
Abstract
Objective
Neck-specific exercises for individuals with chronic whiplash-associated disorders (WAD) have shown promising results, but there is also a need for more efficient and flexible ways of rehabilitation, such as use of digital health tools. Understanding physiotherapists’ experiences of an internet-based tool may help to improve digital tools within physiotherapy. The purpose of this study was to describe how physiotherapists’ experience an internet-based neck-specific exercise program for patients with chronic WAD.
Methods
This study has a qualitative design. Focus group discussions were held with physiotherapists who have been treating patients with chronic WAD, using an internet-based neck-specific exercises program in a randomized controlled multi-center trial in south and central Sweden. Three focus groups were held with three participants in each group. Phenomenography was applied as a research approach for data analysis.
Results
One main category was identified as “internet-based program as a complement to regular rehabilitation,” with five descriptive sub-categories: (a) support in patient work; (b) usefulness based on a patient's prerequisites and preferences; (c) physiotherapist and patient interaction; (d) increasing efficiency in rehabilitation; and (e) enabling patient participation, autonomy and self-management.
Conclusions
From a physiotherapy perspective, an internet-based program could work as a method of complementary support to the standard rehabilitation treatment for patients with chronic WAD, as long as it is interactive and adjustable to the individual. The internet-based program could lead to increased autonomy and self-efficacy, and save resources and time for physiotherapists and patients. Further, more research is needed to strengthen these digital tools within the healthcare system.
Keywords
Introduction
Globally, neck pain continues to be one of the leading causes of years lived with disability. 1 A common cause of neck pain is attributed to whiplash injury from a car accident. 2 As many as 50% of those injured will report continued pain and disability after 6 months (chronic whiplash-associated disorders, WAD).3–6 Individuals with WAD may have a worse prognosis than those with non-specific neck pain, having higher levels of pain and disability. 7 There is growing evidence on the efficacy of neck-specific exercises (NSE) for individuals with chronic neck pain and WAD,8,9 but there is also an evident need for more efficient and flexible ways of distributing rehabilitation than the traditional face-to-face sessions. 9 The World Health Organization (WHO) has recently called for the development of evidence-based digital health interventions. 10 Within physiotherapy, tele-rehabilitation has shown promising results, comparable with conventional face-to-face rehabilitation approaches for individuals with musculoskeletal, cardiorespiratory and neurological conditions,11,12 but there was a heterogeneity of the clinical trials included in these reviews, and better quality trials are needed to move digital health interventions forward. 12 For individuals with acute WAD, Bring et al. found similar effectiveness of a behavior change program delivered face-to-face or on the internet, 13 but there is scarce knowledge on chronic WAD. To address the lack of studies on individuals with chronic WAD, Peolsson et al. conducted a randomized controlled trial (RCT) that compared NSE delivered over the internet (NSEIT) combined with four physiotherapy visits, with NSE over 24 physiotherapy visits. 8 NSEIT was found to be non-inferior to NSE, with improvements over time and sustained clinically important changes in pain and disability. 14 These findings are promising for individuals with chronic WAD, but, as emphasized as a research gap by WHO, the knowledge and attitude of patients and healthcare professionals and their behavior toward digital health are also important to unravel. 10 Understanding physiotherapists’ experiences of treating patients with chronic WAD supported by an internet-based tool may help to improve internet-based programs within physiotherapy.
The aim of this study was to describe how physiotherapists’ experience internet-based neck-specific rehabilitation for patients with chronic WAD.
