
Abstract
Objective
Adolescent females in the United States continue to have unmet sexual and reproductive healthcare needs. Research shows that interventions incorporating peer support can augment perceived self-efficacy and reinforce healthy behaviors. Yet, few user-centered digital sexual health interventions incorporate peer support, and aim to change perceptions of peer norms and model social skills. The objective of this study was to design and demonstrate the receptivity of adolescent females to illustrated digital social media stories that promote healthy sexual behaviors and peer social support.
Methods
We conducted a three-phase study approved by our Institutional Review Board. In Phase 1, we presented sexually active adolescent female emergency department patients aged 14–19 with eight sexual health scenarios via a survey study. Participants wrote three text messages addressed to the protagonist of each scenario which motivated and encouraged her to consider the use of contraceptives. Messages were scored based on the construct of peer support (emotional, tangible, informational, and belonging). In Phase 2, we worked with a professional artist and screenwriter to design digital sexual health comics using the gathered messages. In Phase 3, we gathered feedback on the comics from adolescent female emergency department patients.
Results
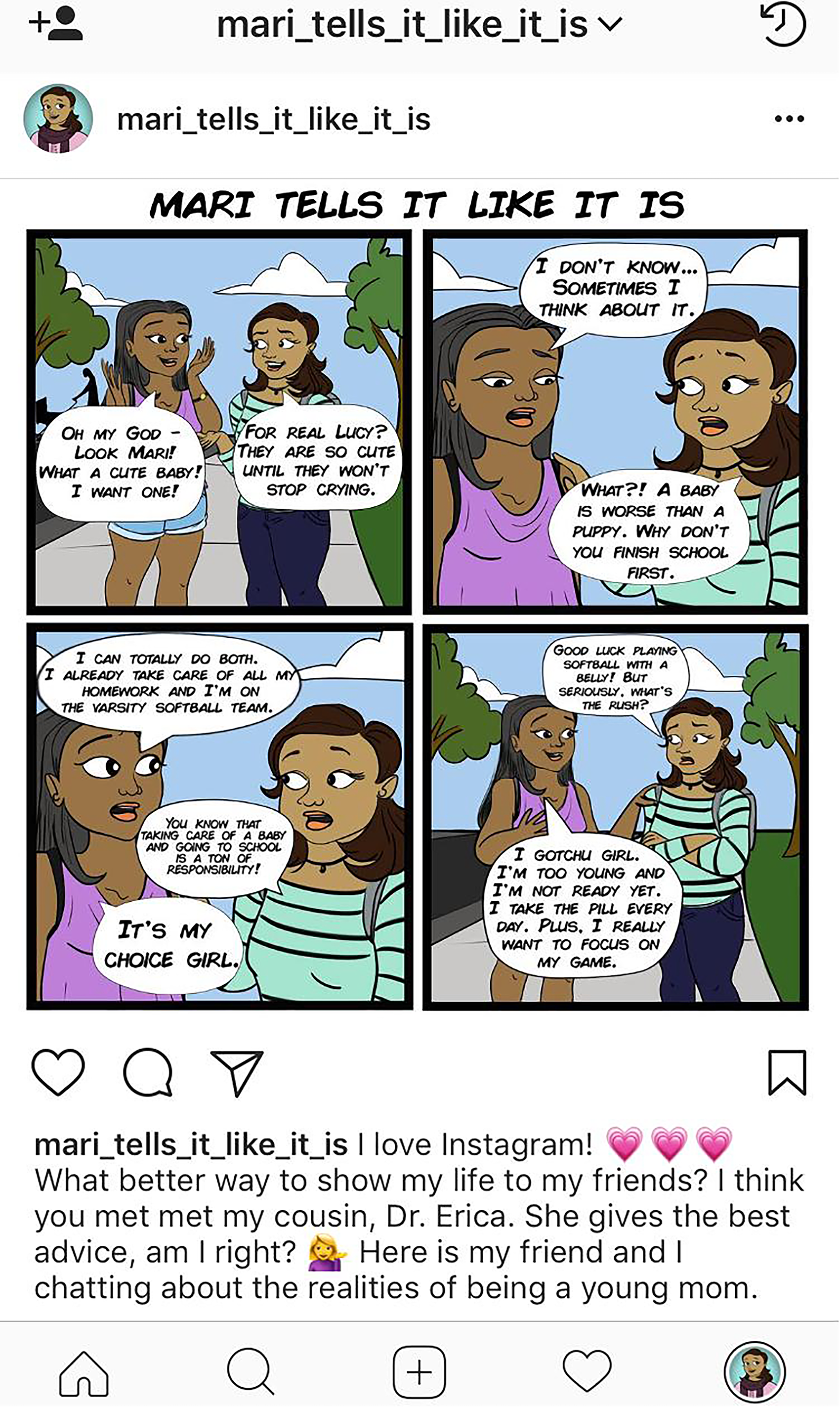
Females (n = 22) provided 352 messages. Using top rated messages, we designed five digital visualizations in a running story called Mari tells it like it is. Each story incorporated 5–12 peer-authored quotes. We inserted the final images into Instagram®. Additional females (n = 39) found the images “relatable,” “super-realistic,” and “educational.”
