
Abstract
Background
Mobile apps for health (mHealth) have the potential to support people living with dementia. However, dementia is a complex and progressive condition that imposes specific constraints on the introduction/use of mhealth. Few studies have explored mHealth adoption and use within the complexity of everyday domestic settings. This study used an existing App co-designed with people living with mild cognitive and communication impairment (PWMCCI) due to learning disabilities and examined the usefulness for PWMICCI due to dementia and their carers.
Methods
A qualitative study of people with dementia and their carers. Data were collected in a phased approach to identify the potential need for, as well as the usability and utility of the app. Analysis employed the Domestication of Technology Model (DTM) to explore, in a novel way mHealth, in this user group(s).
Results
Most participants did not adopt the mHealth during the study period but some (n = 2) did routinely as it fulfilled a unique, unmet need. The use of DTM highlighted the complexities of dementia, pressure on carers and duplication of effort created barriers to app adoption and use in the long term.
Conclusions
The ability of mHealth to support PWMCCI due to dementia and/or their carers may have potential. Users were motivated to try the technology but for any potential to be fully realised, the interplay between complexity of the condition including its progressive nature, demand on carers and nature of the technology needs to be more fully understood. Such issues place unique constraints around the size and window of opportunities for mHealth in this user group.
Introduction
Government policy in the United Kingdom (UK) has long advocated the use of technology to support the nation's growing healthcare needs.1,2 Understanding if, and how, technology may, or may not work for different users/groups is however central to supporting the design and adoption of any digital health intervention (DHI) and forms the underlying philosophy of design approaches such as human-centred or user-centred design. 3 Research in this area is still developing and there is a need to understand the various design considerations which can be complex due to the intersection of individual health and social care contexts. 4 As a result, much technology deployed at the frontline of health and social care is still designed for use by the general population or the ‘worried well’ 5 and does not meet the needs of people living with specific needs who are likely to need solutions that are tailored to their requirements.
The number of people living with dementia worldwide is increasing and is predicted to increase to over 1 million in the UK by 2025 (8). People living with dementia (PWD) have specific communication and cognitive problems with the additional issue that their condition is one of progressive decline.6,7 Consequently, PWD often rely on family carers or paid carers for support to access healthcare and can experience problems in care such as poor health information exchange and follow-up leading to a cascade of patient safety issues such as errors 8 and, at the most extreme, even premature death. 9 Proposed technological approaches to address some of these issues are varied. DHIs have been cited as a way of potentially supporting PWD and/or their carers who can have various difficulties in communicating as well as performing their activities of daily living including their health and social care needs. 10 Historically, there was a focus on telecare and telemonitoring approaches focusing largely on safety and security in the community (e.g. alarms for safety in the home) but more lately mobile health (mHealth) apps housed in regular technology such as smartphones and tablets have been developed. A review of mHealth apps for people with mild cognitive impairment, including those with Alzheimer's disease and dementia, highlighted the technology (e.g. mHealth for cognitive training) appeared to improve health outcomes such as cognitive ability.11,12 Some mHealth apps may also be viewed as an assistive technology (AT) defined as technologies designed to maintain or improve an individual's functioning and independence to facilitate participation, safety and to enhance overall well-being. 13 This study is concerned with this type of AT, specifically that which is designed to have direct benefits such as helping PWD manage their daily activities and communication needs in order to function as independently and safely within their homes as possible; and thereby also potentially have the indirect benefit of alleviating some caregiver burden. 14 It is AT that is used by and/or with PWD and their carers that is the focus of this study.
Various reviews on AT for PWD highlight the variability of available technologies and quality of evidence regarding their impact.15,16 One significant issue identified across the reviews, however, is the lack of co-design in the development of AT and the importance of flexibility to allow personalisation and adaptation of technology to meet the progressive nature of dementia.
It is against this background that our study was developed. We planned to adopt a participatory approach to evaluating a digital AT that was identified to have the potential to support PWD who have mild cognitive and/or communication impairment and/or their carers. Specifically, we aimed to explore the potential usefulness and understand the ‘fit’ of an existing app originally co-designed with/for people living with mild cognitive and communication impairments (PWMCCI) and their carers due to learning disabilities for a new user group, namely PWMCCI due to dementia and/or their carers. The study was intended to be a first step in a co-production process for determining the potential usefulness of an mHealth App for people living with dementia and their carers and to identify any adaptations that might be needed for this new user group.
Method
Design
The study employed a longitudinal qualitative research design investigating the usefulness of an existing health and wellbeing app (originally designed for PWMCCI due to learning difficulties) for PWMCCI related to dementia. There were three stages in designing the study and some necessary COVID-19-induced adaptations. A phased longitudinal design was adopted to collect data from different stages of using the App (introduction, training and home use). We collected data using qualitative methods of semi-structured interviews and focus groups conducted remotely.
