
Abstract
The Health-Esteem Model identifies four health-behavior motivational variables that involve thinking about self-determined ideals: health-esteem, goal alignment, goal feasibility, and goal investment. This study provides a psychometric foundation for using this model to understand motivation for exercise. A sample of 401 participants considering or pursuing exercise goals completed an online survey containing a new questionnaire assessing the four Health-Esteem Model variables, along with three measures of exercise and eight existing scales assessing types of personal motivation for exercise. The new scales each produced robust correlations with exercise, explained variance that could not be explained by existing scales, and demonstrated unique associations with scales involving similar types of evaluation. The sales had bell-shaped distributions with high ceilings, adequate test-information curves, and good fit to an expected factor structure. This study provides strong psychometric support for Health-Esteem Model variables which are theoretically important for health intervention research and distinct from existing scales.
Keywords
Engaging in regular exercise and physical activity is one of the most important things people can do for their health (Tsao et al., 2023; U.S. Department of Health and Human Services, 2018), and the amount of exercise that people achieve may be associated with their ideal-prompted thoughts about health. These are thoughts people have when they are prompted to reflect on their own self-determined health-related ideals, such as the health traits they view as most valuable and the goals they wish to achieve. This type of ideal-prompted thought might be important for understanding motivation for health behavior such as exercise, and it is specifically encouraged in many behavioral health interventions, including those based on Self Determination Theory (SDT, Ryan and Deci, 2000, 2008) and Motivational Interviewing (Miller and Rollnick, 2023). Ideal-prompted thoughts are different from the thoughts people have when they are asked to think about externally determined standards or behaviors – which are standards or behaviors that the person did not actively select as being personally relevant. For example, ideal prompted thought would be elicited by the question “Do you identify as having the health traits you most value?” (because one’s valued traits are self-determined), but not by the question, “Do you identify as being someone that exercises?” (because, when asked this way, it is a question about an externally determined behavior). This distinction might be important because self-determination is crucial for satisfying a basic human need for autonomy and it can produce powerful forms of internal motivation (as suggested by SDT, Ryan and Deci, 2000). Consequently, people may experience ideal-prompted thoughts as highly self-relevant. As it stands, however, most of what we know about personal motivational predictors of exercise is based on research studies where people are asked to think about externally determined standards or behaviors.
Choi and colleagues (2017) conducted a review of reviews and identified four key types of personal motivational variables that correlate with engaging in regular exercise. These include one variable involving an evaluation of self-identity, called perceived fitness, and three variables involving evaluations of exercise behavior, including outcome expectations of exercise, self-efficacy (and perceived behavioral control) for exercise, and intent to exercise. These four types of variables are commonly included in models of health behavior change (e.g., Ajzen, 2012; Bandura, 1998; Rosenstock, 1966; Ryan and Deci, 2000; Schwarzer, 2008) and they are typically defined as types of thought about externally determined standards and behaviors. Each variable, however, involves a basic type of cognitive evaluation that could be transformed into ideal-prompted thought if it is used to evaluate one’s own ideals regarding desired health traits and self-determined exercise goals.
For example, perceived fitness involves thinking about how much one identifies with an externally defined standard (being fit), and this becomes a type of ideal-prompted thought called
These types of ideal-prompted thoughts are especially important because they align with proposed mechanisms of action in interventions designed to promote health behavior change, especially interventions based on SDT (Ryan and Deci, 2000, 2008) and Motivational Interviewing (Miller and Rollnick, 2023). In these interventions, clients are encouraged to identify their own self-determined values and goals, and to respond to questions about discrepancies between how they perceive themselves and how they want to perceive themselves (which is health esteem), how their goals align with their values (which is goal alignment), how they evaluate their ability to accomplish their goals (which is goal feasibility), and how they evaluate steps they have taken to accomplish goals (which is goal investment) (Miller and Rollnick, 2023; Patrick and Williams, 2012; Ryan and Deci, 2008). As it stands, research testing interventions based on these models has focused on variables that involve thoughts about externally defined standards and behaviors, such as internal motivation for exercise (or autonomous regulation) and self-efficacy for exercise (or perceived competence) (Ng et al., 2012). A meta-analysis of clinical trials of interventions based on SDT found relatively weak mediation effects when these variables are tested as mechanisms of action (Sheeran et al., 2020). It is possible that these mediation effects are weak because researchers are not capturing the most theoretically relevant types of thought. Ideal-prompted thoughts may be more salient, and the first step toward investigating this possibility is to determine the feasibility of assessing these thoughts.
