
Abstract
Living with long-term conditions requires adaptation and coping. It is unclear how young adults – often still in unstable social relationships – and their partners or friends cope with the challenges of a long-term condition. Our study aimed to explore how young adults and their friends or partners arrange themselves with this situation. In a comparative design, we interviewed 24 young adults with differing long-term conditions and 30 of their friends or partners in episodic interviews, which we analyzed with thematic coding. We identified four patterns of dyadic arrangements of coping for both sides: Joint Management and Supportive Arrangement show congruence and cooperation in dealing with the condition. Divergence and Diffusiveness illustrate conflicts and tensions. Our results show the importance romantic partners or close friends can have for dyadic disease management in young adulthood and suggest including friends and partners in training courses on long-term conditions and in professional support.
Introduction
Long-term conditions are among the most frequent causes of death and disability in Germany and worldwide (Hacker, 2024). They are characterized by their persistence as well as by a dynamic course determined by a (rapid) alternation of stable, unstable and crisis-prone phases (Schaeffer and Haslbeck, 2023; Whittemore and Dixon, 2008). In order to control the course of the disease as much as possible and avoid complications of it, people diagnosed with long-term conditions must monitor and manage symptoms, obtain adequate information about their disease and its treatment, and cooperate in the care process (Byron et al., 2020; Desborough et al., 2020; Eassey et al., 2020). At the same time, people experiencing long-term conditions have to deal cognitively with their illness and learn to manage the strong emotions that occur in the disease process (Visagie et al., 2024). In addition, they face the challenge of integrating the disease into everyday life and adapting it to disease-specific requirements (Ambrosio et al., 2015). Due to the changeable course of long-term conditions, challenges to coping and self-management skills arise repeatedly in new ways.
Long-term conditions affect not only the people themselves who were diagnosed, but also their social environment. Close caregivers, especially partners, often have a comparable degree of distress as the people with the long-term condition experience (Bertschi et al., 2021). Partners suffer from impaired well-being and experience fears and insecurities in the face of their partner’s diagnosis. Beyond the individual challenges faced by people with the long-term condition and their caregivers, the disease also calls into question the interaction patterns, roles and responsibilities established in the relationships. For example, close relatives or partners of the person with the diagnosis often have to adjust to taking on nursing tasks as the disease progresses (Engblom-Deglman and Hamilton, 2020; Neate et al., 2019). Long-term conditions can occur at any age. This article focuses on young adults with long-term conditions (YALTCs) – thus on an age group that has rarely been the focus of research compared to children and adolescents or old people with long-term conditions (Rasalingam et al., 2023; Wilson and Stock, 2019).
Literature review
Long-term conditions in the developmental phase of young adulthood
Young adulthood, the period between the ages of 18 and 29 (Arnett, 2024), is seen as a time of searching and exploring, a time of self-focus and the (yet) incomplete search for identity. Young adults try out many things and discard their ideas and life plans again (Arnett, 2024). From a relational point of view, young adulthood is determined by the development of even closer and more intimate relationships with peers compared to adolescence.
Friendship relations between young adults may be stronger than relations between family members (Barry et al., 2016). Because of the frequent transitions in young adulthood – e.g. from school to (university) training and from there to the labor market – as well as changes in the personal living environment (e.g. moving to a different town for studying), previous friendship networks are becoming fragile at the same time (Santucci et al., 2022). New friendships are formed, often mediated by existing friendship dyads. However, building romantic relationships is central to young adults (Arnett, 2024).
Romantic relationships in young adulthood can differ significantly in terms of their stability and commitment. For example, there are relationship patterns that are characterized by great instability, non-commitment and exploration, as well as relationship patterns that show a high degree of consolidation or patterns that are characterized by emotional warmth and support, but also a high level of conflict (Beckmeyer and Jamison, 2021).
If young adulthood as a whole is a period of instability (Arnett, 2024) and friendships or romantic relationships are easily irritated in young adulthood, it can be asked as to the extent to which young adults cooperate with peers or act more individually in dealing with a chronic condition.
Existing research has drawn a complex picture of the importance of peers in the coping and self-management process of YALTCs. For young adults with cancer, for example, it has been found that family members and partners are the main source of support (Hauken and Larsen, 2019; Iannarino, 2018). Relationships with friends, on the other hand, have been lost, especially as the duration of the disease increases (Hauken and Larsen, 2019; Lidington et al., 2021). However, studies have also shown that young adults with cancer had difficulty establishing and maintaining romantic relationships (Rabin, 2019) and that romantic partners had to justify themselves for sticking to their relationships with partners with cancer (Iannarino, 2018). Again, YALTCs may have had difficulty accepting support because it would have meant disclosing the condition to peers and thus revealing themselves as different (Kirk and Hinton, 2019).
Long-term conditions and dyadic coping
When long-term conditions become a challenge for the patients and their close caregivers, they require not only individual but also joint adaptation and coping efforts. Research on dyadic coping focused on how patients with a long-term condition and their caregivers dealt with (illness-related) stress as a couple. Dyadic coping refers to “(…) how partners communicate about stress, support each other in times of stress and deal with stressors together” (Weitkamp et al., 2021). According to the systemic transaction model (Bodenmann et al., 2016), dyadic coping represents a dynamic, transactional process in which the experience of stress and the coping of both partners of a dyad are interdependent. As a result of their review, Weitkamp et al. (2021) have shown positive effects of dyadic coping on physical health, well-being and relationship satisfaction.
Various models of dyadic coping have been discussed in the literature, but these are not discussed here (as an integrative review of such models: see Falconier and Kuhn, 2019). Weitkamp et al. (2021) distinguished four forms of dyadic coping following Bodenmann’s systemic transaction model: a) common dyadic coping, both partners in a couple have been affected by the stress and approach coping together as a unit; b) delegated dyadic coping, in which one partner has taken on tasks to reduce the stress load of the primarily stressed partner; c) supportive dyadic coping, in which one person has been primarily affected by the stressful event and the other person has been supportive; d) negative dyadic coping. In the latter case, the partner has tried to help the affected person, but ineffectively, e.g. by making disparaging statements, trivializing stresses, appearing distant or behaving in an overly protective manner (Bodenmann et al., 2016; Falconier and Kuhn, 2019; Weitkamp et al., 2021).
From a more general point of view, dyadic coping is influenced by contextual factors, such as relationship quality or the specific disease and its course, as well as sociocultural factors such as gender (Berg and Upchurch, 2007). For example, studies have shown greater cooperation between couples of a male patient and of a female support person. Women initiated more support interactions and offered a wider range of support services than men (Berg and Upchurch, 2007; Ruark et al., 2024). Women were also more involved than men in the disease management of their partners: In the case of type II diabetes, for example, they provided more support than men and took it for granted to take on the caring role. However, women also controlled their partners’ dieting behavior more closely (August et al., 2021; Dimova et al., 2021).
Existing studies on dyadic coping have focused on one type of conditions such as cancer (Acquati and Kayser; 2019; Opsomer et al., 2019); coronary artery disease (Kitko et al., 2015; Rapelli et al., 2021); neurological long-term degenerative conditions such as Parkinson’s disease (Manceau et al., 2023) or multiple sclerosis (Carberry et al., 2024; Desborough et al., 2020) or acquired brain injuries (Engblom-Deglmann and Hamilton, 2020; Jeyathevan et al., 2019). In addition, studies usually have referred to relationships of couples who had lived together and/or had been married for many years (Acquati and Kayser, 2019). In contrast, only a few studies have dealt with dyadic coping of younger couples. These studies pointed to a particular susceptibility of younger couples to disease-related distress, as (collaborative) coping skills only developed in the course of life (Acquati and Kayser, 2019).
Limitations of existing research and the current study
Studies looking at dyadic coping of younger couples have often focused on the age group of middle-aged adults of ≤45 years (Acquati and Kayser, 2019; McCarthy and Bauer, 2015) and ≤50 years (Fergus et al., 2022). However, in young adulthood, the period between the ages of 18 and 29 (Arnett, 2024), long-term conditions have become also increasingly prevalent (Wilson et al., 2021). Questions such as whether and to what extent YALTCs and their close caregivers arranged themselves as a dyad in order to cope with and manage the condition has so far only been marginally addressed (e.g. Gorman et al., 2020).
A recent study on romantic relationships of young adults with chronic pain has looked at how young pain patients and their partners perceived and experienced their relationship with each other and the impact chronic pain had on the relationship (Carter et al., 2023). Results of this qualitative study showed 1) the importance of an exchange characterized by reciprocity - “recognized and understood by couples as a key part of their relationship“ (Carter et al., 2023: 10), such as joint pain management - for the continuation of the romantic relationship. 2) Reciprocity “includes an exchange of emotions, thoughts, and behavior and is a central factor in romantic relationships among adults from diverse backgrounds“ (2023: 10).
For our own research this role of reciprocity and exchange in romantic relationships and coping with long-term conditions has been a strong focus similar to Carter et al. (2023). In researching Google Scholar, Pubmed or EBSCOhost, we have only found studies that dealt with dyadic coping in young adults in exceptional cases. We have not identified any study in which the dyadic coping model has been applied to other relationships such as friendships.
