
Abstract
Case summary
An 8-year-old castrated male mixed-breed cat was presented with recurrent vomiting, weight loss and abdominal distension. Blood work revealed hyperbilirubinaemia and elevated liver enzyme activities. Abdominal ultrasound and CT showed marked dilation and obstruction of the common bile duct (CBD) due to chronic cholecystitis and cholangiohepatitis. The cat was diagnosed with CBD obstruction secondary to chronic cholecystitis and cholangiohepatitis and was initially treated with antibiotics and prednisolone. Surgical intervention was performed because of complete CBD obstruction and worsening icterus that was unresponsive to medical management. A choledochoduodenostomy was performed using a simple side-to-side anastomosis between the CBD and the duodenum. The patient recovered uneventfully after surgery without significant complications. At the last follow-up, 6 months postoperatively, the cat remained clinically stable.
Relevance and novel information
There is limited information on choledochoduodenostomy in cats. This is the first veterinary report describing a simple side-to-side anastomosis between the CBD and the duodenum to resolve severe extrahepatic biliary obstruction secondary to chronic cholangitis and cholecystitis. As a result of the dilation and thickening of the CBD wall, this technique was feasible. This case study lacks information on long-term prognosis and continued monitoring is important.
Keywords
Introduction
Extrahepatic biliary obstruction (EHBO) may occasionally develop in cats as a result of cholecystitis, pancreatitis, cholelithiasis, parasitosis, diaphragmatic hernia and neoplasia.1 –3 Medical management with antibiotics and anti-inflammatory drugs are often attempted as the initial line of treatment; 1 however, if patency of the common bile duct cannot be restored, a biliary bypass procedure is necessary to decompress the biliary tree.4,5 Because EHBO is uncommon in cats, the level of evidence for its surgical management remains low. 6 Although there are reports on cholecystoduodenostomy,7,8 placement of a temporary cholecystostomy tube and choledochal stenting as surgical approach for EHBO in cats, there are limited reports on other surgical approaches. 9 The aim of this report was to describe a case in which choledochoduodenostomy using a simple side-to-side anastomosis between the common bile duct (CBD) and duodenum was performed to resolve severe EHBO secondary to chronic cholangitis and cholecystitis. To our knowledge, this is the first detailed report of side-to-side anastomosis between the CBD and duodenum in cats.
Case description
An 8-year-old castrated male mixed-breed cat presented with recurrent vomiting and weight loss. On physical examination, abnormalities included moderate icterus of the pinnae and mucus membranes. Blood work revealed elevated serum total bilirubin (Tbili), serum liver enzyme activities and serum amyloid A (SAA) protein (Table 1, day 0). SNAP feline pancreatic lipase immunoreactivity (fPLI) (Idexx Laboratories) was negative. The total thyroxine level was 2.36 μg/dl (reference interval [RI] 0.9–3.7 μg/dl). An abdominal ultrasound demonstrated dilation of both the intrahepatic and extrahepatic biliary tree (Figure 1a,b). The gallbladder could not be reliably identified from the abnormal surrounding ducts. The dilated biliary structures occupied the majority of the abdomen and revealed marked hyperechogenic sediment accumulation (Figure 1c). On abdominal CT scan, the intrahepatic bile ducts, cystic duct and CBD were markedly dilated and saccular in appearance. In particular, a fusiform dilatation of the CBD was observed. The duodenum was displaced to the left side by the dilated CBD. Findings of thickening and contrast enhancement of parts of the gallbladder wall and bile duct wall suggested cholecystitis and cholangitis. A definitive cause for the CBD obstruction was not identified on the CT scan (Figure 2).
