
Abstract
Objective
To examine the experience of Italian nurses posted on social media and discover changes, if any, over the waves.
Methods
A mixed methods study reported according to the Good Reporting of a Mixed Methods Study criteria. All narratives (texts, letters and interviews) posted by Italian nurses from February 2020 to May 2020 (first wave) and from October 2020 to May 2021 (second/third wave) on the five most famous Italian professional social media platforms. The data were analysed qualitatively (first wave) and then quantitatively (second/third wave).
Results
A total of 380 narratives (202,626 words, 2510 quotes) were posted in the first wave, and 161 (68,388 words, 835 quotes) in the second/third wave. In the first wave, the following five themes emerged: (a) ‘sharing what is happening within myself’ (891; 35.5%); (b) ‘experiencing unprecedented working conditions’ (749; 29.8%); (c) ‘failing to rehabilitate the image of nurses in society’ (376; 15%); (d) ‘experiencing a deep change’ (253; 10.1%) and (e) ‘do not abandon us’ (241; 9.6%). The same themes and subthemes also emerged in the second/third wave with some significant differences, indicating changes in the lived experience of nurses. Moreover, in the second/third wave, a new theme emerged: ‘experiencing the mixed emotions towards jabs’.
Conclusions
By analysing their posts, Italian nurses continue to face challenges during the COVID-19 pandemic, with changes in their lived experiences across the waves. Governments, nursing associations and health care organizations should consider these changes to design policies to prevent the further loss of nurses.
Introduction
Coronavirus Disease 2019 (COVID-19), which developed in early 2020 around the world, remains a global pandemic issue,1,2 having reached a total of 528,816,317 confirmed cases by 1 June 2022. 3 Although vaccinations have started worldwide, the COVID-19 outbreak continues to spread, leading to high pressures on the health care system. 4 Accordingly, hospital staff (e.g. clinical nurses) is required daily to face challenges and organizational changes to ensure an adequate level of care, resulting in increased physical and mental distress. 5
Several qualitative systematic and scoping reviews have reported the concerns and the vulnerability perceived by nurses.6–11 Overall, studies have highlighted their experiences regarding the poor organizational support, the lived difficulties in wearing personal protective equipment (PPE), the physical symptoms experienced (e.g. insomnia, headache, and fatigue) and the frustration of not being able to read up on the best evidence about COVID-19.6–11 In addition, nurses have reported experiencing psychological exhaustion as fear (e.g. of being infected and infecting their acquaintances), depression, anxiety and feelings of helplessness and uncertainty, as well as post-traumatic and work-related stress disorders.6–11 However, nurses’ perspectives have been documented mainly according to qualitative approaches (e.g. phenomenological and descriptive)6–11 using interviews and focus groups to collect data on lived experiences from the frontline.
On the other side, within the context of the COVID-19 pandemic, social media has become crucial to investigating unpredictable issues narrated spontaneously and openly by nurses on a daily basis as personal and professional communication (e.g. sharing experiences and searching for help). 12 Furthermore, given their nature, content reported on social media during COVID-19 offers the opportunity to capture multi-dimensional facets of nurses’ experiences (e.g. physical, psychological and social issues). 12 On the one hand, it acts as a historical memory to remind society and policymakers that nursing was at the forefront of humanity's worst moments. 13 On the other hand, it helps to provide an in-depth analysis of the nurses’ lived perceptions during the different waves of the pandemic, which might shape the public perceptions of the role of nurses, even after the pandemic. 14
Several studies have described the nurses’ experiences on social media during the first COVID-19 pandemic wave.15–19 O’Leary et al. 15 have considered the online interactions, the social networks, and the perspectives of nurses at the individual and organization levels by examining the conversations about COVID-19 that emerged on Twitter from 10 March 2020 to 10 May 2020. Four main topics emerged from the 10,574 tweets, namely ‘the outbreak and the clinical management of the infectious disease’; ‘education and information sharing’; ‘social, economic, and political context’ and the need for ‘working together and supporting each other’. 15 Moreover, Carvalho et al. 16 have performed a thematic analysis of the content of YouTube videos regarding nursing professionals during the COVID-19 pandemic posted from 11 March 2020 to 11 April 2020. As a result, the following themes emerged: ‘nursing work conditions in different countries’, ‘recognition of the importance of professionals during the pandemic’, and ‘claims of the profession to improve working conditions’. 16 At the singular national level, Fontanini et al. 17 considered the 380 narratives posted by nurses on the five most popular Italian professional social media platforms from 23 February 2020 to 3 May 2020 during the lockdown. There was not ‘shared what is happening within each nurse’, but also ‘unprecedented lived working conditions’, triggering ‘a deep change in the profession’; however, despite the relevance of the role played, nurses perceived to ‘fail in increasing the image of nurses in society’ and called all citizens to ‘not abandon us’. 17
However, despite the following waves dealing with different health and public health strategies (e.g. lockdown or not), few studies18–19 at the international and national levels have investigated the perceptions of nurses over time with the intent to detect changes, if any (e.g. emotions and issues). Koren et al. have collected over 110,993 Facebook discussion posts and comments from March 2020 to November 2020. They have found that the main topics discussed were related to the impact of the COVID-19 pandemic (e.g. the difficulty of working during a pandemic and misinformation from media). They also have reported a change in the emotions from the beginning of the pandemic (e.g. fear and anxiety) to the later phases (e.g. exhaustion, frustration, anger and depression). 18 Moreover, Elyashar et al. have examined online discussions on their topics and emotions, as reported among 53,063 Twitter profiles by different health care providers (including nurses) during 2020 and compared them with 2019. The authors described that most of the discussions were related to the professional implications (e.g. the pandemic) and accompanied by negative emotions (e.g. reduction of joy and enhancement of fear, sadness and disgust). 19 Therefore, to date, there is a paucity of longitudinal data describing the nurses’ experiences from social media during the waves of COVID-19 that occurred from the beginning of 2020 to 2021.
