
Abstract
Objective
To describe the latest evidence of effectiveness and impact of networked communication interventions for young people with mental health conditions.
Methods
Searching five databases from 2009 onwards, we included studies of any design investigating two-way communication interventions for the treatment of young people (mean age 12–25) with a chronic mental health disorder. The data were synthesised using narrative summary.
Results
Six studies met the inclusion criteria, covering a range of mental health conditions (depression, psychosis, OCD). Interventions included an online chat room (n = 2), videoconferencing (n = 3) and telephone (n = 1). Where studies compared two groups, equivalence or a statistically significant improvement in symptoms was observed compared to control. Views of patients and clinicians included impact on the patient-clinician interaction. Clinicians did not feel it hindered their diagnostic ability.
Conclusion
Networked communication technologies show promise in the treatment of young people with mental health problems but the current available evidence remains limited and the evidence base has not advanced much since the previous inception of this review in 2011.
Practice implications
Although the available research is generally positive, robust evidence relating to the provision of care for young persons via these technologies is lacking and healthcare providers should be mindful of this.
Introduction
Worldwide, mental health conditions are a significant source of disease burden. 1 The costs are high both on a macro level, with high economic costs, 2 and on an individual level correlating with poor physical health and emotional wellbeing, lower educational attainment and decreased social capital.3–5 In young people, this is particularly significant over the life-course. Many mental health problems begin in childhood or young adulthood, 6 and their prevalence increases with age, affecting 7.7% of 5–10 year olds, 11.5% of 11–16 year olds and around 23% of 18–20 year olds.7,8 Mental health conditions may become chronic and there is evidence to show that early intervention and good care are cost effective and can improve both short and long-term outcomes. 9
There are a number of challenges associated with providing health care for young people. They face multiple barriers to access including insufficient training of healthcare providers and issues around confidentiality when navigating young adulthood.10,11 This is exacerbated by behavioural issues such as risk-taking behaviour and problems transitioning from paediatric to adult services. 12 There is scope to consider how these barriers can be overcome to facilitate service provision and reduce the development of long-term problems.
The use of networked communication technologies is increasingly widespread, particularly amongst young people and adolescents. In the UK, 91% of 16–24-year-olds own a smartphone, 13 giving them access to text messaging, email, social networking and videoconferencing in any location where there is network coverage. Health professionals working with young people with mental health conditions are increasingly using digital communication to engage with them, using both one way and two-way communication channels. 14 This review examines the impact of the use of two-way communication between health professionals and young people with mental health conditions.
To date, only one review has described the effectiveness and impact of networked communication interventions specifically in young people with mental health conditions. 15 This review found just 12 studies which investigated the use of email and/or web-based electronic diaries, videoconferencing and email communication. Email consultation was linked with symptom improvement and patients showed willingness to use networked communications, but overall the results were inconclusive due to the small number of studies and varied outcomes. As the field of digital communication is swiftly evolving, the current review will build on this previous work, including only literature published since the search date from this previous review (2009), as part of a series of rapid reviews for the LYNC study. The LYNC study explored the use of two-way digital communication technologies in healthcare provision for young people (aged 16–24 years) with long term conditions, 14 and the rapid reviews were conducted as a means to support and add value to the case studies within the LYNC study and to place the case study findings in a wider research context.
Methods
The review aims to present evidence for the effectiveness and impact of digital networked communication interventions in the treatment of adolescents with mental health disorders. A rapid review differs from a traditional systematic review primarily in the time taken to complete the review; a rapid review is often conducted within eight weeks. 16 Rapid reviews must, however, adhere to the core principles of systematic review. The protocol of the rapid review was registered in the International PROSPERO database under the following number: CRD42016038792.
Population
Our population was adolescents or young adults (mean age 12–25 years) with a mental health condition as defined by the Diagnostic and Statistical Manual of Mental Disorders (DSM-IVTR). 17 We did not include participants with neurodevelopmental disorders or non-chronic mental health conditions.
Intervention
The intervention was networked communication technology (e.g. telephone, email, text message and videoconferencing) allowing two-way communication between the patient and healthcare professional. Computerised cognitive behavioural therapy (CCBT) interventions were not included where the focus of the study was the automated computer program. We did not include interventions that allowed only one-way communication.
Comparator
We included comparison with usual care.
Outcomes
We included clinical outcomes, patient outcomes and clinician outcomes.
