabetes mellitus (T2DM), and eight discussed cardiovascular diseases (CVDs).
Inclusion criteria
Consultations that discuss T2DM or CVD as part of a patient's presentation or past medical history.
Consultations where any lifestyle advice, self-management support or behavioural modifications related to T2DM/CVD management or prevention were discussed by the GP or patient.
Consultations where a transcript and/or de-identified video recording of the consultation between GP and patient was available.
Exclusion criteria
Consultations with patients with gestational diabetes, type 1 diabetes or prediabetes.
Consultations with patients with T2DM or CVD that did not contain any discussion of lifestyle advice, self-management support, or behavioural modifications related to diabetes management or prevention.
Consultations where T2DM or CVD was discussed did not concern the patient(s) physically present at the GP office.
Data analysis
Descriptive statistics, content analysis, and visualisation analysis were used to analyse the 19 transcripts (see Supplemental Appendix A, Figure 1).

Comparison of average frequency and duration across clinical tasks conducted by general practitioners (GPs) during a consultation (n = 19).
Statistical analysis
Descriptive statistics were reported for patient demographics (e.g. age and gender) and consultation characteristics (e.g. whether a companion was present, topics and conditions discussed, and use of subjective and objective measures during consultation). A Mann-Whitney U-test was used to compare the average count of topics discussed between T2DM and CVD consultations to confirm there were no statistically significant differences between them before grouping the conditions to be analysed as one group.
Content analysis
To examine the tasks conducted by GPs during consultations, as well as topics and actions discussed between GPs and patients, we adapted Assarroudi's three-phase directed content analysis approach, 25 and devised 14 steps for preparation, organisation and reporting to analyse the transcripts (shown in Table 1).
Directed content analysis.

Visualisation approach
We used visual inspection to identify different visit types common in consultations involving T2DM and CVD. We also referred to the ‘Present Complaint’ code from Kocaballi et al. 26 framework to identify whether the visit was related to medication review, investigation/test results review, or review of condition. We used Miro software 29 to illustrate flowcharts representing each visit type, where codes from both GP and patient-centred activity frameworks were used in the visualisation.
Results
Patient demographics and consultation characteristics
Table 2 describes patient demographic and consultation characteristics of included consultations. Overall, 19 in-person consultations are analysed in this study, where 11 pertain to T2DM and eight to CVD management.
T2DM and CVD demographics and consultation characteristics (n = 19).

T2DM: type 2 diabetes mellitus; CVD: cardiovascular disease; BNP: Brain Natriuretic Peptide; IVF: in vitro fertilization; HRT: hormone replacement treatment.
Consultation activities
GP-centred activities
Across the 19 consultations, a consultation on average contains 9.7 GP-centred activities (SD = 2.2) meaning GPs on average are engaged in 9.7 clinical tasks in a consultation. Similar numbers are found across T2DM consultations (mean = 9.9 GP-centred activity codes; SD = 2.1) and for CVD consultations (mean = 9.4; SD = 2.2). A Mann-Whitney U-test was performed to confirm there was no significant difference in the average number of GP-centred activity codes across CVD and T2DM consultations (U = 38.5, p = 0.645), suggesting CVD and T2DM consultations in this sample can be combined for analysis on GP-centred activity codes.
Figure 1 compares the average frequency and duration across clinical tasks conducted by GPs during a consultation. This classification of tasks was adapted from Kocaballi et al. 26 All consultations (100%, 19/19) involved Assessment (i.e. assessing a patient's situation during a consultation), where Assessment is also the task that took the longest during a consultation (30% average duration). The next most frequent clinical task that GPs conducted during a consultation was Treatment-Follow up, where 89% (17/19) of consultations incorporated this task and on average occupied 4% of a consultation. Non-pharmacological Treatment was discussed in 74% (14/19) of consultations, where discussion on average took 6% of a consultation.
Patient-centred activities
Across the 19 consultations, a consultation on average contains 7.3 patient-activity codes (SD = 1.5), meaning patients on average perceive 7.3 topics were discussed that are related to self-management during a consultation. Similar numbers are found across T2DM consultations (mean = 7.3 patient-centred activity codes; SD = 1.9) and for CVD consultations (mean = 7.3; SD = 0.83). After conducting a Mann-Whitney U-test, no significant difference was found in the average number of patient-centred activity codes across T2DM and CVD consultations (U = 43.0, p = 0.932), suggesting CVD and T2DM consultations in this sample can be combined for analysis on patient-centred activity codes.