Methods
Design
This is a qualitative study using data from focus group discussions with physiotherapists. Focus group discussions were chosen because the interaction facilitates the participants’ ability to speak more freely, to express and clarify their beliefs, attitudes, and experiences, and to uncover more or less unconscious beliefs and understandings, which may be more difficult to achieve through individual interviews. 15 Phenomenography was applied as a method of data analysis to acquire knowledge about the qualitatively different ways in which a phenomenon is experienced, conceptualized, understood, perceived and apprehended.16,17
Context and participants
This study is part of a larger research project with a multi-center RCT, aiming to compare two different ways of distributing neck-specific rehabilitation to individuals with chronic WAD in primary health care in Sweden. 8 After written and oral informed consent, 140 individuals with chronic neck problems corresponding to WAD grades 2–3 18 verified by clinical examination, were included in the RCT and randomized into one of two groups. Both groups received the same NSE for 12 weeks. Exercises were chosen from a clear and written frame and included exercises for the deep neck muscles, continuing with the endurance, training of neck and shoulder muscles. Part 1: Activation by supine isometric exercises 5 repetitions 5 times a day with progression to next part. Part 2: Progression from supine to sitting isometric exercises 3 × 10, 3 times a day. Part 3: Endurance training, starting with 5–10 repetitions and progression to 3 × 20 if tolerated, 3 times a week. Training of neck and shoulder muscles were included, 3 × 10, 3 times a week. The exercises are individually adjusted according to the individual's physical conditions and progressively increased in severity and dose. These exercises have been used with good results in a previous RCT, where the program is described more in detail.19,20 The first visit to the physiotherapist take approximately 60 minutes and the others 30 minutes. Group A received internet-based support in combination with four visits to the physiotherapist while group B received two visits/week to the physiotherapist but without the internet-based support. 8 This internet-based support consisted of a digital platform with information provided in text, pictures and videos about pain, pain management, WAD, neck muscle function, how to perform the NSE, as well as an opportunity to report daily exercises and receive SMS reminders to do the exercises. No tools or special aids were provided for the internet-based support.
Physiotherapists who had experienced at least one patient randomized to the internet-based support group were eligible to participate in this focus group study. To facilitate group discussions, we strived for a variation of physiotherapists regarding age, gender, length of work experience, working in public and private primary care centers and different regions in south and central Sweden. Eligible physiotherapists were approached by e-mail with information of the study, and interested physiotherapists were given extended written and oral information. Nine physiotherapists chose to participate, and were strategically distributed into one of the focus groups to reach a variation of experiences (different regions, public/private clinic, age, etc.). Three focus group discussions were held with three physiotherapists in each group. Participant characteristics are shown in Table 1.
Overview of the participating physiotherapists in the focus group discussions.
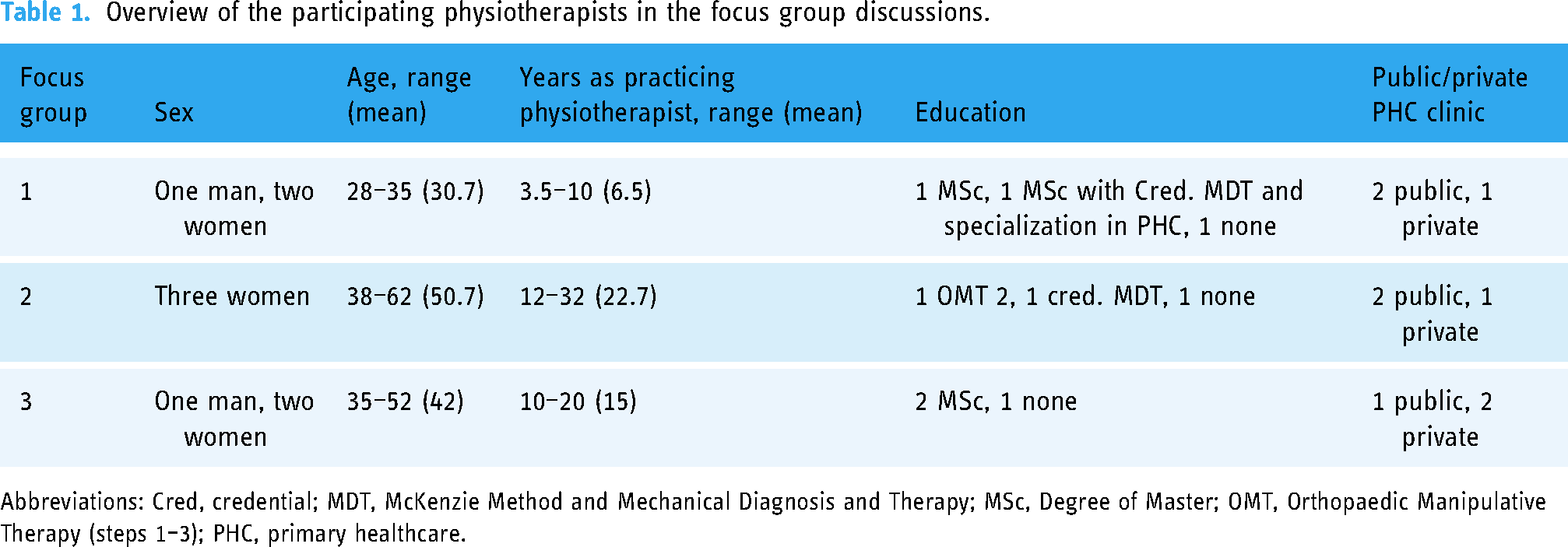
