
Abstract
To identify factors associated with higher levels of anxiety and poorer quality of life in women with abnormal results in a cervical screening programme. A cross-sectional study was conducted among 140 women aged 25–65 years with abnormal cervical screening results referred to the Cervical Pathology Clinic at Donostia University Hospital between May and November 2022. Anxiety and quality of life were assessed using the State-Trait Anxiety Inventory (STAI) and the Human Papillomavirus-related Quality of Life (HPV-QoL) questionnaire, respectively. Multivariable linear regression models were used to identify factors independently associated with emotional outcomes. Higher state anxiety (STAI-S) was independently associated with greater baseline trait anxiety (STAI-T) (p < 0.001), a first positive HPV result (p = 0.05), and low-to-medium educational level (p = 0.03). Among HPV-positive women, poorer HPV-related quality of life was independently associated with higher baseline trait anxiety (p = 0.008) and lower educational level (p = 0.032). Baseline anxiety is the strongest determinant of emotional impact after an abnormal cervical screening result, followed by first-time HPV positivity and lower educational level
Introduction
Almost all cases of cervical cancer are caused by the high-risk human papillomavirus (HPV) (Bosch et al., 1995, 2002). The knowledge of this causal link, together with technological advances, has led to changes in cervical screening strategies (McCaffery and Irwig, 2005). The current recommendation nationally and internationally is to use HPV testing to screen >30- to 35-year-olds (AEPCC, 2014), since it has shown greater sensitivity than conventional cervical and vaginal cytology for identifying women at high risk of precancerous cervical lesions (Ronco et al., 2014). HPV is generally sexually transmitted and is very widespread, being found in around 8% of women tested (Australian Institute of Health and Welfare, 2022; Rebolj et al., 2019).
All screening programmes have pros and cons that everyone tested should be aware of in advance (IARC, 2023). One of the negative effects of screening is the emotional impact on participants when they obtain an abnormal result. In the context of cervical screening, an increase in anxiety has been observed and analysed when the screening test is cervical and vaginal cytology (Marteau et al., 1990), or HPV testing (Maissi et al., 2004; McCaffery et al., 2003a). Moreover, the sexual nature of HPV transmission can cause additional anxiety and distress (IARC, 2023; McCaffery et al., 2003a; McCaffery et al., 2004; McCaffery and Irwig, 2005), leading to emotions such as disgust, self-blame, shame, and stigma (McBride et al., 2021a; Waller et al., 2007). Given that cervical screening is being implemented population-wide, tens of millions of women worldwide undergo HPV testing every year. Therefore, even if only a small percentage of women experience adverse effects, the total number who experience psychological sequelae and/or negative behaviours may be very high.
Some anxiety is to be expected after abnormal screening results, and this may provide the necessary motivation to adhere to the recommended treatment. On the other hand, high levels of anxiety may negatively influence the processing of information and lead women to judge the danger they face to be disproportionately higher than their actual risk (Maissi et al., 2004). It may even discourage support-seeking and increase non-attendance at future screening rounds (Nick et al., 2021). Given these unwanted potential effects and their impact on women’s quality of life, it is important to identify factors associated with the onset of anxiety due to an abnormal result, to develop strategies to manage it.
Among potentially relevant factors, some authors have identified age, with lower levels of anxiety among older women (Maissi et al., 2004; Pirotta et al., 2009). Regardless of the cytology results, women with a positive HPV test tend to have higher levels of anxiety than those with a negative result (Maissi et al., 2004; McCaffery et al., 2004). Social and cultural norms may influence psychological and social responses. Higher levels of anxiety were observed in women from Indian or Pakistani ethnic groups, in which extramarital sexual relationships are prohibited (McCaffery et al., 2003a). Qualitative research indicated stronger adverse emotional effects in lower-income countries (Brazil, Colombia, Taiwan, and Tanzania) (McBride et al., 2021b). Personality type (more or less anxious) may also influence anxiety level after an abnormal screening result (McBride et al., 2020).