The present article addresses the research gap identified above based on our own current study. Different from Carter et al. (2023), our study focused less on relationship management and more on the questions of the extent to which young adults and their peers have come to terms with the disease as a dyad; how this was related to the type of peer relationship (friendship or partnership) and the long-term condition experienced, and what possible consequences resulted from the nature of the arrangement for the peer relationships.
Aims
We have concentrated in our study on YALTCs and their peers
1
and their dyadic perspectives on coping with long-term conditions and self-management. Following the short review of the literature above, a higher degree of informality in social relationships can be assumed in comparison to older, long-term married couples, who have so far been the focus of studies on dyadic coping. Questions about how dyadic coping developed in new relationships (Berg et al., 2020) or in non-marital relationships (Ferraris et al., 2022) have been neglected so far. We have started from this research gap and focus in this article on dyadic arrangements of coping between YALTCs and their friends or partners with whom they have been living together for a comparatively short time. In our study we did not refer to a single long-term condition – as many studies on dyadic coping did – but to several of such conditions that differ in terms of the demands and needs associated with them (see below). The following questions were the focus of our study: What patterns of dyadic arrangements of coping can be identified in dealing with the disease? Which interplay and divergences between YALTCs and peers characterize these patterns? To what extent have the patterns of the arrangement been influenced by components such as the type of peer relationship the exact disease entity as well as gender? Which consequences can be derived from the different dyadic arrangements for the relationship between YALTCs and peers?
Methods and methodology
Design
In a qualitative comparative cross-sectional design (see Flick, 2023), young adults with long-term conditions (self-reported) and their peers have been interviewed using episodic interviews (Flick, 2022). The research started from theories from health psychology and medical sociology such as the theory of social representations of health and illness (Flick, 1998; Herzlich, 1973; Moscovici, 1973). This social constructionist approach is concerned with how social groups differ in their ideas about a particular issue and how particular circumstances of their everyday lives and sources of knowledge influence these ideas in daily life.
In the context of the present article that approach has been referred to how young adults with various long-term conditions and their peers (friends or partners) developed differing group-specific ideas about coping with long-term conditions.
Ethical approval
The ethics committee of the Freie Universität Berlin approved the research proposal for the first three years of funding on 21 September 2020 (approval no 038/2020). When we applied for an extension of the funding for another three years, the extension proposal was approved again on 05 March 2024 (approval no 005/2024). All participants received written information prior to the interview, informing them about the background of the study, its objectives, and the procedures for data collection and analysis.
Participants were assured that the gathered data would be confidential and anonymised. In addition, participants were assured that they could withdraw from the study at any time and for any reason without fear of negative consequences. On the basis of that information, they gave written consent to participate.
Field access and sampling
In the study, sampling was applied in two steps. First, YALTCs with one of the following long-term conditions were included to cover a wide range of disease related experiences: Cancer, widely discussed as a “death sentence” (Moser et al., 2021) and therefore frightening for both the diagnosed people and their peers (Knox et al., 2017). Diabetes type 1 requiring constant management with significant effects on everyday life and routines (Wiebe et al., 2018). Inflammatory bowel disease (IBD), seen a social taboo and associated with negative feelings for the sufferer including fear, shame and disgust (Polak et al., 2020). Some cases of YALTCs with rare, life-limiting diseases (cystic fibrosis, end-stage kidney disease) were also included. YALTCs as well as friends or partners were confronted by these diseases with their own finiteness and with the need to adapt everyday life and life plans to strong imponderables and a perhaps rapidly changing health situation (Helms et al., 2015).
For accessing the field and participants we searched for self-help groups, patients’ organizations, advice centers, (rehabilitation) clinics, and healthcare services addressing patients with one of the above-mentioned diseases and specifically YALTCs. We informed relevant decision-makers in these groups and institutions about the study and asked to post calls for participation for it on their websites or to forward these directly (via social media) to YALTCs. Student representatives of universities were asked to provide students with the study information in general. YALTCs who had learned about the study and were interested in participating contacted the researchers to schedule an interview.
Second, peers were involved by asking the YALTCs at the end of their interviews to refer a good friend or partner for an interview if these peers were subjectively relevant to them in the course of the long-term condition. We gave the YALTCs written study information for this purpose, which we asked them to forward to their peers. If the peers were interested in participating, they made an appointment for an interview with the researchers.
We left it up to the YALTC to decide who should be interviewed as their ‘peer’ and did not define other criteria for the peer sample. Our primary focus was on the YALTCs living with their conditions. The role of the peers was studied as a part of the YALTCs’ situation of living. So, we kept the YALTCs in the study as a whole, if they could not or did not want to arrange the contact to a peer for an interview.
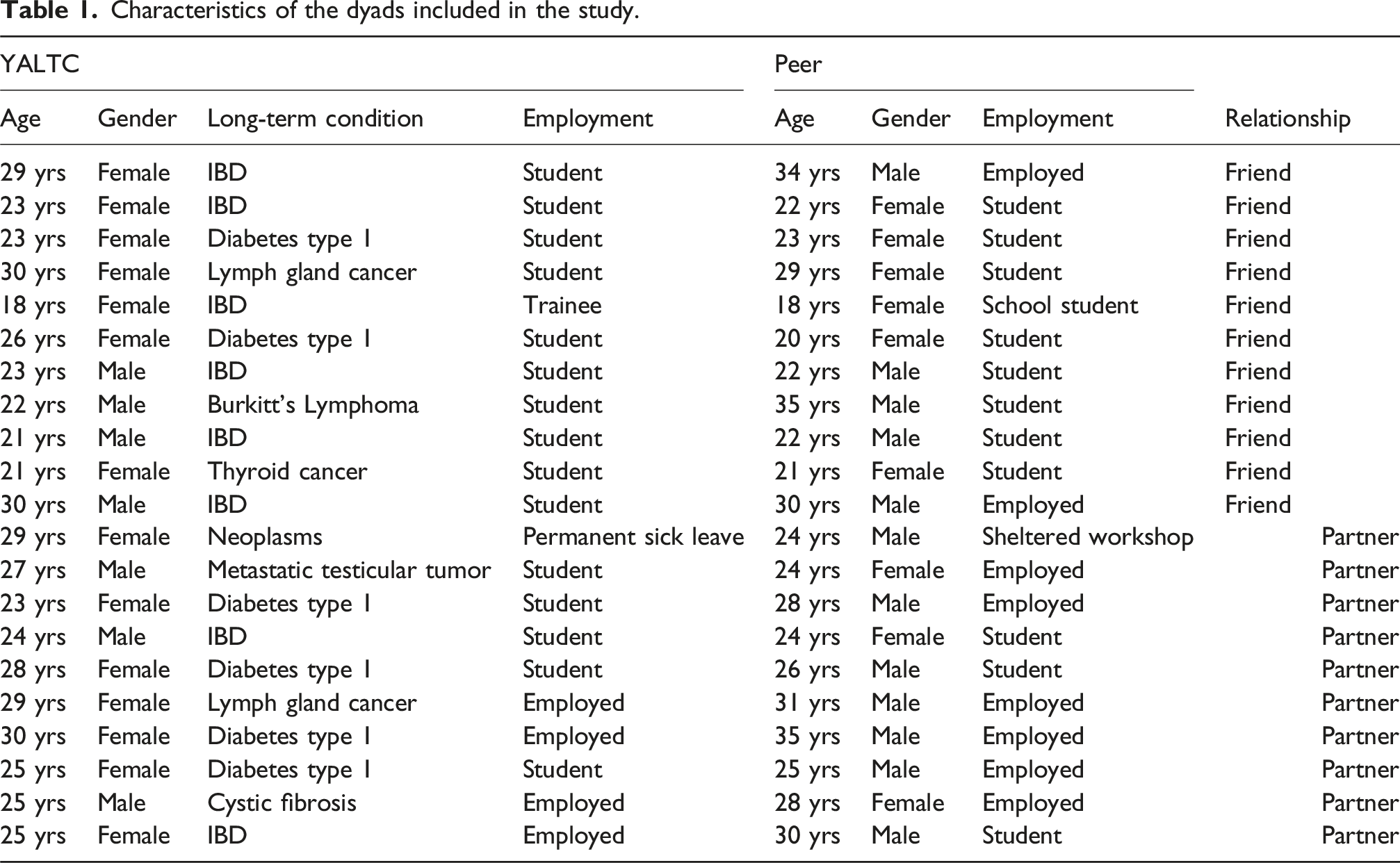
Characteristics of the dyads included in the study.
Overview of the cases in which two or three peers were interviewed or in which the YALTCs’ interviews are missing.