Continuing to investigate their narratives as posted spontaneously might help to identify changes (e.g. new needs and issues) by considering social posts as a proxy indicator of the health and wellness of nurses. 12 Specifically, analysing the frequency and the content of messages that nurses shared on social networks might highlight their coping strategies used to tackle the pandemic (e.g. to overcome isolation, to recognize others with the same experiences and to strengthen existing relationships),20,21 thus informing interventions that health organizations should offer them. Moreover, accumulating data regarding the lived experiences of nurses might inform and shape strategies in future outbreaks and discover new trends, if any, in the public image of nurses as perceived by citizens, given that social media forms this image. 22 Accordingly, this study aimed to examine the experience of Italian nurses posted on social media in different waves of the COVID-19 outbreak and discover changes, if any, over time.
Method
Research design
We performed a mixed methods study
23
as an emerging health research methodology that combines the strengths and counteracts the weaknesses of quantitative and qualitative methods during analysis and interpretation, resulting in an enriched and deeper understanding of complex and multifaceted health research problems.
24
According to the framework of Creswell and Clark
23
—sequence, priority and integration—we have based this mixed methods study on the following characteristics:
Sequence: Our data were obtained from two sources. First, we performed a qualitative descriptive study during the first wave of the pandemic in Italy (February 2020 to May 2020) to collect daily posts and describe themes and subthemes according to content analysis.
17
Then, we continued with a longitudinal study from October 2020 to May 2021 (second and third waves), intending to compare data over the waves. Priority: The quantitative method prevailed to assess changes, if any, in the themes and subthemes over the waves (‘QUAN→qual’).
25
Integration: We integrated data in the data analysis and findings by using the themes and subthemes that emerged in the qualitative study during the first wave
10
to categorize data that emerged in the second and third waves as collected longitudinally.26–28
Finally, herein, we reported the study according to the Good Reporting of a Mixed Methods Study (GRAMMS) criteria (Supplementary Table S1).
29
Setting and sample
Social media platforms allow individuals and communities to share different activities (e.g. get involved, communicate, cooperate and have fun). 30 Thus, our study accessed professional social media platforms 31 where nurses can post various types of topics and experiences in a ‘dynamic’ format, allowing for a shared discussion among peers and the public. Specifically, we identified the most popular nursing websites and Facebook pages among Italian nurses using the user/follower ratio. 32 Then, we considered as eligible all forms of narratives (texts, letters, posts and interviews) as posted by nurses from 23 February to 3 May 2020 and from 13 October 2020 to 23 May 2021, reporting the experiences of nurses during the first, 17 second and third waves of the COVID-19 pandemic in Italy, respectively. We considered the second and third waves as a continuum (after this called ‘second/third wave’) because they shape a unique wave with two uninterrupted peaks in Italy. 33 Moreover, given that these have been documented as second waves at the international level, we considered the waves together to ensure the comparability of the findings with other evidence in the field. 34
We included all narratives: (a) written in Italian or English; (b) produced by nurses working in Italy; (c) published during the time frame identified by Italian regulatory bodies as delimiting the waves of the COVID-19 pandemic 33 ; and (d) that appeared on Facebook pages and the websites of five Italian nursing webpages (National Nursing Board [FNOPI], AssoCareNews.it, Nurse24.it, InfermieristicaMente and NurseTimes).
Per exclusion criteria, we have not considered written or audio posts from nurses working overseas, nursing students and other health care providers. We also excluded those narratives posted by presidents of Italian Nursing Professional Associations when they did not report their direct experience in the field.
Data collection
Two researchers examined the identified professional social media daily (RF: during the first wave; VP: during the second/third wave). Accordingly, they selected and extracted all posts by transcribing the texts into a Microsoft Word file. They also maintained the chronological progression in which they appeared online; furthermore, they copied all available details (day, hour, name of the nurse if reported, age and setting [e.g. units]). In 8 days, randomly selected, two researchers (EV and AP) performed independent blended scrutiny of the same social media pages, thus comparing findings with those obtained by researchers involved in the data collection. No discrepancies emerged. As a result, we obtained 475 pages and 202,626 words in the first wave 17 and 132 pages and 68,388 words in the second/third wave.
Data analysis
First, elements of narratives were anonymized (e.g. name), as well as the name of the hospital when reported. Then, for each post, an acronym was applied indicating the source (e.g. FNOPI social media), and a progressive number (FNOPI1), thus rendering the entire data extraction process verifiable.
