
Abstract
Objective
The aim of this study is to review the evidence for tailored eHealth weight-loss interventions, describing in detail: 1. how tailoring was implemented in these studies and 2. whether these tailored approaches were effective in producing weight loss compared with generic or inactive controls.
Methods
A systematic review was carried out. Five databases were searched up until 15 March, 2018, including: EBSCO, Science Direct, Pubmed, EMBASE and Web of Science, using combinations of the concepts ‘tailoring’, ‘eHealth’ and ‘overweight’.
Results
Eight articles relating to six interventions were accepted. Tailoring was carried out in a number of ways, based on, for example, anthropometric data, health-related behaviours (e.g. dietary intake, physical activity), goals (e.g. weight goal), theoretical determinants (e.g. confidence/willingness to change behaviours), psychosocial factors (e.g. social support) and participant location. Systems acquired data using strategies that ranged from online questionnaire administration, to the dynamic gathering of data from web-based diaries, websites, mobile applications and SMS messaging. Tailored interventions were more effective in supporting weight loss than generic or waitlist controls in four of the six articles. Effect sizes were very small to moderate, with evidence for fluctuations in effect sizes and differences of effect between tailoring and non-tailoring interventions, and between tailoring types, over time.
Conclusions
We contribute an enhanced understanding of the variety of methods used for the tailoring of eHealth interventions for weight loss and propose a model for categorising tailoring approaches.
Keywords
Introduction
There is an urgent need to identify effective and scalable strategies to address what the World Health Organization terms ‘the obesity epidemic’. Indeed, the number of overweight and obese individuals has increased from 857 million in 1980 to 2.1 billion in 2013. 1 However, we have yet to see strong evidence for a successful population-wide obesity intervention. In standard lifestyle interventions, behavioural therapy is delivered to participants by trained interventionists to support modification of diet and physical activity levels in an individual or group setting; it has been found to be effective in producing weight loss when compared with pharmacological strategies. 2 This approach is resource-intensive, requiring significant input from both the patient and the interventionist, and can be costly to deliver, which poses a challenge for widespread translation of these approaches. 3 Accessible and cost-effective interventions are necessary to bring about impact on a large scale. Two developments that appear promising for scalable, effective interventions are the use of eHealth tools in the delivery of interventions and tailoring of intervention content.
eHealth approaches to treating obesity
Research suggests that by delivering interventions via the Internet (eHealth), some of the cost and scalability problems of obesity interventions are mitigated.4,5 eHealth interventions can be deployed through websites, emails, text messages, monitoring devices, mobile applications, computer programmes, podcasts and personal digital assistants. 5 eHealth systems can set individualised goals for users, monitor diet and physical activity behaviours, and respond to data with personalised guidance, among other behaviour-change strategies.
To establish the viability of these systems for large-scale impact, research into the implementation and outcomes of eHealth interventions is needed. Hutchesson et al. 5 conducted a series of meta-analyses drawing on 88 eHealth weight loss or weight maintenance interventions. eHealth weight-loss interventions achieved modest weight-loss compared with no treatment (mean difference: –2.70 [–3.33, –2.08], p < 0.001; nine studies pooled in meta-analysis) or minimal treatment (mean difference: –1.40 [–1.98, –0.82], p < 0.001; 16 studies pooled in meta-analysis). Studies were found to be heterogeneous in both groups of pooled studies, I2 = 49%, p = 0.04 and (I2 = 72%, p < 0.001), respectively in terms of intervention strategy, technology usage and interaction style. eHealth interventions with extra features/behavioural components (e.g. self-monitoring, personalised feedback) or technologies (e.g. applications, texts or social networks) were more effective than standard eHealth programmes (drawing on either the Internet or podcasts only) (mean difference: 1.46 [0.80, 2.13], p < 0.001). 5 Arem and Irwin 6 also found the Internet-based weight-loss interventions included in their review to be heterogeneous. This was both in terms of the nature of the intervention (e.g. contact with participants, sample size and study duration) and their outcomes, with weight loss ranging from <1 kg to 4.9 kg. Crucially, since the interventions included in these reviews differed from each other in so many ways, it was impossible for the authors to make specific recommendations regarding which intervention components were necessary to bring about weight loss.
These effect sizes are modest in comparison with what may be achieved using traditional behavioural approaches. The modest weight losses demonstrated by the Hutchesson 5 review are several times less than in-person interventions. For example, an in-person behavioural weight-loss intervention of 4–6 months of weekly group-based lifestyle counselling and intensive dietary restriction showed that participants lose on average 10.7 kg. 7 These may be due in part to the varying intensity of behavioural-change strategies, personalisation strategies and supportive accountability provided by a human counsellor. To ascertain the effective components in these interventions, it is necessary to draw together the interventions that implement a common strategy.
A significant challenge to the wide-scale usage of eHealth interventions is that they typically suffer a steep decline in usage over the course of the intervention and have poor completion rates. 4 Neve et al. 8 highlight that use of eHealth technological components (both frequency and duration) may prove a useful metric to enable the establishment of an ‘optimal dose’ required for behaviour change. The review demonstrates that the higher the number of log-ins, self-monitoring occasions, chatroom attendances and bulletin board posts, resulted in greater weight loss, and this pattern was evident in the majority of studies included. Participant attrition is a key issue in assessing the efficacy of Internet-based interventions, as low levels of completion compromise the feasibility of implementing such interventions on a larger scale.