Abbreviations: Cred, credential; MDT, McKenzie Method and Mechanical Diagnosis and Therapy; MSc, Degree of Master; OMT, Orthopaedic Manipulative Therapy (steps 1–3); PHC, primary healthcare.
Data collection
A questioning route for focus group discussions outlined by Krueger and Casey was developed, starting with an opening question, “What are your previous experiences of working with digital health interventions as a physiotherapist?,” followed by introductory, transition, key and ending questions. 15 Questions were inspired by previous research within the field and discussions within the research group. The key questions focused on the physiotherapists’ experiences of treating patients who had been participating in the internet-based neck-specific rehabilitation program for chronic WAD, its applicability, benefits and weaknesses. The interview guide was pilot-tested in one individual interview and in one group discussion, which resulted in minor revisions to clarify the questions and include two additional questions. These pilot interviews were not analyzed. The physiotherapists were encouraged to speak freely and from their experiences and perceptions. Follow-up questions and probes were used to develop and deepen the answers. 15 The focus group discussions were conducted between January and May 2020, with one author (FG) as moderator. Another author participated as observer (AH or ENS), taking field notes and asking additional and clarifying questions at the end of the discussion when needed. The interviewers were not involved in the design of the ongoing RCT. To facilitate participation and reduce time and costs for travel, the group discussions were performed digitally as a video conference meeting with Zoom, where the informants could see each other. This is a new resource-efficient approach to conducting focus group discussions, which enables group interaction and preserving depth and breadth. 21 A time was set for the focus group discussions in agreement with the physiotherapists. Oral and written informed consent was obtained before each discussion. The discussions lasted between 51 and 69 minutes and were digitally recorded. The audio files were sent to a professional transcriber contracted for the research project and transcribed verbatim. To ensure confidentiality, the focus group discussions were coded 1, 2, and 3, and the physiotherapists pseudonymized and assigned a code (A–C).
Data analysis
Data was analyzed when all focus group discussions had been conducted. Transcripts were imported into NVivo 12 (QSR International, Melbourne, Australia) to manage and code the data. Phenomenography was used to analyze how physiotherapists experienced the internet-based neck-specific rehabilitation program for patients with chronic WAD.16,17,22 In phenomenographic research, the structural (“what”) and referential (“how”) aspects of the phenomena studied are essential.23,24 Thus, when the interviewed physiotherapists talked about this internet-based program, we were interested in knowing what they talked about and how they talked about it. The analysis followed the consecutive steps described previously 22 (Table 2). Three authors were main analysts (FG, AH, and ENS). In the first step, familiarization, all transcripts were read thoroughly by all three analysts. The condensation was performed by FG. Steps 3–5 were performed by the three authors (FG, AH, and ENS), first independently and then followed by discussions among the authors until agreement was reached on the relationship between codes and categories. Steps 6 and 7 were carried out by the three authors together. There was a constant interplay between the steps in the analysis, and continuous discussions were held by the three authors (FG, AH, and ENS) during the entire analysis.