The cat was diagnosed with obstruction of the CBD due to chronic cholangiohepatitis and was treated with enrofloxacin 5 mg/kg PO q24h, prednisolone 0.7 mg/kg PO q12h and metronidazole 10 mg/kg PO q12h. The medical treatment temporarily improved icterus and decreased the level of hyperbilirubinaemia (Table 1, day 7). However, after 2 weeks, surgical intervention was performed in the face of elevated TBili levels unresponsive to medical management (Table 1, day 14). The cat was premedicated with fentanyl 5 μg/kg IV and atropine 50 μg/kg IM, and induced with propofol 6 mg/kg IV. Anaesthesia was maintained with isoflurane vaporised in oxygen delivered with peak inspiratory pressures of 10 cm H2O. Fentanyl was administered as a constant rate infusion (CRI) at a rate of 10 μg/kg/h. The patient was kept on a heating pad during surgery, with its vital parameters monitored every 5 mins. Surgical exploration of the abdomen revealed an enlarged gallbladder and dilated CBD that was severely thickened and fibrotic with omental and mesenteric adhesions (Figure 3). Upon performing a duodenotomy, it was confirmed that the major duodenal papilla was severely thickened, making catheterisation and flushing of the CBD impossible. As a result of marked dilation of both the intrahepatic and extrahepatic bile ducts, the distance between the duodenum and gallbladder was significantly increased, making cholecystoduodenostomy unfeasible. A choledochoduodenostomy using a simple side-to-side anastomosis between the CBD and duodenum was performed to relieve the CBD obstruction. The anastomosis was performed in the extramural CBD, approximately 5 cm distal to the major duodenal papilla. After placing two stay sutures to approximate the CBD and duodenum, an incision of approximately 3.0 cm was made in the extramural CBD and descending duodenum (Figure 4a,b). A simple side-to-side anastomosis between the CBD and duodenum was performed with 4-0 polydioxanone monofilament suture material in a simple continuous pattern (Figure 4c).
For biopsy, the margin of the quadrate lobe of the liver was excised using Metzenbaum scissors, and haemostasis was achieved with electrocautery. A wedge-shaped excision was made in the distal common bile duct wall, approximately 3 cm away from the major duodenal papilla, using a sharp blade scalpel. In addition, a biopsy of the gallbladder was performed using a 6 mm punch biopsy. The biopsy site was closed with simple interrupted sutures. A bile sample was also collected for bacterial examination, including aerobic/anaerobic culture and sensitivity testing. The peritoneal cavity was lavaged with warm sterile saline and then closed routinely. The cat was maintained on fentanyl CRI at 3 μg/kg/h for 24 h postoperatively. All medications, except for antibiotics (enrofloxacin 5 mg/kg PO q24h), were discontinued postoperatively.
Two days after surgery, abdominal ultrasound showed resolution of the previously noted dilation of the CBD, with no evidence of leaking bile (Figure 5). On blood work, Tbili was decreased (Table 1, day 16). One week postoperatively, the cat was discharged as it was voluntarily consuming over 80% of its resting energy requirement. At the time of discharge, no medications were prescribed except for antibiotics. Chronic suppurative cholangitis with infiltration of inflammatory cells was confirmed by histopathology of the liver tissue sample. Histopathology of the gallbladder sample revealed chronic neutrophilic proliferative cholecystitis. Bacterial colonies were not observed within the inflamed gallbladder tissue. Histopathology of the tissue taken from the obstructing site of the CBD demonstrated abundant dense fibrous connective tissue and infiltration of inflammatory cells. There was no evidence of neoplasia (Figure 6).
Follow-up examinations were performed 2 and 6 months postoperatively, during which time the cat remained clinically stable. Blood tests showed an improvement in hyperbilirubinaemia and liver enzyme activities (Table 1, days 46 and 194). On day 194, although a CT scan demonstrated gas in the gallbladder originating from the digestive tract, no evidence of anastomotic stenosis was observed (Figure 7).