Figure 2 compares the average frequency and duration across patient-centred activities related to self-management during a consultation. All consultations (100%, 19/19) involved Condition monitoring (i.e. monitoring of clinical parameters, symptom measures and daily activities related to the condition), where Condition monitoring is also the activity that took the longest during a consultation (20% average duration). The next most frequent activity during consultation was Medication, which occurred in 95% (18/19) of consultations and on average occupied 19% of a consultation. Lifestyle Choices were discussed in 79% (15/19) of consultations, where discussion on average constituted 16% of a consultation.

Comparison of average frequency and duration across topics perceived by patients related to self-management during a consultation (n = 19).
Content and visualisation analysis
Content analysis and visualisation approach revealed three major activities performed during T2DM and CVD consultations, namely medication review, results review, and condition review. Definitions and details of each visit type are found in Supplemental Appendix A. A focus on how often and how long Lifestyle Choices were discussed during a consultation are also outlined for each of these three visit types.
Medication review
Figure 3 illustrates a typical consultation for CVD and T2DM where medication review is the major activity. These consultations discuss how the patient has been taking their medications, any concerns on medication adherence behaviours, side effects reported by the patient, and whether medication or the existing dose needs to be changed. These consultations also discuss other aspects such as symptoms and lifestyle. Amongst medication reviews (n = 5), Lifestyle choices were discussed in 80% (4/5) of consultations, where it occupied 17% of a consultation.

Example of a typical medication review consultation.
Results review
Figure 4 illustrates a typical consultation for CVD and T2DM where results review is the major activity. These consultations discuss the results of an investigation ordered previously. They often acknowledge a patient's understanding, and their progress is defined by GP and patient discussion on the results of the investigation. Amongst results review (n = 10), Lifestyle choices were discussed in 90% (9/10) of consultations, where it occupied 17% of a consultation.

Example of a typical results review consultation.
Condition review
Figure 5 illustrates a typical consultation for CVD and T2DM where condition review is the major activity performed. A condition review often includes a discussion of recent or past investigations, diabetes or heart complications like diabetic foot, neuropathy, kidney diseases, as well as any new or ongoing symptoms. These consultations encompass the chronic condition as a whole, rather than referring to specific aspects in isolation. Amongst review of condition (n = 4), Lifestyle choices were discussed in 50% (2/4) of consultations, where it occupied 11% of a consultation.
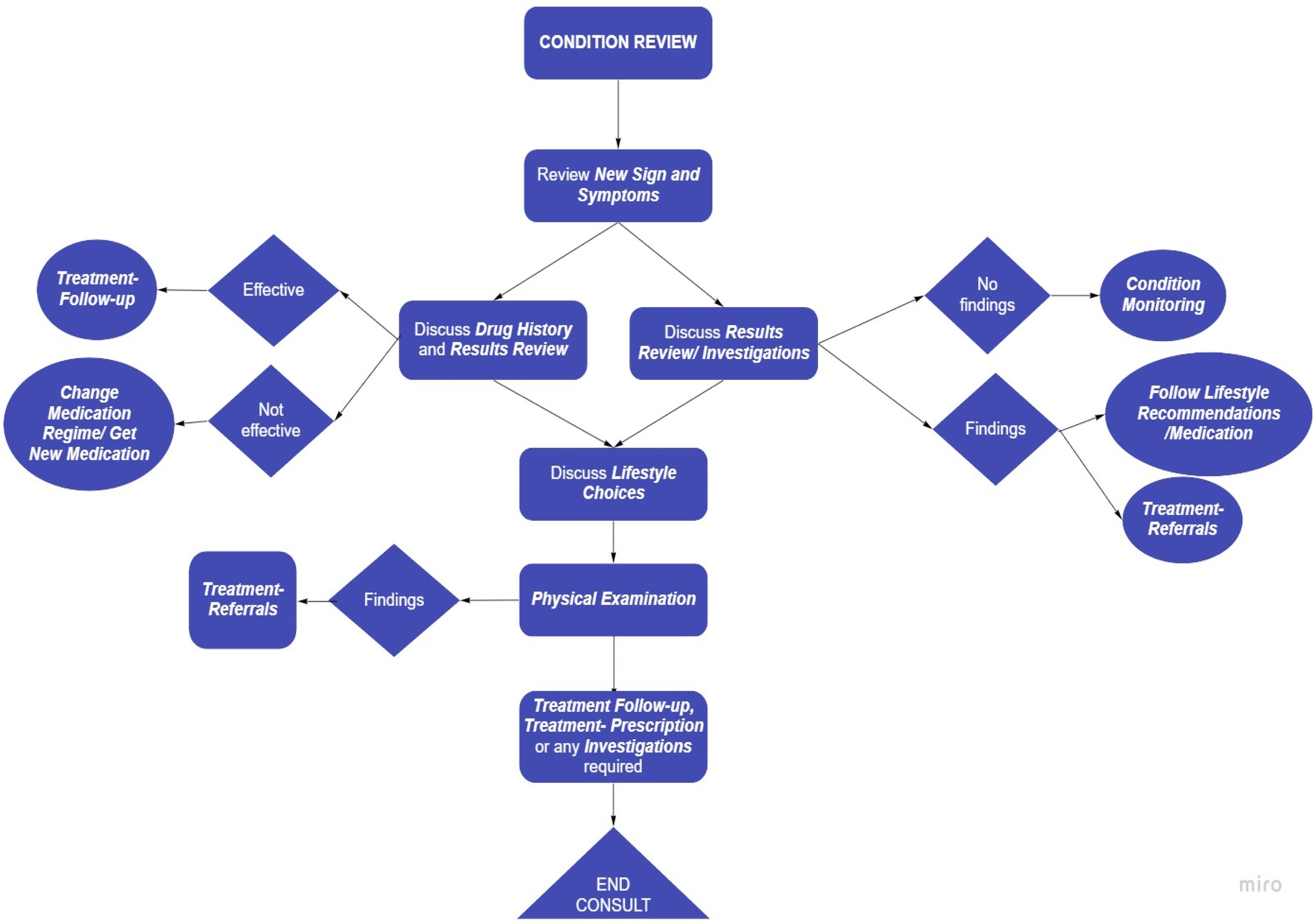
Example of a typical condition review consultation.
Actions required of patients during and after consultation
Table 3 describes the actions required of patients during and after a GP consultation relating to self-management of T2DM and CVD. The top five most frequent actions required of patients during GP consultations are: seek clarification about their current condition (89%, 17/19); discuss medication rationale and use (79%, 15/19); monitor clinical measures (e.g. blood pressure, temperature) (79%, 15/19); discuss referrals (68%, 13/19); and listen to GP's explanation (e.g. test results) (68%, 13/19).