Inclusion criteria
This review looked at publications from May 2009 onwards. A previous review, published in 2011, searched from inception of databases to 2009. 15 This review updates the literature since that period. We included any study design and studies in any language. Conference abstracts were excluded unless the abstract itself contained sufficient data to be included in the analysis.
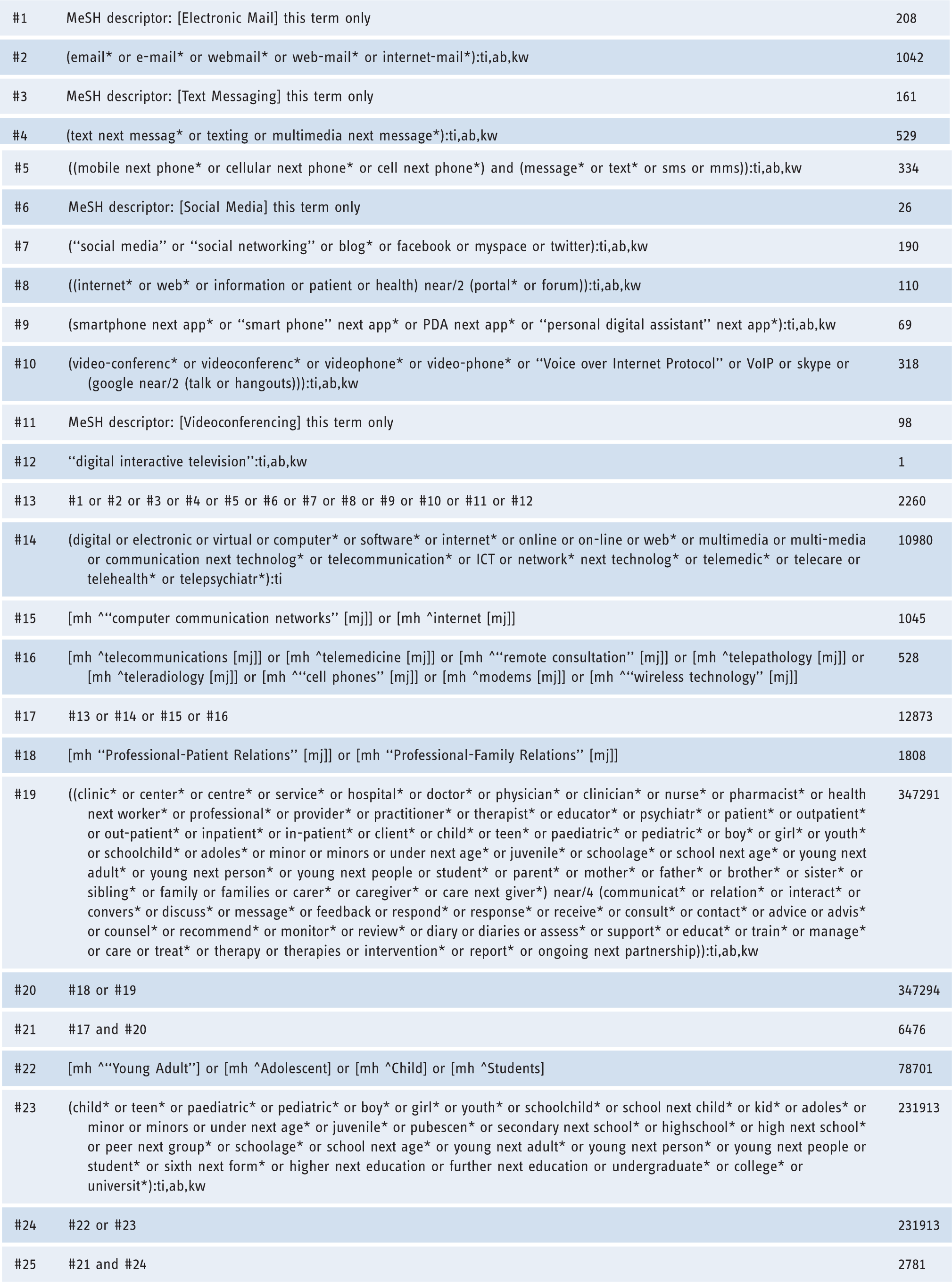
Search strategy
The search strategy was developed by an information specialist (RC). As part of a series of rapid reviews within the wider LYNC project, a common search was conducted within five electronic databases (MEDLINE (Ovid), Medline In-process (Ovid), Embase (Ovid), PsycINFO (Proquest), Cochrane Library (Wiley)) using free-text and thesaurus terms for the concepts ‘technology’, ‘clinical communication’ and ‘population’ (see Appendix for search strategy). The searches were undertaken in August and September 2015. Records were exported to a bibliographic management software (EndNote X7) and a relevant subset identified by searching within this list for specific conditions and terms relating to ‘mental health’.