Pre- and postoperative blood examination in a cat that underwent choledochoduodenostomy

Alb = albumin; ALP = alkaline phosphatase; ALT = alanine aminotransferase; AST = aspartate transferase; BUN = blood urea nitrogen; Ca = calcium; Cl = chloride; Cre = creatinine; GGT = gamma-glutamyl transferase; GLU = glucose; HCT = haematocrit; HGB = haemoglobin; IP = inorganic phosphorus; K = potassium; Na = sodium; PLT = platelet; RBC = red blood cells; RI = reference interval; SAA = serum amyloid A protein; TBili = total bilirubin; TP = total protein; WBC = white blood cells

Ultrasonographic image of the liver and dilated common bile duct. (a) Marked saccular dilatation of intrahepatic and extrahepatic biliary tree was confirmed. Thickening and high echogenicity of parts of the gallbladder wall and bile duct wall were observed. (b,c) There is a collection of organised, dependent echogenic debris within the common bile duct dilatation (asterisks)
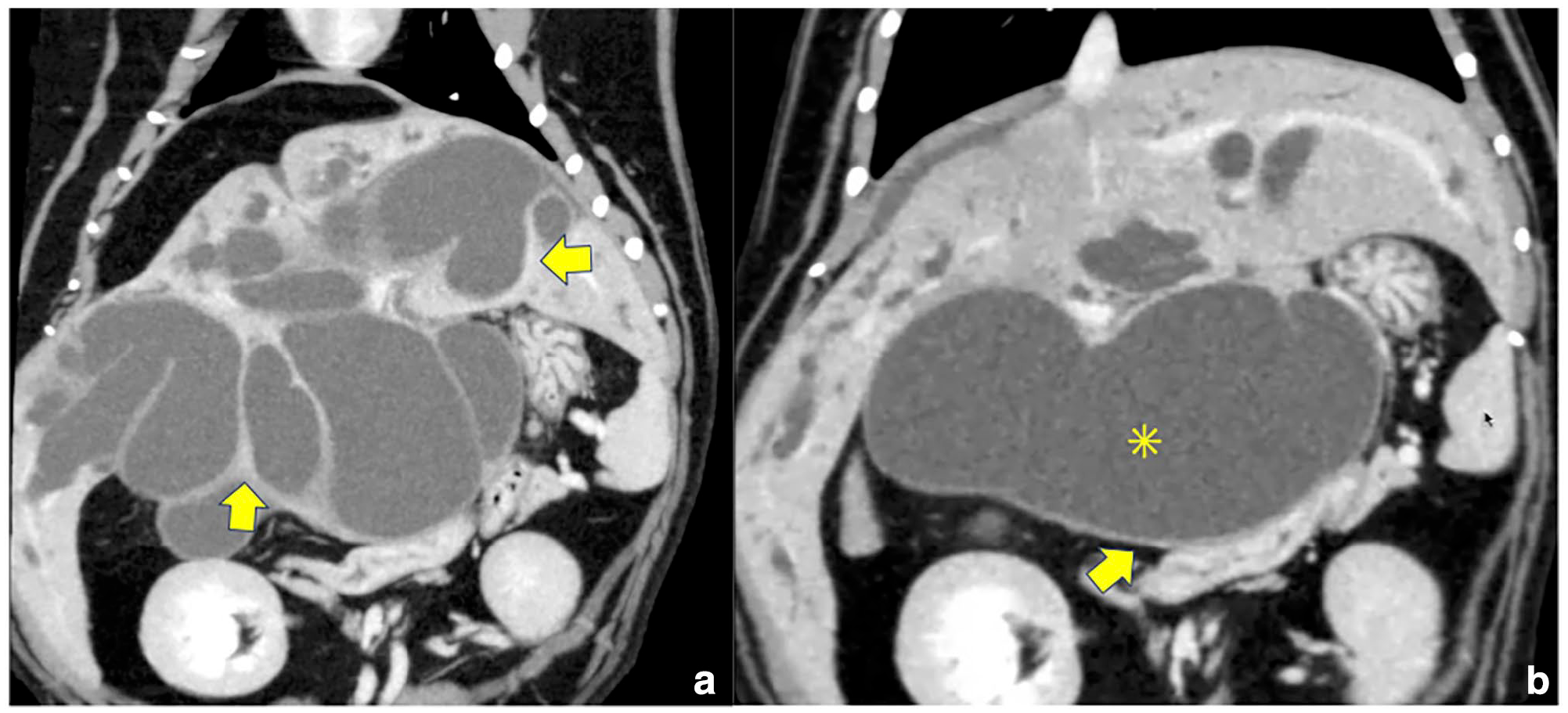
Coronal view of the abdominal CT scan. (a) Multiple dilated bile ducts are visible, including intrahepatic and extrahepatic ducts. Thickening and contrast enhancement of parts of the gallbladder wall and bile duct wall are observed (yellow arrows). (b) The duodenum is displaced to the left side by the dilated common bile duct (asterisk)

Surgical exploration of the abdomen. (a) Enlarged gallbladder and dilated common bile duct were confirmed. Tape measure in centimetres shown for scale. (b,c) A thickened and hardened common bile duct was observed, with adherence to the omentum and surrounding fat. The black circle indicates the thickened and hardened region of the common bile duct. The black arrow indicates the orifice of the common bile duct. CBD = common bile duct; DUO = duodenum; GB = gallbladder
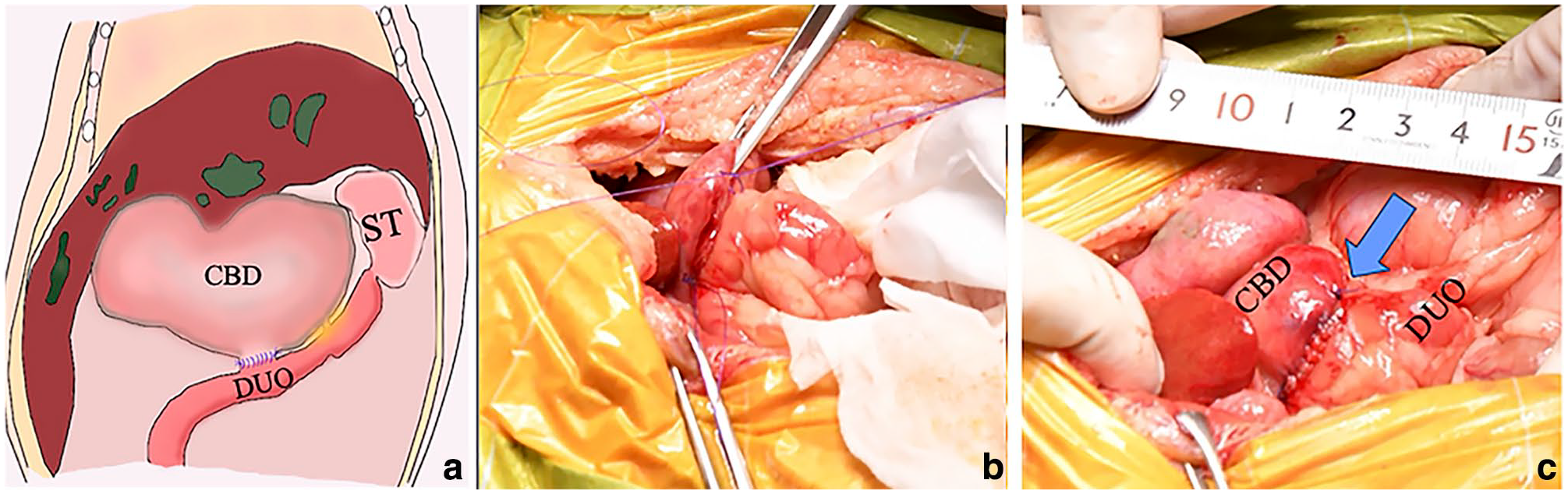
