
Abstract
This study explored the association between body mass index (BMI), weight and appetite change, the severity of depression and anxiety, and related physical symptoms in youth seeking treatment for depression and/or suicidality. Youth completed self-report surveys and were categorized by BMI into healthy weight, overweight, and obese groups. Findings demonstrated overweight and obese participants were more likely to come from low-income households. Obese youth were more likely to report recent increases in appetite compared to healthy and overweight youth and in perceived weight compared to healthy weight youth. Obese youth had worse depression severity than overweight youth and worse physical function compared to healthy and overweight youth. Appetite and perceived weight changes were generally associated with worse clinical symptoms, with appetite more consistently associated with poorer presentations. These findings suggest high BMI, particularly within the obese range, is of concern for depressed youth, potentially putting them at risk for poorer clinical characteristics.
Introduction
Youth weight gain is a rapidly developing public health crisis, with over 16% of American youth classified as overweight (body mass index [BMI] between 85th and 95th percentile), and over 19% classified as obese (BMI ≥95th percentile) (Fryar et al., 2020). According to the World Health Organization (2022), childhood and adolescent obesity rates in the U.S. are projected to reach 25% as early as 2030. Similarly, there have been alarming increases in instances of youth depression (Substance Abuse and Mental Health Services Administration, 2019) and anxiety (Benton et al., 2021), all potentially exacerbated by the COVID-19 pandemic (Eneli et al., 2022; Racine et al., 2021). While the link between extremely high body weight and deterioration of physical health has long been established in both the clinical literature (Dixon, 2010; Uzogara, 2016) and public perception (Emmett and Chandra, 2015), previous studies are limited in terms of examining different weight categories and their associations with variables related to depression or other related mental health challenges.
A substantial portion of the existing literature suggests that obese youth are more likely to struggle with symptoms of depression and anxiety than their healthy-weight counterparts (Lindberg et al., 2020; Wang et al., 2019). Galler et al. (2024) found that among overweight and obese youth diagnosed with a psychiatric condition, the proportion of severe obesity (BMI ≥97th percentile) was higher in individuals with depression (23.7%) and anxiety (17.8%) when compared to obese youth without a mental health diagnosis (13.5%). Correspondingly, a chart review of 102 adolescents in a weight management clinic showed the odds of having severe obesity versus obesity were 3.5 times higher for patients with depression and 5 times higher for patients with anxiety compared to youth with weight issues and no psychiatric diagnoses (Fox et al., 2016). Some researchers have even proposed the presence of a bidirectional relationship between weight gain and mental health symptoms (Mannan et al., 2016; Muhlig et al., 2016). However, though quite compelling, these findings are far from concrete or universal. A meta-analysis of 28 studies carried out by Moradi et al. (2022) found no association between overweight/obesity status and the risk of depression and anxiety, while a meta-analysis by Quek et al. (2017) demonstrated a positive association between youth obesity (but not overweight) and depression, and Burke and Storch (2015) argued that the relationship between weight status and anxiety in the existing literature is significant, although effect sizes were very small. Additionally, much of the literature either solely focuses on obese youth (Marmorstein et al., 2014), combines overweight and obese youth in the same category (Drosopoulou et al., 2021), or uses seemingly arbitrary cut-offs for defining weight categories (Zeiler et al., 2021) which limits the ability to draw conclusions about overweight youth and whether mental health continues to worsen as weight increases.
It is also important to consider that the relationship between depression and body weight is not static and could be impacted by fluctuations in appetite. Previous studies have shown that appetite is associated with weight gain (Blundell and King, 1996) and may be impacted by individual differences (Lowe et al., 2009), adiposity (Wardle and Carnell, 2009), and patterns of neural activation in response to seeing food (Baxter, 2016). The appetite-depression link is strong enough to remain a diagnostic criterion (American Psychiatric Association, 2013), making appetite a crucial variable to consider. Interestingly, changes in appetite and weight (in either direction) are more prevalent in depressed youth than in depressed adults (Rice et al., 2019); and while more depressed youth appear to lose the desire to eat (Maxwell and Cole, 2009), some literature shows an opposite trend (Mooreville et al., 2014). When it comes to youth anxiety, however, the role of appetite has not been explored and warrants investigation.