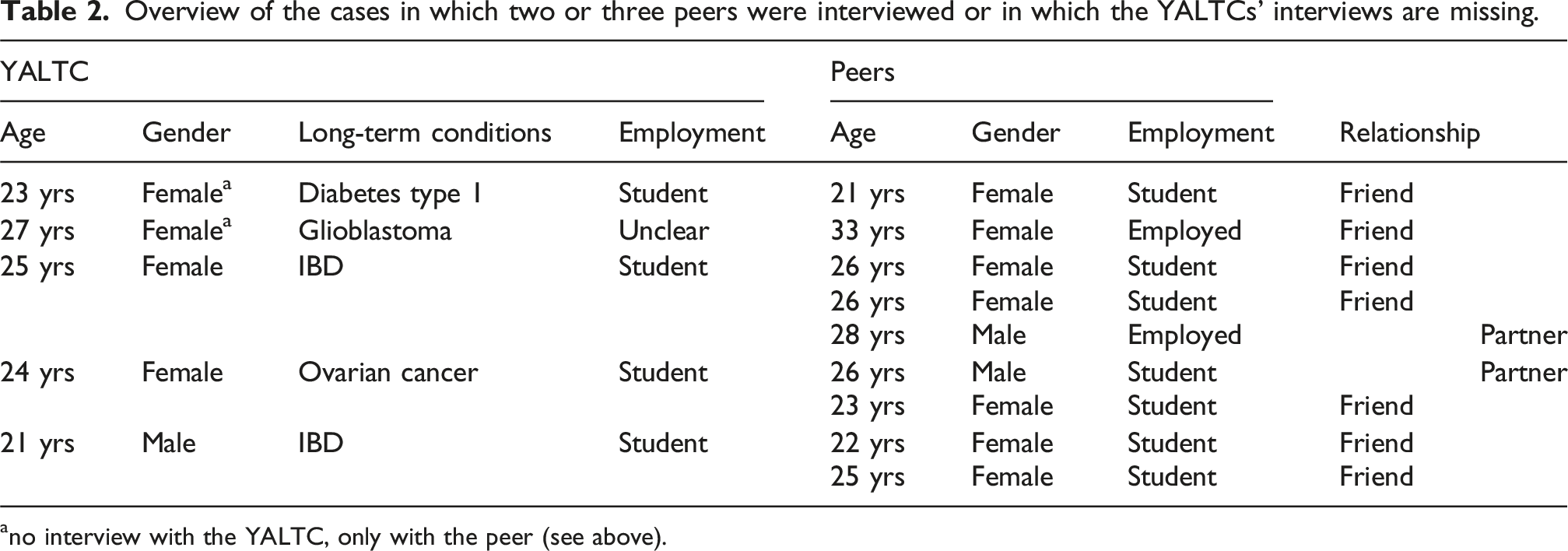
ano interview with the YALTC, only with the peer (see above).
In total, we were able to recruit N = 30 peers for the study (N = 16 female and N = 14 male) between December 2021 and October 2022. The interviewed peers were between 18 and 35 years old (mean: 26 years).
18 of the peers were YALTCs’ friends, 12 were romantic partners. At the time of the interview, 18 peers were studying, 10 were working (six of them have finished their studies), one peer is a high school graduate, one peer was on sick leave due to depression. Two peers had a migration background (Russian, Austrian). Although we kept YALTCs who did not mediate a peer for being interviewed in the study, for the current article about dyadic views on disease management and self-management, we only selected and included those YALTCs who have referred a peer to us for an interview. If a YALTC has mediated more than one peer, we analyzed the dyadic relationships of the YALTC to each peer but not the relation between the peers. We also included the two cases in which the peers were interviewed but the YALTC could not be interviewed because she was not longer alive or the recording of interview with YALTC had not worked.
Data collection
The data were collected by a female researcher (Diploma in socio-therapy; PhD) by means of episodic interviews (Flick, 2022). Two interview partners (one YALTC, one peer) were known to the researchers from previous work contexts or from the wider circle of acquaintances, all other study participants had no previous relationship with the researchers.
Examples of questions in the interviews with YALTCs and peers.
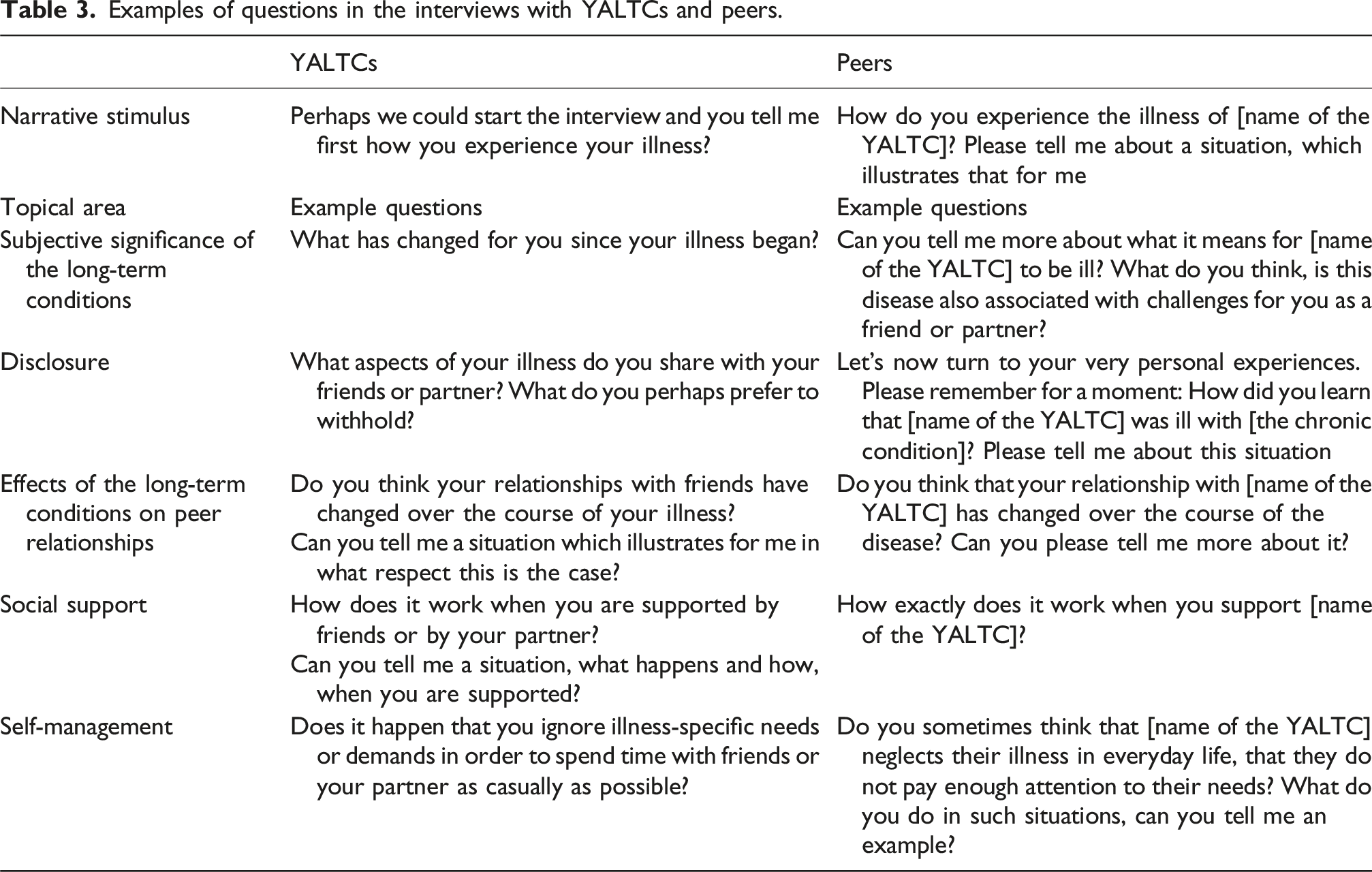
Interviews with the YALTCs and peers began with an open narrative stimulus. Then the interviews focused on areas such as subjective significance of the long-term conditions; Disclosure; Effects of the long-term conditions on peer relationships; Social support; and Self-management – especially in the context of peer relationships.
The peers we interviewed were asked questions about areas and topics that matched those we asked the YALTCs about. The questions were not general ones about long-term conditions or peer relations, but about the specific condition or relation in the case of the YALTC who had mediated the peer for the interview (see the examples in Table 3).
The interviews with the YALTCs addressed the topic of peer relations first more generally and then focused on the current partner or a specific friend for several reasons: It only became evident during the interview whether a) the YALTC had a partner or friend at all and b) whether they were ready to invite their partner or friend for being interviewed by us and c) whether the partner or friend would be willing to be interviewed 2 . The interviewed YALTCs often referred to their current partner or friend but also to their experiences with peers in general or with having no peers.
The interviews with the YALTCs lasted for 51 to 109 minutes (mean 75 minutes). The interviews with peers lasted for 23 to 85 minutes (mean 45 minutes). Since the data were collected during the Covid-19 pandemic, the interviews were not conducted face-to-face, but by using secure online methods. Online and telephone interviews represent “valid and trustworthy alternatives to traditional face-to-face interviews” in health research (Saarijärvi and Bratt, 2021: 5). They provide cost-effective access to study participants from different, even remote geographical regions of a country. In our study, which was conducted during the pandemic, distance interviews were also intended to help protect the risk group of YALTCs from additional corona infection risks that could not have been ruled out in face-to-face interview. The interviewees could choose being interviewed online (Webex) or by telephone. Most of the study participants (52 out of 60 YALTCs; 26 out of 30 peers) opted for an online interview with the camera turned on. The latter created a relatively personal interview atmosphere, although the interview was conducted at a distance. Interviewees and researchers were able to maintain eye contact.
This allowed the researchers to look for nonverbal signs of emotional distress or fatigue in the interviewees. This is necessary from a research ethics perspective to be able to avert potential harm from the participants (Pocock et al., 2021). For example, all study participants were offered a break after completing longer or emotionally stirring narrative passages.