The assessment of ideal-prompted thought requires a unique process, and this process may have an advantage of providing conceptual separation between the personal factors presumed to motivate exercise and measures of exercise itself. Ideal-prompted assessment requires first asking participants to identify their own self-determined, desired health-traits and exercise goals, and then asking them to respond to questions where they evaluate their selected traits and goals. A person’s desired health traits might include physical traits pertaining to health, fitness, or the body (such as being athletic, attractive, or able-bodied) and character traits pertaining to the ways in which a person pursues goals for health, fitness, and the body (such as being determined, resilient, or disciplined). A person’s goal may be whatever the person identifies when given an option to state an existing exercise goal or to make a goal for consideration. The distinguishing feature of questions assessing ideal-prompted thought is that these questions ask about traits and goals that a person actively selected as being personally relevant, and the questions do not directly ask about exercise itself. Therefore, the content of the questions used to assess types of ideal-prompted thought is different from the content of questions asking about exercise outcomes. In contrast, traditional scales assessing personal motivational factors directly ask people to think about exercise (e.g., “What is your ability to exercise?” or “Do you identify as being someone that exercises?”), and this creates a greater risk that people might answer questions simply by describing how much they exercise. Thus, with traditional scales, there is often ambiguity about the extent to which questions assess personal motivational factors or merely assess the presumed outcome.
Another reason to assess ideal-prompted thought is that this might address psychometric limitations of commonly used scales for assessing personal motivational factors. One problem is that, when scales assess thoughts about externally determined standards and behaviors involving exercise, they tend to have highly skewed distributions, with low ceilings, such that most people score near the positive end of the scale (Courneya et al., 2006; Wilson et al., 2006). This issue can render scales nearly useless in research seeking to identify potential mechanisms for increasing exercise, because if almost everyone scores at the top of the scale, then there is no room for improvement. Another issue is that scales purported to assess theoretically distinct types of motivation for health behavior sometimes corelate greater than .7 (e.g., Chan et al., 2020; Howard et al., 2017). Correlations this large represent acceptable reliability for two measures of the same construct and thereby indicate problems with scale distinctiveness. These issues might be partly caused by scale demand characteristics, which could be prominent if questions about exercise are perceived as questions about a recommended behavior prescribed by experts. This might be mitigated in scales assessing ideal-prompted thought, which could seem more self-relevant to respondents and might elicit more self-reflection.
Taken together, the variables of health-esteem, goal alignment, goal feasibility, and goal investment are a set of ideal-prompted variables that comprise a new conceptional model of motivation for exercise called the Health-Esteem Model. The first step toward exploring this model is to develop scales assessing these four variables. To be maximally useful, scales need to meet several psychometric criteria. First, each scale should have a reasonably bell-shaped distribution with a sufficiently high ceiling. Second, in item response theory (IRT) analysis, each scale should demonstrate high discrimination over a wide range of levels. Third, the four scales should demonstrate factor validity by fitting a 4-dimensional confirmatory factor analysis (CFA) model. Fourth, as a preliminary test of convergent validity, each scale should be correlated with self-report measures of exercise. For example, this includes scales assessing one’s level of physical activity during the preceding week (Sanford and Elkins, 2024), the extent to which a person has established a habit of exercising (Verplanken and Orbell, 2003), and the extent to which a person meets or exceeds CDC guidelines for exercise (2023). Fifth, correlations between scales should not be excessive.
A sixth criterion is that scales should demonstrate theoretically expected associations with other widely used scales that directly assess thoughts about exercise. Each type of ideal-prompted thought is expected to involve a distinct type of cognitive evaluation, and it should have associations with other existing scales involving similar types of evaluation. Although these associations should not be so large to suggest scale redundancy, similarities should be apparent. It should be possible to demonstrate that each ideal-prompted scale captures something that is theoretically distinct, and that each scale produces unique effects that remain significant after controlling for the other types of ideal-prompted thought.