Conclusion
Collecting peer-authored texts from our local adolescent community led to the creation of well-received sexual health visualizations. This novel method of design incorporated adolescent voices to promote peer support and healthy behaviors.
Keywords
Introduction
Despite widespread programmatic efforts, adolescents continue to have unmet sexual and reproductive health needs.1,2 Rates of unintended pregnancy and sexually transmitted infections (STIs) in the United States remain high, with half of all new STIs diagnosed each year among those aged 15–24. 3 Evidence-based sexual education and access to effective contraceptive methods, especially long-acting reversible contraceptives, differs geographically. 4 Disparities in unintended pregnancy and STI rates persist across races and ethnicities.4,5 Innovative sexual health interventions could help address these gaps, especially interventions that are theory-based and user-informed and have a broad reach.6–8
Interventions that incorporate social support, specifically peer support, can improve well-being. Social support is a broad construct comprising both the social structure of an individual's life and the specific functions served by various interpersonal relationships. 9 Adolescence is characterized by the rise in importance of peer groups. Peer support may be particularly important during adolescence, given the changes in social roles and responsibilities experienced over that period. 10 Peer support can augment perceived self-efficacy and reinforce new healthy behaviors through observation and modeling. While peer influence in some instances can negatively influence behaviors, peer social support can significantly and positively influence health.11–14 Given how social environments influence behavior, several conceptual models incorporate social support, stressing the influence of peers on behavior. For example, the Theory of Planned Behavior aims to predict a person's intention to engage in a behavior in a specific time and place. 15 Constructs include subjective norms, which is the belief about whether most people approve or disapprove of a behavior, such as peers. Another example of conceptual model incorporating peer support is the Social Cognitive Theory. 16 This theory considers the social environment in which the individual performs the behavior. Observation learning occurs through “modeling” of behavior. Interventions that enable individuals to perceive greater support can lead to positive behavior change.17–20
Digital media offers a means to deliver innovative health interventions and provide peer social support that may lead to behavior change. For decades, public health efforts have communicated behavior change messages through media channels, such as mass media (radio and television) or small media (comic books and newsletters), with topics that range from promoting seatbelt use to family planning to smoking cessation.21–23 Currently, young adults are the largest users of mobile technology in the United States and mobile health technology shows promise as a way to engage patients in their healthcare and deliver evidence-based health information.24,25 Health professionals aim to communicate with teenagers through an array of digital content, including social media, text messaging, and apps. Digital tools are accessible, broadly reaching a large audience at low costs, teaching skills to a group in a way that is readily available and familiar and can be delivered with relatively ease with high fidelity. 26 Interventions can also be tailored to specific subgroups, such as lesbian, gay, bisexual, and transgender (LGBT+) youth, racial/ethnic minority youth, and adolescent girls and boys.27–29 The interventions can also provide privacy, which is particularly important for adolescents. Data shows that these interventions can lead to positive behavior change in the area of adolescent sexual health.30–35
There are, however, several challenges to designing, studying, and implementing digital health interventions, especially in the field of sexual health. These include how to best tailor the intervention so it feels relatable to the individual, the rapidly changing landscape of technology and how it can lag behind the trials testing the interventions, a debate on the appropriate biological versus patient-centered outcome, and, importantly, how behavioral change in adolescent is particularly difficult, with individual and environmental factors interplaying at all times.36,37 Another factor that can limit the effect of an adolescent intervention is the design of these digital interventions itself, which are typically built around the constructs of an existing healthcare system constructs, such as the electronic medical record, and minimally involving end-users. 