Screening
All titles and abstracts resulting from this search were screened for inclusion by one of two reviewers (AV or AU). A random selection of 20% was screened by both. A third reviewer (FT) resolved any disagreements. Reasons for exclusion were recorded.
Articles that met these criteria after the initial screen were screened as full texts by two reviewers (AV and AU). Any discrepancies over inclusion were resolved through discussion or with the help of a third reviewer (HA).
Data extraction and quality assessment
Data were extracted from the included studies using a data collection form which collected information on population, intervention, setting, comparator and outcomes. All included papers were assessed for quality using the appropriate Critical Appraisal Skills Programme (CASP) critical appraisal instrument for the study design. 18 Studies with no limitations identified during this process were classed as ‘good’. Studies with one or two limitations were classed as ‘fair’, and any research with three or more flaws as ‘weak’.
Data synthesis
Due to the variation in study design and technology type included we present the findings using a narrative summary.
Results
The search identified 3503 articles. 3281 were excluded based on title or abstract. 222 articles were read in full and a total of six studies met our inclusion criteria and formed part of the review.19–24 See Figure 1 for a flow chart.
Study flow diagram.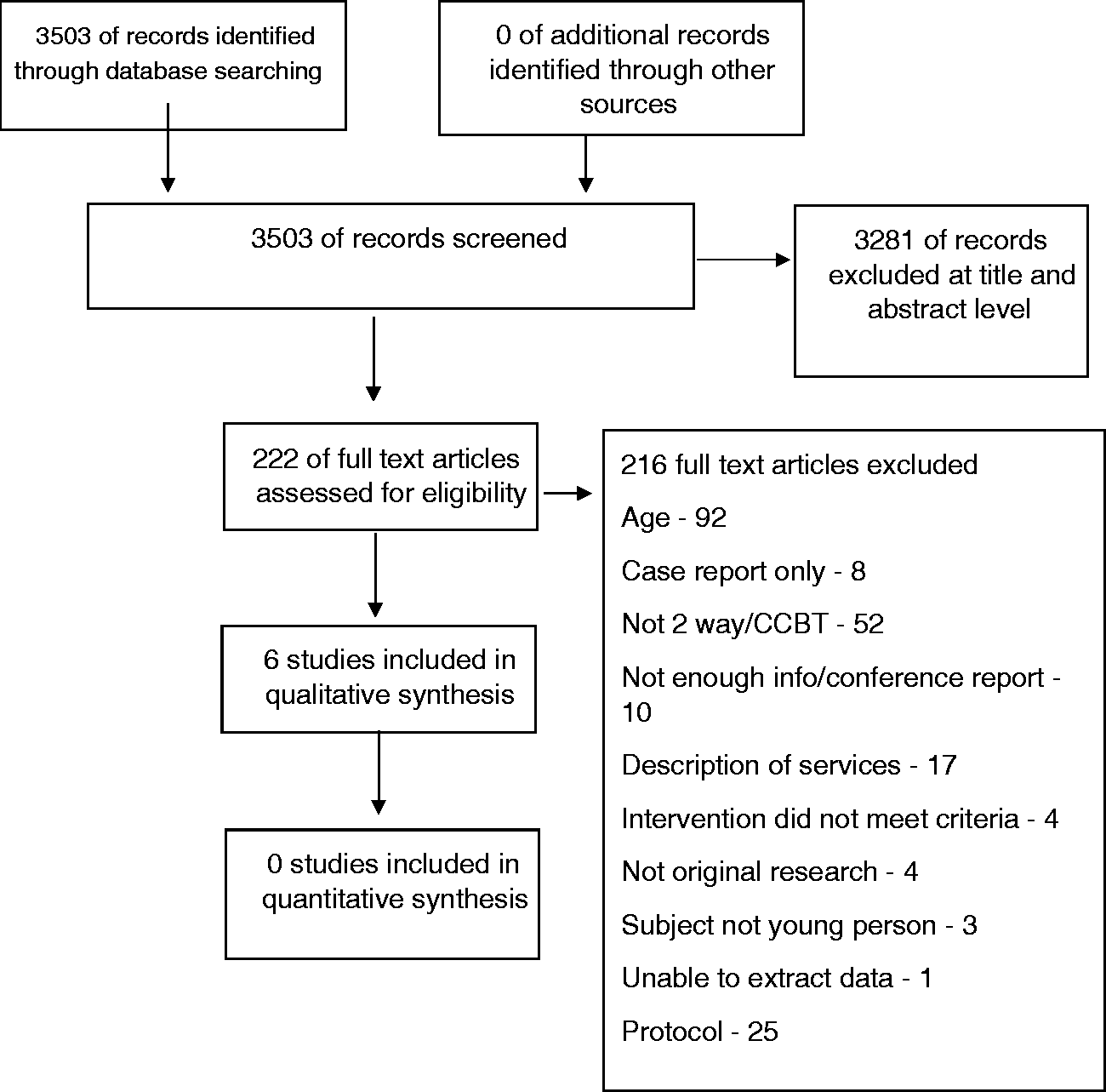
Characteristics of included studies.