Two key physiological factors implicated in weight change, depression, and anxiety are fatigue and physical function. Higher fatigue is a frequently occurring characteristic of obese youth (Norris et al., 2017; Vantieghem et al., 2018) and plays a noticeable role in mental health outcomes in adolescents, including depression and anxiety (Lamers et al., 2013; Wolbeek et al., 2011). Similarly, compromised physical function is another common challenge in youth with obesity (Shultz et al., 2014; Tsiros et al., 2013) and does appear to impact the mental health of adults (Lever-van Milligen et al., 2017; Van Milligen et al., 2012), though there is a shortage of published evidence in youth. To our knowledge, there is no published literature exploring the role of fatigue and physical function in overweight and obese youth with depression and/or suicidality.
There are several limitations in the existing literature, which makes it difficult to draw reliable conclusions about the relationship between weight and mental health symptoms. The available literature varies significantly in how weight groups are categorized or avoids some groups entirely. Similarly, few studies assess critical weight-related factors like appetite, fatigue, and physical function, with little research done in depressed populations. Lastly, even well-constructed studies come to conflicting conclusions, requiring further investigation. Thus, in the present study, we examined whether overweight and obese youth vary significantly from healthy-weight youth on measures of depression, anxiety, fatigue, and physical function. Subsequently, we assessed whether being overweight or obese impacts acute appetite and weight changes. Lastly, we explored if the relationship between bodyweight categories and depression, anxiety, fatigue, and physical function levels are impacted by acute changes in weight and appetite, as well as various demographic factors.
Methods
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the University of Texas Southwestern Institutional Review Board (STU2020-0665).
Study design and sample description
The Texas Youth Depression and Suicide Research Network (TX-YDSRN) is a statewide learning healthcare network funded by the Texas State Legislature as a part of the Texas Child Mental Health Care Consortium (TCMHCC). TX-YDSRN has established a registry of children, adolescents, and young adults between the ages of 8 and 20 who screened positive for depression or suicidal ideation or who were undergoing treatment for depression at the time of enrollment.
After completing informed consent/assent, participants and their caregivers, or Legally Authorized Representative (for those under 18), completed a battery of clinician-administered assessments and self-reported questionnaires. A comprehensive description of the network design, as well as the sample characteristics of the first 1000 participants enrolled, are provided in Trivedi et al. (2023). All data used in the current analyses were collected during the initial baseline visit. Among the first 1000 participants, 46 were excluded due to missing baseline body mass index (BMI) data, and 32 were excluded due to an underweight BMI categorization. Underweight youth were excluded from analyses due to the small group size. A final sample of 922 participants was used for BMI, depression, and anxiety analyses, and 871 of these had completed the Inventory of Depressive Symptomatology Self Report (IDS-SR) for inclusion in IDS-SR item-specific analyses.
Measurement tools
Body Mass Index (BMI) is a value frequently used in epidemiological research derived from the weight and height of a person (Nuttall, 2015). In TX-YDSRN, heights (in inches) and weights (in pounds) of the participants were self-reported to the study assessors (64%), pulled from the medical chart (20%), or measured in person by research coordinators (16%) and recorded in the Research Electronic Data Capture (REDCap) system (Harris et al., 2009). BMIs were automatically calculated within REDCap using this formula: weight (lbs.) / [height (in.)]^2 x 703. For this study, participants were divided into three categories using the guidelines for children and adolescents proposed by the Centers for Disease Control and Prevention (2022): healthy weight (BMI between 5th and 85th percentile), overweight (BMI between 85th and 95th percentile), and obese (BMI ≥95th percentile).