38 Digital health interventions, especially those that target adolescents, must consider the needs and perceptions of the intended audience so that the intervention will be perceived as easy to use, valuable, and appealing. 25 To address these challenges, user-centered mobile health design is a strategy that can incorporate the perspective and needs of intended end-users into technology design. 39 Several interventions have included users in their design, which may have led to their success.40,41 This is particularly important when interventions try to incorporate peer support, which can be a complicated construct to recreate especially digitally. While certain interventions have demonstrated success in this area in topics such as preventing maternal depression and physical activity, others have showed limited success such as those supporting caregivers of children with complex care needs.19,42,43
More research is needed on how to best incorporate peer support into digital health interventions, especially those that focus on adolescent sexual health. The objective of this study was to design and demonstrate the receptivity of adolescent females to illustrative digital comic stories that promote healthy sexual behaviors and peer social support. This manuscript presents the three-phase development and evaluation process of the illustrative social media stories. The first phase used user-centered design methodology to gather language that reinforced peer support for healthy sexual behaviors and relationships. In Phase 2, we worked with an artist and screenwriter to design peer-authored sexual health messages to be inserted into Instagram® sexual health visualizations. In the third phase, we gathered feedback of the digital sexual health visualizations from adolescent female Emergency Department (ED) patients.
Methods
Phase 1: Survey study
Study design and participants
Figure 1 represents all phases of the study. In Phase 1, we conducted a survey in one urban pediatric ED. Our ED primarily cares for our local inner-city, urban community, whose population lives within a few miles of the hospital. Based on our prior work, our adolescent ED population also predominantly identifies with being Hispanic and of “Other” race. 29

Three phases of study design.
We enrolled a convenience sample of sexually active female ED patients aged 14 through 19 years who had ever used effective contraceptives (n = 22). We defined effective contraception as use of an intrauterine or implantable device, injection (Depo-Provera or medroxyprogesterone acetate), ring (NuvaRing), transdermal patch (Ortho Evra), or oral contraceptive pills. 44 We excluded patients who were cognitively impaired, were in foster care or wards of the state, did not speak English, or were too ill for participation per the ED attending physician (which included a heightened physical or emotional state). Common reasons for ED presentations for females include abdominal pain, fever, and injury. We chose to enroll from the ED as over 18 million adolescents seek ED care each year, and many participate in sex without contraceptives, making them an important population to both study and include in future sexual health studies.45–47
Conceptual model
Social support can be conceptualized in two categories. 11 Structural support refers to the extent to which individuals are situated within or integrated into social networks, such as marriage or social isolation. It is typically measured by assessing social integration, such as part of social networks. 48 Functional support divides into two categories: perceived support (a person's subjective account of the support them perceive as available to them) and received support (aid actually given by others to them). 49 Such functional support can take on many forms. These resources can be emotional (e.g. offer empathy, acceptance, or encouragement), tangible (e.g. provide financial or physical assistance), informational (e.g. provide guidance and advice), and companionship or belonging (e.g. share social activities and promote social belonging). 11
Procedures
Enrollment times were based on researcher availability, typically Monday to Friday between the hours of 9 am–10 pm. Using an electronic medical record (EMR) tracking board, a member of the research team identified female ED patients aged 14–19. The medical provider caring for that patient then assessed eligibility criteria and interest in study participation. If the patient was eligible and interested, a member of the study team explained the study in full and the patient provided informed consent. The Institutional Review Board (IRB) approved this study with a waiver of parental consent. Participants completed the electronic survey in a private location and received a local transportation card as compensation.