Overall the quality of included papers was fair. Only one paper was classed as good; 21 four were fair,19,20,22,23 but one was weak according to our pre-specified criteria. 24
Clinical outcomes
Summary of main results.
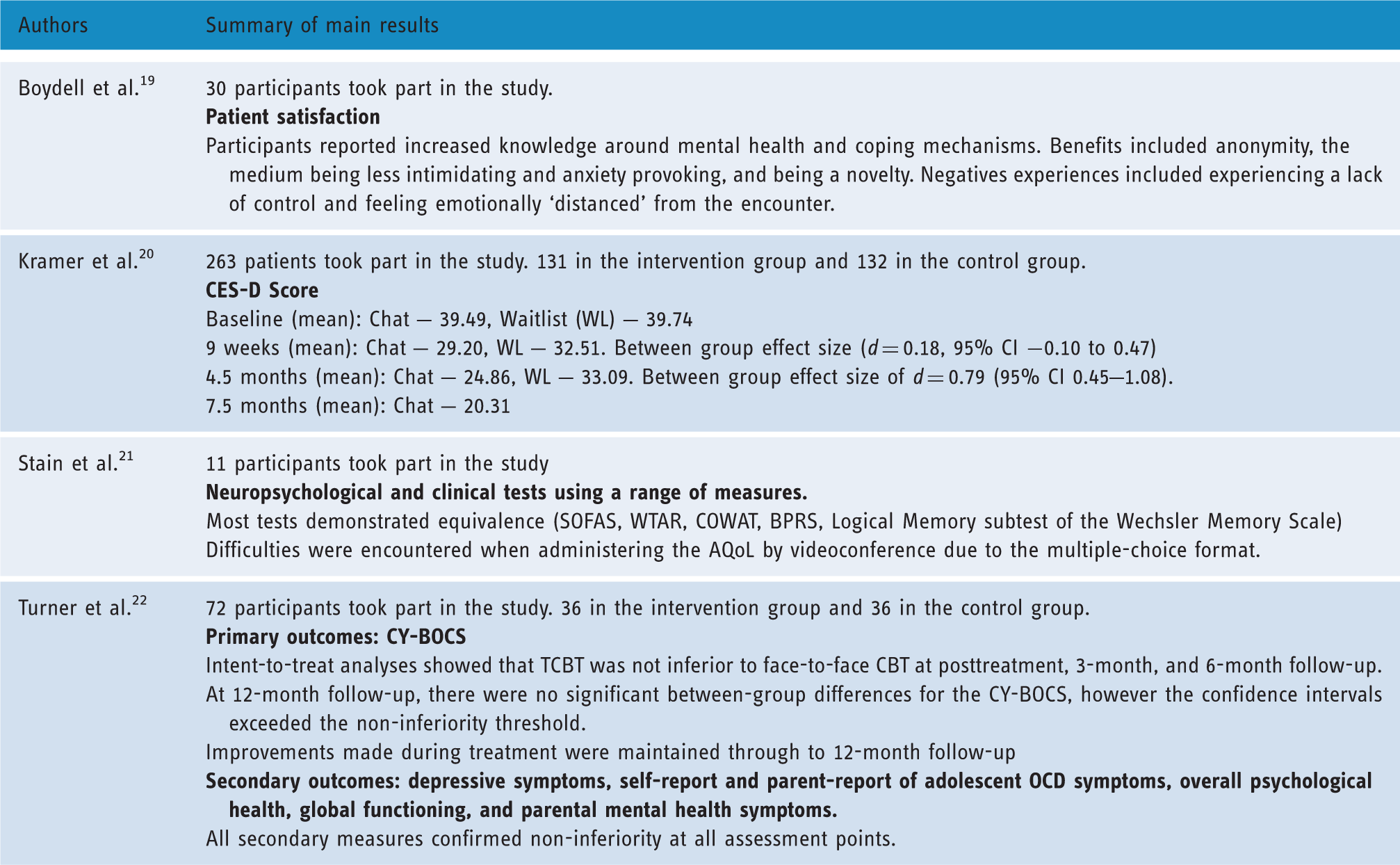
The delivery of CBT via telephone was investigated by Turner et al. 22 They compared telephone CBT to face-to-face CBT for adolescents with OCD and found no significant clinical difference between the two groups following treatment after assessment with several clinical scales (Children's Yale–Brown Obsessive-Compulsive Scale (CY-BOCS), Children's Obsessional Compulsive Inventory–Revised (ChOCI-R), Beck Depression Inventory for Youth (BDI-Y), Strengths and Difficulties Questionnaire (SDQ)). Their findings indicated non-inferiority of telephone CBT compared to face-to-face treatment. 22
Stain et al. investigated the feasibility of neuropsychological testing via videoconferencing in adolescents with early psychosis. 21 Most tests demonstrated equivalence (Social and Occupational Functioning Assessment Scale (SOFAS), Wechsler Test of Adult Reading (WTAR), the Controlled Oral Word Association Test (COWAT), the Logical Memory subtest of the Wechsler Memory Scale and the BPRS) indicating that they can reliably be carried out by videoconferencing. Difficulties were encountered when administering the Assessment of Quality of Life (AQoL), however, owing to the multiple-choice format. 21
Two qualitative interview studies gave an insight into the patient experience of psychiatric consultations conducted by videoconferencing (see Table 2).19,24 It is important to note that both these papers reported on patient experience after a single telepsychiatric consultation only. Participants generally found the consultations useful and they were reported to increase knowledge of the mental health disorder and coping methods. Some appreciated the consultation taking place at home where they felt comfortable, and also the anonymity provided by the clinician's distance. This separation made the encounter less stressful and intimidating