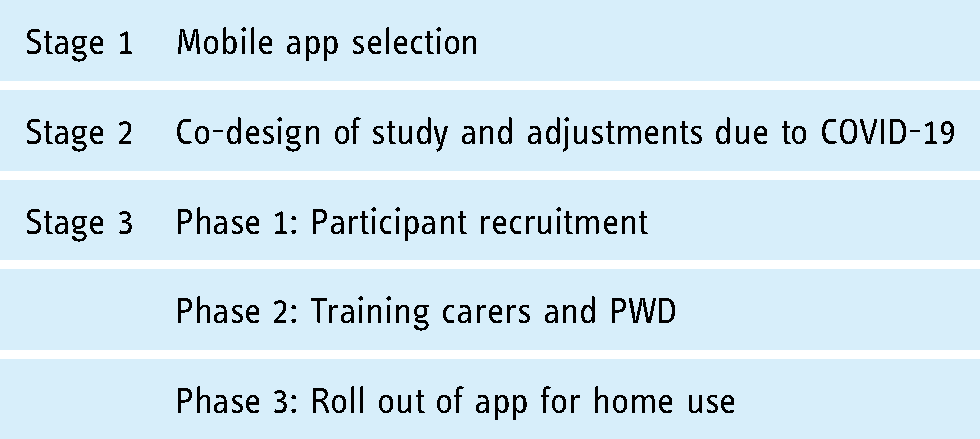
Stage 1: app selection and provider partnership formation
The research team identified an app that was designed for people with cognitive/communication impairments via the National Health Service (NHS) library of apps 1 and web-based tools designed to help people manage their health and well-being. Apps in the library have been approved in terms of clinical safety, data protection and security with some evidence around usability. 17 Through this library, we identified a potential mobile health application called Hear Me Now 2 . 18 The app had been through an inclusive design process with people with learning disabilities and their carers. The outcome of this process was an app, Hear Me Now (HMN), intended to be customisable to support the varied communication and assistance needs of individual PWMCCI due to their learning disabilities and/or their carers (see box 1). Hear Me Now had been shown to have some utility for this user group. 19


The research team and app provider, Maldaba discussed the potential for evaluating Hear Me Now for a new user group, PWMCCI due to dementia (see box 2). Maldaba considered the app had potential to support PWMCCI due to dementia (see box 3) and the study was seen as a way to understand the context of using the mHealth application for this new user group. The study aimed to explore any additional design and support needs for Hear Me Now that would be specific to PWMCCI due to dementia and/or their carers and in turn which may affect the adoption of any such technology (see box 3 for a summary of how HMN may act as an AT for PWMCCI due to dementia and/or their carers).

Stage 2: co-design and study (re-)design
From the outset, we worked with Maldaba, PWMCCI due to dementia and their carers, and a care provider in order to determine key aspects of the final study design prior to, and during a research pause caused by the COVID-19 pandemic. We chose a longitudinal qualitative approach to capture the testing and adoption process. Initially, the original design of the study included walk-through workshops plus observation and face-to-face interviews, all of which could not be conducted due to measures introduced to manage the spread of COVID-19. Instead, we adopted remote engagement and data collection methods which via our early involvement with a care organisation, were felt to be feasible for interviews. In place of the walkthrough workshops, we opted for two final focus groups with the carers discussing the broader usability, design and adoption issues around the app including any required adaptation(s) for PWMCCI due to dementia. This change had a bearing on the nature and timing of data collected throughout and ultimately constrained the participatory approach as originally planned. In the original design, the idea was that any barriers could have been raised early directly with the app providers – with potential to make some adaptations that would support testing. This means the testing took place without this foundation and issues were only raised during interviews and at the end.
Further study design feedback was done through the recruitment and training (via Zoom) of a small number of formal carers on the app. One researcher (SCS) observed these sessions. The carers provided feedback to the research team and providers on the content and duration of the training, the app content, potential utility that supported the feasibility and validity of the study aims. The training was well received in terms of length, format, content, understanding of the HMN features and potential uses. Issues around the capabilities of older users in addition to their cognitive and other health issues were raised and included factors such as their vision, hearing and dexterity. These were seen as key potential mediating factors affecting the app's adoption. Carers identified issues regarding the ability to clearly input and read information on a larger screen as well as a larger device having potentially greater audio-visual capabilities. Consequently, tablets were chosen as the main hardware for testing the app which was preferred to smartphones due to their larger size. Previous research supported this choice, indicating that a significant proportion of PWMCCI due to dementia are able to independently and successfully interact with such technology, even if they had not utilised it previously. 21 The app was available on both devices however, and participants were made aware of this during the study. Some carers also chose to download the app on their smartphones during the study.
Stage 3: the evaluation study
The design of the qualitative evaluation study involved 3 separate but inter-related phases:
Phase 1
Participant recruitment (three approaches):
PWMCCI and carers were invited to take part through a partner care organisation via advertisements through community organisations via a researcher (SCS) contacting research volunteers through the Join Dementia Research website
Initial Interview: PWMCCI were interviewed, together with their carers, in order to understand their everyday lives and care needs and how they currently managed these needs (e.g. strategies, technologies, social support). All participants were able to give informed consent, PWMCCI gave their consent based on the advice provided by family and care professionals, following the guidance outlined in the Mental Capacity Act in England and Wales.