Survey
Participants completed a two-part survey. Part 1 was a brief questionnaire regarding demographics, use of medical care and technology, sexual practices and behaviors, and pregnancy intentions. We selected and adapted 18 survey questions from the Youth Risk Behavioral Surveillance System (YRBSS) and National Survey of Family Growth (NSFG); both of these surveys had been found to be valid and reliable with a cohort of patients similar to our patient populations.50,51 In addition, investigators added 11 de novo questions based on their content expertise, although we did not assess the validity or reliability of these questions. Part 2 of the survey presented eight sexual health scenarios. To design the sexual health scenarios, experts in the fields of adolescent sexual health, adolescent medicine, and pediatric emergency medicine chose ideas drawn from established sexual health curricula.52,53 Scenario topics included (a) reasons for using contraception; (b) how to find contraception; (c) reasons to delay pregnancy; (d) healthy relationships; (e) communicating with an adult about contraception; (f) reasons for completing school; (g) where to find condoms; and (h) reasons for using condoms. We also presented a scenario asking what it is like to be a teen mother to those adolescents who answered that they were a parent.
Each scenario consisted of a static image of a young female and an associated storyline. An example of one scenario read as follows: Meet Melissa. She is 16 years old and the youngest of four siblings. She is having sex with her boyfriend but is scared to go to the clinic alone for birth control. She doesn’t know what her parents would think if they found out she was having sex. Please write TWO text messages that tell her HOW TO TALK TO AN ADULT IN HER LIFE ABOUT BIRTH CONTROL. Participants read the story of each protagonist and wrote text messages to the protagonist to provide information and motivate her to use birth control. We instructed participants to write text messages that were no more than four sentences, could include abbreviations and slang (but no cursing), and were only in English. We asked for text message examples for three reasons. First, texting is a popular and familiar communication tool between adolescents. 54 Second, adolescents text with language reflects colloquial vernacular. 55 Third, text messages tend to be brief and straightforward.
Scoring
We developed a text message scoring system based on the four constructs of functional social support. Validated scoring systems do exist that measure individual perceptions of social support, but we found no validated scale that measured social support within a written message. 