The primary objective of this study was to assess the state of anxiety in women with an abnormal result in cervical screening, as well as factors associated with greater anxiety. As secondary objectives, we analysed quality of life in women with an HPV-positive result and factors associated with a poorer quality of life.
Methods
A cross-sectional study was performed aiming to assess the anxiety and quality of life of women with abnormal cervical screening results. We included women referred to the cervical pathology clinic at a tertiary hospital in northern Spain between May and November 2022 for colposcopy due to an abnormal HPV test result, in line with the current protocol (AEPCC, 2014). The exclusion criteria were having been seen previously at a cervical pathology clinic; having received information about screening for HPV or the virus itself from a healthcare professional, except for the telephone call informing them of the abnormal findings; not having a sufficiently high level of Spanish to be able to understand and complete the questionnaires; and being emotionally unstable at the time for any other reason. The research team contacted women by telephone to inform them about the study and invite them to participate. Before this study-related call, women had already been informed of the abnormal screening result and the indication for colposcopy through routine clinical care. The study call was limited to explaining the study aims, and no additional information regarding HPV, screening, or colposcopy was provided, nor did participation modify the clinical pathway. All study procedures were conducted during a single in-person visit. Participants were recruited using a consecutive sampling strategy, whereby all women referred to the cervical pathology clinic during the study period were contacted. Recruitment was conducted on a weekly basis and limited only by clinic capacity (12 appointments per week), without selection based on clinical, sociodemographic, or psychological characteristics. Those who agreed to participate were given an appointment and an informed consent form. During this visit, no information was provided concerning HPV, the screening test, or the colposcopy procedure.
A standardised interview was used to collect the following data: age, considering four groups: 25–34 years, 35–44 years, 45–54 years, and 55–65 years; level of education, classified into three groups: low (lower secondary education or less), medium (upper secondary education or vocational training), and higher education (tertiary education or higher); and place of birth (which was divided into Spain or elsewhere, to simplify the analysis). Cytology and HPV results were retrieved from their health record. The cytology results were divided into three categories: normal or negative; low grade (atypical squamous cells of undetermined significance [ASCUS] and/or low-grade squamous intraepithelial lesion [LSIL]); and high grade (atypical squamous cells – cannot exclude high-grade squamous epithelial lesions [ASCH], high-grade squamous intraepithelial lesion [HSIL] and/or atypical glandular cells [AGC]); while the results of the HPV test were grouped as: HPV negative, HPV positive, and persistent HPV (two positive results within a year).
During this visit, women completed the Spanish version of the State–Trait Anxiety Inventory Trait (STAI-T) scale (Spielberger et al., 1970, 2015) to characterise baseline personality. The STAI-T scale refers to how people feel day-to-day, before and independently of the event analysed. It has 20 items, with a score ranging from 0 to 60, and a mean score of 24 among working women (Spielberger et al., 1970). The results obtained as numerical values are converted into percentiles to facilitate the analysis. This transformed scale allows comparisons with a normative sample, indicating an individual’s position relative to the general population. To analyse this variable, participants were divided into two groups (high vs low levels of trait anxiety), women being classified into the high trait anxiety group if they had a score of ≥30, equivalent to the 70th percentile or above.
Outcome measures
The outcome measures were the State–Trait Anxiety Inventory State (STAI-S) score to assess state anxiety level and the HPV-QoL score to assess the impact of receiving screening results on quality of life in HPV-positive women. Both scales have been validated in Spanish, and they were completed by participating women during the first study visit. The STAI-S scale (Spielberger et al., 1970, 2015) has 20 items and can be employed to measure how individuals feel at a given time, that is, their transient emotional state. Using this scale, we assessed the emotional state of each participant after receiving their abnormal HPV test results. Scores on this scale range from 0 to 60; the higher the score, the greater the level of anxiety. The HPV-QoL questionnaire (Coronado et al., 2022) was developed to assess the impact of HPV infection and related interventions on health-related quality of life. It consists of 15 items covering four domains: general wellbeing (including psychological and social wellbeing subdomains), health, contagiousness, and sexuality. The scores range from a minimum of 0 (worst quality of life) to a maximum of 100 (best quality of life). Raw HPV-QoL scores obtained from the 15-item questionnaire (range 15–75) were transformed to a standardised 0–100 scale according to the scoring instructions provided by the instrument developers.