We first extracted the demographic and professional data from narratives when available (e.g. gender and age) by calculating frequencies, percentages, averages, standard deviations (SDs, ±) and ranges according to the nature of the variable. Subsequently, we examined data about each post (number and number of words) in their correlations (Pearson, r), if any, with the number of new cases and deaths as reported officially in Italy every week (Supplementary Table S2).
Then, we considered the findings from the qualitative descriptive study performed during the first wave of the pandemic in Italy. 17 This qualitative study was based on the content analysis performed on the posts of the first wave by systematic coding and categorizing the large volume of textual information aimed at emerging patterns and their frequencies. 35 Thus, four researchers (one couple: RV, VP; another couple: EV, AP) extracted the significant units of narratives (e.g. quotes) 36 from each post of the second/third wave. All of them were categorized in the themes and subthemes that emerged previously during the first wave 17 by reading and re-reading each to assess its appropriateness. One researcher conducted the process for each couple, which was then verified independently by a second researcher; disagreements were discussed. Moreover, in the case of non-categorizable quotes suggesting a potential new theme, two other researchers (GR and JL) developed a new categorization by using content analysis, 35 also labelling the emerging themes and subthemes. In the entire process, the principal investigator assisted the researchers by helping to overcome all disagreements through dialogue.
Researchers calculated frequencies and percentages for each theme and subtheme as the number of quotes categorized in each out of the total number of quotes that emerged in each wave. Therefore, to assess changes, if any, in the patterns as to how posts have longitudinally evolved in their content, we compared frequencies and percentages by using the chi-square test (Fisher's test when appropriate) and continuous variables with the Mann Whitney U-test, considering p values as <.05 statistically significant.
Rigour
We ensured credibility, dependability, confirmability and transferability by applying the following strategies
37
:
Credibility was promoted by reading and re-reading the posts, extracting quotes several times and providing a trial code (Supplementary Table S3). Dependability was ensured by providing a research protocol including a clear description of the data collection processes and analysis procedures to all members of the research team. Confirmability was ensured by promoting discussion among researchers to reach an agreement when data analysed independently were not fully agreed upon. Transferability was increased by extracting all data available (e.g. age, gender and units) from the posts, thus allowing for the external validity of the findings (e.g. ages of nurses and units).
Ethical considerations
We developed the study according to the principles of the Declaration of Helsinki. 38 Furthermore, according to the Italian rules, no ethical approval was required considering the nature of the study; however, the research group has carefully considered the ethical issues 39 regarding social media studies by following the recommended strategies. Namely, we protected participants, ensuring the complete anonymization of the nurses’ narratives (e.g. when reporting the names of nurses) freely available on social media and obtained without asking for their consent. Furthermore, we guaranteed confidentiality of the hospitals, when cited in the posts, by removing their details, if any, from the quotes extracted to preserve nurses from the consequences of disclosing sensitive data associated with their working positions without asking for any authorization.
Results
Narratives
A total of 380 narratives emerged in the first wave (from 12 to 74/week) and 161 in the second/third wave (from one to 12/week), with 202,626 words (on average, 533 words/narrative) and 68,388 words (on average, 425 words/narrative), respectively (Supplementary Table S2). The number of narratives was significantly correlated with the number of cases (first wave, Pearson, r = 0.993; p ≤ .01; second/third wave, Pearson, r = 0.617; p < .01) and with the number of deaths (first wave, r = 0.963; p ≤ .01; second/third wave, r = 0.991; p < .01) on a weekly basis as reported nationally. Similarly, significant correlations emerged with the number of words of each narrative and the number of cases (first wave, r = 0.993; p ≤ .01; second/third wave, r = 0.621; p < .01) and deaths (first wave, r = 0.964, p ≤ .01; second/third wave, r = 0.990; p < .01), respectively.
In the first wave, 219 narratives were written by female nurses (out of 371; 59%); 48 (13%) of them reported their age, with a mean of 35.3 (±9.2) years. Nurses were working in the most affected region in Italy (Lombardy, 67/200; 33.5%) and in critical care settings (93; 51.9%) (Table 1). In the second/third wave, female nurses authored 95 narratives (out of 155; 61.3%); 155 (96%) of them reported their age, with a mean of 43.5 (±16.4) years. The nurses were operating in the most affected region in Italy (Lombardy, 13/69; 18.8%) and in critical care settings (41; 52.6%) (Table 2).
Profiles of nurses according to the narratives included.