Accordingly, the following hypotheses specify how each type of ideal-prompted thought is expected to have unique associations with two different personal motivation variables measured using existing scales. Because health esteem involves thoughts about identity, it should be uniquely associated with a variable drawn from SDT called integrated regulation, which is the extent to which a person is motivated to exercise because it is part of the person’s identity (Pelletier and Rocchi, 2023). It should also be associated with exercise enjoyment (or “intrinsic motivation”), because exercise identity and enjoyment are closely intertwined and they comprise the two highest forms of internal motivation according to SDT (Howard et al., 2017; Pelletier and Rocchi, 2023). Because goal alignment involves thoughts about consequences, it should be uniquely associated with two variables involving outcome expectations for exercise. This includes beliefs about perceived benefits, as proposed by the Health Beliefs Model (Rosenstock, 1966), and a variable called “instrumental attitude” drawn from the Theory of Planned Behavior (TPB, La Barbera and Ajzen, 2022). Goal feasibility is expected to be uniquely associated with self-efficacy for exercise, which is a key variable proposed in many models of health behavior including Social Cognitive Theory (Bandura, 1998), the Health Action Process Approach (Schwarzer, 2008), TPB (Ajzen, 2012), and SDT (Williams et al., 2006). Also, goal feasibility should be inversely associated with the perceived burden of exercise, which a key variable in the Treatment Adherence Perception model (Sanford and Rivers, 2020). Because goal investment involves judgments about levels of dedication, it should be uniquely associated with intent to exercise, which is a component of TPB (Ajzen, 2012) and with a variable called “action planning,” drawn from the Health Action Process Approach (Schwarzer, 2008).
Overview
This study evaluates a new 21-item questionnaire assessing the four variables of the Health-Esteem Model. Items for the questionnaire were identified in a series of three pilot studies, and items use multiformat response options. This is an approach where different types of response option scales are used for different items. It is used to maximize content validity and reduce response bias, and it can result in relatively brief scales with high discrimination and validity (Sanford and Clifton, 2022; Sanford and Elkins, 2024). The primary objective of the study was to determine if this tentative questionnaire assessing the four variables of the Health-Esteem Model meet all the psychometric criteria listed above when evaluated according to preregistered specifications.
Method
Participants and procedure
A sample of 401 people completed an online survey. Participants were recruited using the CloudResearch platform Connect (Hartman et al., 2023), which maintains a pool of people screened and verified for participation in online research. Members of the pool are required to pass tests of participant engagement and electronic checks for account integrity, and they create profiles by responding to demographic questions. To ensure survey relevance, this study employed targeted recruitment to draw 50% of the sample from people with profiles indicating they currently meet CDC exercise guidelines, and 50% indicating they plan to meet these guidelines in the next 6 months. Participants were also required to pass multiple attention checks embedded in the survey and provide meaningful answers to questions requesting written responses (because the Connect screening process is thorough, only 23 people out of 424 were excluded due to failing these checks). Potential participants were told that the study was about making exercise goals and required indicate informed consent before starting the survey. The study was limited to people residing in the United States. The median survey completion time was 20 min, and participants were paid US $3.25. The protocol for this study was reviewed and assigned exempt status by the Baylor University IRB.
Demographically, the sample identified as 47% female, 51% male, and 2% nonbinary. Regarding Racial/Ethnic identity, the sample included 10% Asian, 13% Black, 7% Hispanic or Latino(a), 66% White, non-Hispanic, and 4% other racial/ethnic categories. The mean age was 37.26 (SD = 12.25). The median household income was between 60 and 80 thousand (with 24% below 40 thousand), 60% reported having a 4-year college degree or more, and 36% were married or cohabiting.
Measures
Health-Esteem Questionnaire
Health-Esteem Questionnaire confirmatory factor analysis standardized loadings.