Frequency of actions required of patients during and after GP consultation relating to self-management of T2DM and cardiovascular health (n = 19

However, the top five frequent actions required of patients after a GP consultation are: organise administrative tasks (e.g. book appointments, insurance) (89%, 17/19), follow lifestyle recommendations (79%, 15/19), visit other healthcare professionals (79%, 15/19), obtain new medications (68%, 13/19) and measure and record changes in signs and symptoms (63%, 12/19).
Use of digital technology during and after consultation
Digital support for self-management was not a major topic of discussion during consultations. 26% (5/19) of consultations discussed the use of digital devices for self-management, and only one consultation involved a GP demonstrating use of digital devices to patients for self-management. Post-consultation, patients are recommended in 37% (7/19) of consultations to get digital devices to monitor their clinical measures (e.g. glucometer and blood pressure monitor).
Emergent gaps in self-management for digital health
Analysis informed by patient-centred activity codes revealed a number of areas where self-management may have been insufficiently addressed during the consultation. These ‘emergent gaps’ are potential targets for digital health technology to improve self-management both during and after primary care consultations.
Lifestyle discussions are prone to subjective inquiry and objective measures
Lifestyle factors are a significant discussion topic and often involve extensive inquiry by GPs to collect objective measures (such as blood pressure, blood glucose levels), as well as subjective measures regarding a patient's diet, exercise, or social habits. Facilitating patients to collect and retrieve objective and subjective measures of their health during GP consultation may allow patients and GPs to develop actionable tasks after the consultation. This combination of facilitating objective measures during subjective inquiry requires further investigation in the design of the GP-patient interactive system, as well as patient-facing digital technology to support self-management.
Overwhelmed by self-management
Patients express reluctance and uncertainty about the amount of medication, appointments, and their ability to manage multiple self-management tasks simultaneously. Some of these patients have companions to help them manage their health.
Expectation that ancillary services will perform more in-depth examinations
There is an expectation that certain in-depth tasks will occur outside of the GP office by nurses or other healthcare professionals. Often GPs perform examinations but possibly for lack of time, indicate that a nurse will perform certain tasks. This may complicate the primary care process for patients if it requires arranging and finding time for extra appointments. There is potential for digital health to streamline GP consultations so that these investigations can be performed within a single consult and the patient does not require multiple appointments.
Table 4 describes ‘emergent gaps’ in self-management for digital health. For each ‘emergent gap’, the relevant patient-centred activity code, transcript reference, author observations, insights for digital health, and relevant transcript quotes are provided as supporting evidence. Refer to Supplemental Appendix A, Supplementary Extracts for full consultation transcript extracts.