These findings provide promising support for the efficacy of eHealth interventions for weight loss.5,6 They confer an additional advantage over traditional methods, for example, in-person behavioural counselling in delivering weight-loss interventions in a cost-effective, effectual manner suited equally to the individual and at a scale needed to address the global obesity epidemic. Efforts to investigate specific strategies that are effective for weight loss, which address the issues of modest effects and low levels of engagement are needed. Delineating the precise strategies within eHealth efforts that are effective in bringing about the greatest decrease in weight requires a granulated examination and specification of the various components, modes of delivery, technological features and behavioural theory that inform these eHealth approaches, as well of usage of technological components as part of these efforts. Web-based weight-loss interventions have been reported as being less effective than face-to-face interventions,6,9 however, enhanced web-based interventions (e.g. more interactive and tailored) are more efficacious than basic, more generic interventions (e.g. purely informational). 9 Web-based interventions may prove to be clinically effective and feasible if they can mimic some of the tools and strategies of the in-person interventions, while reaching a larger population. 6 Enhancing web-based interventions through tailoring the eHealth interventions to characteristics of the user or patterns of behaviour is supported by a recent systematic review that evaluated web-based interventions for weight loss and maintenance. 9
Tailoring as a strategy to enhance eHealth interventions
Tailoring is a process whereby the provision of information, advice and support is individualised to the user. 10 Noar et al. 11 explain that the process of tailoring involves an assessment of individual-level characteristics gathered by a person or self-administered (input: the basis for tailoring). This information then gets processed by either a human (human tailoring), or an expert system (computer tailoring) that uses algorithms to select content (i.e. text, images, recommendations and intervention messages) from an expert-developed database for the individual (tailoring process). Tailored material (output) is adapted using a variety of strategies to be delivered to the individual via multiple delivery modes.
Compared with non-tailored, generic materials, tailored health-messages command greater attention and are more likely to be read, elaborated upon, recalled and understood. 12 As such, tailored health-messages are considered to be processed more deeply, contain less redundant information, and are perceived more positively by health consumers. 13 Tailoring strategies can range from relatively simple, for example, employing the user’s name, to the more complex, for instance adapting content to personally relevant variables. 14 Work has also been undertaken to draw together concrete definitions of tailoring strategies.13,15,16 Krebs et al. 17 add to this by defining ‘dynamic tailoring’ as the assessment of intervention variables prior to each feedback and ‘static tailoring’ where one baseline assessment provides the basis of all subsequent feedback.
Impact of tailored approaches on health outcomes
While there is little evidence for the impact of tailored eHealth interventions for weight loss, evidence has accrued for the effectiveness of tailored web-based approaches to health interventions. For example, Lustria et al. 10 conducted a meta-analysis to assess the impact of tailored web-based interventions targeting physical activity, nutrition, smoking/tobacco use, drinking, medication adherence (asthma management), stress management and faecal soiling (encopresis). Forty experimental and quasi-experimental studies were analysed and web-based tailored interventions effected significantly greater improvement in health outcomes compared with controls both at post-testing, d = 0.139 (95% CI = 0.111, 0.166, p < 0.001, k = 40) and at follow-up, d = 0.158 (95% CI = 0.124, 0.192, p < 0.001, k = 21). While these results are encouraging, (similarly to the eHealth reviews discussed earlier5,6) the authors identified that there was great variability in how tailoring was carried out among their included articles, including differences in intervention features, formats, and levels of interactivity.
A series of meta-analyses by Krebs et al. 17 also assessed the effect of 88 computer-tailored interventions, using computer, print, or telephone communication channels that focused on four health behaviours: smoking cessation, physical activity, diet, and mammography screening. A significant, small effect size (Hedges’s g = 0.17) was found for tailored interventions, taking the average of the four health behaviours. This is encouraging evidence for tailoring as an approach to health behaviour change in general, but more specific approaches, honing in on one specific outcome may allow for in-depth conclusions to be drawn, considering that the determinants of health behaviour change interventions differ by outcome.
These studies provide support for tailoring as a strategy for use in health behaviour-change interventions, but we argue that previous research on tailored health interventions has focused primarily on understanding whether tailoring works, rather than focusing on how it works, or which approaches are most useful under which circumstances.12,15
The current study
Without meticulous description of intervention designs, the science and practice of tailoring within eHealth intervention design and implementation cannot be advanced. Previous work on tailoring has met with difficulty in differentiating the range of approaches to tailoring, differences in modality, intervention features and components. 10 In addition, Harrington and Noar 16 have called for improved reporting standards in tailored research.
The aim of the current paper was to review the evidence for tailored eHealth weight-loss interventions. We aim to describe in detail: 1. how tailoring was implemented in these studies and 2. whether these tailored approaches were effective in producing weight loss compared with generic or inactive controls. Specifically, we sought to identify what individual factors were assessed as part of the tailoring process, what tailoring strategies and eHealth tools were used, how engagement with eHealth interventions was conceptualised and whether tailoring increased this and, lastly, whether tailored approaches produced larger effect sizes than generic information and waitlist control approaches for weight loss.
Methods
Design
Systematic review of pre–post intervention trials with a control group, following Cochrane methodology and Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (see Appendix A). 18 The review was registered with PROSPERO (CRD42017072901). 19
A systematic review of tailored eHealth interventions for weight loss was carried out, with a title and abstract screening phase (Phase 1) and a full text screening phase (Phase 2).