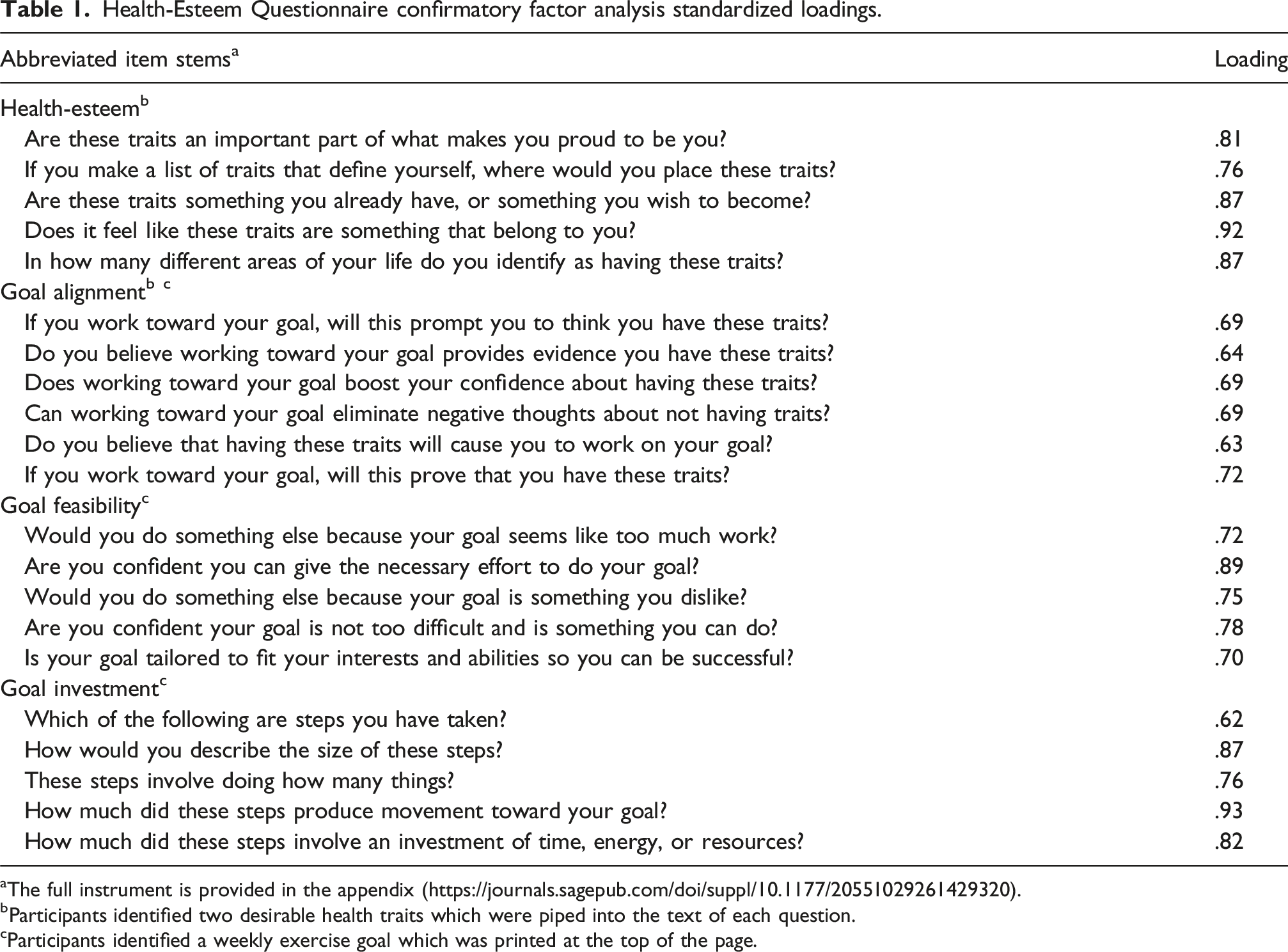
The full instrument is provided in the appendix (https://journals.sagepub.com/doi/suppl/10.1177/20551029261429320).
bParticipants identified two desirable health traits which were piped into the text of each question.
cParticipants identified a weekly exercise goal which was printed at the top of the page.
Descriptive statistics for personal motivation variables.

aFails criteria for scale distribution because more than 25% of cases fall above the reference high score.
bFails criteria for scale distribution because mode is above the reference high score.
This instrument was developed through a process that began with writing a pool of items to capture the content of each scale domain. To maximize breadth and minimize the risk of response format bias, items were written using response options that are unique to each item and tailored to match the language of the question stem (Sanford and Clifton, 2022; Sanford and Elkins, 2024). A series of three pilot studies were conducted (total N = 313) to test items and guide decisions about lists of possible desired traits, item revisions, item additions, and the selection of items for each scale. This produced a proposed 21-item scale and a set of three spare items (one for each of the first three scales), all of which were completed by participants in the present study. Based on a preliminary analysis of data from the present study, two post-hoc modifications were made to the instrument that were deviations from the pre-registered plan. First, an originally proposed 5-item goal alignment scale produced a Cronbach’s Alpha of .76, which was judged to be slightly lower than ideal, and therefore the spare goal alignment item was added to this scale. Second, an originally proposed item for the goal investment scale was judged to be unnecessary and dropped. These modifications raised the reliability and test information curve for the goal alignment scale, and otherwise, these modifications did not noticeably influence results.