Data analysis
All interviews were recorded and transcribed verbatim and anonymized. We allocated an identifying code to every YALTC and their partners or friends that showed them as ‘belonging’ to each other. The analysis of all interviews was MAXQDA-supported based on a grounded theory informed thematic coding (Flick 2018). First, we analyzed the interviews with YALTCs and partners or friends separately, beginning with the interviews with the YALTCs.
Analysis of interviews with the YALTCs
We initially coded the interviews on a case-by-case basis by developing preliminary framework categories oriented on the interview guide and on the theoretical frameworks of disease management and self-management from a dyadic perspective. In the main step, we first coded the interview material oriented on Charmaz’s (2014) concept of initial coding and the coding paradigm (Corbin and Strauss, 2015: 89). To this end, the text was broken down by sensitizing questions (How …? Why…? etc.) to inductively develop initial codes that were closely linked to the material. In a next step, these initial codes were bundled to sub-categories. This allowed to elaborate the initial codes and to further differentiate them oriented on Charmaz’s (2014) concept of focused coding. Then we compared the included cases in order to develop a cross-case thematic structure (see Flick, 2023). The cases were compared in minimally and maximally contrasting ways in terms of how YALTCs try to cope with their diseases in an active and problem-related way. In addition, the comparison included the extent to which YALTCs open up to their friends or partners in their disease management and self-management and try to involve them.
Guiding questions for analyzing the interviews and resulting codes and patterns.

Analysis of interviews with friends or partners of YALTCs
For analyzing the interviews with the peers (friends or partners), they were first grouped according to which of the YALTCs they were related to. From a formal point of view, a first preliminary assignment of peers to four groups based on the four main categories developed for the YALTCs (Acceptance; Tackling; Normalization; Being lost) was made. Then, we coded the interviews with the peers assigned to these groups on a case-by-case basis. Subsequently, we compared the cases within the grouping in minimally and maximally contrasting ways and between the groups. Analytic questions focused the extent to which peers differ in the perception of the YALTCs’ support needs as well as in their attempts at support and their intention (e.g. social control).
This again allowed to classify the peers’ views by assigning the interview material to four main categories (Getting involved; Giving support; Wanting to get off the ground; Overtaxing oneself – see Table 4), which in turn comprise three to four subcategories.
Data interrelations: Analysis of data on the dyadic level
On the basis of the initial separate analysis of the interviews, we finally related the statements of the YALTCs about coping with illness and self-management in a dyadic way to the statements of their friends or partners on social support. As part of this, thematically relevant statements were compared with each other and examined for contrasts, overlaps and additions. The total of eight main categories (four on the side of the YALTCs: Acceptance; Tackling; Normalization; Being lost; and four on the side of friends and partners: Getting involved; Giving support; Wanting to get off the ground; Overtaxing oneself) and their subcategories, which were worked out from the interviews with YALTCs and their friends or partners, were thus combined into four patterns of dyadic arrangements (Joint management; Supportive arrangement; Divergence; Diffusiveness). These four patterns were finally analyzed in more detail for their characteristics and meanings (see Table 4).
Coding from text to main categories for YALTCs and peers and to patterns for integrating both sides, exemplified for the pattern “diffusiveness”.
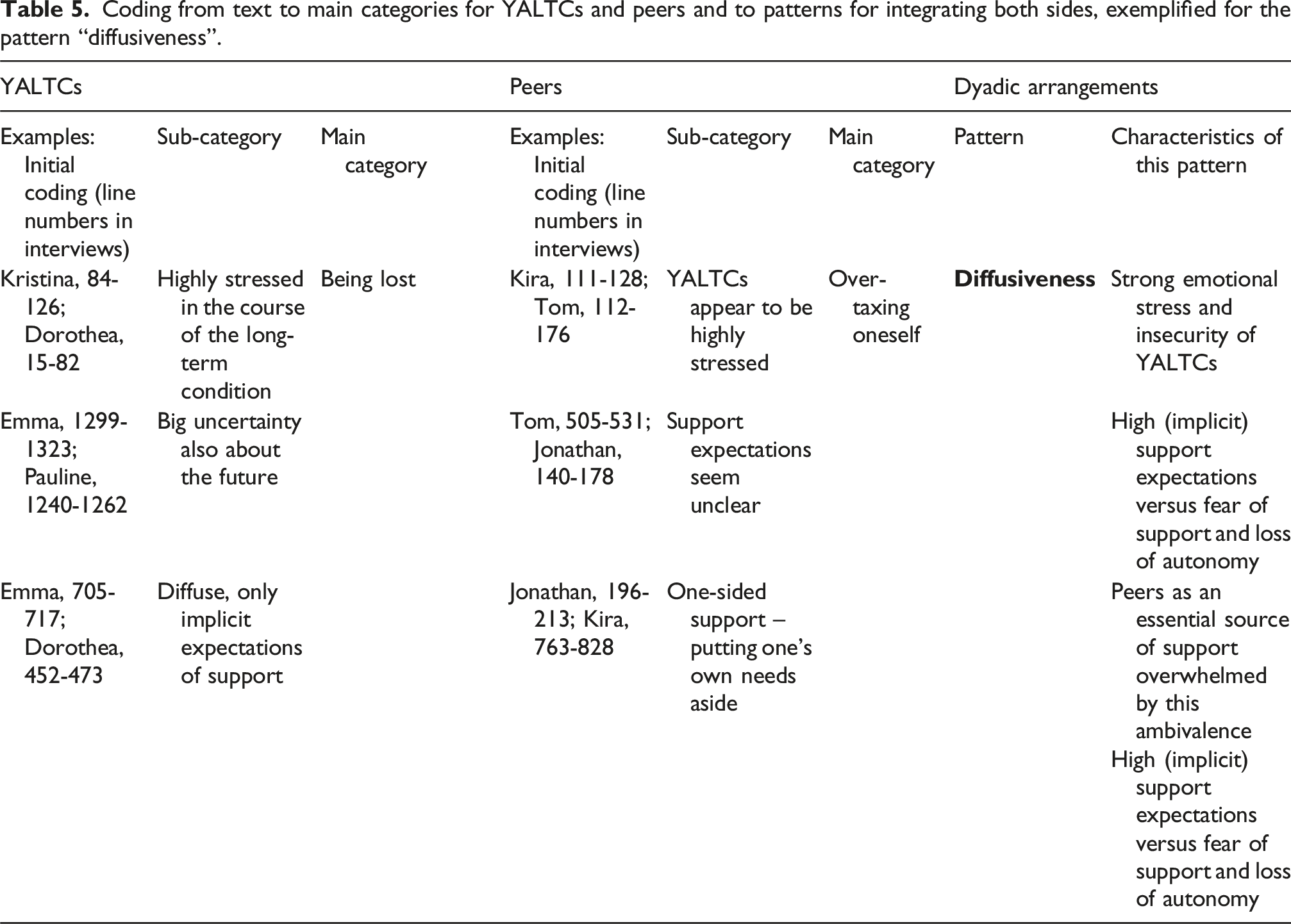
We then assigned the corresponding peers to the YALTCs whose self-management and coping behaviour had been categorized as “Being lost”. As mentioned, we have first coded the peers’ disease-related support behaviour on a case-by-case basis and then compared with that of the other peers. A comparison was made with the peers who were also assigned to the group of YALTC categorized as “Being lost” as well as with peers of YALTCs who were categorized as “Normalizing”, “Tackling”, or “Accepting” based on their coping behaviour. This comparison showed that peers of YALTCs in the group of “Being lost” perceived these YALTCs as highly stressed. These peers mentioned that it was unclear for them how they could support the YALTC they were related to and what expectations this YALTC had in terms of support. In addition, these peers described one-sided, non-reciprocal attempts of supporting the YALTC in the context of which they had set their own needs aside. In this context, the peers highlighted their own feelings of being stressed and tendencies of refusing to support the YALTC. Their support behaviour was categorized as “Overtaxing oneself.”
In a final step, we linked the views of the YALTC, who were categorized as “Being lost” by coping and self-management, to the views of the peers, whose support behaviour was categorized as “Overtaxing oneself”. As a result of such a comparison of overlaps and additions, the pattern “Diffusiveness” was worked out, characterized by: Strong emotional stress and insecurity of YALTCs; High (implicit) support expectations versus fear of support and loss of autonomy; Peers as an essential source of support overwhelmed by this ambivalence; Peers wear themselves out, ultimately withdraw from support activities.
Credibility
We used Lincoln and Guba’s (1985) criteria for establishing credibility such as triangulating the perspectives of the YALTCs with those of their partners or friends. 3 Including many different voices (in the form of quotes) also contributed to trustworthiness by allowing the reader to create their own impression of the congruence between the (researchers’) interpretation and the original quotes. Purposive sampling (Patton, 2015) contributed to generalisability by comparing several long-term conditions. Recruiting participants with different conditions expanded the data by bringing in a wider range of illness-related experiences (Lincoln and Guba, 1985). 4
As a cancer survivor, the researcher responsible for the data collection and analysis had her own experience with life with long-term conditions. A possible over-identification with study participants with long-term conditions and a ‘blindness’ to their views was counteracted by the fact that the principal investigator, who was also involved in analyzing the data, was an outsider with regard to the research subject. For reflecting role conflicts or the researchers’ sensitivities, the exchange with other scientists who were not involved in the research in the sense of a peer debriefings (Lincoln and Guba, 1985) was established as part of the research process.