22
Phase 2
Step 1: training carers and PWMCCI
Familiarisation with tablet technology and setup (if required)
Learning to use the app – run through key features and examples
Understanding options for and how to access support
Maldaba had previously co-created a training model whereby professional health and care staff were the primary recipients of training. Upon discussion with Maldaba and the partner care organisation, we agreed to follow the same model reasoning that any training delivered to carers could then be adapted to meet the needs of the individual PWMCCI by those who know them best. All carers received remote training (via Zoom/MS Teams) from the providers in using the technology and received immediate follow-up support in the form of written materials. Remote support options (via monthly group user support sessions, telephone and/or email) were also available. Carers then (in step 2) introduced the app and trained those that they cared for on the app features and their potential uses. In some cases, (n = 3), PWMCCI due to dementia wanted to be part of the provider training session and were seen by their carers to be technologically and cognitively capable to participate.
Step 2: interviews
Follow-up interviews with PWMCCI and their carers were conducted within a week of the training delivered and were designed to gather initial impressions of the app's suitability for either the person with dementia and/or their carer in terms of its design and potential use(s).

Phase 3
Roll out of app for use at home for 3 months
o Formal carers were given a protected hour per week dedicated to support their clients’ use/support needs with the app.
End of try-out focus groups
Participants were then asked to test out the app in supporting their everyday health and caregiving needs and activities over a period of up to 3 or more months with a final set of group interviews to provide feedback on the app's design and use. Maldaba continued to provide ongoing technical support throughout the study period.
Analysis
The data collected through the individual and focus groups were professionally transcribed verbatim. Emerging issues were discussed with the app provider throughout the data collection. Three researchers (SCS, CS and BNO) familiarised themselves with the data by independently reading through all the transcripts. SCS and BNO each coded the transcripts inductively at first using NVivo 12. The data were further analysed using the framework from The Domestication of Technology Model (DTM).23–25 This has been developed specifically to consider the adoption of technology in the home setting and related well to the first level of analysis undertaken in our study. DTM was chosen due to a focus on technology adoption within the domestic setting and the fact that it related well to the initial process of inductive coding and emerging themes. DTM is used to describe and analyse the processes of acceptance, rejection and use. Users are seen as social entities and the model aims to provide a framework for understanding how technology innovations change, and are changed, by their social contexts. The specific dimensions of the theory are found in box 4. Coded data were mapped against the four dimensions of the DTM and grouped into one of the four dimensions, thus the results will be reported accordingly.
Ethical approval
Ethical approval was obtained via The University of Manchester's ethics committee.
Results
Participant characteristics: The final sample (Table 1) includes 13 PWMCCI and their carers (a total of 25 participants 3 ). Five PWMCCI due to dementia and their carers were recruited via our partner care organisation and eight via advertisements circulated in the community and/or from direct approach by SCS over the phone via the Join Dementia Research website. 26
Participant characteristics.

1 = Not confident at all, 2 = not very confident, 3 = neither, 4 = fairly confident and 5 = Very confident.
Withdrew from the study – ID 02 and 12 withdrew after the initial training and try out phase. ID03 withdrew after the first interview.
PWMCCI had a mean age of 78 years (range 64–96), 5 (39%) were female, and had a mean length of time of diagnosis of 2.9 years. From a social/domestic perspective, all PWMCCI except one lived in their own homes and 7 (54%) PWMCCI lived with a partner, 5 (38%) lived alone and one with another family member (adult daughter). Carers had a mean age of 58, 12 (92%) were female and reported an average confidence of technology use of 4.25 (out of a maximum of 5), all reported owning and using both a smartphone and tablet.
Appropriation: reasons for taking part – motivations, expectations and hesitations about the app
Initial interviews with all the participants revealed a key reason for deciding to take part was based on altruistic motives that research, in general, was a ‘good thing’ and that this research could help advance knowledge about interventions to help others with the condition: I just felt I’d like to find out some more and I’d like, you know, what we know of it to hopefully help other people in the future. (ID08_female carer_initial interview) Well the idea of having some app that might prompt [PWMCCI name] memory was something that interested us. His long term memory is fine, it's literally just his short term memory. So things that I thought might be useful, when he's talking to his son. He's got to then remember the wife's name and the kids’ names and ask questions about people. And I think that's what he finds more difficult. (ID10_ female carer_initial interview)
The participant below was looking towards the future and expected that support for his communication needs would increase and that this app might help with some of these issues: And I get frustrated now in struggling to remember the things that [carer-wife] would be interested in, about…because she wants to know and how is [friend] and how's his wife, et cetera, and I struggle to be able to remember those things. And that extends itself to other areas, really, where I just don’t have the information which I picked up at the start of our conversation. That's gone. So that's a bit frustrating and that, when I saw what you were planning to do, I thought this is for me. You know, this is exactly what I’m hoping is going to be coming up over the years to help. And this would absolutely be one of helping. (ID11_male PWMCCI_initial interview)
The importance of staying connected with family and friends was highlighted by several carers and the expectations that an app that could be tailored to meet these needs was a driver for participation: My father has challenges with his dementia, in that simple things, particularly communication is difficult. So, his short-term memory is very limited. And he used to communicate quite regularly with his grandchildren, and his great grandchildren, and me, via the likes of Facetime, but that sometimes gets a bit confusing…So, something like the app that is supposed to be on there that somehow or other is designed with people with these kind of challenges would be extremely useful. (ID12_male carer_initial interview)