The State–Trait Anxiety Inventory comprises two complementary 20-item subscales assessing trait anxiety (STAI-T) and state anxiety (STAI-S), which were used in this study to distinguish baseline anxiety from the situational emotional response to abnormal screening results.
Ethical statement
The study received approval from an independent ethics committee for health research in January 2022. All participants provided written informed consent prior to completing the questionnaires. The study ensured strict confidentiality, and all data were anonymised to prevent the identification of individual participants. All data generated or analysed during this study are included in this published article. No additional datasets were generated or deposited.
In writing this article, we followed the STROBE cross-sectional reporting guidelines (Von Elm et al., 2008).
Statistical analysis
Continuous variables were presented as mean and standard deviation (SD) for normal distributions and median and interquartile range (25th–75th percentiles) for skewed variables; discrete variables were expressed as absolute values and relative percentages. Student’s t test and analysis of variance were used to compare means. In the case of non-parametric variables, Mann–Whitney U or Kruskal–Wallis tests were employed. The chi-square test was used to compare proportions. Multivariable linear regression models were used to analyse factors independently associated with STAI-S and HPV-QoL scores. Covariates included in each model were those showing statistically significant associations in univariate analyses (p < 0.05). Categorical variables were entered into the models using binary (dummy) coding, with the clinically more favourable category as the reference. A two-sided p value of 0.05 was considered statistically significant. The statistical software used was SPSS v.29.
Results
We included 140 women (see Figure 1 for the flow of participants through the study), with a mean age of 40.7 years (SD: 12.01). The majority of the participants were born in Spain (70.7%) or Latin America (25%), and had a medium or high level of education (20% upper secondary or vocational training and 42.8% university qualifications). The STAI-T indicated that 27 women (19.3%) had high trait anxiety levels at baseline, according to the cut-off established. Table 1 summarises these and other baseline characteristics of the women included in the study. Flow of participants through the study. Patient baseline characteristics. Patient baseline characteristics. Data are expressed as mean and standard deviation for quantitative variables and number of cases and percentages for qualitative variables. AGC: atypical glandular cells; ASCUS: atypical squamous cells of undetermined significance; ASCH: Atypical squamous cells – cannot exclude high-grade squamous epithelial lesions; EU: European Union; HSIL: high-grade squamous intraepithelial lesion; LSIL: low-grade squamous intraepithelial lesion; STAI-T: State-Trait Anxiety Inventory Trait Scale.

State-Trait Anxiety Inventory State (STAI-S) scores stratified by patient clinical and personal characteristics State anxiety (STAI-S) scores stratified by patient clinical and personal characteristics.

Data are expressed as mean and standard deviation. Cytological results: Normal (negative for malignant cells), low grade (atypical squamous cells of undetermined significance and/or low-grade squamous intraepithelial lesion), and high grade (atypical squamous cells – cannot exclude high-grade squamous epithelial lesions, high-grade squamous intraepithelial lesion and/or atypical glandular cells). STAI-T: State-Trait Anxiety Inventory Trait Scale.
Including these variables in a linear regression model, high trait anxiety (p < 0.001), a first HPV-positive result (p = 0.05), and a low-to-medium level of education (p = 0.03) were found to be independently associated with higher levels of state anxiety. Place of birth no longer had a significant impact (p = 0.47). The highest state anxiety scores were obtained by women classified as having higher trait anxiety at baseline. Further, the greatest difference in mean STAI-S scores (13.7) was observed as a function of STAI-T scores. Notably, we also observed that state anxiety scores did not differ significantly (p = 0.785) between HPV-negative and persistent HPV groups.