Analysis procedure according to Dahlgren and Fallsberg. 22

Categories were positioned in an outcome space, consisting of the variations of, and logical relationship between, the descriptive categories. 24 The outcome space is hierarchical, where one main category was on a higher, more abstract level. The descriptive sub-categories were structured horizontally and considered equal in relation to the main category; however, described qualitatively different ways of experiencing the phenomena. The conceptions should be seen as descriptions on the collective level, not as individual qualities.24,25 This systematization of categories has been previously described. 26 Quotations from the participants were used to illustrate and support the descriptive categories.16,27
Ethical considerations
The participants provided written informed consent after receiving both oral and written information about the study, including the voluntary nature of participation, the option to withdraw any time without explanation, and assurance that all collected data would be handled confidentially, and no individual would be identifiable in the results or the quotations. The audio recordings and transcripts were coded and saved on a password-protected server. The code key, transcripts and written consents were stored in a safe locker. All data were accessible only to the research team. Only coded data was discussed among the authors. The participants were informed of the moderator's and observer's professional backgrounds, reasons for interest in the topic, and that the data would be published in a scientific journal. There was no relationship with any of the participants prior to study commencement. All data will be archived in accordance with current legislation and local procedures for at least 10 years after publication. The study followed the ethical principles of the Helsinki Declaration. 28 The Regional Ethical Review Board in Linköping decided that no approval was needed according to the Swedish Act on ethical vetting (approval number 2019-02383).
Results
The main category, “Internet-based program as a complement to regular rehabilitation,” is composed of five sub-categories describing different qualitative ways of experiencing internet-based NSE program for patients with chronic WAD. These comprise: support in patient work; usefulness based on a patient's prerequisites and preferences; physiotherapist and patient interaction; increasing efficiency in rehabilitation; and enabling patient participation, autonomy, and self-management (Table 3). Within in all five categories, the overarching experience of internet-based program, as described in all the focus group discussions, is that the internet-based program should be a complement to regular rehabilitation rather than a single tool.
Categories describing physiotherapists’ experiences of internet-based neck-specific exercise program for patients with WAD.

Support in patient work
The internet-based program was described as a useful tool for patients’ in-between the physiotherapy sessions, allowing them to repeat the NSE by looking at instructional videos and/or photos, read about WAD, fill out the exercise diary, and receive reminders. The internet-based program provided additional support for worried and fear-avoidant patients, or those uncertain about how to perform the exercises correctly. Repetition and feedback were acknowledged as important aspects provided by the internet program. “My experience with whiplash patients is that, when they do these neck-specific exercises, they do not know if they are doing them right or if it feels wrong. And what did he say two weeks ago, or whatever? So this, that they could, at all times, go back and check: how was I (i.e. the patient) supposed to do.” (Informant 1C)
The physiotherapists suggested that increased access to the program would develop it further, especially when including individuals with subacute WAD, as this could prevent longstanding disability.