Finally, some hoped that the HMN app could act as an organisational device to aid in care and other daily tasks: [I’m hoping it will] bring order to our lives. At the moment, [carer_wife] has to chase me around, you know. If we had something where we could synchronize it between us, between, you know, between ourselves, then it would greatly aid our lives. (ID07_male PWMCCI_initial interview)
It was difficult to ascertain with certainty whether some of the PWMCCI themselves had clear ideas as to how the HMN App could potentially support them and for some, this was related to their lack of familiarity with smart technology in general. These participants explained that their family could see the benefit of them being more digitally enabled and this was a driver for their initial interest in study participation: So I know this is something my daughters have been asking me to do for ages, because they think they can communicate with me better than just a telephone call. So the daughters will be thrilled about this. Quite frankly I’m terrified of it. (ID02_female PWMCCI_initial interview)
However, the apparent socially derived motivation to adopt technology for these users, did not lead to actual participation beyond the training stage of the study, and in the case of the woman below, the attempts to learn how to use both the touchscreen tablet technology and the app caused considerable anxiety and brought the limitations due to their dementia to the fore. This resulted in eventual drop-out. The formal carer recounted: After I left the tablet with [PWMCCI], she was getting upset as she tried to use it but was not able to remember how to turn [one and use] the tablet. She kept getting upset and was speaking to the carers that she does not want to continue ‘this’ as it only makes her feel incompetent. (ID02_male carer_initial interview)
A small number of participants expressed hesitation around the usefulness of a technological intervention at the start of the study. Some simply expressed apprehension about technology itself as a solution and others doubted whether they or those they cared for had the capacity/capability to learn new technology and the role that disease progression would have on learning: I’m a very slow learner. When I was a social worker, they decided we needed to use phones, that was a big thing for me moving into using phones, even, but I do try, I’m not brilliant at this technology thing. (ID05_female PWMCCI_initial interview)
What I thought was, knowing the state of my memory, whatever he tells me – and he's been very good, he's patient with me – I will forget. (ID02_female PWMCCI_initial interview)
Objectification: determining what the technology is used for
Participants received an initial introduction to the HMN app via the training and then provided their views about the potential usefulness of the app for their own situation.
The majority of participants, in particular the carers, expressed positive initial impressions about the HMN app's usability after their brief training. They also thought it offered potential for routine use in some aspect(s) of their lives currently: I think it's easy to use, it's very nice, and I think once we get into it now, I will enjoy using it with him. I think it's going to be a joint project, but I think it will help me too with lots of things; I’ve so much to remember that it will help me as well…. I’m hoping that it will… I can’t really comment much further until I’ve sort of built it into our routine if I can really, you know. (ID08_female informal carer_step 2 follow-up interview)
You see, like I could probably think, like the one tablet that [PWMCCI], say I go to the shop, he has to take a tablet after his lunch, right, after dinner? It's only an aspirin, but it's important, this aspirin is important. And it's a one that he forgets to take. So maybe I could say…remind [PWMCCI] at half past 12 to take his tablet? And he would. So, that's where it would be good. So yeah, something like that on an app would be good, like a prompter, you know? (ID13_female informal carer_ Step 2 follow-up interview)
I Well, her singing on a Wednesday is at eight o’clock, so I set the computer up for her before I go at quarter past seven. But, it's quite a long time between quarter past seven and eight o’clock and, you know, if there was something that could prompt her to remind her that at five to eight, don’t forget to make sure it's clicked on. (ID01_formal carer_initial interview)
Participants also envisaged that the app could aid cognition and help maintain independence for the PWMCCI and consequently potentially reduce the cognitive and/or task-related aspects of care work. There were examples of informal carers becoming visibly upset during the interviews when talking about issues associated with their caregiving work and a lack of respite from it. For some informal carers, HMN appeared to offer hope of respite from certain aspects of their care work, particularly the need to repeat instructions for task-related activities and/or the day's planned activities due to PWMCCI's memory impairment: I think that diary part will be very good, and the one that we were looking at that he liked was My Day, and I think rather than…because he will ask me the same question many times over and he liked the idea that he could read his day and that it sort of said it to him, so he was happy with that. (ID08_female informal carer_Step 2 follow-up interview)
I filled in the diary, so…because every day it's like, what are we doing today? Right. And then I tell him and we just walk to the car and he still…then it's where are we going? But I thought if I could have the day out on a tablet and just keep giving it to him so he could read where he was going. So the diary I think might work. (ID10_female informal carer_step 2 follow-up interview)
For other PWMCCIs HMN did not appear to meet their care needs and/or offer added value to their existing strategies or technologies which were seen to provide successful solutions. Moreover, they expressed that learning and adapting to a new technology for managing their needs required significant effort: I just couldn’t see how it would apply to my life and it seemed time consuming. I thought I’d just…I’d rather just put it on the calendar and look it up there instead of opening things and so on. I looked around a bit and looked at the tablet, but I just couldn’t see any…how it would enhance my life. (ID09_female PWMCCI_ step 2 follow-up interview)