The study is reported in line with the Standards for Reporting Qualitative Research (O’Brien et al., 2014 – see Appendix 2 in the Supplemental Material).
Results: Patterns of dyadic arrangements of coping
From analyzing how the YALTCs and their partners or friends tried to come to terms with the challenges of long-term conditions and what such an arrangement meant for their relationship we could identify four patterns of dyadic arrangements. They show differing degrees of congruence and interplay in dealing with the condition to conflicts and tensions.
In the presentation of the results, we will start with the two more cooperative patterns in which congruence and interplay worked better and end with the more confrontative patterns, in which that was less developed.
Joint management
Joint management – Characteristics of the cases.

aPaula could not be interviewed because she had already died (see above).
These YALTCs reported that they took their condition seriously as something that seemed to belong to them. It was important to them to take disease-specific needs into account, even if this meant being ‘smiled at’ by friends or partners. As Emilia described, for example, she distanced herself from friends who, from her point of view, had little understanding of the long-term condition and did not recognize disease-related demands. Because I have to be super correct often to keep my values in a good range. And there are one or the other who say 'Why do you have to do this so precisely here? It works. You've got an insulin pump.' These are always exactly the people who have little idea about it and also quite little empathy (YALTC Emilia, 23, Diabetes type 1, 2009)
5
.
Emilia and other YALTCs received emotional support – including in situations in which they were doubted in their handling of the long-term condition – by close friends or from their partner. (…) my partner in particular knows when he can help me and when I want him to help me above all (YALTC Emilia, 23, Diabetes type 1, 2009).
These friends or partners described that they had dealt with what it meant to have a long-term condition for the sake of their partner YALTC experiencing the condition. They had familiarized themselves with everyday disease management and knew how to support them in it. The disease thus became a shared experience. In this context, Tino emphasized that he did not doubt the competence of his partner YALTC Emilia to deal adequately with her diabetes, but that he saw the disease as something that affected Emilia and himself together. (…) in everyday life, when we go somewhere (...) I find the things for her to change the catheter or sensor (...) she can do it all herself (...) where she gets support, so to speak, in that she simply has to do less herself and as a team the whole thing more efficiently (Tino, 28 / partner of Emilia, Diabetes type 1).
YALTCs like Emilia considered it important to deal openly with the long-term condition and actively involved friends or partners in its management. At the same time, YALTCs with diabetes type 1 in particular made it clear that they wanted to be recognized by partners in their skills to deal with the condition appropriately. They set limits to attempts at support if they believed that friends or partners wanted to lecture them.
When these YALTCs described how their friends or partners stuck by them despite the long-term condition – when they paid attention or supported them in diabetes management – such experiences nevertheless helped them not to let the long-term condition get them down. YALTCs with cancer in particular noticed that they set goals for the time when stressful therapies had been completed and they felt better again. In addition, they emphasized that although they were seriously ill, the disease process had also contributed to subjectively important insights. YALTC Cornelius, for example, emphasized that he had learned to enjoy the little things in life and that he now valued and respected his peers more than before the onset of the disease. (…) noticing the physical limits (...) would be a positive example that you can trust friends to do more than you might have thought at the beginning. Or that small moments have a greater significance than before the start of therapy (...) negative examples are then of course (...) fears (...) that the chemotherapy will not work (YALTC Cornelius, 22, Burkitt's Lymphoma, 2022).
Similar to Cornelius, Philipp (YALTC) described profound experiences in the disease process that had changed his self-view. He pointed out that having to endure physically and mentally very strenuous therapies had allowed him to face many everyday stresses and challenges more calmly and relativize their importance. The growing serenity described by Philipp is also supported by the knowledge that his partner strengthened his back in dealing with his illness and listened to him when he wanted to talk about illness-related stress. (…) what is a job interview compared to chemotherapy or a life-threatening illness or surgery. The horror of many things has now subsided, because the bar is simply much higher (…) my partner, she has an endless ear luckily enough (...) that's why I'm not completely on my own (YALTC Philipp, 27, Metastatic testicular tumor, 2020).
If interviewees like YALTCs Cornelius or Philipp, who experienced serious conditions or whose condition was already advanced, nevertheless seemed composed in their situation and, for example, emphasized that they wanted to continue their studies as soon as possible, this earned them the respect of their friends or partners. As the friends or partners pointed out, it was easier for them to support these YALTCs, if they faced their condition and were willing to endure very stressful therapies.
Friends or partners emphasized in this context that they made it clear to YALTCs that they could rely on them almost unconditionally in the disease process. At the same time, they saw themselves strengthened in their confidence by the perseverance of friends or partners that the fight against the disease was ‘worthwhile’. Johannes, for example, described how the ‘positive’ attitude of his friend Cornelius became a source of strength for himself. And what was very important for me was this point, to see, hey, hey, he's doing the way now and he's going the way now and is taking one step after the other (...) huge balls, that's exactly how I told him how he deals with the matter. And he is also helping me to deal with the situation more easily, because I finally have this feeling that everything will be okay again (Johannes, 35 / friend of Cornelius, Burkitt-Lymphoma).
Friends such as Johannes and partners such as Tino mentioned above or Leonie noticed that they themselves had changed in their priorities and values as a result of the condition of the YALTC they were related to. In their view, health and healthy nutrition in particular had become more important. They also emphasized that the relationship with the YALTC had grown due to the condition. They illustrated how proud they were when the relationship did not break down because of the disease, but was confirmed in its value. Leonie, the partner of the aforementioned Philipp, saw the maintenance of the still young partnership under the conditions of a life-threatening illness as a ‘shared effort’ and as a strength that positively distinguished her from couples of the same age. Leonie also described her confidence, which had grown in the course of the (joint) arrangement, that she would be able to ‘solve’ future burdens together with her partner. (…) who can say that he has gone through something like this at such a young age in such a fresh relationship (...) what could there be that you can't do together if you go through something like that together? (Leonie, 24 / partner of Philipp, Metastatic testicular tumor).
In exceptional cases, joint management could only be reconstructed retrospectively in our study: For example, Sonja, friend of Paula who died of Glioblastoma at the age of 27, reflected in an interview on the hope with which Paula tried to defeat her disease and how she, Sonja, was always filled with this hope – even against her better judgment. The fight against cancer thus became a common task, which for Sonja also consisted of establishing normality as far as possible. Sonja emphasized how she stuck to previous self-evident things in dealing with Paula, at least in the early phase of the disease, and tried to bring her own preferences into their everyday life together in order not to let the focus on the incurable disease become overpowering. I have never treated her as if she is about to die or as if she were seriously ill (...) for example, she always wanted us all to sing karaoke (...) I said “no, no, no, you can forget about that now. I didn't do it before I won't do it now. Same rules.” (…) the affected person fights (...) we fight together (Sonja, 33 / friend of Paula, Glioblastoma).
In the late and terminal phase of the disease, the arrangement changed: Sonja took on nursing tasks in order to compensate as much as possible for the functional losses that Paula suffered.
In summary, it became clear that these YALTCs as well as their peers saw themselves affected by the long-term condition and tried to work together as a ‘team’ in dealing with it. Optimism and hope seemed to be central to coping behavior. The accounts of these YALTCs and peers also showed that their relationship intensified in the course of the joint coping process.
Supportive arrangement
Supportive arrangement – Characteristics of the cases.

These YALTCs pointed out that they have dealt intensively with their long-term conditions and knew what is good for them. They assumed that friends or partners had little experience with (serious) long-term conditions. Therefore, these YALTCs hardly involved their friends or partners, especially in treatment decisions. At the same time, interviewees such as YALTCs Friederike, Elias or Alexander described that they talked to friends or partners about their long-term conditions and felt that they were being taken seriously. As Friederike mentioned, the experience of her friend being there for her when she needed her has contributed to her greater openness towards this friend. This in turn intensified their friendship. In any case, I have a different relationship with the friends who have gone through this [her cancer – the authors] with me (...) because you deal much more openly with fears and worries and that has remained, at least with one of my best friends. With her, it has really, I would say, become even tighter. You [addressing the interviewer – the authors] will also get to know her. That's the one who got in touch [for being interviewed – the authors] (YALTC Friederike, 24, Ovarian cancer, 2017).
Friends or partners of these YALTCs pointed out, that they neither doubted the severity of the long-term conditions nor the YALTCs’ ability to deal with these competently. From their points of view, the friends or partners provided support above all by signaling to those experiencing the long-term conditions that they were there for them: They kept them company and offered distraction. Friends or partners also described how important it was for them to consider whether their support really met the needs of those who were experiencing the long-term conditions. Inka, for example, wanted to avoid forcing her support on her friend, YALTC Friederike, at all costs so as not to burden her additionally. (…) if I then noticed (...) she doesn't feel like talking about it much now, I didn't get in touch for a few days (...) I didn't want to annoy her if she was already feeling bad anyway (...) but still to show, 'I'm here, if you want to talk about it, you can definitely do that' (...) (Inka, 23 / friend of Friederike, Ovarian cancer).
Inka and other friends or partners such as Friedrich or David described understanding for the fact that they were usually not the first person of contact for illness-related stress. In most cases, they saw themselves as outsiders compared to relatives. From their point of view, it would be presumptuous and would jeopardize the close relationship if they wanted to compete with the importance of relatives in the course of illness. Similar to Inka, David also emphasized that he always had an open ear for Friederike and tried to behave as empathetically as possible towards her. This could also mean reverently restraining oneself in certain situations. (…) in the context of the family (...) because I am a very outside person. She thinks it's good that I'm involved, but I don't think she would like me to really speak up (David, 26 / partner of Friederike, Ovarian cancer).