Physical activity level
Physical activity was assessed using a standard type of short recall physical activity questionnaire developed by Sanford and Elkins (2024). First, participants were given brief definitions for six levels of physical exertion (sedentary, very light exertion, light exertion, moderate exertion, vigorous exertion, and high intensity exertion), with definitions reflecting distinctions suggested by the American Heart Association classification system (Strath et al., 2013), the DHHS guidelines for physical activity (2018), and the “talk test” for assessing exertion levels (Kwon et al., 2023). Using these definitions, participants were asked to rate their highest level of physical exertion within the last week. If relevant based on responses to this preliminary prompt, participants were given follow-up questions asking them to report the number of days during the last week they engaged in: (a) high intensity exertion, (b) vigorous exertion, and (c) moderate exertion. Using only these top three levels, a weighted physical activity score was calculated equal to: number of moderate exertion days times 1, plus number of vigorous exertion days times 2, plus number of high intensity days times 3. This type of short recall physical activity questionnaire has been found to have adequate test-retest reliability and moderate correlations with accelerometer recordings of physical activity (Craig et al., 2003; Strath et al., 2013).
Exercise habit
The extent to which people have an established habit of engaging in exercise was assessed using a version of the Self-Report Habit Index developed by Verplanken and Orbell (2003), shorted to six items by Morean et al. (2018), with items written to focus on exercise. A sample item is: “Exercising is something that I do without thinking.” Each item is rated on a 7-point agreement scale, and items are summed to produce a total score (Reliability and descriptive statistics are in Table 2).
CDC guideline adherence, perceived benefit, and perceived burden
The Treatment Adherence Perception Questionnaire (TAPQ, Sanford and Rivers, 2020) was used to assess three variables: (a) adherence to CDC guidelines for exercise, (b) perceived benefit of following guidelines, and (c) perceived burden of following guidelines. The CDC exercise guidelines include two options based on amounts of either moderate exercise or vigorous exercise, and before completing the TAPQ, respondents were asked to read the guidelines and select which option seemed most applicable. Their selected version of the guideline was printed at the top of subsequent pages containing questions.
Exercise enjoyment, instrumental attitude, self-efficacy, and exercise intention
Four variables were assessed using an instrument developed by Courneya and colleagues (2006) for assessing constructs relevant to TPB.
Integrated regulation
Participant’s levels of integrated regulation were assessed using the integrated regulation subscale from the Behavioral Regulation in Exercise Questionnaire-3 (Markland and Tobin, 2004; Mullan et al., 1997; Wilson et al., 2006). This instrument is a widely used instrument designed to assess types of motivation proposed by SDT, and the integrated regulation scale includes four items (e.g., “I consider exercise part of my identity”), which are each rated on a 5-point scale and summed. Scale reliability and descriptive statistics are in Table 2.
Action-planning
Participants completed a version of the Exercise Goal-Setting Scale (Rovniak et al., 2002) which was modified based on results from a psychometric study by Elavsky and colleagues (2012) to include only five items that produced strong loading in factor analysis. Drawing from the Health Action Process Approach (Schwarzer, 2008), this scale assesses the extent to which participants have engaged in action planning, which involves taking steps to make effective goals for exercise (e.g., “I usually set dates for achieving my exercise goals”). Items are rated on a 5-point scale and summed. Scale reliability and descriptive statistics are in Table 2.
Results
Except for analyses labeled as “preliminary” or “exploratory,” and aside from the one deviation listed above, all analyses were conducted and evaluated according to a preregistered plan. This report does not include analyses identified in this plan as “secondary and non-essential.”
A preliminary analysis was conducted to describe participant responses to prompts asking them to identify goals and desired health traits. The average goal description was 28.25 words (median = 25 words, SD = 16.25); 78% of participants described goals they already established prior to the study, and 97% of goals mentioned a numerical value to indicate a specific amount, frequency, or count of a target goal behavior. The most popular desirable physical traits (selected for inclusion on one’s list by at least 10% of the sample) were “healthy” and “in shape,” and the most popular character traits were “disciplined,” “determined,” and “consistent.” When participants were asked to identify their top two traits, 45% identified a pair of physical traits, 48% identified one physical and one character trait, and 7% identified a pair of character traits.
Criterion 1
The first criterion for evaluating the new instrument was that each scale would have a reasonably bell-shaped distribution with a sufficiently high ceiling. A pre-registered plan for testing this criterion was established based on a review of existing measures and a judgement of what would be sufficiently stringent yet reasonable. The approach involved calculating a reference high score for each scale that corresponded to 80% of the scale’s observed range: [minimum + (maximum – minimum) (.8)]. The preregistered criterion was that at least 75% of scores should fall below the reference high score, and the scale mode should fall below the reference high score. Results from this analysis are reported in Table 2 and all four new scales produced excellent distributions that clearly exceeded the criterion. In addition, histograms for each scale are depicted in Figure 1, and they all appear reasonably bell shaped. For comparison, an exploratory analysis was conducted to evaluate the eight existing scales directly assessing thoughts about exercise, and six of these scales failed to pass this criterion. Five of these scales were skewed to the point that more than 25% of cases fell above the reference high score, six had modes above the reference high score, and four had modes at the scale ceiling. Health-Esteem Questionnaire scales: histograms and item response theory test information curves.