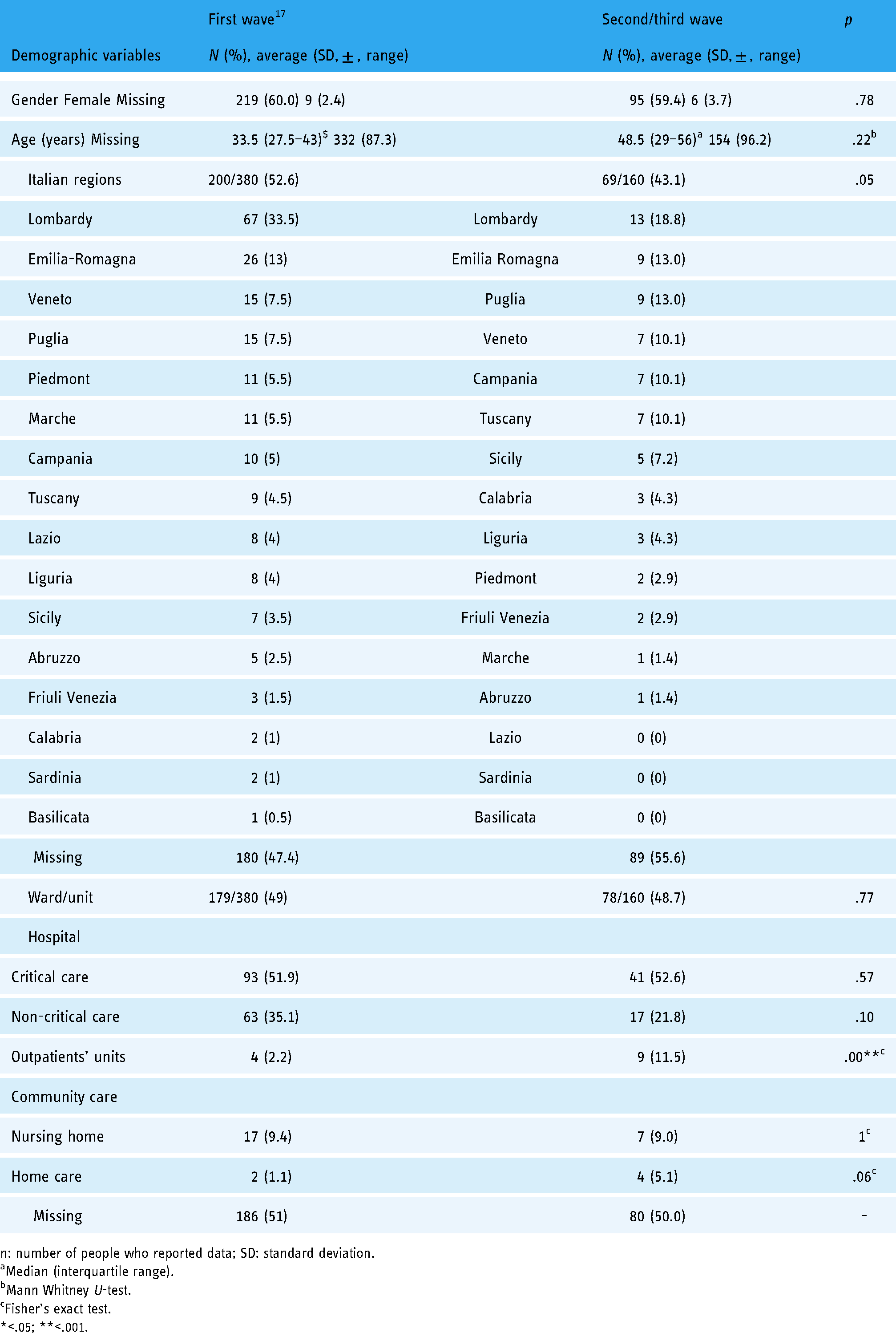
n: number of people who reported data; SD: standard deviation.
Median (interquartile range).
Mann Whitney U-test.
Fisher's exact test.
*<.05; **<.001.
Themes and subthemes: comparison between the first wave and the second/third wave.

The bold values are the N and % value of a specific theme.
N: number.
Fisher's exact test.
*<.05; **<.001.
Themes and subthemes
From the 380 and 161 narratives of the first and second/third wave, we extracted 2510 and 835 quotes, respectively. Five themes emerged in the first wave; in the second/third wave, a new theme emerged in addition to the five themes. ‘Sharing what is happening within myself’ was the most frequent theme in the first wave (891; 35.5%), and ‘experiencing unprecedented working conditions’ (267; 32%) was the most frequent theme in the second/third wave (Table 2). Examples of quotes that emerged from nurses’ narratives during the first and second/third waves are reported in Supplementary Table S3.
Theme 1. ‘Sharing what is happening within myself’
With 891 (35.5%) quotes in the first wave, the occurrence of this theme significantly decreased in the second/third wave (237; 28.4%) (p = .00). However, among four out of five subthemes, no significant differences emerged, namely ‘experiencing emotional ups and downs’ (first wave 276; 31% vs. second/third wave 93; 39.2%, p = .96), ‘dealing with physical discomfort’ (267; 30% vs. 69; 29.1%, p = .06), ‘feeling proud’ (81; 9.1% vs. 31; 13.1%, p = .57) and ‘being a person under the mask’ (27; 3.0% vs. 6; 2.5%, p = .42). Differently, the subtheme ‘protecting my family’ significantly decreased in frequency from 240 (26.9%) to 38 (16%) quotes between the waves (p = .00) (Table 2).