Eligibility criteria
All papers that were deemed relevant at Phase 1 were included if they were quantitative peer-reviewed articles, published at any time, in the English language, with a pre-test–post-test intervention design (either randomised controlled trials (RCT) or pilot study) using a control comparison group (generic or inactive) approach. Interventions of any duration that aimed to bring about weight loss in overweight or obese (Body Mass Index (BMI) >25), free-living participants without specified clinical disease were included. Articles were required to have a stated tailored approach, which we operationalised as ‘if the intervention was personalised, and based on an assessment of individual characteristics’. 20 The intervention was required to be behavioural in nature (e.g. aimed to change diet and physical activity), and delivered primarily via the Internet (Internet-based); in-person measurement of weight was permissible, as was briefing to randomisation group components. Articles were excluded if the intervention was not tailored at the individual level (e.g. generic in nature or tailored based on shared rather than individual characteristics, e.g. gender tailoring), not delivered online (e.g. delivered in-person), not aiming to change behaviours (e.g. pharmacological), and if the primary aim of the intervention was not specifically for weight loss; however, articles were included if there was more than one main aim, as long as weight loss was stated as one of the aims. Articles were excluded if they stated that the participants had a clinical population (e.g. type 2 Diabetes patients who may have been taking medication to control their condition), or if they were not published in the English language. Authors of studies that met the criteria but did not report the body weight of participants at baseline and follow-up (e.g. reported the BMI only) were contacted in an attempt to include them in the review.
Sources and Searching
Searches were run in December 2016 in five databases, including: EBSCO, Science Direct, Pubmed, EMBASE and Web of Science. Combinations of the concepts ‘tailoring’, ‘eHealth’ and ‘overweight’ were searched as part of the search strategy. For example, EBSCO search included the following combination: TI personalis* OR individualis* OR tailor* OR custom* AND AB (ehealth or e-health or website or web or web-based or website-based or online or Internet) AND SU (overweight or obesity or obese or weight management or weightloss or weight loss or diet* or physical activity). Searches were re-run on 15 March, 2018. An example of the search strategy is included in Supplemental material (Appendix B). Hand-searching was conducted of reference lists of included articles, systematic reviews and meta-analyses of eHealth interventions for weight loss, as well as in the Journal of Medical Internet Research.
Data extraction
Data extraction was conducted by KR. Fifty per cent of the extracted data were checked for accuracy by author SD and 50% by author CL. Two accepted articles had associated adjunctive articles, published separately but reporting details of the development of the tailored eHealth weight-loss intervention. Data from these articles were also included in the extraction and qualitative synthesis, in tandem with the original accepted article. The extracted information included participant information, intervention information and weight-loss outcomes. This included details on study setting; study population and participant demographics and baseline characteristics; details of the tailoring intervention and control conditions; study methodology; recruitment and study completion rates; outcomes and times of measurement; suggested mechanisms of intervention action; and information for assessment of the risk of bias. Specific to the process of tailoring, we identified the individual factors that were assessed as part of the tailoring process, how the assessment was conducted (e.g. what eHealth technology/modes of delivery were used), how often it occurred (e.g. static tailoring or dynamic), how the message output was devised, what specific tailoring and behavioural strategies were implemented, how engagement with the eHealth intervention was conceptualised and measured, whether tailoring increased this and, lastly, whether tailored approaches produced greater weight loss compared with generic or waitlist approaches. Authors were contacted for any missing information.
Data analysis
There were two components to data analysis: qualitative and quantitative synthesis. Qualitative synthesis involved examining how tailoring approaches were conducted within each intervention using information in each article’s intervention description and any corresponding intervention development articles.21,22 As part of this process, terms listed in Harrington and Noar 16 were used to identify the tailoring strategies described. These included the following terms: ‘content-matching’ (adapting intervention content based on theoretical determinants), ‘feedback’ (providing messages to individuals about their psychological or behavioural states, which may involve description of objective data back to participant (‘descriptive feedback’), comparing their data to norms (‘comparative-normative feedback’), their previous states (‘comparative-progress feedback’) and providing an interpretation or judgement of their data (‘evaluative feedback’) and ‘personalisation’ where recognisable information relating to the participant is relayed to them, including the use of their name (‘identification’), telling participants that the intervention content has been created especially for them (‘raising expectation of customisation’) and framing messages in a context that is meaningful to them, e.g. through gender-, cultural- or ethnicity-related cues (‘contextualisation’).
Quantitative synthesis involved evaluating the effect of the tailored eHealth interventions on weight loss: effect sizes were calculated to estimate the difference between the intervention and control groups (both active and waitlist controls). Effect sizes for weight change at follow-up assessments were calculated based on the mean pre–post change in the treatment group minus the mean pre–post change in the control group, divided by the pooled pre-test standard deviation (SD). 23 In one case, the post-test SD was used as a proxy where the pre-test SD was not reported. 24 A pooled SD was calculated using Cohen’s 25 formula, squaring the baseline SD of weight of the intervention group and adding the squared baseline SD for weight for the control group, and taking the square root of these. Effect sizes are therefore reported in SD units of change. Changes between the intervention and control were considered to be small (0.2 to <0.5); moderate (0.5 to <0.8) or large (>0.8). 25
Quality appraisal
Quality of methodology was assessed by authors KR and SD using the Cochrane Collaboration’s tool for assessing risk of bias for RCTs. 26 Bias was assessed as a judgement (high, low, or unclear) in the following domains of bias: selection, performance, detection, attrition, reporting and other bias. In this review, as the outcome of significance was weight, we included an assessment of measurement bias for weight as part of the quality review. Studies using self-reported weight, or using one-off (not averaged) weight measurements were considered to have an increased risk of measurement bias.