Participants discussed how, in many cases, current technology use was already fulfilling areas that HMN could help with such as reminding PWMCCIs of medication use and other daily activities/tasks: She's [already] got a tablet, she's got her tablet on the dining room table, that gives out prompts if she, like, have you had enough to drink, have you taken your morning medication? I don’t know what sort of tablets she takes but it's obviously set up, it's been set up by one of her daughters, so on the days we come it says, [name] carer day, have you taken your morning medication? Have you got your phone by you, have you…? And it lists up various prompts. (ID02_female carer_initial interview)
Some preferred low-tech solutions which were also seen as being sufficient for their needs, easy to use and more ‘tangible’ than technology: You know, I’ve got masses of post-its, here, and those are for me, because as I say, my memory is failing. It's not, I don’t know which is worse, but between us we remember things, but a lot of it gets put on post-its. And passing those onto somebody else, rather than just scrambling around on the phone somewhere outside. Pick it up, take it out to the milk woman, or whatever, you know. This concrete thing. (ID06_female informal carer_final interview)
Despite initial indications/hopes around appropriation, two cases (ID12 and ID 02) dropped out after the HMN training. ID12's carer felt that he could not see how the PWMCCI could benefit after they had examined the features in more detail: Even though he [PWMCCI] could understand how to use the app – I can’t see him being motivated to so do. That is what would he gain by using it – I struggle to see the gains and believe that he wouldn’t be motivated to pick it up. (ID12_male informal carer_step 2 follow-up interview)
Effectively, incomplete objectification led to a lack of motivation to use HMN for a minority of participants. Furthermore, issues relating to the PWMCCI's increasingly impaired memory and other health conditions made interactions with the tablet technology and HMN itself difficult and precluded uptake. As highlighted previously ID02 (PWMCCI) had difficulty turning on the tablet and this frustrated her greatly because she previously held a working role where she trained others on technology and technology use was routine. According to her carer, she discontinued engagement with the study because it made her feel ‘incompetent’. These barriers are not specific to HMN and would have likely occurred with other similar software using existing hardware.
Incorporation: practical hands-on use and maintaining use
The final group interviews were conducted after participants utilised the tablet for several weeks or months, and therefore had practical hands-on use of the HMN app over a period of time. We extended this construct with the addition of ‘usefulness’ in order to capture how participants continued to evaluate the system as it became more or less integral to their daily lives.
The process of incorporation was influenced by participants’ attitudes to, preferences for and competencies in using digital technologies. Incorporation did not happen easily due to the complex interaction between these factors.
a. Adopting and interacting with Technology.
All carers owned and were regular users of various smart technologies (see Table 1). They saw themselves as confident users of technology for everyday tasks such as banking, shopping and making online health care appointments. However, they recognised the technology challenges faced by the people they cared for. Comments indicated that they viewed IT technology as difficult to navigate which would then make it challenging to use a new app. This was in part related to the speed at which increased memory impairment was occurring: My husband, I mean, he was certainly the technical buff in this household, and always had been, because that was his work. But, sadly, the Alzheimer's, you know, his Alzheimer's actually affected his sort of visual, spatial abilities to do things. So he really struggles with all technology, now. And I think we were certainly attracted to something that would use, possibly an IT type solution, maybe to support us, and he got very, well we both got very excited about that. And I think, I don’t think it's anything to do with the App itself, probably, because [PWMCCI] struggles to switch on his computer, he has trouble to switch on the iPad. (ID11_female carer_final interview)
I think it's got slightly, you know, I think it takes her longer to do things, and it's, she forgets things more easily. (ID01_female carer_final interview)
Other health conditions (e.g. arthritic hands) and sensory impairments also hindered PWMCCI's ability to engage with technology and caused difficulties in operating certain technological features: Facetime was the way we did it [communicating whilst abroad]. Problem number one, he didn’t hear it [partial deafness]. It's not that loud, to be honest, it's not his fault. (ID12_male carer_final interview)
There's also an issue of he takes his hearing aids out when he's relaxing, and then so some sort of alert went off with the thing, he might not even hear it. (ID07_female carer_final interview).
b. Adopting and interacting with the App.
The next issue surrounded the usability of HMN itself, with many users expressing limitations and difficulties with HMN compared to technology that they were already familiar with and used for caring-related tasks. Carers and those with high cognitive abilities wanted a higher level of functionality than the current iteration of the app: But I mean, looking at it, the app itself, if [PWMCCI's] condition got worse, which it can do over the years, the App would not be of any use to me. I wouldn’t be able to get into it quick enough, like I could my phone, or my own tablet. To me, it's not got the speed, for me. (ID07_female carer_final interview) You put an appointment in, okay, but it doesn’t cross-link to the Contacts. I can’t put more than one bit of information in and the biggest part is that it doesn’t go to My Week [diary feature within App]. (ID07_male PWMCCI_final interview) But I think the functionality around the diary, and the scheduling, is perhaps not as useful to us as I would have hoped it might have been. Simply because we lose [sight of] that information, it's not backed up and stored anywhere [visible within the app]? (ID11_female carer_final interview) I have a diary on my phone which I’m used to, so not for me, personally, no. No. I could see it maybe if PWMCCI was in permanent care or something like that, that people could put reminders in for medication and stuff like that. But for me, personally, it's kind of on my phone, that, already. (ID13_female carer_final interview)
Usefulness
Reflections on the usefulness or potential usefulness of the app were often set within the context of barriers to the use of technology in general, as well as strategies they had already developed in their daily lives to cope with memory impairment. These comments were derived from the accounts of two regular users, and eight irregular users of the app.