for some, while for others it stimulated less engagement. Members of the younger group reported excitement at the novelty but also a lack of control. They were required to have an adult in the room with them during the consultation. Issues with sound or video quality were reported but these were generally brief and seemed not to interfere with the overall consultation.
One study reported that clinicians felt confident in making their diagnosis via videoconferencing. 24
Discussion and conclusion
Discussion
This rapid review found that networked communication technologies for the treatment of mental health disorders are generally acceptable to young people. It included data on a range of technologies including videoconferencing, telephone and online chatrooms. Due to the clinical and methodological heterogeneity between the included studies, it was not possible to combine results relating to individual technologies or a specific mental health disorder, which would be useful in drawing robust conclusions. We found evidence relating to a range of mental health disorders (anxiety, depression, psychosis, OCD).
Two studies demonstrated the equivalence of interventions delivered via telephone and videoconferencing as compared to face-to-face.21,22 Another study reported improved clinical outcomes compared to waitlist controls in those who received online group CBT. 23 Together, this seems to indicate networked communication technologies could be a viable alternative to standard face-to-face therapy.
In the earlier version of this review, which examined studies up until 2009, 15 networked communication technologies for the treatment of mental health problems were generally positive, but there were only 12 studies identified. This latest version of the review noted fewer reservations about privacy, with participants instead reporting the distance enabled them to feel more anonymous. 19 This could perhaps reflect an increasing trust in technology over time. Furthermore, equipment quality seemed to have improved since the previous study and significantly fewer issues were reported.