In summary, we see that these YALTCs tried to manage their long-term condition as their own responsibilities and saw friends or partners as a ‘safe haven’ where they could expect support and emotional support. These YALTCs and friends or partners seemed to agree on this division of roles. When friends or partners in addition carefully considered how to support those who experience the condition in a way that met their needs, they signaled empathy and thus contributed to strengthening the relationship.
The patterns of dyadic arrangements described so far show different forms of cooperation between YALTCs and friends and partners in dealing with the disease. In contrast, the following two patterns point to conflicts and tensions – when friends or partners tended to overprotect the YALTCs or, conversely, did not seem to perceive the YALTCs’ needs, or YALTCs and friends or partners tended to overwhelm each other and lost themselves in diffusiveness.
Divergence
Divergence – Characteristics of the cases.
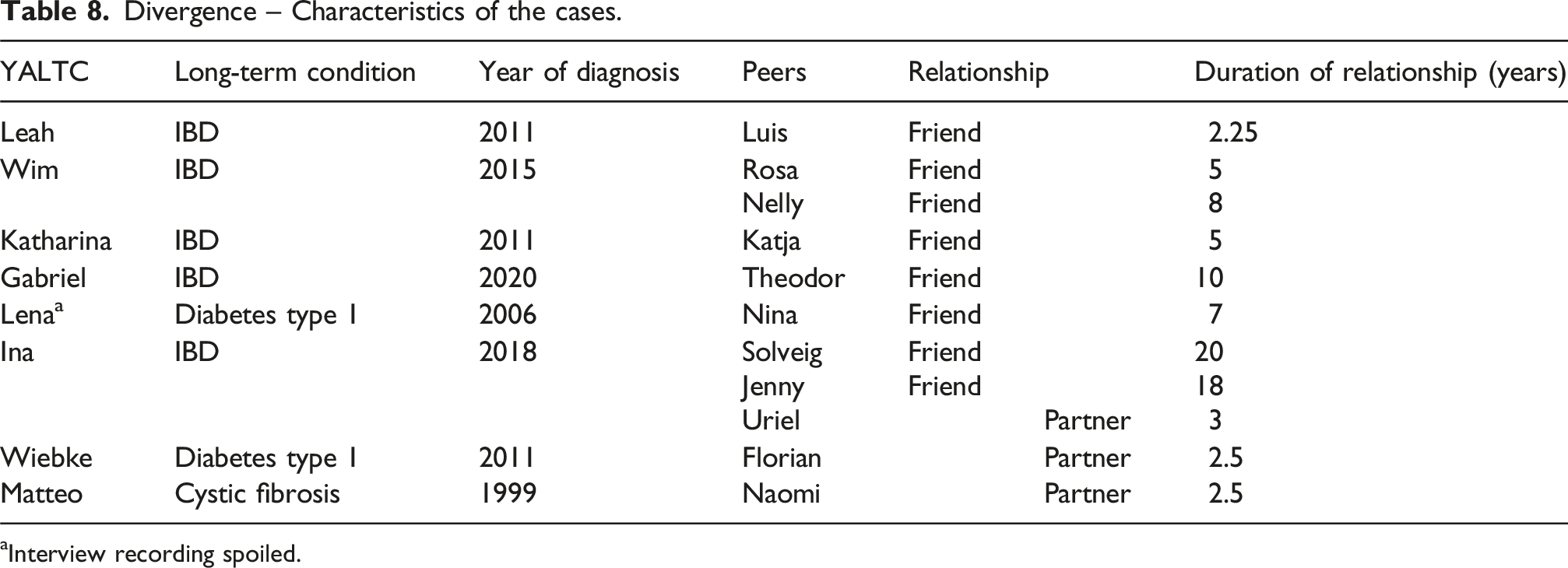
aInterview recording spoiled.
These YALTCs tried to ignore their physical vulnerability, even at the price of worsening symptoms. In order not to be perceived as different, these YALTCs disregarded needs related to the condition, especially when they were with partners or friends. YALTC Leah emphasized that, in her view, it would violate social conventions if she insisted on certain diets during a meal in a relaxed atmosphere. (…) If you go somewhere and then constantly reject something, it often comes across as rude. Especially when people don't know me so well, I always say YES and eat that or drink that so as not to seem rude (YALTC Leah, 29, IBD, 2011).
Contrary to what these YALTCs (implicitly) assumed, their partners or friends had little understanding when the YALTCs did not pay attention to their own disease-specific needs. Friends or partners rather thought that the YALTCs had themselves to blame if the course of the long-term condition came to a head because therapeutic recommendations had not been taken into account. It is clear from these friends’ or partners‘ accounts that they underestimated the challenge of implementing often complex treatment regimens in everyday life. Luis, on the other hand, did not seem to suspect that there were good reasons for Leah, with whom he is loosely friends, to pay little attention to disease-specific needs. (…) then I always show her [Leah – the authors] what I cook (...) whether she can tolerate it. And then she always says, yes, she's eating everything again. She doesn't pay attention to it anymore. And I sometimes find that a bit negligent. But in the end, I accept it (Luis, 34 / friend of Leah, IBD).
If the long-term condition were to worsen, from Luis’ perspective, it would be Leah’s individual problem. According to their accounts, both Leah and Luis avoided talking to each other about the long-term condition or ways of dealing with it and sharing their own worries and fears. However, in our interviews we also found that peers openly expressed their concerns about how the YALTCs they were related to dealt with their long-term condition. This was usually the case when the relationship between YALTCs and peers was closer – as in the case of YALTC Ina. She described how important it was to her to spend the day like her peers. So that she did not become a burden to them and do not attract attention in social situations, Ina rarely talked about her long-term condition and suppressed her symptoms. She tried to avoid attending the doctor as much as possible. Similar to other YALTCs, for example Wim, Wiebke or Katharina, Ina emphasized that she wanted to forget the disease as much as possible in her everyday life. In this context, however, Ina also described that she had to deal with close friends who tried to encourage her to deal with the disease differently. Sometimes I just don't want to be sick and don't feel like dealing with it. And then I put off the next colonoscopy very much in front of me (...) then says for example Solveig [a friend – the authors] “Yes, if you didn't call tomorrow, I'll call there.” And that's something I sometimes regret that they know so much (YALTC Ina, 25, IBD, 2018).
As the example of Ina illustrates, attempts by these YALTCs to ignore their illness were perceived as risky by friends or partners – especially if they had their biographical references to long-term conditions, e.g. because members of their family are ill. These friends or partners therefore suspected the complications that long-term conditions can be associated with. They wanted to protect the YALTCs they were related to from this at all costs. In the case of Ina in particular, it became clear how differently peers can react to the disease behavior perceived as risky: Solveig, for example, who had been friends with YALTC Ina since childhood, wanted to persuade her to take her illness more seriously. However, she suspected that she was restricting Ina’s autonomy too much if she gave her clear recommendations on how to deal with the disease. Solveig feared that her tendency to overprotectiveness could have a negative impact on their relationship, but did not know how to resolve the conflict of ‘protection from harm vs. granting autonomy'. It's sometimes a tightrope walk when you put it so metaphorically (...). 'May I go so far (...) is that my position at all? Am I allowed to patronize them? Actually, no. Am I allowed to do that in this situation? Yes, but (...) that's no longer my role as a friend (...) I just know a little more from a purely medical point of view (Solveig, 26 / friend of Ina, IBD).
Jenny, who had also known Ina since childhood, assumed, like Solveig, that Ina’s illness was more severe than she wanted to admit. Unlike Solveig, however, Jenny tried to meet Ina less with professional competence and more with a lot of understanding. Jenny hoped to trigger a greater sensitivity to Ina’s own needs on the basis of care and affection. I am then very understanding and also know that she already perceives it, but simply tries - yes, not to let the disease determine her everyday life too much (...) but I'll tell her that she has to take care of herself in any case (Jenny, 25 / friend of Ina, IBD).
In contrast to Ina’s friends, Uriel, her partner, was reluctant to give advice on how to deal with the disease. Uriel also noticed that Ina did not take her condition seriously enough. Unlike Solveig and Jenny, who both studied medicine and aimed to control symptoms with their partially overprotective behavior, Uriel saw more of the need for Ina to have to live with the condition in everyday life - and to do so as well as possible. For Uriel, this meant that taking into account disease-specific needs should not always come first, as this would mean depriving oneself of the joy of life. Uriel assumed that Ina is competent enough to decide for herself when she should prioritize her illness and when her social needs. The catch with the story is: If you give one hundred percent to prevent everything, you partly forget to live and have a good time, because then you forbid yourself this, that, and what and forget the pleasure of life (...) that's why I think that Ina (...) has found a very good line (...) (Uriel, 28 / partner of Ina, IBD).
In summary, we found that these YALTCs and their friends or partners differed in their assessment of how severe the long-term condition was and how it should be treated. For their part, the peers differed in how they reported such divergences to the YALTCs they were related to and in this context (implicitly) tried to maintain a good relationship with the YALTCs: While some friends or partners blamed the ones with the long-term condition for a possible escalation of its course, for other friends or partners it was important to treat the person with the long-term condition with appreciation. However, in these cases, the friends or partners did not see themselves personally affected by the long-term conditions of the YALTCs.