Results
Initially 516 articles were captured in the searches and a further 14 records were identified from hand-searching reference lists of accepted articles and relevant systematic reviews.5,6,8 Following the removal of duplicates (N = 218), there were 312 articles for title and abstract screening, of which 80 were subjected to full text review. Searches were re-run in March 2018, which led to an additional three articles suitable for full text review.27–29 Articles were excluded due to relating to wrong outcomes (e.g. cardiovascular risk, BMI), wrong study design (e.g. review articles, face validity evaluations); being an RCT development article; wrong intervention aims (e.g. aiming to increase physical activity, diabetes prevention); wrong route of administrations (e.g. in-person), wrong population (e.g. those with diabetes mellitus) and wrong source (e.g. conference abstracts). A systematic review of tailored eHealth weight-loss interventions ultimately yielded a total of eight articles,21,22,24,30–34 describing six interventions. See the PRISMA flow diagram below (Figure 1).

PRISMA flow diagram.
A summary of the included studies is presented in Table 1. There were 14 intervention arms, 2 interventions had three arms, and 4 interventions had two. There were N = 4356 participants (baseline), with 2243 assigned to the intervention groups, and 2113 assigned to the control groups. Participants were recruited from the general population (82.5%), university students (10.5%) and university staff (7%). The mean retention rate to final follow-up was 39.04%. The average age of participants was 37.11, SD = 7.54. Their mean BMI at baseline was 30.06, SD = 4.05. They were mostly female, 82.18% and Caucasian, 56.67%. Studies were published between 2006 and 2016. There were five RCTs30–34 and one randomised pilot study 24 with the majority (N = 5) conducted in the USA24,30–33 and one in Europe. 34 The intervention durations ranged from 5 weeks to 24 months, with the average length being 24.5 weeks. There was an average of 2.33 follow-ups where participants’ body weight data were collected. Four of the six studies measured weight objectively24,30,33,34 with two relying on self-report methods.31,32 Four out of these six studies compensated participants for taking part.24,30,33,34
Characteristics of eligible studies.

Note: CT = computer tailoring; HT= human tailoring; PA= physical activity; M = mean; SD = standard deviation; SMS= short message service (text); NR= not reported.
There were two articles considered to be of low risk of bias, three of moderate quality, and one of high risk. Random sequence generation, allocation concealment and blinding of participants and personnel were judged to be adequate strategies in three articles, blinding of outcomes assessment was described in two articles. Five articles were deemed to be low risk in regards to reporting incomplete outcome data. Two articles had published protocols and thus were considered to have a low risk of bias for selective outcome reporting. Two articles relied upon participants’ self-reported weight for their analysis, and this was considered to have a high risk of bias in relation to the measurement and reporting of weight. One was considered to be low risk owing to the inclusion of two objective measurements of weight and taking the average. A summary of the risk of bias results is included in Figure 2.

Risk of bias graph for quantitative articles (n = 6). (a) Summary of included articles using Cochrane’s Risk of Bias tool. (b) Summary of risk of bias across studies.
How was tailoring implemented?
There were six interventions included in the review, referring to 14 intervention arms, four articles compared computer tailoring to generic information control,24,32–34 or to waitlist control;24,31 one compared human tailoring (devised by human health counsellors) to generic information control; 33 one used a combination of computer tailoring and human tailoring 30 compared with a generic information control.
Computer tailoring, when feedback is delivered by a system, was implemented through a tailored website devised by Tailorbuilder 34 and a tailored expert system. 32
What was tailoring based on and how was it gathered? (Tailoring input)
Theoretical models of behaviour change are integral to tailoring and so any difference in theoretical components that provides the basis for the tailoring process may underlie any similarities or differences in intervention outcomes. Four out of six studies mentioned one or more theories that informed the development of the intervention: Social Cognitive Theory; 31 Cognitive Behavioural Theory; 33 Self-Regulation Theory, the Theory of Planned Behaviour, the Precaution Adoption Process Model; 34 and Behaviour Change Theory comprising Social Cognitive Theory, Control Theory, Operant Conditioning, Ecological Theory, and Social Network Theory. 30 Tailoring was based on anthropometric data and personal characteristics including age, height, weight, gender,31,32 family history and prior weight-loss experience; 32 behaviours including dietary factors, e.g. calories, level of physical activity,24,30–32,34 theoretical concepts such as future weight goals,31,32,34 physical activity and diet goals, 30 advantages and disadvantages of weight management, confidence and willingness to change behaviours, 34 physical location, 30 whether self-monitoring occurred; 24 high-risk habits, 24 health-related habits, barriers to physical activity; as well as a range of psychosocial characteristics around stress management, attitudes to overweight people, comfort eating, and sources of motivation to lose weight, among others 32 (see Table 2 for further details).
Summary table of tailoring methods.

Note: CT = computer tailoring; HT= human tailoring; PA = physical activity; M = mean; SD = standard deviation; SMS= short message service (text); NR= not reported.
Tailoring input, which provided the basis for the process of tailoring was gathered using online questionnaires at baseline,31,32 web-based diaries, 33 via purpose-built tailored website, 33 study-designed mobile applications, 30 SMS messaging, 29 Facebook, and emails from a remote health coach. 30
Self-tailoring or ‘customisation’ 15 reflected personal preferences, and was based on desired features, e.g. whether they wanted a newsletter, 31 their desired intervention mode of delivery, 31 and how often users wanted feedback, tracking and goal reviews. 30
How was tailoring conducted? Computer tailoring
Dynamic tailoring (based on dietary or physical activity behaviours or weight, self-monitoring status or location) was conducted through daily and/or weekly input24,30,33 or less regular input and based on theory, e.g. recommended every two weeks 34 or a self-determined pattern of tracking and feedback. 30 Static tailoring involved a process of distributing an online questionnaire at baseline.31,32
Two tailoring approaches were explicitly named and described: a tailored website 34 and a tailored expert system. 32
One intervention delivered computer-tailored feedback and human tailoring via health coaches who also delivered feedback, 30 and whether or not participants received the intervention depended on the usage of these components. In the other instance, daily feedback appeared to be automated as messages were programmed and feedback was immediate, however it was not explicitly stated who or what devised the weekly personalised messages; an automated system appeared to have gathered daily behavioural data and this was provided to participants through a secure link delivered by Facebook message. 24 The computer-tailored feedback in Tate and colleagues’ study 33 was based on the participants’ responses and matched with a response from a bank of messages previously devised by experts; a series of decision rules ensured that automatically generated feedback was provided on the webpage.