56 Therefore, we developed a process to assign four scores to each peer-authored text message, one score for each of the four social support constructs (emotional, tangible, informational, and belonging/companionship). Scores for each construct ranged from 0 (low application of specific type of social construct) to 2 (high application of specific type of social construct). The first part of this process consisted of investigators organizing the peer-authored text messages based on the scenario and rating a random sample of 40 texts. Scores were discussed to agree on construct definitions and scoring. Next, one investigator scored all texts; two investigators concurrently scored a separate 25% of the messages to ensure scoring consistency. Therefore, 50% were scored by two people. Any message that differed by +/-1 point or more in any of the four categories of peer support was discussed iteratively among all three investigators until consensus was reached. Scoring was conducted after all messages were collected.
Phase II: Creating illustrative digital sexual health visualizations
Sexual health topics
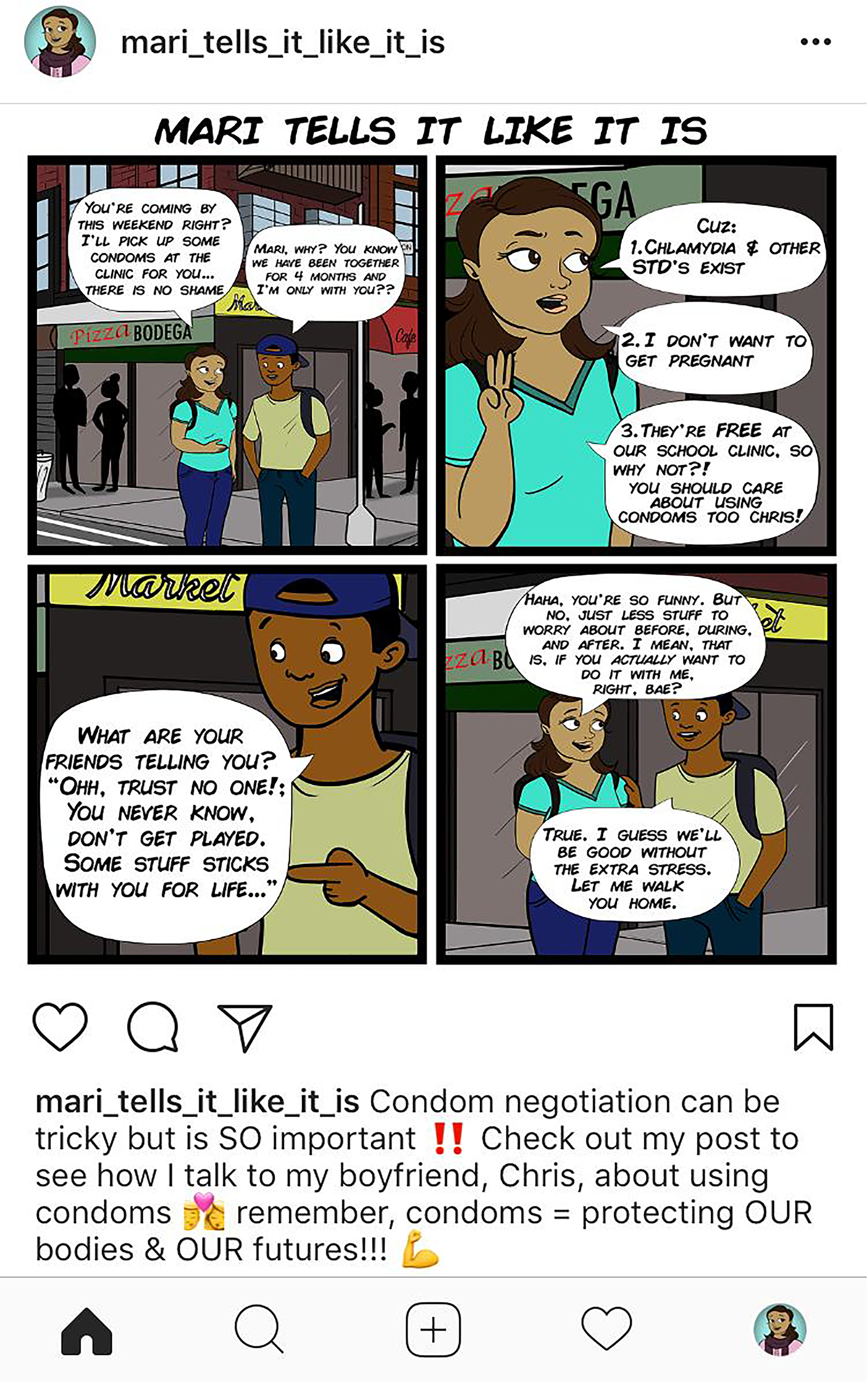
The aim of Phase 2 was to design digital sexual health visualizations using the data gathered from the survey. Each sexual health story consisted of four static frames or panels. While there were many salient topics we could have addressed, we chose topic areas most often addressed by the messages and felt most relevant to prevent STIs and pregnancy. We distilled scenario topics into the following story topics: (a) why to wait to become pregnant, (b) condom negotiation, (c) dispelling birth control misconceptions, (d) talking to an adult about sex, and (e) healthy relationships.
Procedures
The design process consisted of four steps. First, we collected the top-rated peer-authored messages; this led to ideas for each sexual health scenario. For example, one survey participant wrote about how it was hard to play softball “with a belly,” and that idea became a part of a storyboard about the responsibilities of being a teenage mother. A storyboard is a graphic organizer in the form of illustrations or images displayed in a logically sequenced order. 57 For each of the four comic panels, we sketched ideas for the looks, clothes, and setting to represent the neighborhood surrounding our local ED. We inserted top ranking peer-authored text messages into the storyboard speech bubbles, aiming to include messages that provided tangible, emotional, informational, and companionship peer support whenever possible, yet still maintain the flow and clarity of the storyline. This led to the creation a comic running narrative describing Mari, a fictional local teen confronting adolescent sexual health challenges.
Second, a professional artist used the storyboard to digitally illustrate each sexual health comic. In order for the visualizations to represent the local culture, we provided digital images of the surrounding neighborhood along with demographic characteristics of the local community who frequents the ED to the artist
Third, we sought expert opinion in two ways. We submitted the comics for critique to a panel of information visualization/health communication experts that meets regularly at our university. The panel recommended changes to improve the clarity and cultural congruence of the visualizations. The digital artist made these changes. Then, a professional screenwriter edited the comic script to improve the flow of the language and storyline.