Diffusiveness
Diffusiveness – Characteristics of the cases.

These YALTCs described themselves as highly stressed because their disease was very restrictive in everyday life and unpredictable in its course and consequences. Planning their everyday lives or even a personal future therefore seemed hardly possible. YALTC Pauline, for example, showed that she felt so exhausted in the face of side effects of her cancer therapy and so insecure due to the disease itself that it was difficult for her to continue her studies and to prepare for the start of her professional life. (…) a permanent burden, this chronic pain, and I keep asking myself how I can function in work life (...) I think I will find a job. But (...) whether I can keep it (...) now with this chronic pain, that's a much, much higher requirement (YALTC Pauline, 30, Lymph gland cancer, 2015).
When Pauline and the other YALTCs allocated to this pattern described feelings of being lost, such sensitivities also structured their social relationships: Partners or friends found that the YALTCs they were related to had changed very much and no longer seemed to be like who they once were. These peers also assumed that the balanced give and take that once determined their relationships was shifting to the point that they themselves were only the ones who provided support. For Pauline’s friend Kira, for example, this was challenging because she assumed that she could help Pauline only to a limited extent. Pauline’s condition-related irritations seemed to become a constant topic that permeated all communication and increasingly strained the relationship. (…) that I try to get her to keep trying things and not give up right after the first semester. But on the other hand, of course, I know that she is not as resilient as I might be (...) I often find that difficult to empathize with (...) the conversations are rarely relaxed now (...) it's just mostly about pretty existential topics (Kira, 29 / friend of Pauline, Lymph gland cancer).
YALTCs like Pauline also described the challenge of negotiating dependency and independence in relationships with peers. These interviewees reported that they refused to be taken care for by friends or partners. At the same time, they mentioned that it became increasingly difficult for them to hold on to everyday habits and liabilities and, for example, to run the household. Thus, they saw themselves as depending on their partners’ or friends’ support, empathy, and consideration. However, these YALTCs avoided disclosing their expectations of support and as a result experienced that friends or partners were not as supportive as desired. YALTC Dorothea, for example, described how everyday life with her (former) partner was determined by constant conflicts, which, in addition to her illness, contributed to profoundly reducing her well-being. At the same time, Dorothea emphasized how disappointing it was for her not to be able to rely on the support of friends. (…) lived with my ex-partner, therefore also many arguments, many obligations (...) that's where it started with my anxiety disorders (...) when I had really bad stomach cramps, and then we had a big conflict, because she [a friend of hers – the authors] didn't know how to react at all. And that's when we noticed that we had never talked about it before (...) I thought she might be informing herself (YALTC Dorothea, 25, IBD, 2021).
Unspoken expectations, as in the quote from Dorothea’s interview, had a deterrent effect on the partners or friends. In some cases, they were unclear from the outset how they could support the YALTCs they were related to. Otherwise, partners or friends noted that they felt exploited and overwhelmed when the YALTCs did not clearly communicate what support they expected from them and how they should deal with disease-specific stresses. These peers were also unsettled by the YALTCs‘ ambivalent requests for support. They also described that they experienced them as increasingly overwhelmed in dealing with the disease, so that they felt morally obliged to provide support. In order to provide support when everyday life – together – became increasingly determined by the imponderables of the disease, these peers put their own needs and interests aside. They believed that they should not complain about this. While the partners or friends were actively involved in the organization of everyday life and took on care work, they also complained about a lack of recognition or even a rejection of their efforts. Jonathan, Dorothea’s (aforementioned former) partner, emphasized that such experiences contributed to an increasing distance from Dorothea and ultimately to the dissolution of the relationship. (…) that I'm doing care work somehow. But the fact that I try to relieve her (...) that was then again (...) often wrong in Dorothea's eyes, because she didn't ask for it (...), what was a very big challenge for me personally and also led to us parting ways again, was this self-abandonment on my part (Jonathan, 30 / former partner of Dorothea, IBD).
In summary, YALTCs and partners or friends allocated to this pattern described how the long-term condition dominated everyday life and assigned them roles that they did not feel up to. However, the relations here were characterized by unclear expectations and uncertainties in both directions. While these YALTCs seemed to be unclear about what they expected in terms of support, their friends or partners were unsure about what support they were willing to give and what their limits were. This led to mutual disappointment and recrimination. Relationships broke up or threatened to break up because of this diffusiveness.
Discussion
The aim of this qualitative study was to investigate dyadic views of YALTCs and their peers (friends or partners) on disease management and self-management in detail. Four patterns of dyadic arrangements could be identified. These patterns reveal shared and divergent social representations of dyadic arrangements of coping. Like in the results of comparable studies (Manceau et al., 2023; Werner et al., 2021), these patterns differ with regard to whether the dyadic arrangement between YALTCs and peers is characterized by support and cooperation or by confrontation and pressure. First, we will again discuss the two patterns that are oriented towards cooperation and relate them to the current literature.
Cooperative patterns of dyadic arrangements
For N = 7 of the dyads in our study we found that YALTCs and friends or partners were trying together to cope with the disease and manage disease-related needs. We were able to identify such joint management, in which YALTCs as well as friends or partners saw themselves as affected by the disease, especially in the case of cancer. It has been shown repeatedly in the literature that cancer, as a “we disease” (Acquati and Kayser, 2019; Opsomer et al., 2019), affected patients and their (family) support system, forcing them to rethink their previous lives. However, while existing studies referred to long-term married couples in middle and older adulthood, the interviewees in our study were in young adulthood. At this stage of life, young adults often have yet to figure out which path in life is right for them, leading to frequent upheavals in their personal life situation and instabilities in social relationships (Arnett, 2024; Barry et al., 2016). Nevertheless, the results of our study show that the interviewed YALTCs and friends or partners were able to face challenges such as serious long-term conditions together.
In our study, joint management was described also by YALTCs with diabetes type 1 and their peers. That means, we observed this form of coping not only in a disease such as cancer, which is understood as a thoroughly relational experience (Boer et al., 2019) that requires the people experiencing the condition and their relatives to make a variety of changes in everyday life (Tranberg et al., 2021), but also – in the case of diabetes type 1 – in a disease with which the YALTCs have grown up. In contrast, the literature emphasizes that people with type 1 diabetes often view their disease as an individual problem that they have learned to manage on their own (Berg et al., 2020).
Among our interviewees, joint management could be identified primarily among YALTCs who lived with partners without being married. However, this form of coping could also be found in friendships, as long as the relationship was described as very close. In other studies, older couples’ common dyadic coping feeds on the fact that many burdens have already been endured together (cf. Carberry et al., 2024; Manceau et al., 2023). In comparison, our interviewees (YALTCs and their partners or friends) illustrated the optimism for the future that the stresses overcome during the course of the disease will continue to contribute to ‘successful’ stress management.
Our results underline the importance of friends as support figures in the process of coping with illness in young adulthood. We found this for joint management, but even more so for the pattern supportive arrangement we identified in N = 7 dyads with its clear division of labor between YALTCs who manage their long-term condition independently and peers – especially friends – who provide support. While friends in the supportive arrangement had an open ear for the YALTCs and offer distraction, in the context of joint management they were more involved in coping with the condition, e.g. by taking on nursing tasks or visiting the YALTCs regularly in the hospital. The importance of close friends that emerged in our study partially contrasts with the results of existing studies, which show that friends of YALTCs in particular turn away from the disease process, especially in the case of threatening conditions such as cancer (Hauken and Larsen, 2019; Lidington et al., 2021).
In dyads with joint management and also in dyads with supportive arrangements we found a comparatively high proportion young women with a long-term condition and male partners or friends. This is in contrast to study results, according to which women with long-term conditions are more likely than men to shy away from coping together, e.g. because they do not want to be a burden on their partner (Helgeson et al., 2022).
Existing studies show that male spouses are less willing than female spouses to support their partner (cf. Berg and Upchurch, 2007). In addition, men illustrate pragmatism in their support, block emotions and focus on factual, action-oriented or financial help (Calasanti and King, 2007; Ruark et al., 2024). In our study, young men not only provided support by taking on smaller tasks in diabetes management. Based on a high level of attachment to friends or partners, they also did “women’s work” (Russell, 2007) by providing emotional affection and being there – which is considered a key element of supportive relationships in adolescence (Woodgate, 2006; cf. Camara et al., 2017).
Carter and colleagues’ (2023) study on young adults with chronic pain and their partners with a dyadic perspective has shown, that supportive relationships were characterized by reciprocity, partnership, and mutual sensitivity (Carter et al., 2023). Such reciprocity is also characteristic of the “joint management” and “supportive arrangement” patterns identified in our study.
Confrontative patterns of dyadic arrangements
The two patterns just discussed are determined by differently contoured cooperation between YALTCs and peers. The other two patterns we identified – “divergence” (N = 8 dyads) and even more so “diffusiveness” (N = 4 dyads) – are characterized by pressure and ambivalence – and thus by confrontation. Both patterns have a confusion of roles in common, as has been similarly demonstrated in other studies as typical of tense dyadic coping (cf. Werner et al., 2021): In terms of divergence, it can be seen that peers tended to conceive the disease not as their problem, but as that of YALTCs (on shared problem perceptions in long-term conditions: cf. Helgeson et al., 2018). Based on an assessment of the severity of the disease that differed from the views of YALTCs, peers also tended to overprotect friends or partners or to control them socially out of a motive of concern (on different motives for overprotective, socially controlling behavior, cf. Gerwitz et al., 2023).