Emergent gaps in self-management for digital health.

Discussion
Main findings
Our findings indicate that chronic care consultations for primary care patients with T2DM and CVD are largely driven by three major activities – medication review, results review and condition review. Nevertheless, GPs typically perform similar tasks for these cohorts regardless of whether medication; condition; or results review was the major purpose for the consultation.
Self-management, in particular, is a common topic of discussion for these cohorts and pertains to many issues including medication, condition assessment, lifestyle choices and psychosocial assessment. In particular, discussions around lifestyle management are explored extensively and often in great detail during consultations in this study. Another insight was that patients sometimes feel overwhelmed by the extent of their self-management, in some cases leading to non-adherence and consequent poor health outcomes. Possibly for lack of time, physical examinations are sometimes not performed in-depth and there is an expectation that ancillary health professionals will do so.
Furthermore, within these cohorts, there is a wide variety of actions required by patients to self-manage their conditions. The most frequent actions required of patients during consultations include seeking clarification about their current condition, discussing medication rationale and use, and monitoring clinical measures. After consultation, the most frequent actions required of patients include organising administrative tasks, following lifestyle recommendations, and visiting other healthcare professionals.
Strengths and limitations
Analysing video and transcript data from actual consultations, rather than self-reported data which is subject to recall biases, enabled a more accurate representation of what happens during a GP consultation. A limitation of this study is that we do not have access to prior or follow-up consultations. Therefore, it is unknown whether self-management strategies were previously implemented and whether they have been successful. Another limitation is that chronic disease management requires multi-disciplinary care, and this data is limited to GP consultations. Therefore, the extent to which allied health and other health specialists discuss or implement self-management strategies is unknown. Lastly, this study has a small sample size with consultations in the UK only. Future studies may want to explore other sources to incorporate consultations from other countries, healthcare systems, and different clinic setups (e.g. urban vs. regional, different GP demographics).
Comparison with existing literature
Many studies have analysed self-management in primary care consultations. Lim et al. surveyed patients with T2DM and hypertension to assess the level of self-management support provided in primary care. 30 Blakeman et al. 27 conducted semi-structured interviews with a sample of patients living with long-term conditions and subsequently interviewed the health professionals. Our study used an observational study approach to ensure insights drawn reflects the true nature of GP–patient interactions occurring during consultations, which helps illuminate the context that remains poorly understood by self-reported data alone.31,32
In particular, our findings revealed that self-management discussions, particularly concerning lifestyle management, are explored in great detail. This is in contrast to findings of Blakeman et al. 27 which found a tension between doctors and patients whereby GPs were reluctant to address self-management for fear of disrupting the professional relationship. In another study, Abdelgadir et al. 33 examined doctor–patient communication to identify whether they resulted in improvements in T2DM care. They highlighted that preparing patients to identify their priorities, and learning to ask more questions, were key strategies for improving diabetes outcomes in primary care. 33
Our research also highlighted areas where digital technology could help patients with self-management during or after GP consultation. Eikelenboom et al. 34 conducted a randomised controlled trial that demonstrated personalised self-management support could enhance patient's self-management behaviours. A number of systematic reviews have demonstrated that digital interventions can improve self-management and health outcomes for patients with these conditions.35–40 Further research is required to investigate whether these digital interventions actually address the needs and concerns raised between patients and GPs during their consultation, as well as ways to integrate the use of these interventions during and/or after GP consultations.
Implications for digital health
Digital health to support self-management discussion during consultations
This study indicates that self-management tasks performed during consultations include seeking clarification about current condition, monitoring clinical measures, discussing medication, discussing referrals, and listening to GP explanations. In addition, this analysis revealed three emergent gaps in self-management during consultations, including the subjective nature of lifestyle inquiry, patients being overwhelmed by self-management, and expectations that ancillary services will perform more in-depth examinations. Researchers working in the digital health space need to be mindful that for digital technology to be effective, it will have to address these common tasks discussed, as well as ‘emergent gaps’ concerning self-management during consultations between GPs and patients.
This study also identified that some T2DM and CVD patients feel overwhelmed by self-management but may only have sporadic encounters with primary care. These patients are at heightened risk of poor health outcomes, 41 and there is a need for digital technology that can keep patients who struggle with self-management linked to the health system.
In fact, the most common ‘patient-perceived’ self-management tasks discussed during consultations to a large extent involve objective measurements (e.g. weight and BP) or discussions about treatment, results or medication. It is imperative that digital technology designed for patients and consumers can support the collection of daily activities data in order to facilitate these discussions with their GPs during consultations. There is evidence that digital health interventions (e.g. mobile apps for diabetes self-management) that involve healthcare providers have better outcomes for self-management. 42 However, despite the numerous approaches for digitalisation to improve self-management, safety concerns arise from the abundance of unregulated apps and devices on the market. Greater research is needed on the safety of widescale adoption of digital health technologies for self-management. Further research should evaluate methods to integrate digital technology into the workflow of primary care consultations.