Specifically, nurses reported, as the primary lived experience, the difficulty of coping with emotions and physical discomfort, generating emotional ups and downs. Nurses narrated a sense of guilt for deaths, anxiety, fear, discouragement, helplessness and panic as negative emotions capable of leading to burnout. Besides emotions, nurses experienced physical discomfort (e.g. fatigue, headache, breathlessness and dermatitis) due to the excessive length of shifts and the necessity of wearing PPE all day, making their faces wounded and painful. Despite the difficulties, nurses have also described their experience of caring with a feeling of pride, demonstrating the desire to give their best, with passion, commitment, professionalism, sense of duty and enthusiasm.
Different experiences about their relationships with their own families emerged. They felt isolated from their family, lonely and sad without smiles, hugs and kisses; nurses felt also fear of infecting or a sense of guilt for having infected their loved ones, trying strenuously to protect their families. Although often described as heroes, nurses have reported the need to be considered individuals under their masks, recognizing themselves as fragile, scared and helpless.
Theme 2. ‘Experiencing unprecedented working conditions’
This theme was homogeneously represented in the first (749; 29.8%) and in the second/third waves (267; 32%) (p = .26). However, some subthemes, such as ‘caring for terrified patients and families’ (first wave 243; 32.4% vs. 74; 27.7%, p = .52) and ‘resisting and resisting’ (164; 21.9% vs. 69; 25.8%, p = .10), were homogeneous. Differently, ‘working in a changing environment’ significantly diminished in frequency (137; 18.3% vs. 12; 4.5%; p = .00), whereas ‘they are playing with our lives’ increased in frequency (205; 27.4% vs. 112; 42%, p = .00) (Table 2).
Nurses have shared the unprecedented working conditions experienced, reported principally as caring for frightened patients and families in modified health care settings where the shortages of human and physical support are a new reality. In these circumstances, resistance represented an obligatory choice. In a context where patients have experienced fear and agony far from their families, nurses have represented the only ones capable of assisting them in loneliness and suffering. They have learned to relate with them beyond words (e.g. using eye contact and keeping their hands gentle). During this challenging time, the hospitals and wards have changed their layouts and processes of care, generating nostalgia among nurses regarding the pre-COVID-19 working conditions. Thus, the nurses’ narratives have also described unprecedented work settings characterized by a shortage in the staff's high level of competence and professional skills, as health care providers were often inexperienced and unprepared. This scenario has led nurses to reorganize their free time, sacrificing their holidays and leave to cover shifts, ensuring the continuity of care and mentoring new colleagues.
Moreover, nurses have experienced a lack of security and protection (e.g. adopting non-compliant PPE) during their shifts. They have seen their rights trampled, feeling deceived and abandoned by health organizations and the political system, and criticized for preferring the economic issues to the health of citizens and health care providers. Despite the difficulties, nurses have also claimed their desire not to give up, fight and win their battle with the virus at all costs, calling all health care providers to action.
Theme 3. ‘Failing to rehabilitate the image of nurses in society’
This theme remained stable in its frequency over the waves (376; 15% vs. 107; 12.8%, p = .13). However, two subthemes have significantly reduced their frequency across the waves, namely ‘being just a nurse, not a hero, nor an infector’ (first wave: 294; 78.2% vs. 39; 36.5%, p = .00) and ‘remembering and still experiencing aggressions’ (33; 8.8% vs. 3; 2.8%, p = .02). Instead, ‘despite everything, still devaluated’ significantly increased (49; 13% vs. 65; 60.7%, p = .00) (Table 2).
Several concrete expressions of support from citizens (e.g. patients and families) and the whole community (public opinion) have triggered an immense recognition of nurses as angels and heroes. However, nurses confirmed their desire to be considered just like nurses in their service, although with a lesser frequency over the waves. Nevertheless, a part of society has continued to identify nurses as propagators of the virus over the waves, well remembering the aggressions (e.g. insults, threats and blows) that nurses received before the COVID-19 outbreak that are still present even if with a downward trend over the waves. However, despite their immense efforts to struggle with the pandemic, the nurses’ images have been reported in more posts as still under-evaluated and depreciated by the public from the first wave to the second/third wave. Nurses shared their hope that the community will remember the strains and struggles of nurses when the COVID-19 pandemic is over by implementing adequate resources at the bedside and providing proper compensation.
Theme 4. ‘Experiencing a deep change in life’
This theme remained stable at the overall levels across waves (253; 10.1% vs. 95; 11.4%, p = .31). However, while two subthemes were homogeneous, namely ‘living in fear for colleagues: I’m with you’ (116; 45.9% vs. 27; 28.4%, p = .10) and ‘thinking of my future: staying or leaving?’ (20; 7.9% vs. 13; 13.7, p = .08), two other themes changed significantly, namely ‘changing sides: becoming a COVID-19 patient’ increased in frequency from 35 quotes (13.8%) to 31 quotes (32.6%) (p = .00), whereas ‘impressing this experience in my life’ decreased in frequency (82; 32.4% vs. 24; 25.3%, p = .01) (Table 2).