In our study, attempts to persuade the patients to adopt a supposedly more adequate disease behavior tended to be described by friends or partners of YALTCs who suffered from IBD. Unlike type 1 diabetes, for example, where monitoring and (blood sugar) self-monitoring are important for successful therapy (Lee et al., 2019), IBD is a disease in which self-management is at least partially characterized by learning from trial and error and by listening to one’s own body when dealing with the disease (DuBois et al., 2024; Peters and Brown, 2022). Against this background, overprotective or socially controlling attempts by peers to cope threatened to come to nothing. Among peers who tended to adopt such coping strategies, the proportion of young women was disproportionately high in our study.
In an arrangement characterized by diffusiveness, peers here described an increasing burden as caregivers – similar to what is also found for family caregivers (cf. Jeyathevan et al., 2019; Tranberg et al., 2021). A diffuse arrangement, in which the patients presented themselves as emotionally highly stressed and exhausted, could only be identified in our study among female respondents, comparable to the results of other studies that women with long-term-conditions reported greater distress than men (Rassoulian et al., 2021).
We found the pattern “diffusiveness” – like the pattern “joint management” – more in dyads with cancer. While in the first case the serious condition seemed to lead to mutual overload, which ultimately endangers the relationship between YALTCs and peers, the disease became a test for dyads with joint management that strengthened the relationship.
The patterns identified in this study in the light of dyadic coping models
Relating the patterns of dyadic arrangement we have identified to the four facets of dyadic coping according to the Systemic Transactional Model (Bodenmann et al., 2016; cf. Weitkamp et al., 2021) revealed points of contact and overlaps, but also contrasting findings:
The pattern of “joint management” elaborated in our study is comparable to common dyadic coping (Bodenmann et al., 2016), in which both the patient and his partner see themselves affected by the disease and try to cope with it through coordinated strategies.
Similar to the supportive dyadic coping of the Systemic Transactional Model, the “supportive arrangement” we identified means that there was the primarily affected person, in our case the YALTCs, supported by another – unaffected – person from their environment in dealing with the disease. In our study, more friends than partners were support persons.
Two of the patterns we identified (“divergence” and “diffusiveness”), are characterized by the fact that there was hardly any cooperation or interaction between YALTCs and their friends or partners in dealing with the disease. It is also typical for these two patterns of dyadic arrangements that friends or, more rarely, partners tried to socially control YALTCs in order to encourage them to supposedly ‘more appropriate’ self-management (“divergence”) or that friends or partners were overwhelmed in their attempts to support (“diffusiveness”).
This can be linked to the negative dyadic coping described by Bodenmann et al. (2016, p. 3; see also Weitkamp et al., 2021) and characterized by the partners behaving in a hostile manner – which, however, could not be found for our interviewees. Such negative coping also means that partners support only superficially and without empathy and are unwilling and unmotivated in their supportive behavior.
Delegated dyadic coping in the sense of Bodenmann and colleagues (2016), in which partners try to relieve the burden by taking on tasks and obligations that would normally be taken on by the patient, could not be identified as a separate pattern in our study. One possible explanation for this could be that the YALTCs we interviewed were only temporarily severely impaired – e.g., in the course of stressful (chemo-) therapies or as a result of major surgery for IBD. In such cases, YALTCs mentioned that they usually received support from their parents, not from friends (or partners).
Conclusions
The four patterns of dyadic arrangements we found in our interviews can be related to contextual factors (type of long-term condition, type of relationship) and sociocultural factors (gender).
The pattern of “joint management” we found more in cases of YALTCs with cancer or diabetes type 1 and more often in partnerships than in friendships. Coping behavior, when patients and their partners are jointly affected by disease-related stress and consider self-management to be teamwork has been described repeatedly in the available literature about people with cancer (Bertschi et al., 2021; Fergus et al., 2022; Opsomer et al., 2019; see). For our sample we also saw that young women were more likely to be among the YALTCs and young men more likely to be among the peers. This is in contrast to the results of existing studies, according to which women are more likely to want to avoid coping together with their partner (Helgeson et al., 2022).
The pattern of “supportive arrangement” is more evident in friendships than in partnerships in our findings. According to our literature research, dyadic coping in friendships has not yet been a topic in relevant studies. Future research should address this and systematically investigate how dyadic coping of YALTCs differs depending on the form of relationship, e.g. to derive different intervention strategies for a stronger bond between the dyads.
For the pattern of “divergence” we found that among the YALTCs in our sample were mainly those with IBD and that the proportion of women among the peers as support persons was relatively high. That mainly women try to control their partners’ health has been shown in other health care studies as well (August et al., 2021; Dimova et al., 2021).
For the pattern of “diffusiveness”, we found a comparatively high proportion of young women with cancer. All YALTCs we assigned to this pattern “diffusiveness” and who described a high level of emotional stress and insecurity in view of their condition are female. Other studies have also shown that women with long-term conditions experience greater distress than men (Rassoulian et al., 2021).
Strengths and limitations
Our study shows the range of dyadic arrangements of YALTCs and their friends and partners in dealing with long-term conditions and thus focuses on age and target groups that have so far been neglected in the context of research on dyadic management of long-term conditions (Berg et al., 2020; Ferraris et al., 2022). This is a strength of our study which at the same time is not free of limitations: As mentioned earlier, the reported findings are part of a broader study of peer relationships in long-term conditions. For the results presented here, the research on dyadic coping forms an analytical point of reference, but it is not the guiding point for our entire study, as we did not conduct dyadic, but separate interviews with YALTCs and peers.
Individual interviews offer the advantage that individuals can freely express themselves on sensitive topics such as long-term conditions without fear of damaging close caregivers by revealing certain information in the interview (Taylor et al., 2021). At the same time, however, individual interviews limit researchers’ ability to record and analyze interactions and co-constructions of members of a dyad. For example, we cannot make statements about how YALTCs reacted to overprotectiveness of peers (cf. Rapelli et al., 2021) because they have not commented on this point in their narratives.
As in other qualitative (Farre et al., 2019) and quantitative (Rabin, 2019) studies, young women are in the clear majority in our sample. We can therefore only show tendencies in how gender influences the patterns of dyadic arrangements we identified.
Another limitation arises from the cross-sectional design of our study: Future studies should be longitudinal in order to map dyadic arrangements in the course of long-term conditions and, for example, to compare arrangements in stable or early phases of the disease with those in the late stages. In addition, a longitudinal design could more adequately capture the effects of relationship breakdowns, which are not uncommon in young adulthood, in terms of their effects on self-management and coping. As a limitation, there were only heterosexual couples among the YALTCs and peers in the partnerships in our sample.
Practical implications
Nevertheless, the results of our study also have practical implications: They illustrate the importance that friends or partners can have for the self-management and coping behavior of YALTCs. In order to take this importance into account, training courses on long-term conditions should no longer be aimed only at YALTCs, their parents and siblings, as is customary at least in Germany (cf. Warschburger and Wiedebusch, 2021). If YALTCs have a fundamental interest in the involvement of peers in their own coping they should be encouraged by people working in the health care system to invite selected friends or partners to such training. Once peers have developed a better understanding of long-term conditions and disease-specific needs after such training, this can help YALTCs to accept their disease and apply self-management measures even in the presence of peers (Tuohy et al., 2019).
For their part, health professionals should be aware of how important good friends or partners can be as close caregivers for YALTCs. The results of our study show that such close relationships can also become fragile in young adulthood due to the burden of the disease. To counteract this as much as possible, health professionals working with YALTCs should approach them about their peer relationships and inform them about services offered by the care system, which are aimed at young family caregivers and are intended to relieve them, for example.
Supplemental Material
Supplemental Material - “It’s sometimes a tightrope walk…” – Exploring dyadic coping arrangements between young adults with chronic conditions and their peers (friends or partners) in interviewing both sides
Supplemental Material for “It’s sometimes a tightrope walk…” – Exploring dyadic coping arrangements between young adults with chronic conditions and their peers (friends or partners) in interviewing both sides by Uwe Flick, Gundula Röhnsch in Health Psychology Open.
Footnotes
Acknowledgments
We thank the interviewees who shared their time and their experiences. The authors thank the German Research Foundation for the financial support of the study and the Freie Universität Berlin for funding the Open acccess publication.
Ethical considerations
The ethics committee of the Freie Universität Berlin considered the research proposal and gave its approval on 21 September 2020 (038/2020) and an extension proposal on 05 March 2024 (005/2024). The decisions were based on the ethical guidelines of the German Psychological Society.
Consent to participate
Based on comprehensive written study information, all young adults and all peers provided written consent to participate in the study.
Consent for publication
Written informed consent for publication was obtained from all study participants.
Author contributions
UF and GR conceptualized this article, reviewed the referenced studies, drafted and edited the article, and authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by the German Research Foundation. Grant no: FL 245/12-1; FL 245/12-2. Supported by Open Access Funds of Freie Universität Berlin.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in the research cannot be shared with any person: The participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the research, sharing data is not available.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.