HPV-related quality of life scores (0–100 scale), overall and by domains.
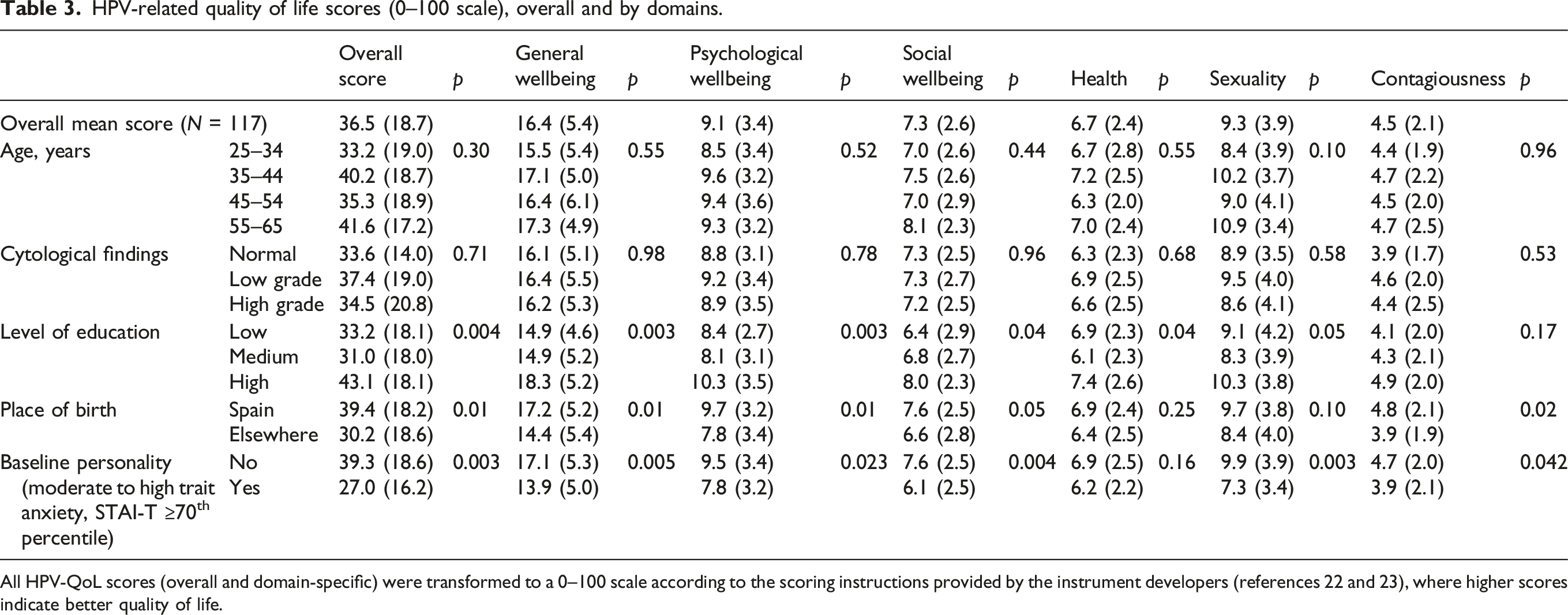
All HPV-QoL scores (overall and domain-specific) were transformed to a 0–100 scale according to the scoring instructions provided by the instrument developers (references 22 and 23), where higher scores indicate better quality of life.
Table 3 reports the analysis of the impact of various variables on quality of life in HPV-positive women. We assessed the overall score and those for each domain and subdomain. Low and medium levels of education were associated with significantly lower scores overall and in all the domains except for contagiousness, indicating poorer quality of life. Place of birth was linked to significantly lower scores overall and in all the domains except for health and sexuality, while higher baseline trait anxiety was related to significantly lower scores overall and in all the domains except for health.