Digital health to support self-management tasks after consultations
There is often a discrepancy between the actions required of patients during and after their GP consultations. The most common post-consultation tasks include organising administrative tasks (e.g. booking appointments) and following lifestyle recommendations (e.g. making dietary changes). Furthermore, it is clear that after consultations, there is a significant burden on patients to perform administrative tasks, as well as following lifestyle recommendations. If digital technology is to assist in self-management in a meaningful way, it needs to reconcile this discord to ensure discussions or tasks discussed during consultations become actionable items, such that patients can follow through after consultations.
How diabetes and CVD primary care consultations would adapt in telehealth
For T2DM and CVD consultations, visits are commonly categorised into three visit types: medication review; results review; and condition review. As telehealth gets rapidly adopted in primary care, it is important to assess whether T2DM and CVD consultations can indeed be supported in Telehealth. One important aspect concerns physical examinations, which occur frequently across these three visit types for patients with diabetes and CVD. Future research should examine whether tasks (e.g. physical examination) observed during in-person consultations regarding T2DM and CVD are indeed translatable to telehealth. Additionally, further research is warranted to investigate whether there are significant differences in the quality of care and health outcomes amongst people with T2DM and CVD in the long term, depending on whether they received care in-person or via telehealth. It is possible that the structure of consultations will need to adapt to telehealth, as in which steps of the consultation are either missing or added compared to in-person consultations, with reference to the different visit-types.
Conclusion
We performed a secondary multi-method analysis to understand how observation of in-person GP consultations could illuminate the nature of self-management discussions in primary care, and inform digital solutions for patients with T2DM and CVD. The results reveal disharmony between the self-management actions required of patients during and after consultations. Furthermore, this study revealed a number of emergent gaps for digital health to support patients with T2DM or CVD in self-management during and after their GP consultation. Further research is needed to explore the role of digital technology during primary care consultations, and to support the multitude of self-management tasks for patients with T2DM and CVD after consultation.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231176162 - Supplemental material for How general practitioners and patients discuss type 2 diabetes mellitus and cardiovascular diseases concerns during consultations: Implications for digital health
Supplemental material, sj-docx-1-dhj-10.1177_20552076231176162 for How general practitioners and patients discuss type 2 diabetes mellitus and cardiovascular diseases concerns during consultations: Implications for digital health by Urvashi Rohilla, Jayashanthi P Ramarao, Jared Lane, Neha N Khatri, James Smith, Kathleen Yin and Annie YS Lau in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to express their sincere thanks to Prof. Fiona Stevenson and her team for conducting the HaRI project, and for sharing their data with us in order to facilitate this research. The Harnessing Resources from the Internet (HaRI) project was funded by the UK National Institute for Health Research School of Primary Care Research. The views expressed are those of the authors and not necessarily those of the NIHR, the NHS or the Department of Health. NHS costs were covered via the Local Clinical Research Network. The authors thank Sunayana Raghuraman for her assistance throughout the project. The authors also thank Dr Tim Tse and Dr Bosco Wu for their clinical perspective as general practitioners and their feedback on the manuscript.
Author's note
James Smith is also affiliated at School of Medical and Health Sciences, Edith Cowan University, Perth, WA, Australia; School of Population Health, Faculty of Health Sciences, Curtin University, Bentley, WA, Australia; Centre for Healthcare Resilience and Implementation Science, Australian Institute of Health Innovation, Macquarie University, Level 6, 75 Talavera Road, North Ryde, Sydney, Australia.
Contributorship
Study conception: AL and JR. Study design: AL, UR, NK, JR, JS and KY. Data analysis: UR, JR, NK and JL. First draft: UR, JR and JL. Subsequent draft: all authors reviewed, edited & approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this analysis was obtained from ‘Macquarie University Human Research Ethics Committee for Medical Sciences (reference number: 52020558018892), as well as the National Health Services (NHS) (REC reference: 19/LO/0364; IRAS project ID: 257924) and NHS (RED reference: 16/LO/1029; IRAS project ID: 197875)’.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AYSL was supported by the New South Wales Health Early-Mid Career Fellowship, and her research was supported by the National Health and Medical Research Council Grant APP1134919 (Centre of Research Excellence in Digital Health) and Grant ID 1170937 (Centre of Research Excellence in Connected Health).
Guarantor
UR
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.