For some PWMCCIs, their impaired memory was a barrier now and potentially in the future. Even for the two regular users of HMN, carers doubted whether long-term use could be accomplished as their cognitive abilities declined: I don’t think it's anything to do with the app itself, probably, because [PWMCCI] struggles to switch on his computer, he has trouble to switch on the iPad. And then once he's actually switched it on…he has forgotten where to go next. Which is absolutely devastating for him, because knows that, you know, roll back three or four years and he would have been the one teaching me what to do, and showing me how to operate the technology. But we’ve stuck with it, because there are aspects of the app that I think have, really, have been very useful to us. (ID11_female carer_final interview) I was duplicating stuff, and sort of, my mother-in-law's first impression was, well this isn’t going to add anything to my life, I’ve now just got to duplicate everything here, that I’ve already got on bits of paper elsewhere in my life. (ID09_female carer_final interview)
Despite many carers feeling that HMN had potential, this was not realised due to the perceived time required to invest in making HMN a workable solution for their everyday caring needs. In essence, the caring burden seemingly placed a barrier on the time to learn and use the app in the way that it was intended. These carers experienced tension between facilitating independence for the PWMCCI and a need to accomplish daily activities that may once have been shared or delegated to the PWMCCI but who were now less able to complete those tasks: And, you know, on a good day I can be okay at it and on a bad day things aren’t good. Because I can feel myself just… You know, I’ve got so much I need to get done and I’ve asked for one job and it's not been done, so… But I know that it will get done no better if I get more uptight about it. I might just as well leave it and come back to it later. (ID11_female informal carer_final interview) For a dementia carer such as myself I think the App would be of good value. However, in my opinion it would really involve quite an amount of input by the carer in the first instance – e/g diary / photos / procedures for daily tasks etc. – especially as you can’t import such data as it doesn’t interface with cloud based diaries or photo albums / to do lists etc. (ID12_male carer_step 2 follow-up interview) Well, I find that I’m putting things in, but then, he's forgotten about them anyway, you know, so, it was sort of, I felt, whereas I can go and get a photo album, or putting some music on. I was creating something that was an extra chore for me, and then, without me actually being there physically to take him to and show him, it was no good to him. (ID08_female carer_final interview) I think once I’ve actually got a lot of… I haven’t had a lot of time. I think I’ve done five boxes [on the App]. Like I say, I’ve not had a lot of time. (ID13_female carer_step 2 follow-up interview)
Conversion: intent to continue using app
Two participant pairs (ID11 and ID06) out of the 10 that completed the study, expressed a desire to continue to use HMN beyond the end of the study, demonstrating potential usefulness for this user group. These two participants were also the same people that had regularly chosen to use certain features of the App. They both used the app as a repository for various types of information. ID06 (PWMCCI) had collated and continued to add information into HMN in terms of medications, key health professional contacts and things about his personhood so that it could be accessed by others in his social support network. This participant valued the fact that everything was in one place and could easily be accessed in case of acute illness in the short-term or in the longer-term progression of his cognitive decline. This participant's wife also felt reassured that the banking of such information within HMN was an avenue to ‘future proof and protect the self’: Because what it's done for him, when he first started doing it, it addressed some of the concerns that we had. I suggested to him to keep a journal, …but by keeping a journal, he himself can reflect on how he's changed, and this has changed, and what are the results when we look back….he downloads all his medications and everything, and uploads his personal details, and he does all that. And that was because he starts forgetting, well we’ve got a massive lot of files here with everything on paper, and it's also on computer. So if he starts to sort of come out of this, it’ll be in one place, and that's a valuable thing. And he regards the app as an assurance. (ID06_female carer_final interview) I think…populating some re-information in a place which at the moment [PWMCCI] accesses. Just as an aide memoire, so that if somebody asks you something unexpected, because you can prep for a meeting with friends and you can prep for other occasions, but it's the unexpected that sometimes is a bit something like one of the boxes, which is headed up approximately, might just give you, I don’t know, three or four items that might be useful to start the conversation. And then that gives you some breathing space to think oh, right, okay, yeah, I’ve told you those four things. And by the time we’ve chatted about those I’ve relaxed and I’m in the flow and I can think of more things if that's what you chose to develop. (ID11_male PWMCCI_final interview)
As outlined above, his wife played an important role in populating the app with relevant information to maintain his independence and to continue his valued activities: I think it would be fair to say that we need to do the populating together. Ideally it would be lovely if you could access that quickly enough so that it wasn’t a cumbersome bit of kit. But at the moment we populate it together, but it's there as the aide memoire. (ID11_female carer_final interview)
The remaining eight participant pairs had stopped using the App by the time of the follow-up interview. Although comments also indicated the kind of adaptations that would improve the function of the app, were they to be implemented in a new version, and could lead to further conversion in the future.