As an example of an in-depth level of computer tailoring, Rothert et al.
32
described the action of the tailored expert system in their intervention: participants reporting a family history of a particular disease received information regarding the connection of obesity to this class of diseases; participants who reported greater ability to change diet than physical activity received more dietary advice; specifically cited barriers and lack of efficacy were addressed with messages tailored to those issues; psychosocial stress was compared with reported coping abilities and accompanied with tailored stress management advice; and participants who reported that overweight individuals lacked willpower were given messages attempting to change this perception to a more controllable, external attribution (p. 268).
Human tailoring
Tate et al. 33 drew on human tailoring by human counsellors who had behavioural weight-loss experience and degrees in nutrition, psychology, health education, and exercise physiology. Feedback was based on their clinical judgement in interpreting the participants’ self-reported weekly weight, daily caloric intake, use of meal replacements and exercise, in their electronic, web-based diaries on the study website. The content of feedback for approaches involved comparative-progress feedback for weight, comparative-progress feedback on calorie goals consumed and burned compared with individualised diet and exercise goals, behavioural strategies for improving adherence to self-monitoring diet and exercise, overcoming barriers, and motivation or praise depending on logging frequency. This detail was not provided in the other study.21,30 Based on the description provided we determined that feedback was based on app usage, behaviours and progress to goals.
How tailored interventions were delivered
A range of modes were used in the delivery of tailored interventions. Websites were used in all studies.24,30–34 Two used SMS messages as well as Facebook.24,30 Two studies used humans to tailor information: one used health counsellors who contacted participants via email 33 and one used health coaches who could instant message, telephone or video-call participants. 30
Type of Tailored Strategies and Output
Tailoring strategies were identified from the descriptions in the articles. Content-matching,31,32,34 evaluative feedback,24,30,31,33,34 descriptive feedback,24,34 and comparative-progress feedback,24,30,33,34 identification, 34 contextualisation, 30 as well as self-tailoring (customisation)30,31,34 and personalisation 34 were implemented by a range of eHealth systems. Location-tailoring was also used. 30
Output typically consisted of feedback on weight loss, physical activity and diet (e.g. calories burned and consumed) compared with individualised diet and exercise goals.24,30,31,33,34 Visual graphs of progress, behavioural feedback, differential behaviour-change strategies, personalised certificates and personal reward plans were also delivered to participants. 34 Output also included a personalised nutrition plan and newsletter around their goals. 31 Feedback on behaviours such as daily self-monitoring also featured, 24 as did a weight management plan with behavioural strategies (e.g. action plans) matched to the individual. 32
Did tailoring work to increase engagement?
Four studies did not explicitly define engagement within the context of their intervention. As such, there was no consistent method of conceptualising and measuring engagement with eHealth interventions. Some studies reported usage metrics such as number of log-ins or use of eHealth features e.g. web-based behavioural diary, 33 registration to a website, 31 while others used process evaluations using subjective participant reports of amount of provided material read. 32 One study drew on both online module visits and subjective process measures. 34
Engagement was explicitly defined in Godino et al. 27 and also in Napolitano et al. 24 Godino et al. 30 defined it as the sum of a participant’s recorded interactions on the study Facebook page (e.g. a post, comment, or like) and mobile apps (e.g. entry of the number of steps taken per day), text messages sent and replied to, and communication with the health coach between each study measurement. Napolitano et al. defined engagement as the number of times participants ‘liked’ a study-related post, posted a comment, and RSVP’d to an event. 24 Tate and colleagues 30 examined log-in frequency and number and use of online diary submissions, counting the number of weeks where behavioural diaries were submitted.
Two articles conducted a process evaluation, capturing participants’ subjective views of the intervention through self-report questionnaires.32,34 Rothert et al. 32 reported that the tailored group responded more favourably than the information-only group for each item, including reading the intervention information completely; rating the materials as more helpful, more personally relevant, and easier to understand; and reporting that they would recommend programme to others, all ps = 0.0001. In research by van Genugten et al. 34 the tailored intervention group also perceived the material to be more personally relevant, and found content to be more novel than those in the generic information group, ps < 0.01, but contrastingly reported that they read less of the information, p < 0.001. They perceived the length of the information as less appropriate than those in the generic group, p = 0.01. There was no difference among groups in their ratings of usefulness of the information, attractiveness of the design, appreciation of the tool, whether they would recommend it to others, and overall rating.
Did tailoring support weight loss compared with control conditions?
A summary of the intervention groups compared with the controls is provided in Table 3.
Summary table of results of included studies on weight loss.