Nurses have reported episodes of heartfelt transformation as individuals. They have continuously shared their fear regarding the contagiousness of colleagues, attempting to preserve reciprocally, perceiving a sense of cooperation and mutual help never experienced before. As the main difference reported, nurses narrated complete compliance with the advice given by health organizations and the endless awareness of respecting suitable actions for themselves and other health care providers. However, unfortunately, these attentions have resulted in an unfavourable scenario, as the virus has also infected nurses, causing them to change sides and experience what it means to be a COVID-19 patient. Moreover, nurses have reported their anxieties of being judged guilty for having missed the health care recommendations capable of limiting the contagiousness of their patients and teams. Accordingly, these concerns have stimulated essential changes in analysing their thoughts and giving meaning to life. Given the strong impact of COVID-19 on their lives, some nurses have also claimed to rethink their professional choice as nurses. As emerged from narratives, they have considered the possibility of leaving the profession in the post-pandemic period, a thought that has remained stable over the waves.
Theme 5. ‘Do not abandon us’
From 241 (9.6%) quotes in the first wave, this theme had a reported frequency of 77 (9.2%) in the second/third wave (p = .80) (Table 2). Nurses still reported ‘living a surreal drama’ during the second/third wave of COVID-19 in a homogeneous frequency (83; 34.4% vs. 25; 32.5%, p = .74). Their narratives highlighted unreal working conditions, revealing the demanding challenges faced during every shift. Moreover, although without statistical significance, nurses have slightly increased their posts regarding their ‘experiencing a war on the frontline’ (50; 20.8% vs. 27; 35.1%, p = .05), describing themselves as fighters against the bombs of an invisible enemy. From this frontline, nurses have still called on citizens to nurture a shared sense of responsibility, giving a sense to the extensive efforts of health care providers with moral behaviours aimed at breaking the chain of contagion. In this challenging time, social media represents a tool capable of improving the awareness of citizens and society, spreading the critical message: ‘stay at home’ (108; 44.8% vs. 25; 32.5%, p = .11).
Theme 6. ‘Experiencing the mixed emotions towards jabs’
This theme emerged only during the second/third wave, resulting in a frequency of 52 (6.2%) quotes (Table 2). Nurses have reported ‘being grateful to science’ because it has provided the vaccine quickly, offering the opportunity to restart a life of freedom where kisses and hugs represent the normality. Nurses have ‘dedicated their immunization’ to those who died before the vaccination campaign and those cared for in their last moments of life when they were alone. However, nurses’ narratives also oscillated between the ‘fear and the joy of being vaccinated’. On one side, they have shared the apprehension of adverse effects (e.g. unpredictable effects). On the other side, the incredible emotion of receiving the first jab has overcome some hesitations. Nurses also shared the perception of ‘being obligated to be vaccinated’ in two directions: as a moral duty, with the desire of acting as an example of responsibility and altruism towards society, and as a non-negotiable and imposed choice given its mandatory nature for health care workers. While the moral obligation has helped to overcome hesitancies, nurses narrated their surprise about COVID-19 anti-vax colleagues and their obstinacy to defend conspiracy theories without a scientific basis. At times, nurses have stated that they feel negative emotions towards their COVID-19 anti-vax colleagues (e.g. shame, contempt and anger), wishing the professional body would disbar them from the national registry.
Discussion
Narratives
To the best of our knowledge, this is the first mixed methods study analysing the narratives of nurses posted on social media over the COVID-19 waves by considering all their ‘voices’ as unique stories. 40 At the overall level, we observed a reduction in the number of posts and in the number of words used from the first wave 17 to the second/third wave, and this may be interpreted two-fold, as a sort of adaptation and resignation to the situation and as a sign of fatigue, discomfort and helplessness. 41 However, similarities in correlations across waves emerged between the amount of cases and deaths reported at the national level and the number/length of narratives posted, suggesting the need for nurses to use posts to communicate their experiences as the severity of the pandemic advances. Evidence has recognized social media as cathartic instruments for mitigating stress and loneliness in nurses living during the COVID-19 pandemic. 42
As emerged during the first wave, 17 and in the second/third wave, nurses reported some details (e.g. age, gender and unit) in almost half of their posts, confirming the desire to share their experiences openly and transparently. Moreover, the profiles of nurses were similar in gender, with females reporting more posts than males, although a slightly older age emerged among those sharing their posts in the second/third wave as compared to the first wave. 17 These findings seem to align with the evidence available regarding social media use among health care workers. 43
Themes and subthemes
Over time, the theme ‘sharing what is happening within myself’ significantly reduced overall frequency and had a homogeneous occurrence in four out of five subthemes. As already documented in the first wave, 17 nurses have also continued, in the second/third wave, to use social media to share their physical and emotional sufferance due to the gruelling working conditions (e.g. lack of rest between shifts and overuse of PPE) imposed by the COVID-19 pandemic. Moreover, nurses have continued to share intense emotional ups and downs (e.g. swinging from fear of infecting and guilt for the dead to pride and enthusiasm for their profession) over the waves, suggesting the presence of signs of psychological distress is in line with the findings of other countries (e.g. Republic of Ireland, Uganda and UK).44–46 Health organizations are recommended to monitor their emotional health and burnout long term. 47 Moreover, through narratives, nurses called to consider themselves as normal people ‘under the mask’ (e.g. frail, fearful), 17 thus willing to lead to a detachment from the stereotype of superheroes affixed to them by society.13,48 While acknowledging the loneliness from family and the desire to avoid contagion, nurses have used fewer narratives for the subtheme ‘protecting my family’, resulting in an element of novelty compared to the first wave. 17 This might be interpreted as an increase in perceived safety due to the vaccination campaign giving priority to all health care workers, thus increasing their sense of protection.