Other previous reviews looking at the use of communication technologies within mental healthcare for young people have generally been broad in their inclusion criteria. Many are dominated by CCBT, perhaps because of its ready uptake by healthcare providers. Example of this are the studies by Ye et al. (anxiety or depression) and Aardoom et al. (eating disorders),25,26 in which the majority of included articles focus on CCBT (6/7 articles and 14/21 respectively). Nevertheless, few reviews have looked specifically at CCBT for the treatment of young people. Those that have are generally positive in their findings but indicate that further research is needed.27,28 In contrast, this review has looked exclusively at two-way communication and has therefore excluded interventions such as CCBT.
Two-way communication is more similar to current clinical treatments for mental health disorders such as counselling and psychotherapy but assumptions about its equivalence are unwise. Different technologies involve different levels of human contact (compare videoconferencing to a text message) and it seems possible that effectiveness may vary with the method used.
A 2014 rapid review of interventions in ‘e-mental health’ took a broad approach and found that the majority of interventions were aimed at adults with depression or anxiety symptoms. Effectiveness was demonstrated in some early trials and other studies summarised benefits that included flexibility and engagement. 29 However, this review focused on adult populations and was not restricted to two-way communication. A review and meta-analysis of e-mental health interventions to treat post-traumatic stress disorder (PTSD) in adults showed a significant improvement in symptoms for those using the e-mental health interventions. However, this study included interventions that had no communication, or one-way communication. 30
Overall, the evidence available regarding young people and their use of two-way networked digital communications remains limited. Nevertheless, findings are generally positive with studies reporting improved symptoms scores or equivalence to current treatment. It is unclear whether drop out might be an issue for this particular young population. Drop out is known to be lower when interventions are delivered online. 31 However there is no age specific data and so it is not possible to assess whether this might be a particular issue for those in adolescence and young adulthood.
This review was conducted to inform a wider study looking at networked communication technologies for the treatment of young people. 14 This gave us an overview of its use in practice and allowed us to see mental health within this context but restricted the time taken in conducting the review. Taking a ‘rapid’ approach meant that grey literature was not included and it is therefore possible that some relevant data may have been missed. Nevertheless, the search was broad and covered a wide range of mental health conditions, included non-English language papers, and was developed by an information specialist. This review examines the more recent literature since publication of the previous version of this review, which was important given the rapid pace of change within digital technologies.
Conclusion
Networked communication technologies show promise in the treatment of young people with mental health disorders but there are many conditions and methods of treatment that have not yet been fully investigated. The use of communication technology is widespread amongst young people and adolescents and is already becoming more prevalent within healthcare. Research into this important age group has not kept up with policy and practice and evaluation of these approaches is much needed.
Practice implications





Totals:
N.B. Many records will include more than one of the above terms. Therefore, the totals below are not the sum of the numbers above.
1. Specific condition keywords in any fields: 2835
2. General mental health keywords in title: 1292
3. 1 OR 2 = 3503 (final total for screening)
Supplemental Material
Appendix -Supplemental material for Effectiveness and impact of networked communication interventions in young people with mental health conditions: A rapid review
Supplemental material, Appendix for Effectiveness and impact of networked communication interventions in young people with mental health conditions: A rapid review by Alice Verran, Ayesha Uddin, Rachel Court, Frances Taggart, Paul Sutcliffe, Jackie Sturt, Frances Griffiths and Helen Atherton in Digital Health
Footnotes
Acknowledgements
We thank the wider LYNC project team for their general support and input into the wider project, of which this review was a part.
Contributorship
All authors approved the final manuscript. Alice Verran led the review, conducted screening and data extraction, analysed the data and co-wrote the manuscript. Ayesha Uddin contributed to screening, data extraction and analysis. Rachel Court assisted with planning the review, developed and undertook the searches and contributed to writing the manuscript. Frances Taggart contributed to the design and conduct of the review and the writing of the manuscript. Paul Sutcliffe contributed to the review concept and design and contributed to the manuscript. Jackie Sturt co-led the LYNC project with Jackie Sturt, conceiving and designing the wider LYNC study, supervised the conduct of the review and editorially reviewed this manuscript. Frances Griffiths co-led the LYNC project with Jackie Sturt, conceiving and designing the wider LYNC study, supervised the conduct of the review and editorially reviewed this manuscript. Helen Atherton supervised the conduct and completion of the review, analysed data and co-drafted the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not required for this review article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute for Health Research, Health Services & Delivery Research (project number 12/209/5).
Guarantor
FG
Peer Review
This manuscript was reviewed by two individuals who have both chosen to remain anonymous.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.