In our fourth and final step, we inserted the digital images into the social media platform, Instagram®. At the time of this project, Instagram® was one of the largest social media platforms used by adolescents in the United States. 24 Captions for Mari's Instagram® site were written and edited iteratively by investigators.
Part III: Collecting feedback
Study design and recruitment
Mari's Instagram® stories were a part of a larger intervention, titled Dr. Erica (Emergency Room Interventions to improve the Care of Adolescents), which is a 10-week pregnancy prevention text messaging program. The brand of Dr. Erica is that of a reliable caring ED physician who provides evidence-based sexual health information via personalized and interactive text messaging. Mari represents Dr Erica's younger cousin.
We conducted an IRB-approved pilot randomized controlled trial of Dr. Erica to assess its feasibility and acceptability. Information about the intervention has been published previously. 29 Participants were enrolled from the same pediatric ED as described above. Participants were eligible if female age 14–19, sexually active with a male in the prior 3 months, not wanting to become pregnant in the next year, and not used at last intercourse and were not currently using an effective form of contraception. Our exclusion criteria were similar to that mentioned above in the survey study with additional exclusion criteria, such as not having access to a personal mobile phone. A member of the research team enrolled participants with informed consent; we were granted a waiver of parental consent from our IRB.
Procedures
Participants were randomized 1:1 to the intervention arm (Dr. Erica) or control arm (standard referral to primary care provider). Intervention participants received 10 weeks of personalized and interactive text messages aimed to educate and motivate adolescent females to choose and initiate an effective contraceptive based on her personal preferences. As a part of the intervention arm, Mari’s Instagram® stories were texted to intervention participants. The stories were sent as an image rather than a link to Instagram. Five Mari stories were sent every other week, for a total of five messages.
For follow-up, participants completed either an online survey 12 weeks after study enrollment, which was 2 weeks after the last text message. To gather acceptability data on the Mari stories, participants rated the stories on a 10-point scale (0 being does not like and 10 being liked the most) and were asked to recall what they liked and did not like about the images. If participants did not complete the online survey, we conducted telephone follow-up. During the telephone follow-up, if they did not recall the stories, the research coordinator texted the Instagram image in real time as a reminder. Research coordinators did not audiotape the interviews but rather documented comments verbatim on an excel spreadsheet.
Data analysis
We used descriptive statistics to measure how much participants liked the Instagram stories. We then organized participant feedback to the images gathered via follow-up by online survey or phone call into the four types of peer support: companionship, emotional, informational, and tangible.
Results
Survey study
From May 2017 to August 2017, we enrolled 22 participants, the majority being age 18–19 (15, 69%), Hispanic (19, 86%), publicly insured (15, 68%), and had primary medical providers (12, 55%). Race was most often described as “Other” (14, 64%). More than half had a current sexual partner (12, 55%) and were currently using a birth control method (14; 64%), most often having used the pill (14; 34%) and shot (7; 15%). Four participants identified as a teen parent. Reasons for ED presentation included abdominal pain, sore throat, and injury.
Participants provided 352 text messages text messages. We rated each text in four categories, leading to 1408 peer support scores. Of the 704 scores rated by two people, approximately 56 scores differed by more than +/- 1 point to require iterative discussion. The mean message functional social support scores of the messages were 0.44 (companionship), 0.63 (emotional), 1.01 (informational), and 0.06 (tangible). Most rated texts scored a 0 (885; 63%) followed by 289 (21%) with a score of 1 and 231 (16%) with a score of 2. Examples of top scoring messages and the type of peer support provided by the message were as follows: (a) “I know it’s hard RN (right now) but it’s sooo worth it girl, come on we can walk that stage with our cap n’ gowns together, I love you” (companionship); (b) “If your partner doesn’t want to see you winning he is not the one for you” (emotional); (c) “If you go to a clinic, anything you say is confidential” (informational) and (d) “LMK (let me know), I can pick some [condoms] up for you at the clinic” (tangible). Additional examples can be seen in Appendix A. Examples of low scoring messages included those that could be conceived as having a negative connotation, such as “Trust NO ONE!” and “You are still a child.” We prioritized those texts with the highest scores for the next phase.