(a) Surgical procedure: schematic figure on the surgical technique. After cutting the common bile duct and duodenum (5 cm distal from the duodenal papilla), the anastomosis between the common bile duct and duodenum was performed. Surgical images: (b) retracting the common bile duct and duodenum using two stay sutures; and (c) choledochoduodenostomy using a simple side-to-side anastomosis between common bile duct and duodenum. The blue arrow indicates suturing site. Tape measure in centimetres shown for scale. CBD = common bile duct; DUO = duodenum; GB = gallbladder

Ultrasonographic image of the liver and intrahepatic and extrahepatic bile ducts 2 days postoperatively. The intrahepatic and extrahepatic bile ducts were not dilated (yellow arrow). No ascites or bile leakage from the surgical site was observed

Histopathology of the tissue taken from the liver and common bile duct (CBD) sample. (a) Collagen fibre proliferation was observed around the portal triads in the liver, indicating moderate fibrosis. Moderate infiltration of inflammatory cells, predominantly lymphocytes, was noted around the bile ducts, with necrotic and exfoliated epithelial cells present within the bile duct lumen (yellow arrow). Hepatocytes exhibited diffuse vacuolar degeneration, accompanied by the deposition of greenish-brown pigment. (b) In the CBD wall, marked infiltration of lymphocytes was observed in the submucosal tissue (black arrowheads). A small number of macrophages were also present, along with cellular debris in the surrounding area

Coronal view of abdominal CT scan 6 months postoperatively. Digestive gas was visible in the common bile duct and extrahepatic bile duct. The yellow arrow indicates the junction of the common bile duct and duodenum
Discussion
Choledochoduodenostomy using a simple side-to-side anastomosis between the CBD and duodenum was performed in a cat with obstruction of the CBD due to inflammation. The patient recovered smoothly postoperatively without complications. Since there are limited detailed reports on choledochoduodenostomy in cats, 8 this case report provides valuable insight, not only into the surgical approach but also into the medium-term prognosis, which has been less frequently documented in the literature.