A linear regression model for the overall score constructed with variables showing statistically significant differences in the univariate analysis showed that both high baseline trait anxiety levels (p = 0.008) and a low-to-medium level of education (p = 0.032) were independently associated with lower HPV-QoL scores, indicating poorer quality of life. In this analysis, place of birth no longer had a significant impact (p = 0.16). Detailed results of the multivariable linear regression model are shown in Supplemental Table S2.
Discussion
This study identifies the emotional impact associated with abnormal cervical screening results. Notably, the mean STAI-S score in this subgroup of patients falls at the 65th percentile in the general population. Moreover, we have identified various factors that are significantly and independently associated with high state anxiety scores. Women with a very anxious personality at baseline obtain the highest scores. A first HPV-positive result and a low-to-medium level of education were also significantly related to higher state anxiety.
The subgroup of HPV-positive women had a mean quality of life score of just 36.5 out of 100, and moreover, 3 out of 4 women scored less than 50. These findings suggest that positive screening results are associated with a marked impairment in quality of life in the population studied. Further, this level of impact is considerably stronger than that observed in a study conducted to describe population-based norms for the HPV-QoL in Spanish women based on analysis of 1352 women, in which the mean score was 45.7 (Calvo-Torres et al., 2024). Considering the median score in our sample, at least half of the women showed low quality-of-life scores, indicating substantial impairment. In our study, this poorer quality of life in HPV-positive women was independently associated with high trait anxiety at baseline and a low-to-medium level of education.
Our findings suggest that personality type at baseline is the independent factor with the greatest impact on levels of anxiety around the time of receiving positive screening test results (p < 0.001). The multivariable model explained a moderate proportion of the variance in state anxiety and HPV-related quality of life, consistent with the multifactorial nature of emotional outcomes in the context of cervical screening. To date, the impact of this factor has been studied very little. The only research identified is a qualitative study (McBride et al., 2021a), which found that highly anxious women expressed more negative cognitions related to HPV and experienced behavioural changes; and an analysis of the emotional impact of abnormal cervical and vaginal cytology results (Hellsten et al., 2007), which found that women with greater baseline anxiety reported greater fear of developing cancer (p = 0.001). Quantitative studies exploring factors related to HPV testing and its emotional impact have not considered personality type or its relationship with other factors. In relation to this, in 2021, McBride et al. published a cross-sectional analysis in which three groups were identified with different perceptions of HPV infection, each associated with different psychological effects (McBride et al., 2021b). These authors concluded that analysis of the specific characteristics of each of these groups could help identify which women are most susceptible to experiencing anxiety. Further, a survey carried out among women with a personal history of mental health problems indicated that the psychosocial response and the duration of the HPV-related quality of life impairment seemed to be influenced by their ability to regulate emotions, among other factors (O’Donnell et al., 2024).
A more anxious personality at baseline is also the factor most strongly associated with poorer quality of life (p = 0.008), across all domains, both social and sexual, except that related to concerns about health consequences. Health professionals must take into account that a positive HPV test result (especially HPV 16/18) can negatively influence the sex life of women when they share the results with their partners (Alay et al., 2020). The impact of HPV infection on quality of life has been explored previously using the Human Papillomavirus Impact Profile questionnaire, but not taking into account baseline personality type (Atallah et al., 2022; Leite et al., 2019). This baseline characteristic has also not been considered in more recent studies that have found a greater emotional impact in women with HPV 16/18 positivity than those with other genotypes (Aker et al., 2023; Alay et al., 2020).
In this study, we have detected significantly higher anxiety levels in women with a first positive HPV result (p = 0.03), with no differences in anxiety between women with persistent HPV and those with HPV-negative findings (p = 0.785). This finding is consistent with previous research describing a reduction in the emotional impact by 12 months after the first positive test (Bennett et al., 2021; Marlow et al., 2022; McBride et al., 2020; McCaffery et al., 2004; Sikorska et al., 2023).