Criterion 2
The second criterion was that scales would provide high discrimination over a wide range of levels. To test this criterion, a graded response IRT model was estimated for each scale (Samejima, 1969), and test information curves for each scale were plotted. Each scale was expected to have a test information curve that exceeded a value of 5 (which corresponds to a reliability of .80) for a range of levels spanning one standard deviation above and below the mean (Sanford and Rivers, 2020). Test information curves are depicted in Figure 1, and results for the health-esteem, goal feasibility, and goal investment scales clearly exceed this criterion. The goal alignment scale just barely passed; however, these results are exploratory because this scale was lengthened post-hoc (as described above), and the originally proposed shorter scale would have failed.
Criterion 3
The third criterion was that the 21-item instrument would fit a 4-dimensional CFA model. To test this expectation, a CFA model was estimated using mean and variance adjusted weighted least squares. Items for each scale were assigned to be indicators of a single factor; the four factors were allowed to correlate, and no error variances were allowed to correlate. Evaluation criteria were that the model would produce a comparative fit index (CFI) value greater than .95, and a standardized root mean residual (SRMR) less than .09 (Hu and Bentler, 1999), with all standardized loadings greater than .55 (Comrey and Lee, 1992). Results met all these expectations. The model produced a good fit (scaled χ 2 (df = 183) = 620.69, p < .001, CFI = .96, SRMR = .05, RMSEA = .08). Standardized loadings are listed in Table 1, and they range from .62 to .93.
To support factor distinctiveness, it was expected that correlations between factors would be less than .85 (Brown, 2015) and less than the square root of the average variance extracted for the factor with the weakest loadings. These expectations were met. Factor correlations ranged between .48 and .67, and these were all below .85, and below the root average variance extracted for the goal alignment factor, which was .68. To test factor distinctiveness further, an alternate 3-dimensional model was estimated in which the two highest correlating factors (health-esteem and goal alignment) were combined into a single factor. This alternate model failed to produce a good fit (scaled χ 2 (df = 184) = 1048 .87, p < .001, CFI = .92, SRMR = .07, RMSEA = .11). Consistent with pre-registered expectations for factor distinctiveness, the fit of this alternate 3-diminsional model was significantly worse than the original 4-dimensional model (scaled chi-squared difference (df = 1) = 181.52, p < .001).
Criterion 4
Correlations between variables.

Note. p < .001 for all correlations in the table except as indicated otherwise (**p < .01, and n.s. = not significant). Bolded correlations are convergent validity correlations expected to be significant.
aPartial correlations with health-esteem control for integrated regulation and exercise enjoyment.
bPartial correlations with goal alignment control for instrumental attitude and perceived benefit.
cPartial correlations with goal feasibility control for self-efficacy and perceived burden.
dPartial correlations with goal investment control for exercise intention and action planning.
Criterion 5
The fifth criterion was that intra-instrument correlations between each of the four scales on the Health-esteem Questionnaire would not be excessive. Specifically, it was expected that all correlations would be significantly less than .7 (which would be acceptable reliability for two measures of the same construct). Confidence intervals were placed around each of the six intra-instrument correlations reported in the top three rows of Table 3. In line with the pre-registered criterion, none of the confidence intervals exceeded .7.
Criterion 6
Standardized beta weights from regression equations.

Note. Bolded effects are incremental validity coefficients expected to be significant.
*p < .05, **p < .01, ***p < .001.
Although the previous analyses demonstrated that each new scale was uniquely associated with a pair of existing scales involving similar types of evaluation, these results could raise the question of whether the new scales merely have redundant functions with these existing scales. To address this question, a post-hoc, exploratory analysis was conducted in which all the convergent validity correlations with measures of exercise were re-estimated as partial correlations. Each partial correlation indicated the association between a measure of exercise and one of the new ideal-prompted scales after controlling for the two existing scales identified as involving similar types of evaluation. These results are reported in Table 3. The partial correlation between goal investment and exercise habit formation became non-significant after controlling for existing scales, and the other 11 partial correlations remained significant (ranging from .13 to .29).