Previous studies have reported cases in which choledochoduodenostomy was performed to resolve EHBO due to malignant tumours.7,8 Choledochoduodenostomy is considered to be a surgery with high technical difficulty and a high rate of postoperative complications. 6 There are only a few reports about the clinical outcomes and surgical techniques of choledochoduodenostomy. 5 A previous retrospective case series presented extrahepatic biliary surgery as a management approach for CBD obstruction refractory to medical treatment, including a cat that had undergone choledochoduodenostomy. 5 In human medicine, choledochoduodenostomy is considered superior to cholecystoduodenostomy for conditions such as CBD obstruction caused by tumours, as it has a lower risk of bile duct bypass failure.12,13 In humans, the CBD is significantly larger, and end-to-end anastomosis of the duct or its connection to the intestine is a common surgical procedure, particularly in liver transplantation. In contrast, a key limitation in veterinary medicine is the small size of the biliary tree, including both the diameter and wall thickness, which makes choledochoduodenostomy a less feasible option in many cases. Given the limited number of clinical reports in small animals, it remains unclear whether choledochoduodenostomy offers any advantages over cholecystoduodenostomy.6 –8,14,15
In the present case, the distance between the duodenum and the gallbladder was significantly increased because of the dilated cystic duct and CBD, making it difficult to perform a cholecystoduodenostomy. Therefore, side-to-side anastomosis of choledochoduodenostomy was performed. The good clinical outcome in this patient was likely due to the severe dilatation of the CBD and its thickened wall, which facilitated the anastomosis. Normally, the relatively small diameter and thinness of the CBD wall make the suture site prone to breakdown.7 –9,16 In this case, since the CBD wall was dilated and thickened by chronic inflammation due to cholecystitis and cholangiohepatitis, a simple side-to-side anastomosis between CBD and duodenum was feasible. Performing a preoperative CT scan was useful to evaluate in detail the CBD and the possibility of performing a choledochoduodenostomy. In this case, no complications were observed 6 months postoperatively; however, since recurrent biliary tract infection secondary to enterobiliary reflux has been reported as a potential long-term complication of biliary diversion surgery in cats,10,11 further follow-up will be necessary.
In the present case, the width of anastomosis between the CBD and the duodenum was 3.0 cm. Although this length has been reported as a reference value for the width of anastomosis when performing cholecystoduodenostomy, 4 it is unclear whether this width was appropriate in this case or not. The anastomosis site may re-occlude because of scar contraction at the suture site; therefore, continuous monitoring is required. Given these considerations, alternative approaches to managing the obstruction should also be evaluated. It is important to consider that stenting the CBD could have been a potential option in this case. In purely inflammatory obstructions, stenting combined with appropriate medical management, including anti-inflammatory and antibiotic therapy, could potentially resolve the issue without requiring biliary bypass procedure. 17 Future cases should carefully evaluate the feasibility of stenting before considering biliary bypass surgery. In addition, distinguishing between segmental and diffuse dilation of the CBD is crucial in the decision-making process for this surgery. As reported by Spain et al, 18 segmental dilatation of the CBD should not prompt surgery. Some cases with segmental dilatation of the CBD may respond to medical management. Although the severity of inflammation and the extent of thickening justified the decision to proceed with a bypass in this case, it is crucial to recognise that not all cases of CBD dilatation necessitate a biliary bypass procedure.
Conclusions
This case report describes choledochoduodenostomy using a simple side-to-side anastomosis between the CBD and duodenum performed in a cat with focal thickening and obstruction of the CBD secondary to chronic cholecystitis. Because the CBD wall was dilated and thickened, a simple side-to-side anastomosis between the CBD and duodenum was feasible. This report lacks information on the long-term prognosis, and continued monitoring is important following these procedures as a result of the potential risks of ascending infections and/or stenosis of the anastomosis.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.