To be honest if they changed that diary, if they changed the appointments and they changed the scheduler, that would just be mammoth. I think that would take it from being something that's very useful and an adjunct to something that was…it could almost become a real necessary tool, a bit of kit to have. (ID11_female carer_final interview)
Discussion
Our findings identified considerable variation in attitudes to and capabilities of people living with dementia to (a) adopt a new mobile app and (b) sustain use longer term. The majority of participants in our study investigating adoption and use of the app, Hear Me Now, expressed a view that participation in the study could generate benefits not only for them personally but also for others with dementia. However, participants’ expectation of personal gains were largely not realised and the technology was not incorporated into routine use in the majority of cases. Two participants were however regular users of the app and others indicated a potential desire to use the app if adaptations were made.
The participants identified a number of issues with adopting the app. We discuss three significant topics raised in the study and relate these to previous research. A summary is provided in Table 2:
Attitudes to, familiarity with and age-related factors affecting smart technology use App design and function Complexities of dementia (progression and impact on learning) and caring context
Summary of findings for mHealth adoption for people living with dementia and/or their carers.

Attitudes to, familiarity with and age-related factors affecting smart technology use
The study identified significant barriers in particular for PWMCCI, relating to using smart technology. These barriers were linked to attitudes to technology, users’ age and other condition-related issues (e.g. dexterity, deafness) that could adversely affect how people manage smart technology.
The most obvious limitation reported by some of our participants related to PWMCCIs attitudes to and familiarity with smart/app technology. For some, the use of touch screens and variability in interactional capabilities with technology in general (due to other health conditions, e.g. deafness) was a significant barrier. Over half of PWMCCIs did not own a smartphone and were therefore unfamiliar with the hardware despite training and support. Such a lack of familiarity led to initial attitudinal barriers which significantly impacted upon their views towards the app both prior to and post-app training. Whilst initial attitudinal barriers are not necessarily a barrier to technology adoption for PWMICC, 27 poor digital literacy was clearly a large factor for some users and one which is highlighted in a number of studies as adversely affecting use of a health app by those with dementia. 28 However, other PWMCCI were familiar and capable of interacting independently with the tablet illustrating the varability of needs that mHealth must consider. Clearly future App users are likely to be more familiar with the technology, as suggested by the accounts of carers who were typically younger in age (average age of 58 vs. 78) and rated themselves as confident users of technology. Nevertheless, we were unable to determine whether lack of familiarity was the key barrier or the complexity of seeing and using touchscreens was instrinsically difficult for older people, given changes in sensory processing and co-ordination. Such issues are likely to pervade given human ageing processes and technology design needs to acknowledge and accommodate this.
App design and function
Carers depicted themselves as regular users of smart technology, they understood the features and intended functions of the HMN app which were initially viewed as desirable and positively aligned with aspects of their caregiving needs. They identified areas as potentially most beneficial in terms of both usability and usefulness, relating to memory prompting via the scheduling of activities and sequencing of daily activities to maintain PWMCCI independence and potentially alleviate some caregiver burden. The multi-media and multi-communication options were positively viewed as a way of facilitating communication between carer and PWMCCI. However, despite the fact that HMN is a customisable app, they identified various usability issues with specific features and areas for improvement within those specific features, in particular the diary function. Accounts suggested that these issues to be addressed in a subsequent re-design of the app that it would positively impact their uptake of the app. These design-related issues highlight the important role of co-design and its impact on the interaction and adoption of mHealth. 29 For the small number of users that did continue to use HMN in its current form, the app appeared to fulfil individual needs that they valued and it aligned with their positive views of how a technological solution might help them. In particular, these needs were: support for engaging in valued leisure activities, maintaining social interactions and information for current and future use. In these cases, HMN supported the PWMCCI's agency in helping them carry out activities unassisted, and thus maintain independence and personhood. 30
Complexities of dementia (progression and impact on learning) and caring context
The challenge of the progressive nature of dementia presents another significant barrier to the adoption of technological solutions for this user group. Some carers expressed that even since their involvement in the study they had noticed a decline in the cognitive abilities of those that they cared for. Despite the ability to personalise HMN, the technology effectively became obsolete as the PWMCCI's ability to interact with technology, comprehend and retain any recently acquired information (from any source) declined. For those that had experienced either little cognitive decline since initial diagnosis or remained stable during the study period, HMN remained relevant. This was illustrated by the two participants who incorporated and converted HMN into aspects of their daily lives. This supports the suggestion that technology designed for PWMCCI due to dementia should be introduced early in the disease timeline as possible. 28
With regards to carers as the potential key users of the app, comments from a number participants indicated that HMN did not, in its current form, fit with existing strategies they had developed to cope with caring-related tasks or existing technologies they used to support themselves or those that they cared for. It appeared that some people weighed up the perceived requirement to invest time to learn and interact with the HMN app within the context of their daily burden of caregiving these caregiving demands formed a barrier to adoption. Caregiver burden can be defined as the strain or load borne by a person who cares for a chronically ill, disabled, or elderly family member. 31 Ultimately this burden meant that some of the informal carers (who formed the majority of our sample) did not feel that they had the capacity to continue to engage with the app beyond an initial try out. The day-to-day needs of caregiving were paramount and took priority over using the app. This emerged despite the expressed need by carers for respite and the potential the HMN may have offered in relation to alleviating some aspects of their care work by supporting the PWMCCI. In effect, the app was seen as another form of work that they were simply unable to accommodate.