Discussion
This study provided preliminary validation evidence for a new instrument assessing four types of ideal-prompted thought called health-esteem, goal alignment, goal feasibility, and goal investment. These scales are unique in that they capture thoughts people have when they are prompted to think about their own, self-determined desired health traits and goals. The general importance of these scales was indicated by the fact that all four scales produced robust correlations with multiple measures of exercise. In addition, each scale demonstrated unique, theoretically expected associations with other existing scales involving similar types of cognitive evaluation. The new scales also provided incremental benefit over these existing scales by explaining unique variance in exercise. Compared to existing scales, the new ideal-prompted scales had improved distributional properties with sufficiently high ceilings. Three of the scales (esteem, feasibility, and investment) clearly surpassed a criterion in IRT analysis to provide high discrimination across a broad range of levels; however, the goal alignment only passed this criterion because an item was added to the scale post hoc. The four scales fit a 4-dimensional CFA model, and results indicated that each factor was reasonably distinct. Taken together, these results provide a foundation for continued work investigating the Health-Esteem Model of motivation for exercise goals.
This study demonstrates the feasibility of assessing ideal-prompted thought, which is a theoretically important type of thought that poses unique assessment challenges. Because this type of thought involves evaluating self-determined goals and standards, it is expected to be motivating (Ryan and Deci, 2000), and it is specifically targeted in interventions for increasing exercise (Miller and Rollnick, 2023; Patrick and Williams, 2012; Ryan and Deci, 2008). It poses unique assessment challenges, however, because people need to be prompted to determine their own schemas for desired health traits and their own goals. In this way, each participant responds to questions based on different self-determined standards and goals. This creates a risk that questions could have different meanings for different people, which in turn could produce high measurement error, and poor psychometric results (Nunnally and Bernstein, 1994). These concerns are generally allayed by the results of the present study, because the CFA results were strong, scales were able to pass stringent criteria in IRT analysis, and each scale produced a distinct pattern of association with other types of personal motivation variables. This level of psychometric rigor is uncommon in research on motivation for health behavior. For example, the primary scale most commonly used to measure exercise motivation based on SDT was validated in a study using more lenient CFA evaluation criteria, no IRT analysis, and no test for scale distinctiveness (Wilson et al., 2006).
A notable theoretical feature of the Health Esteem Model is that it expands on ideas proposed in SDT (Ryan and Deci, 2000). According to SDT, a key personal motivational variable predicting exercise is integrated regulation, which involves being motivated because exercise is part of one’s identity (Pelletier and Rocchi, 2023). Integrated regulation is like health-esteem because both variables pertain to identity, and accordingly, the present study found a large correlation between these two variables. The general importance of identity is demonstrated in previous research showing that integrated regulation is a strong form of motivation associated with long-term persistence in physical activity (Ng et al., 2012; Teixeira et al., 2012; Wang and Hagger, 2023). However, previous research on SDT has relied upon scales (Such as the BREQ, Markland and Tobin, 2004; Mullan et al., 1997; Wilson et al., 2006) that ask respondents to evaluate exercise behavior rather than to evaluate their self-determined standards and goals. This misses a potentially important part of the theoretical model, and the item content is not clearly distinct from the content of questions assessing how much a person exercises. In contrast, the health esteem scale asks about self-determined standards, and does not directly ask about exercise. Importantly, it still explained unique variance in all three exercise outcomes after controlling for both integrated regulation and exercise enjoyment (or intrinsic regulation), which are the two highest forms of motivation according to SDT (Pelletier and Rocchi, 2023). It is also notable that Health-Esteem Questionnaire scales were not excessively correlated, whereas SDT scales assessing different types of motivation often correlate greater than .7 (Howard et al., 2017). In sum, the health esteem construct appears to make an incremental contribution to a large base of work using SDT to explain motivation for exercise.
The Health Esteem Model also builds on TPB (Theory of Planned Behavior, Ajzen, 2012), which is one of the most widely used frameworks for explaining motivation for exercise (Hagger et al., 2002). Each of the new scales demonstrated unique associations with scales drawn from TPB, which includes exercise enjoyment (or affective attitude), instrumental attitude, self-efficacy (or perceived behavioral control), and intent. The goal feasibility scale produced especially strong associations with all the TPB scales. Taken together, these associations are consistent with the expectation that these scales are capturing similar types of cognitive evaluation, yet not so strong to suggest that scales are assessing identical constructs. A key difference is that the four new scales all produced reasonably bell-shaped distributions, whereas the four TPB scales were all highly skewed. This is a known issue with TPB scales, and previous efforts to remove this skew by rewriting items have not proven successful (Courneya et al., 2006). One speculative explanation is that questions asking about eternally determined behaviors have high demand characteristics, whereas questions assessing ideal-prompted thought might be perceived as more self-relevant and elicit more self-reflection. If so, the new Health-Esteem Questionnaire might provide a particularly meaningful method for capturing types of cognitive evaluation that share similarity with TPB variables.