Also, the second theme (‘experiencing unprecedented working conditions’) was homogeneous across the waves. The perception of caring for terrified patients and families remained over time. During their caring experiences, first-line nurses reported that they learned to support patients more (e.g. through touch and gaze). This finding underlines the importance of the non-verbal channel as a vehicle for empathic communication that may have improved over the waves, overcoming barriers imposed by PPE in different settings (e.g. emergency services and intensive care units). 49 Furthermore, nurses have homogenously reported their willingness to resist and develop positive coping and resilient strategies that have been considered protective factors regarding psychological distress during the COVID-19 pandemic. 50 However, compared to the first wave, 17 nurses’ perceptions regarding work in an ever-changing environment have significantly decreased. Specifically, nurses have reported a less frequent shortage of human and physical support within their working conditions. This point might be interpreted as the acceptance of a ‘new’ reality that has now become ‘ordinary’ as already internationally documented, 51 or as a sign of the investment in the care by the national health care system and its increased capacity to react to the challenges. 52 Differently, a significant increase in the quotes communicating anger from the lack of support and protection from the health care organization and political systems has emerged, confirming findings of other countries (e.g. the UK). 53 The sensationalist posts have already been documented, among other professional profiles, whether such conduct conflicts with the existing professional standards and deontological codes. 54 Without entering into this debate, findings suggest the need for governments to establish public health plans to control future outbreaks, 55 and the duty of health care organizations to listen today to nurses’ experiences by creating supportive contexts. 47
As has emerged previously, the third theme (‘failing to rehabilitate the image of nurses in society’) has revealed a similar frequency across the waves but with some significant differences in its subthemes. Signals of gratitude from citizens (e.g. meals and gifts) and the perception of being considered a hero have been reported less frequently, as well as the verbal and physical aggressions received from citizens before the pandemic. Instead, they have more frequently described their dissatisfaction as still being undervalued (e.g. underpaid) or considered negatively (e.g. as virus propagators). Although society is beginning to understand the importance of nursing care during the COVID-19 pandemic, 51 Italian nurses perceived to have missed the opportunity to build a positive reputation among citizens as more recognized in the second/third wave. At a worldwide level, nursing community is still changing its identity from a simplistic and stereotyped image to an independent profession where knowledge, competence and moral values interplay with each other. 56
At the overall level, the fourth theme (‘experiencing a deep change in life’) has also reported a similar frequency across the waves. Different from other countries (e.g. Australia), 57 during the pandemic, Italian nurses have positively experienced teamwork, informing health care organizations of the opportunity to nurture this culture of unity also in the post-pandemic period. 47 However, in their narratives, while the infection progressively spread, 58 nurses more frequently have reported becoming infected, changing sides as ‘COVID-19 patients’, reporting later experiencing a mix of emotions (e.g. anger and depression) as reported in other countries (e.g. Poland). 59 The number of infected nurses in the second/third wave, just before the vaccination campaign, reached impressive numbers in Italy. 60 Furthermore, compared to the first wave, 17 nurses have reported less frequently being permanently impressed by the pandemic experience. This finding might be interpreted as a sign of acquired normality and an indicator of professional exhaustion. Although not significant, the increased number of nurses posting the desire to change their profession once the pandemic is over, also documented in other countries (e.g. the UK), 46 should be considered carefully by health care organizations to prevent the loss of nursing resources and ensure patient care in the long term, 61 given that this pandemic might also have prevented the willingness of new generations from becoming nurses.
Finally, the theme ‘do not abandon us’, and its subthemes displayed similar frequencies across the waves. In our study, nurses used different military metaphors to describe their experiences during the pandemic (e.g. a war and a surreal drama), following what has already been observed nationally 17 and internationally (e.g. Israel). 62 However, the metaphorical military language, which characterized institutional (e.g. government) 63 and media (e.g. newspaper and social) communication64,65 during the pandemic, has been underlined to have positive and negative implications. On the one hand, it facilitates the sharing of alert messages helpful in reducing the chain of infections among citizens. On the other hand, it has the risk of burdening the front-line health care providers with excessive responsibilities that can lead to psycho-emotional exhaustion. 66 The nurses, in their narratives, have highlighted how this war is progressively leaving them alone, tired and hopeless to manage emotional loads never experienced before. As in the first wave,13,17 nurses used social media to share with citizens one message: ‘stay at home’ for the benefit of the entire community.