Creating illustrative digital sexual health visualizations
From September 2017 to May 2018, we designed five digital stories of Mari and her Instagram account titled, Mari tells it like it is. Each story incorporated 5–12 peer-authored quotes. The data visualization experts suggested edits such as changes to facial expressions, clothing choices, and scenery to reflect the local environment. The screenwriter edited storyline script; examples included expanding explanations and changes in tone. We inserted the final comic images into Instagram® along with a running caption. Figures 2 to 6 depicts examples of five sexual health visualizations.
Illustrative social media story.
Illustrative social media story.

Illustrative social media story.

Illustrative social media story.

Illustrative social media story.
Participant feedback
From June 2019 to July 2020, 39 participants rated the Mari Instagram® stories. The majority of these females were aged 18–19 (22; 59%), were identified as Hispanic (31; 79%), and chose “Other” for race (28; 72%). On a scale of 1 to 10, the Mari images were rated an average of 8.7 (median 9.0). Overall, the stories were found to be “educational,” “original,” and “relatable.” We organized verbal feedback of the Instagram stories into the four categories of peer support.
Companionship
Participants found that the Mari images were “super realistic” and “relatable.” As a 19 year-old female described, she could “hear her friends saying things like they said.” For another 17 year-old female, who was pregnant at the time of follow-up, she described how the images would be “useful” for her younger step-sisters, so they do not have to experience what she is “going through.”
Emotional support
The stories offered empathy and acceptance. As an 18 year-old female explained, “They felt real and it was easy to learn about these things without embarrassment and judgement.” Another 17 year-old female stated that the images “made me feel like someone cared about my health—like Mari was putting me and my sisters in our place.”
Informational support
Participants found the images “educational,” “original,” and “not too long.” They considered the content “useful” and “information that I can use later.” As a 17 year-old female explained, “I found it helpful that I would get to read scenarios of certain relationships and ways of using birth control.” Another 19 year-old female described how the Instagram stories “gave me information I didn’t know and made me realize I could start birth control.” For one 16 year-old female, however, some of the information was redundant, having known some of the information already but still wanting to learn more.
Tangible support
Participants did not often provide feedback of the images that referred to tangible social support. However, a 16 year-old female mentioned that the Mari stories “gave me words that made it (birth control methods) easier to talk about.”
Discussion and conclusion
Discussion
This study uses user-centered design methodology to capture the language of adolescents to illustrate sexual health visualizations promoting peer social support. By incorporating the language of adolescent “role models” (contraception users), we aimed to create an engaging storyline about a fictional character who provides evidence-based education, relates to our patients, and promotes healthy sexual behaviors. We utilized the advice, talents, and knowledge of a diverse group of experts in medicine, screenwriting, digital design, data visualization, and the end-user, the adolescents. In the final phase, we found that the digital visualizations were well received and providing a sense of perceived peer support to our local adolescent population.
Our work is novel in two salient ways. First, we used an innovative, reproducible, user-centered design strategy. By blending the principles of survey methodology with storytelling, we developed digital comic narratives using the linguistics and experiences of the adolescents who live in our surrounding community. This is particularly important in the creation of health-promotion media programs.58,59 While traditional mass media programs such as magazines and newspapers can reach large numbers of people, they can be insufficient to change attitudes and behavior change when they are non-dialogic and non-participatory. Media programs should consider incorporating peers and local community members to speak to the needs and experiences of the target audience, as their participation can also lead to designing more relatable, and in effective, impactful interventions.60–63 For example, in a recent literature review of culturally and contextually mobile health sexual and reproductive health interventions for Black and Latina women the authors concluded that we need to create programs that are “culturally and contextually tailored so that they align with lived experiences.” 64 The authors go on to explain that, when interventions that are developed with these components in mind, they can offer promising solutions in providing content to those who otherwise would not have access to such information.