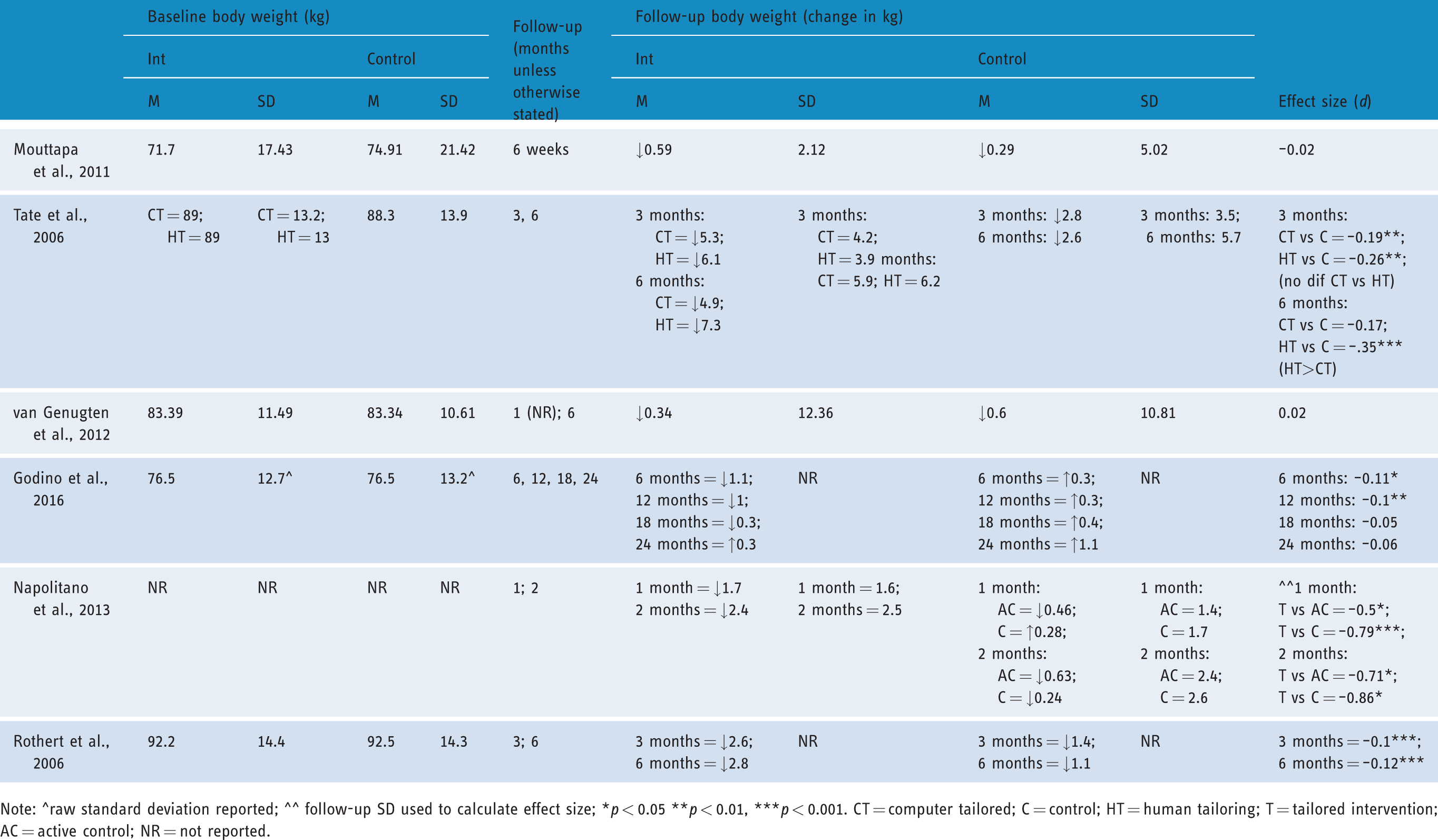
Note: ^raw standard deviation reported; ^^ follow-up SD used to calculate effect size; *p < 0.05 **p < 0.01, ***p < 0.001. CT = computer tailored; C = control; HT = human tailoring; T = tailored intervention; AC = active control; NR = not reported.
Four out of six articles found positive effects for tailoring on weight loss when compared with generic or waitlist controls.24,30,32,33 Two articles found no difference between the intervention and control (waitlist 31 and generic information 34 ). Follow-up time points ranged widely from 1 month to 24 months.
The effect sizes denoting the mean difference in weight between intervention and the control groups ranged from −0.02 to −0.86 but in general are very small to small. 25 In the only article that compared tailoring types, there was no difference between human tailoring and computer tailoring at 3-month follow-up; both resulted in statistically significant weight loss compared with the control group. However, at 6 months, human tailoring was still effective in producing weight loss compared with the control, but this was no longer the case for computer tailoring. 33 Napolitano et al. 24 found the largest effect between the tailored vs waitlist control conditions, d = −0.86, followed by the difference between the tailored and generic information, d = −0.71.
Godino et al. 30 found a significant difference between groups at 6 month and 12 month follow-ups, with the tailored intervention resulting in 1.33 kg more weight loss than the general information control at both 6 and 12 months (p < 0.05), but there was no significant difference at 18 or 24 months, where ultimately the effect size at 24 months was −0.06. Rothert et al. 32 found a significant difference between groups at 3 and 6 months, (mean weight loss for the tailored groups = 2.6 and 2.8 kg, respectively, ps < 0.001) favouring the intervention group, which used a tailored expert system.
Discussion
Summary of key findings
A systematic review of tailored eHealth weight-loss interventions was conducted on six interventions, outlined in eight published articles, to describe how tailoring was implemented, and whether it was effective in producing weight-loss. Tailored interventions were found to be more effective in supporting weight loss than generic or waitlist controls in four of the six articles. Effect sizes were very small to moderate, with evidence of fluctuations in effect sizes and differences of effect between tailored and non-tailored interventions, and between tailoring types, over time.