As a new finding, the theme ‘experiencing the mixed emotions towards jabs’ emerged in the second/third wave. As documented internationally by recent systematic and scoping reviews,67,68 while some nurses have reported being grateful to science for making the vaccine against COVID-19 and not understanding the widespread reluctance of their anti-vax colleagues; others have expressed fear and indecision about its possible adverse effects. Furthermore, if some nurses have lived the vaccination campaign for COVID-19 as a moral obligation and a gesture of social responsibility, others have experienced this vaccine as an imposition, promoting a bioethical debate on its mandatory nature within health organizations.69,70 Thus, in uncertain and pandemic times characterized by misinformation, 71 governments, public health organizations and professional associations are called upon to promote tailored communication campaigns on vaccine efficacy using different channels (e.g. social media) for informing hesitant and opposed nurses making the ‘right choice’ by acting as part of the solution, not the problem. Moreover, as has emerged from the narratives, vaccinations for COVID-19 should be considered a critical point, capable of introducing divisions inside of teams and distance among health care providers already pressured by challenging working conditions for more than one year.
Limitations and strengths
Our study has several limitations. First, the analyses of the nurses’ experiences of the COVID-19 pandemic emerged from their posts may have introduced a selection bias by obtaining a description of the phenomenon only from those nurses who use social media, 12 thus limiting the generalization to all Italian nurses. Second, we considered narratives posted by Italian nurses only on some professional social media, excluding others frequently adopted (e.g. Twitter). 19 Third, we have supposed that nurses wrote all narratives posted, without adopting systems to check their provenience. 17 Fourth, we considered each post as an individual story without analysing the interconnection across nurses’ narratives, 15 hence offering the possibility to investigate this relationship in future studies. Fifth, although we investigated the content of nurses’ narratives (e.g. emotions or issues), considering their change over time, we have missed the opportunity to quantify their intensity systematically (e.g. using machine learning, algorithm, or sentiment analysis)18,19 or adopting other coding models than content analysis. 35 For example, future studies should adopt the coding scheme proposed by Cutrona and Russell 72 to analyse the type of social support (e.g. informational, emotional, esteem, network and tangible) that emerged from social media, offering insights on how health care providers buffer the stress of the pandemic.
Although the combination of quantitative and qualitative data can represent a complex challenge for various reasons (e.g. time-consumption, difficulty in integrating paradigms and need for high skills), we used this research methodology because it is very informative for health organizations and policy. 24 Accordingly, to ensure high methodological standards, we applied different strategies, 24 such as the following: (a) a multidisciplinary team of clinicians and researchers with different backgrounds (e.g. nursing and physiotherapy) and experience in both quantitative and qualitative methods and (b) the guidelines of the GRAMMS. 29
Conclusions
The narratives posted by nurses over the COVID-19 waves touched five main dimensions among the waves—individual, professional, work-related environment institution(s) and society; in addition, a dimension emerged with the second/third wave regarding vaccinations. Some significant changes have emerged inside the mentioned dimensions, suggesting modifications in the nurses’ lived experiences and perceptions.
First, nurses shared their experiences of intense emotional and physical discomfort, which was worsened due to the fear of infecting their families and led to further social distancing to protect their loved ones. However, over the waves, this dimension reduced in frequency, suggesting the ability of nurses to cope or, on the other hand, their emotional exhaustion. Nurses should develop effective coping strategies towards events triggering high psychological implications, whereas health care organizations should offer counselling and support to avoid trauma and long-term effects.
Second, at the professional and working environment levels, they still lived in unprecedented working conditions over the waves, with an increased perception that health care institutions are ‘playing with our lives’. The pandemic was a sort of stress test for health care organizations; however, it is also a great occasion to learn from the experience. Transforming this strong experience into a learning one requires effective environments where nurses can openly express lived difficulties.
Third, despite the perceived recognition from the citizens and the entire community, nurses reported still being undervalued over the waves with a stable frequency. However, as revealed by the fourth theme, the pandemic experience has changed in-depth the lives of nurses with some adaptations over the waves induced by the experience of direct infection while keeping the intent to leave the profession. Losing nurses might exacerbate the dramatic nursing shortage experienced during the COVID-19 pandemic; moreover, keeping these nurses in the workplace, after this tremendous experience, might increase the value of the care and that of the entire health care service given their acquired competencies.
Finally, Italian nurses have interpreted the vaccination campaign differently, both positively (e.g. a gift or an opportunity) and negatively (e.g. an obligation or a concern). These different perspectives might improve the risk of creating division between nurses with potentially negative repercussions for the nursing profession both inside (e.g. workplace tensions) and outside (e.g. loss of credibility among citizens). Therefore, nurse managers, health care organizations and professional bodies should promote evidence-based communication approaches to overcome issues in vaccination among health care workers for the benefit of the entire profession and the society in the short and long terms.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076221129082 - Supplemental material for Italian nurses’ experiences of the COVID-19 pandemic through social media: A longitudinal mixed methods study of Internet posts
Supplemental material, sj-docx-1-dhj-10.1177_20552076221129082 for Italian nurses’ experiences of the COVID-19 pandemic through social media: A longitudinal mixed methods study of Internet posts by Giacomo Rossettini, Verena Peressutti, Erica Visintini, Roberta Fontanini, Davide Caruzzo, Jessica Longhini and Alvisa Palese in Digital Health
Footnotes
Author contributions
Study design: AP, VP, GR. Data collection: VP, RF, EV, AP. Data analysis: VP, RF, EV, DC, JL, GR, AP. Study supervision: AP. Manuscript writing: GR, AP, DC, JL. Critical revisions for important intellectual content: AP.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.