Usefulness based on a patient's prerequisites and preferences
Patients were perceived has having various prerequisites for assimilating the internet-based rehabilitation. Patients perceived as having the best prerequisites were those who would have chosen an internet-based approach for rehabilitation themselves, as preferences and inner motivation were deemed to be of importance for completing the rehabilitation program. “I really think it can be useful, but only if it’s used in the right way, and by those who really chose it themselves; then it can fulfil its function.” (Informant 2C)
“I primarily think of fear and psychosocial factors that make me think that the patient needs more support.” (Informant 1A)
Physiotherapist and patient interaction
To treat patients with chronic WAD participating in an internet-based rehabilitation necessitated a changed work role and working approach. The physiotherapists described that they acted more as a coach, encouraging and putting trust in the patient's ability to understand the content of the internet-based program. Fewer visits at the clinic meant less control over what the patient is doing and his/her progress, which could be difficult to deal with. “A bit hard to let go of the control [laughter] I normally have, I think” (Informant 3B)
Regardless of the way of distributing physiotherapy, a holistic approach and individualized rehabilitation of high quality of care was emphasized. The physiotherapists requested more interaction within the internet-based program, such as communication via chat, as this was perceived to further strengthen the possibilities to offer individualized support, feedback, and follow-up. “I think it’s positive and an efficient working approach, as long as … you can individualise as well. That’s the most important thing, so we don’t let go of what's important for us physios, because it’s about seeing an entire person, not just giving out protocol.” (Informant 3A)
Increasing efficiency in rehabilitation
The physiotherapists emphasized that internet-based rehabilitation is part of the future, saving time and resources, both for patients and physiotherapists. The accessibility to physiotherapy may improve, as more patients can be treated with support from internet-based programs instead of having to make several visits to the clinic. However, challenges were faced in how to implement the internet-based program in their workflows, and focus clinical time for assessments and those patients who need more support. “Also, we are given increasingly more work tasks as physios, and so it would be good to treat digitally what is possible, so we actually spend more time at the clinic to focus on those who really need assessments and actual hands-on physiotherapy. So this will be way more efficient.” (Informant 1C)
Enabling patient participation, autonomy, and self-management
The support of an internet-based program was described as a way to increase patients’ participation in rehabilitation, their autonomy and self-management. More responsibility was placed on the patients since they had access to information as well as videos and photos of exercises, which they could return to whenever they wanted. The physiotherapists described that this made the patients confident and increased their self-efficacy, which contributed to increased independence. Being confident in self-management places the patient at the center of their rehabilitation process. “From an independence point of view, you can, how shall I say, master your own health problems and some way gain some self-esteem by treating yourself. I think it's also largely a part of not becoming dependent or needing to visit the healthcare centre twice a week to get help; instead, you can take care of yourself in a good way.” (Informant 1A)
Discussion
The aim of this focus group discussion study was to describe how physiotherapists experience an internet-based neck-specific program for patients with chronic WAD. The key findings were that the internet-based program was highly appreciated by the physiotherapists, and could work as a complementary support to the standard rehabilitation treatment for patients with chronic WAD, as long as it is interactive and adjustable to the individual. The internet-based program necessitated a changed work role with the physiotherapists acting more as coaches, which was in line with their willingness to increase patient autonomy and self-management. Rehabilitation that is more efficient would also save resources and time, both for physiotherapists and patients.
The use of an internet-based program as a complement to standard treatment complies with the findings from recent qualitative studies, showing that digital health interventions used in a blended approach complement standard physiotherapy treatment in temporomandibular and vestibular disorders.29,30 The benefits of our internet-based program include providing patients with additional support, extra information, exercise pictures and videos, exercise dairy, reminders, and options for repeated information. These are examples of how digital tools can support the physiotherapy treatment process in patients with WAD, and the novelty of this study. Patients with low adherence to rehabilitation programs could be those who need an internet-based tool the most. In the main RCT, patients were randomized into the internet-based exercise program,8,14 but the physiotherapists emphasized that patients’ prerequisites and preferences should be taken into account when offering NSE. Patients should be able to choose internet-based program and/or clinic-based. One of physiotherapists’ main concerns with digital health, in previous studies as well as in the present study, was the maintenance of personal contact between the physiotherapist and the patient.29,31,32 Lack of personal contact has been described as one of the main barriers for implementing digital health, both for physiotherapists and patients. 29 When developing future internet-based programs, interaction between health care provider and patient is necessary, as it facilitates tailored support to the individual's specific needs. It may also enable identification and treatment of psychosocial factors. In this study, the NSEIT group received four visits to the physiotherapist, as a combination of clinical visits and internet-support had previously been recommended. 33 The physiotherapists in this study described a changed work role and working approach, acting more as coaches. The change was daunting for some, but mostly it was perceived as an important part of empowering the patient and increasing their self-management and self-efficacy. These findings are in line with previously identified enablers for digital health interventions: the opportunity to exercise at one owns pace, space, and place, empowering the patient. 34 The findings indicate that digital tools can be a support in physiotherapy, but not entirely replace the physiotherapist. In the future, physiotherapists may have to prioritize patients, and the use of digital health tools or interventions may be one way to work more efficiently.11,12 Further research is needed to strengthen digital tools within the healthcare system, especially studies on internet-based exercise programs in musculoskeletal physiotherapy. In the near future, the main outcomes of a RCT evaluating NSE with an internet-based will be published and contribute to the knowledge on digital tools. 14 In addition, the patients’ perspective of internet-based exercises for WAD, and how an internet-based program can be implemented in clinical practice, need to be explored in future research.