Anxiety levels were lower among women with a higher level of education (p = 0.01) and a better quality of life (p = 0.004). A study in Ireland in 3470 women also observed that low educational attainment was associated with a poorer emotional response to HPV screening results (O’Connor et al., 2018). That study used a questionnaire designed by the authors in which women were asked to imagine testing positive for HPV, though it did not analyse the results as a function of baseline personality type. Other studies have not found either anxiety (Maissi et al., 2004) or quality of life (Atallah et al., 2022; Leite et al., 2019) to be related to level of education, but in the populations studied, women with a low level of education were very under-represented, and this might explain the findings. Ciavattini et al. also found a higher level of anxiety in people without university-level education (p < 0.01) (Ciavattini et al., 2021), although they did not assess its effect independently of other factors. A lower level of education is an indicator of a lower socioeconomic status (O’Connor et al., 2018), and is associated with lower health literacy, which may limit people’s ability to understand health-related information. Moreover, a higher level of education may imply greater access to information and strategies to cope better with an HPV-positive result (Leite et al., 2019).
We did not find an association between age and anxiety levels (p = 0.15), unlike previous studies (Ciavattini et al., 2021; Maissi et al., 2004; O’Connor et al., 2018), though none of them have considered baseline personality. Another possible reason for the different results is the type of population studied; in particular, in some cases, the sample may not have been representative due to an underrepresentation of women aged over 50 years (Ciavattini et al., 2021) or people with a low level of education (Maissi et al., 2004), which may have influenced the multivariate analysis. Further, some studies have used unvalidated ad hoc questionnaires to assess anxiety (Ciavattini et al., 2021; O’Connor et al., 2018) or did not perform multivariate analysis to assess the real and independent effect of age (Ciavattini et al., 2021).
No effect of age on quality of life was observed, overall or in the various areas analysed in our research. A study in Portugal assessed the impact of a positive HPV test on quality of life in 194 women, indicating a poorer quality of life in older women, as well as those with greater psychosocial morbidity and emotional suppression (Leite et al., 2019). The sample was not taken from women undergoing cervical screening but rather was composed of women at high or low risk of HPV as assessed at hospital, only 62.4% being considered at high HPV risk, and moreover, they were aged between 20 and 65 years old (and hence, many would not have been eligible for cervical screening). In another study, higher rates of sexual dysfunction were detected in older or younger women undergoing HPV testing depending on the scale used (Sakin et al., 2019). Therefore, emotional impact and quality of life in this context may be related to age, but might also be influenced by other factors such as baseline personality type and socioeconomic status; therefore, when analysing age, we should perform multivariate analysis including these other factors.
Regarding country of origin, previous studies have found differences in the impact of HPV screening results by ethnicity. McCaffery et al. published a qualitative study indicating greater anxiety among Indian- and Pakistani-origin women (McCaffery et al., 2003a), but they did not perform multivariate analysis with other factors in which there were between-group differences, such as educational attainment and marital status. In our linear regression analysis of all the key factors, place of birth did not remain statistically significant for either of the scores studied. A study carried out in 118 Lebanese women found a greater impact on quality of life among Muslim women (p = 0.039), but not as a function of geographical location (Atallah et al., 2022). On the other hand, an Irish study did observe a greater impact in women living in rural areas and those who were Catholics (O’Connor et al., 2018). The emotional impact of abnormal HPV test results does seem to be related to social norms and religious beliefs, and there is a need for further studies with multivariate analysis that includes these social factors and place of origin, to assess their real independent effect.
In conclusion, this study has identified the emotional impact associated with abnormal screening results, using—in addition to an anxiety scale—a specific HPV-related quality of life scale that allows us to analyse various aspects of quality of life. To our knowledge, this is the first quantitative study analysing the independent effect of factors that influence the emotional impact of receiving HPV test results with multivariate analysis to have considered baseline personality. Notably, according to our data, this factor showed the strongest association with state anxiety and quality of life.