Second, we aimed to amplify functional social support using a relatable form of digital technology with a goal to influence adolescent sexual behavior. One consistent factor affecting adolescent behavior is peer influence. 65 Many health behavior theories (e.g. Reasoned Action Model, Social Cognitive Theory) highlight the critical influence of perceived peer norms on decision-making. Our Instagram stories aimed to dispel sexual health misconceptions and reinforce healthy behaviors by using the words and advice of local peer role models. Given that peer support directly correlates with positive behavior change, our social media stories are meant to provide social support to our community and positively influence their future decisions. Social media, which is not technically considered mass media but rather new media, offers a unique vehicle to spread and target information. For example, provide social media and social networking sites have been shown to have numerous functions for LGBTQ individuals including expressing and constructing identity, managing bullying, and social activism.66–68 Even YouTube channels, which are easy to search and contain an abundance of free content, can facilitate LGBTQ individuals to learn about issues related to identity. 69
Interestingly, many of the peer-authored messages scored low in functional social support. Most often, teens conveyed informational support, such as how a clinic can provide confidential care, or emotional support, such as expressions of empathy and encouragement. On the contrary, the provision of tangible social support was rare, with few examples of messages providing material goods or financial support. This may be because tangible support, such as money for contraception or a ride to the clinic, is difficult to convey via text message or may not be a source that adolescents offer to others in their age cohort. This finding may mimic teen relationships, where informational and emotional support may be high, and tangible support may be lacking. Therefore, researchers should consider provide tangible support within adolescent sexual health interventions to maximize overall functional social support.
There are limitations to this study. First, we had a convenience sample size of 22 participants for phase 1 and 39 participants for phase 3; this will not represent all ED patients nor the general adolescent population, especially since our sample was skewed to older adolescents, predominantly Hispanic, and living in the local community around our particular hospital. Future studies could include a larger national population to develop visualizations that are generalizable to a larger audience. Second, our text message ranking system was developed by the authors and was not validated, although we used an established peer support theory. Third, the social media stories aimed to affect behaviors, and we have no data to show they directly changed behaviors; this will be part of a future study. Lastly, we understood that each female participant presented to the ED with a set of personal experiences and was likely to provide messages that were more meaningful in certain categories. For example, a participant who was satisfied with her current contraceptive but does not use condoms might more likely write representative messages in the category of “why I like my birth control” rather than “why to use condoms.” However, we believed that participants would rarely be representative role models in all categories; therefore, gathering example messages from a variety of participants would provide broad representation of individualized experiences and perspectives.
Conclusion
Technology advancements have led to dramatic shifts in the way peer social support can be communicated. Social media can be a powerful tool for medical providers to educate and motivate adolescents to improve their sexual and reproductive health behaviors. Yet, it is important that these illustrations and messages be in line with the current preferences and lifestyles of the adolescents we aim to engage. 70 With adolescents at the forefront of certain technology, promoting healthy sexual behaviors through relatable digital media is a promising strategy. This study demonstrates the use of a unique methodology to design illustrative digital comic strips that aim to promote healthy sexual behaviors and functional social support by using peer-authored sexual health messages. Using the methodology presented in this manuscript proved to be a creative way to incorporate the voices of our population, create engaging digital media, and be replicated by others to connect to their local population.
Footnotes
Acknowledgments
We would like to thank the adolescent females who participated in this study and the pediatric emergency department at New York-Presbyterian Children’s Hospital for their support. We would also like to thank Naira Hart (@nairahart) for our digital artwork.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Chernick was supported by the National Center for Advancing Translational Sciences, National Institutes of Health (NIH), through grant number KL2TR001874, and by the National Institute of Child and Health Development, through grant 1K23HD096060-01. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. This research was presented at the 2018 Pediatric Academic Society Annual meeting.
Author contributions
LC, PD, AE, SB, CW, JS, and MS conceived the study. AK, AG, and LC collected and analyzed the data. LC and AK wrote the draft; all authors reviewed and edited the manuscript and approved the final version.
Ethical approval
The ethics committee Columbia University Medical Center approved this study.
Informed consent
Participants in Phase 1 and 3 of this study provided informed consent.
Trial registration
Phase 3 of this study was a clinical trial, NCT03866811.