Methodological considerations
This study has some limitations that need to be considered when interpreting the findings. The sample was deemed to be representative of those physiotherapists who participated in the RCT. 14 The study sample was small, although within the recommendations of a focus group study of at least three groups with three to eight participants in each group. 15 Having fewer participants in the groups might be considered to facilitate interaction, since these FGD were conducted as video conferences. However, we cannot ascertain that including another focus group would not have influenced the results. According to the description of informational power, a smaller sample size may be sufficient if the study aim is narrow, the participants are holding characteristics that are highly specific for the study, the dialogue between the researcher and participants is strong and clear and the analysis explanatory. 35 Nevertheless, nine participants in three focus groups is a small sample size and a study limitation impeding the transferability of the findings. The data analysis followed the steps previously outlined, 22 and with two experienced qualitative researchers having main responsibility. The authors responsible for data collection and analysis were not involved in the design of the RCT. 8 We are aware of our perspectives, all authors being women and physiotherapists with clinical experience of patients with WAD. The checklist for reporting of qualitative studies was used to improve transferability. 36
Conclusion
From a physiotherapy perspective, an internet-based program could work as a complementary support to standard rehabilitation for patients with chronic WAD, as long as it is interactive and adjustable to the individual. The internet-based program necessitated a changed work role, with physiotherapists acting more as coaches, which was in line with their willingness to increase patient autonomy and self-management. Digital tools could lead to more efficient rehabilitation, saving resources and time, both for physiotherapists and patients.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231159181 - Supplemental material for Physiotherapists’ experiences of internet-based neck-specific exercises for patients with chronic whiplash-associated disorders
Supplemental material, sj-docx-1-dhj-10.1177_20552076231159181 for Physiotherapists’ experiences of internet-based neck-specific exercises for patients with chronic whiplash-associated disorders by Emma Nilsing Strid, Frida Gustafson, Anneli Peolsson and Anna Hermansen in Digital Health
Footnotes
Acknowledgments
We would like to express our gratitude to all participating physiotherapists for sharing their experiences and thoughts. We are also grateful to Gunnel Peterson, PhD, for invaluable feedback during the research process.
Contributorship
AP, AH, and ENS designed the study and wrote the ethical application. All authors were involved in developing the interview guide. FG, AH, and ENS were responsible for data collection and data analysis. ENS had main responsibility for drafting the manuscript. All authors have been involved in critically revising the manuscript and have given final approval of the version to be published. Each author participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Regional Ethical Review Board in Linköping decided that no approval was needed according to the Swedish Act on ethical vetting (approval number 2019-02383).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Swedish Research Council (2018-02475), the Medical Research Council of Southeast Sweden, Linköping University, and the county councils of Östergötland and Örebro, Sweden, The Swedish Research Council (grant number 2018-02476).
Guarantor
ENS.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.