Formal carers expressed similar constraints and despite the study design allowing for dedicated app support time, organisational factors such as staff shortages and the strain of caring during COVID-19 placed further barriers to the immediate and long-term adoption of the technology. As mentioned earlier, the effect of caregiver burden may have also shaped heightened expectations of what the app may be able to offer them beyond what could realistically be expected of an app. Managing these expectations in terms of how mHealth is positioned within a caregiving context may also aid our understanding of mHealth adoption.
Current research examining the potential of technology and older people has noted that little research has considered the adoption, scalability and cost-effectiveness of technology. 32 Furthermore, involvement of PWD and carers in all stages of ICT development remains limited. Knapp and Wittenberg 32 conclude that a number of technologies are promising and that adapting existing commercial solutions for people with mild dementia, and greater developmental involvement of users could yield positive results. Technology should be deployed within context, and the preservation of personhood, quality of life and well-being of both the PWMCCI and carer have to be key drivers. Our approach provided in-depth qualitative data investigating readiness to adopt apps from a small cohort of PWD and their formal and informal carers who varied substantially regarding lifestyle, background and technology literacy. Our results indicated the positive potential of technology, particularly for carer use and in the earliest stages of dementia, but also revealed the challenges that technology presents people living with dementia. Whilst, the study underlined the importance of involving PWD in the design of resources, it emphasised how problematic this can be, given the complexity of the condition.
Strength and limitations
We used a participatory approach to design the study, but this had to be reconceived due to the restrictions that COVID-19 placed on the process of co-design and data collection. Our response to the COVID restrictions however was to work closely with a care organisation and PWMCCI and their caregivers to design and to re-design our study within the limitations of a pandemic. The design reflected feedback from our partners at each stage and collected rich data from successive in-depth interviews conducted remotely, to understand the varied and complex issues around the usability, usefulness, transferability of HMN and identify any adaptations to the existing mHealth app to support PWMCCI due to dementia and/or their carers. By involving users in the development and testing of a mHealth technology and using a theory that places a focus on the domestic context, we have highlighted some of complexities that need to be taken into account when attempting to tailor and implement such digital solutions. The findings also highlight some of the key considerations for use of AT to support people living with cognitive impairment and dementia. The findings have implications for designers, policymakers, practitioners and researchers. In particular, there is a need to consider wider barriers to digital inclusion for this group such as entrenched attitudes to technology, and the anticipation of deterioration over time that is expected for this group. Additionally, there is a need to consider the support needs of carers as well as people living with such conditions as well as user preferences for design of specific features within apps such as HMN. Finally, the use of an appropriate theoretical model aided our analysis and understanding of the process of adoption and integration within context.
Our study, as with other research, had to be paused due to COVID-19. We had to re-design our study to take into account multiple factors including the extreme vulnerability of the participants. Our final design meant that we continued with a version of the study that would still meet our aims but satisfied the need to safeguard our participants and adjust for their digital knowledge and skills in various contexts. We were, however, unable to do the intended re-design work which would have impacted upon the app design aspects of our results in particular, but we instead collated the feedback on areas where the design of HMN could be improved for this user group and Maldaba are now able to use this data for future work on the app. The move to remote methods of data collection meant that we were unable to undertake the planned observational work that may have provided further insights (e.g. into touchscreen issues). Remote data collection did however offer the advantage of flexible engagement, in particular, with professional carers who were extremely time pressured. The pause also allowed us to continue to build the relationships between the app providers and researchers and with care organisation partners to inform our design and data collection work. We did have some study dropouts, but the reasons for dropout were informative and added to the narrative of this paper. Overall, we feel our approach, demonstrates the importance of investing time into understanding how different types of users may or may not adopt/incorporate digital-health technology into their daily lives.
Conclusions
Using mHealth to support PWMCCI due to dementia and/or their carers may have potential to enhance communication, safety and wellbeing. However, but for that to be realised there is a need to understand the complexities of the target user(s) varied and changing needs due to the nature of such a progressive condition and reflect this in the technology design. mHealth will need to become more sophisticated to offer flexible and personalised support that changes over time. Disease progression places a potentially unique constraint around the window of opportunity for mHealth for people living with dementia in its current and any future forms. The potential for mHealth to meet caregiver needs however is an area that has received less attention and could have great potential and should be explored further.
Footnotes
Acknowledgments
We would like to thank all the people living with dementia and their carers for their time and contribution to this research. We would also like to thank the care organisation Belong for their help in setting up the study and their staff's contributions throughout. The COVID-19 pandemic made this study very challenging for all involved and we are extremely grateful that despite the pandemic and the issues it created for those most vulnerable, we were still able to complete the work on an ever growing topic of importance. Finally, we thank the providers Maldaba for their role in partnering with us to help advance our understanding around mHealth requirements for people living with dementia and their carers.
Contributorship
SCS, CS and BNO all conceived the initial idea for the study. SCS, CS, KD, BNO, LG and HJ all contributed to the design and conduct of the study. SCS, CS and BNO conducted most of the analysis and received feedback from LG and HJ throughout. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
Authors SCS, BNO, CS and KD declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. HJ and LG are the app developers and therefore hold a financial interest.
Disclaimer
The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Institute for Health and Care Research (NIHR) Greater Manchester Patient Safety Translational Research Centre (award number: PSTRC-2016-003).
Guarantor
CS.