Notable limitations of this study are that it was cross-sectional and that all the measures of exercise were based on self-report. The study cannot determine direction of effect, cannot determine if changes in thinking produce changes in exercise, and cannot determine how closely self-reported exercise levels would match more objective measures. In addition, this study used a sample of people registered to participate in psychological research, and it is not clear how well results might generalize to other populations. All participants were able to identify exercise goals, and the scales would not be relevant for people with no interest in thinking about exercise goals. It is also important to note that one item was added to the goal alignment scale post hoc. This modification influenced results of the IRT analysis, in which scales were expected to produce test information curves analogous to a reliability of .8 across a wide range of goal alignment levels. Although the goal alignment scale would clearly meet a less stringent criterion of merely requiring a Cronbach’s alpha of .7, replication is needed before concluding that it meets the more stringent IRT criteria.
Taken together, these limitations indicate that further research is needed before we draw strong conclusions about the Health-Esteem Model. There are already many well-established models of health-behavior change, such as SDT (Ryan and Deci, 2000, 2008) and TPB (La Barbera and Ajzen, 2022). To be useful, the Health-Esteem Model needs to demonstrate an incremental contribution beyond these existing models. While results of the present study are promising, results from this single cross-sectional study using self-report measures are far from definitive. It will be especially important to replicate results, to test the model in studies using longitudinal designs, to use other more objective measures of physical activity, and to support the coherence of the goal alignment construct. Accordingly, the present results supporting this new model need to be interpreted as being preliminary.
A promising direction for future research may be to consider use of the Health-Esteem Questionnaire as a component of intervention programs for increasing exercise. The ideal-prompted scales on this instrument assess a type of thought that is self-referential, that is presumably modifiable, and that is commonly targeted in interventions to increase exercise (Miller and Rollnick, 2023; Patrick and Williams, 2012; Ryan and Deci, 2008). Consequently, the Health-Esteem Questionnaire may be especially well suited for use as a tool for facilitating therapeutic discussion. For example, if a participant in an intervention program receives a score indicating low health-esteem, this may facilitate a discussion about the participant’s schema of desirable health traits and a specific consideration of the extent to which the schema is realistic and beneficial. It could also facilitate discussion of ways in which the participant may be employing a negative self-evaluation bias. Similarly, low scores on the goal-alignment or goal-feasibility scales could facilitate discussion of ways to modify goals. Along this line, it is notable that several participants in the present study utilized an option to provide comments at the end, and they spontaneously stated that participation caused them to change how they think about their own goals or standards. A speculative possibility is that an effective component for an intervention program could involve participants simply completing the Health-Esteem Questionnaire and discussing results.
The Health-Esteem Questionnaire may also function as a valuable assessment tool in future research testing intervention programs for increasing physical activity. According to the NIH Science of Behavior Change approach (Nielsen et al., 2018), a crucial first step in intervention research is to develop scales assessing purported mechanisms of action. The Health-Esteem Questionnaire is unique in its focus on ideal-prompted thought, which captures a type of thinking specifically proposed to function as a mechanism of action for interventions based on SDT (Ryan and Deci, 2000, 2008) and Motivational Interviewing (Miller and Rollnick, 2023). Thus, the Health-Esteem Questionnaire fills a crucial need because it both assesses purported mechanisms of action and has strong psychometric properties. As such it may provide an ideal measure for assessing participant progress in studies designed to test interventions and clarify mechanisms. In sum, the Health-Esteem Questionnaire has application potential in health behavior interventions, both as an instrument for assessing purported mechanisms of action and as a tool for facilitating therapeutic discussion. Results of the present study provide a foundation for investigating these possibilities.
Supplemental material
Supplemental Material - The health-esteem model of motivation for exercise goals: A preliminary study
Supplemental Material for The health-esteem model of motivation for exercise goals: A preliminary study by Keith Sanford in Health Psychology Open.
Footnotes
Ethical considerations
The protocol for this study was reviewed and assigned exempt status by the Baylor University IRB.
Consent to participate
Participation in this study involved completion of an online survey. Potential participants viewed a website page providing a description of the study and were required to click a button indicating consent before starting the survey.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported, in part, through internal department funds.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.