We note the diversity of approaches, input and technology used in tailored interventions; tailoring included a range of approaches including computer tailoring (using purpose-built tailored websites e.g. using TailorBuilder 34 and tailored expert systems 32 ), human tailoring (by remote trained health counsellors 33 ) and a combination of the two techniques. 30 Tailoring was based on a range of inputs, including anthropometric data (e.g. weight) and personal characteristics (e.g. age, prior weight-loss experience), behaviours (e.g. dietary intake, physical activity), goals (e.g. weight goal), theoretical determinants (e.g. confidence/willingness to change behaviours) psychosocial factors (e.g. stress management, social support) and location. A range of tailoring strategies was implemented, including evaluative- and comparative-progress feedback and content-matching, as outlined by Harrington and Noar. 16
Tailoring input was gathered using a variety of technological modes and included static processes of data collection from online questionnaires at baseline.31,32 Dynamic processes also occurred where rolling input was gathered from web-based diaries, 33 via a purpose-built tailored website, 34 study-designed mobile applications 30 and SMS messaging. 24 Conceptualisation of engagement with tailored interventions was not uniformly defined. Our findings suggest that tailored materials were rated by participants as more personally relevant, more helpful, easier to understand, more likely to be recommended to others, and more novel than those in the generic information group.
The first goal of this review was to describe how tailoring was implemented in eHealth interventions. We have described a range of methods, inputs and technology used as part of tailored interventions. Previous reviews describing eHealth interventions have also found heterogeneity in approaches, so this was no surprise given the ubiquity of the Internet and the range of delivery options it affords.5,6 With this advance in delivery methods comes new opportunities for tailoring health information, and we have found that tailoring is being increasingly used in innovative ways. However, if we are to build the science of tailoring it is imperative that the strategies reported in existing tailoring specification efforts15,16 are used. In addition, the input or basis for tailoring should be specified as well as who/what devises tailoring output.
In this vein, our review has attempted to describe the range of tailoring approaches delivered by eHealth means. In Kreuter’s 35 much cited original definition, tailoring is defined as the provision of individualised information, advice and support based on the participant’s known characteristics, behaviours or scores on relevant theoretical constructs. To aid the conceptualisation of tailoring in this context, we devised a model of tailoring depth, which we refer to as deep- and surface levels of tailoring (see Figure 3). This model is by no means exhaustive but we feel it is a step in the right direction in terms of differentiating between types of tailoring input to provide the basis for tailoring. It incorporates concepts discussed by Resnicow et al. in developing culturally sensitive public health interventions. 36 These concepts include surface structures, in other words relating to observable or behavioural characteristics of a population, and deep structures, relating to psychosocial, cultural and historical factors of a target population. This model indicates the distinctions made when the process of tailoring is based on behaviours or observable factors and when it is based on theoretical constructs, and allows for a combination of these. This builds upon Morrison’s assertion that tailoring strategies can range from relatively simple e.g. employing the user’s name, to the more complex, e.g. adapting content to personally relevant variables. 14 Deep-level tailoring refers to tailoring message content based on theoretical determinants of a specific health outcome, and the content that is delivered aims to modify these through strategies, for example like content-matching and evaluative feedback. In our review, input for deep-level tailoring was captured using a questionnaire at baseline (static tailoring). 32 For example, participants who reported a greater ability to change their diet at baseline compared with those who reported greater ability to change their physical activity received more dietary advice. 32 Deep-level tailoring was also conducted in a dynamic manner, gathering theory-based input via modules, using more than one assessment point, in order to ensure the intervention remained suitable to the needs of participants. 34 This is referred to as ‘re-tailoring’ where new information from participants is obtained and feedback given at follow-up time points. 37 It was recently found that participants disengage from eHealth interventions because they believe they are no longer relevant to them and their needs. 38 As such, a more continuous process of adapting and delivering content to the individual may be a promising route.

Model of tailoring depth.
Surface-level tailoring is a more concrete but simpler process, when tailoring is based on participants’ (ongoing) self-reported behavioural data, e.g. amount of physical exercise or dietary intake, and evaluative or comparative-progress feedback is delivered on this basis with the aim of keeping participants on-track with their behavioural goals. We suggest that this type of tailoring is no less important, but is conducted on the basis of behaviours or observable factors, typically relying on more frequent input (e.g. daily or weekly). This process aligns with self-regulation theory in that it enables the participant to learn to self-monitor and regulate their behaviour in line with their goals. 39 There may be a fundamental difference in the mechanisms at play behind this tailoring approach compared with deep-level tailoring, but this will need to be tested empirically in future research.
Tailoring may initiate processes of behaviour change, and it is possible that these processes in turn influence the efficacy of, and engagement with tailored interventions. Dynamic processes of tailoring, including movement between surface and deep level, or by tailoring type (e.g. human or computer), must be examined in relation to the efficacy of the intervention. For example, in the only study to examine human vs computer tailoring, both of these groups were effective at 3-month follow-up, however at 6 months, the human-tailoring group had significantly greater weight loss than the control. 33 This indicates the possibility that over time, the effects of tailoring will vary, and this variation may be related to an interaction on intervention-type by intervention-time. For example, at some intervention phases it may be more effective for a computer-tailored vs a human-tailored intervention to be implemented. This is linked to the suggestion that interactivity should be considered in developing effective eHealth interventions.9 This also highlights the concept of engagement, an under-considered factor in the research design or assessment of factors influencing intervention efficacy. We note that engagement was not explicitly defined in the majority of included studies (N = 4), and among those that did, it was conceptualised in a variety of ways mostly in relation to interaction with study-related content but also through process evaluations of the interventions.