Study Limitations
The interpretation of the results and their generalisation are limited by the sample. Although nearly 60% of people contacted participated in the study, making the sample heterogeneous, women with a lower level of education and those born outside Spain were under-represented. Given that we did not detect relationships that have been observed in other studies between emotional impact and age (Ciavattini et al., 2021; Leite et al., 2019; Maissi et al., 2004; Sakin et al., 2019), or ethnic, cultural, or religious characteristics (McCaffery et al., 2003a), our study may not have had sufficient statistical power to assess the effect of these factors, and therefore, more research is warranted to explore these associations.
Contributions
The recruitment of participants through a population-based screening programme provides a heterogeneous sample representative of the real population in our setting. This approach, excluding women with prior contact with health professionals who have informed them about HPV, facilitates the assessment of the specific response to the abnormal cervical screening result.
Studies like this can identify the subgroups of women that are the most vulnerable when faced with an abnormal screening result, and hence, enable the implementation of targeted measures. In our study, baseline personality type and level of education are the two characteristics most clearly associated with women’s emotional response, and both are factors that can be assessed at the time of screening. This makes it possible to identify women at the greatest risk of emotional impact and who should therefore be the focus of strategies to manage this potential impact.
There is a need to improve general awareness of HPV and cervical cancer, including transmission, prevention, treatment, and cancer risk (Anhang et al., 2004; McCaffery and Irwig, 2005). Increasing awareness may improve participation in screening programmes (McCaffery et al., 2003b) and minimise unnecessary negative effects, such as quality of life impairment and psychosexual distress (Bennett et al., 2021). Given the high prevalence of HPV infection, continued research is warranted to analyse modifiable factors and guide the development of intervention strategies aimed at mitigating its impact on women’s emotional well-being and quality of life.
Conclusions
Higher trait anxiety at baseline is the main factor associated with the emotional impact of an abnormal cervical screening result. Testing HPV positive for the first time and educational attainment are also significant factors. The negative emotional impact associated with abnormal cervical screening results may lead to women refusing to be tested, and hence, reduce rates of participation in cervical screening. Therefore, it is key to anticipate these responses by identifying subgroups of women most susceptible to negative emotions and develop strategies for managing them. Studies like ours help identify which women are at greatest risk of experiencing high levels of anxiety in response to an abnormal cervical screening result.
Supplemental material
Supplemental material - The most influential factors in the psychological impact of an abnormal cervical screening result: A cross-sectional study
Supplemental material for The most influential factors in the psychological impact of an abnormal cervical screening result: A cross-sectional study by David del Valle Peña, Ane Murillo Carrasco, Nuria Torres Gonzalez, Idoia Saenz Diez, Gloria Agesta Hidalgo, Edurne Arenaza Lamo, Antonia Dávila Expósito, Cristina Sarasqueta Eizaguirre, Irene Diez-Itza in Health Psychology Open
Footnotes
Acknowledgements
The authors would like to thank Usue Ganboa Goicoechea and Idoia Mugica Arteche for their assistance in the distribution and collection of the surveys and to Laura Martínez Gallardo for her help in developing the original idea.
Ethical considerations
The Ethics Committee for Health Research of the Gipuzkoa Health Area approved the conduct of the study (approval code: DAV-AUD-2021-01) on January 18, 2022, in accordance with the ethical principles outlined in the Declaration of Helsinki. All participants signed an informed consent form prior to completing the questionnaires. The study ensured strict confidentiality, and all data were anonymized to prevent the identification of individual participants. This study is observational in nature and, in accordance with current guidelines, was not required to be registered in advance. No informed consent for publication was obtained, as the study does not include any identifiable personal data.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Biodonostia Health Research Institute [grant number BU 206/22]. The open access publication of this article was supported by Biogipuzkoa Health Research Institute.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analysed during this study are included in this published article. No additional datasets were generated or deposited.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.