This is in line with how engagement has been conceptualised in eHealth interventions – in terms of both participant experience and behaviours. 40 Future efforts to examine tailoring in eHealth interventions should measure engagement both in terms of participants’ objective usage of intervention components (e.g. behavioural- through log-in metrics, usage data) and subjective experience (e.g. through process evaluations, participant interviews or surveys). This will enable an assessment of the extent to which tailoring (and indeed other intervention features and components) works the way it is theorised to (e.g. via mechanisms of increasing attention, increasing self-referential thinking 15 ) and will provide a platform for future efforts to develop enhanced tailoring approaches addressing these mechanisms.
The second aim of the review was to establish whether tailored eHealth interventions result in weight loss compared with a generic control. Effect sizes were modest, comparable to other reviews in health behaviour change.10,17 However, it has been shown that modest weight loss (3–5% of pre-test body weight) is enough to have a beneficial health impact, e.g. reducing blood pressure, HbA1c, triglycerides and LDL cholesterol 41 and so, even modest effects are desirable.
Four out of the six studies found beneficial effects for the tailored arm of eHealth weight-loss interventions. The two studies that found no effect were less intensively focused on weight loss, as both had a further aim in addition to weight loss, with Mouttapa et al. aiming to additionally provide a dietary intervention 31 and van Genugten et al. to also prevent weight-gain. 34 While they met the criteria for the study, these findings suggest that the intensity of the intervention plays a key role, for example, in the study by van Genugten et al., even though the intervention was rigorously developed using behaviour change theory, the intervention could be finished within 90 minutes. 34 This may suggest that though tailoring was not found to be successful in that case, it may have been that the behavioural ‘dose’ of the intervention was not high enough. The other studies suggest that the effect of tailored eHealth interventions for weight loss is effective up until 1 year with no evidence at follow-up after this point.
Limitations
The number of completed studies using tailored strategies and the Internet to support weight loss in our results belies the number of studies available for review. Despite significant effort, we were unable to secure data on weight for four studies, as weight was not reported in the published record or provided on request, and our results must be considered in this context.
Our review featured participants predominantly from the general population (82.5% of participants) and this suggests that effective tailored approaches can be delivered via the Internet in a scalable manner for weight loss. However, we did not include interventions addressing weight-loss maintenance or weight-gain prevention as part of this review, which are also important foci for population-wide obesity strategies. We note that these are important areas deserving of research attention, however interventions that address these aims differ in intensity to those addressing weight loss and so we advise a delineation of behaviour type to explicate if and how tailoring is effective. The use of tailored eHealth tools in weight-gain prevention and weight-loss maintenance should be examined in future work as we attempt to support both those at risk of becoming overweight and those who need to maintain weight loss in a cost-effective, scalable and effective manner.
Conclusions
eHealth interventions for weight loss are promising in terms of being scalable and effective, 7 but it is necessary to find strategies that help eHealth interventions channel the effectiveness of traditional in-person behavioural counselling approaches.2,7,42 Tailoring is one approach that shows promise. We have found tailoring to have a small but beneficial effect on weight loss in four out of six studies in this review, yet tailoring approaches varied considerably even for one clearly defined health outcome (weight loss) and mode of delivery (Internet). To ameliorate this going forward and to build on previous research, we propose a model of tailoring depth, suggesting that there may be conceptual differences in tailoring approaches. Concepts of deep- vs surface-level tailoring could be tested experimentally to assess the mechanisms or effects of tailoring on the basis of input type, be it theoretical determinants, behavioural input or other tailoring input type. In order to develop the science of tailoring within the domain of eHealth interventions for behaviour change, it is vital to improve research designs (e.g. use tailoring vs generic control group) and methodologies (e.g. use the tailoring strategies and guidelines recommended in this field) 16 and in the wider domain of health behaviour change (e.g. by reporting behaviour-change techniques). 43
Supplemental Material
Supplemental Material1 - Supplemental material for A systematic review of tailored eHealth interventions for weight loss
Supplemental material, Supplemental Material1 for A systematic review of tailored eHealth interventions for weight loss by Kathleen Ryan, Samantha Dockray and Conor Linehan in Digital Health
Supplemental Material
Supplemental Material2 - Supplemental material for A systematic review of tailored eHealth interventions for weight loss
Supplemental material, Supplemental Material2 for A systematic review of tailored eHealth interventions for weight loss by Kathleen Ryan, Samantha Dockray and Conor Linehan in Digital Health
Supplemental Material
Supplemental Material3 - Supplemental material for A systematic review of tailored eHealth interventions for weight loss
Supplemental material, Supplemental Material3 for A systematic review of tailored eHealth interventions for weight loss by Kathleen Ryan, Samantha Dockray and Conor Linehan in Digital Health
Supplemental Material
Supplemental Material4 - Supplemental material for A systematic review of tailored eHealth interventions for weight loss
Supplemental material, Supplemental Material4 for A systematic review of tailored eHealth interventions for weight loss by Kathleen Ryan, Samantha Dockray and Conor Linehan in Digital Health
Footnotes
Conflict of interest
There are no conflicting interests related to this research.
Contributorship
KR and SD conceived the study and devised and piloted the search strategy in consultation with CL. KR and SD conducted title and abstract screening and full text review. KR conducted data extraction and CL and SD checked this for accuracy. KR and SD completed the quality review. KR wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
This work was supported by the Irish Research Council [grant number EPSPG/2016/182].
Guarantor
SD
Peer review
This manuscript was reviewed by two individuals who have chosen to remain anonymous.
Supplementary Material
Supplementary material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.