The Patient Health Questionnaire for Adolescents (PHQ-A) is a 9-item self-reported diagnostic scale used to assess depression severity over the past 2 weeks. Items are scored on a 4-point Likert-type scale ranging from 0 (Not at all) to 3 (Nearly every day). Possible scores range from 0 to 27, with higher scores indicating more severe depression. The PHQ-A is frequently used in depression research and various clinical settings and has been extensively tested, demonstrating sound psychometric properties (Johnson et al., 2002), including in the TX-YDSRN registry participants (Nandy et al., 2023). In this study, we used PHQ-8 (PHQ-A minus the appetite question) to avoid using appetite data in both independent and dependent variables and any undesirable strengthening of the possible effects.
The Generalized Anxiety Disorder-7 (GAD-7) is a 7-item self-reported scale designed to measure the severity of anxiety symptoms over the past 2 weeks, with items scored on a 4-point Likert-type scale ranging from 0 (Not at all) to 3 (Nearly every day) (Spitzer et al., 2006). Possible scores range from 0 to 21, with higher scores indicating more severe anxiety. The GAD-7 is frequently used in mental health research and has been shown to be valid and reliable in TX-YDSRN youth (Guzick et al., 2024).
The Patient-Reported Outcomes Measurement Information System (PROMIS) is a quality-of-life questionnaire developed by the National Institutes of Health (2024) that measures six domains (anxiety, depression, fatigue, peer relationships, physical function mobility, and pain interference). Questions pertain to the last 7 days, with items scored on a 5-point Likert scale from 0 (Never/With No Trouble) to 4 (Almost Always/Not able to do). Existing research establishes PROMIS domains as psychometrically sound (Cook et al., 2016; Minhajuddin et al., 2024). In this study, the participants under 18 years of age completed the pediatric version of PROMIS (DeWalt et al., 2015), the PROMIS Pediatric Profile-25 V2.0, while those 18 or older completed the adult, PROMIS-29 Profile V2.0, version of the form (Reeve et al., 2007). Only the items in the fatigue and physical function mobility domains were considered.
The Inventory of Depressive Symptomatology Self Report (IDS-SR) is a 30-item self-report assessment of depression-associated symptoms (Rush et al., 1996). The scale has demonstrated good validity and reliability (Trivedi et al., 2004) and is cross-culturally validated (Arjadi et al., 2017; Gili et al., 2011). The 16-item version of the scale, Quick Inventory of Depressive Symptomatology Self Report (QIDS-SR16), was psychometrically validated in adolescents (Bernstein et al., 2010). Here, only the items pertaining to acute changes in appetite and perceived weight (the timespan of interest is 2 weeks), which also appear in QIDS-SR16, were explored. For analysis, participants who reported any degree of change on appetite and weight decrease items were coded as “Appetite Decrease” and “Perceived Weight Loss,” respectively, while participants who reported any degree of change on appetite and weight increase items were coded as “Appetite Increase” and “Perceived Weight Gain,” respectively. Participants who selected “no change” on two appetite and two weight items were subsequently coded as “No Change in Appetite” and “No Perceived Change in Weight.”
Statistical analyses
Continuous outcomes are summarized as mean and standard deviation and analysis of variance was used to compare the groups. Categorical outcomes are summarized as frequencies and percentages, with chi-square analyses used to compare the groups. Analysis of Covariance (ANCOVA) techniques were performed to examine the association of BMI and IDS-SR measurements for patient-reported acute changes in appetite and weight with depression (PHQ-8; PHQ-A, minus the question about appetite), anxiety (GAD-7), and PROMIS measures of fatigue and physical function, while controlling for age, sex at birth, gender, race, and ethnicity. All analyses were performed using SAS version 9.4 (SAS Inc., Cary, NC) and p-values less than .05 were considered significant. For post hoc tests, Bonferroni correction was applied to adjust for multiple comparisons.
Results
Demographic and clinical characteristics
Demographics and baseline clinical characteristics based on BMI category.
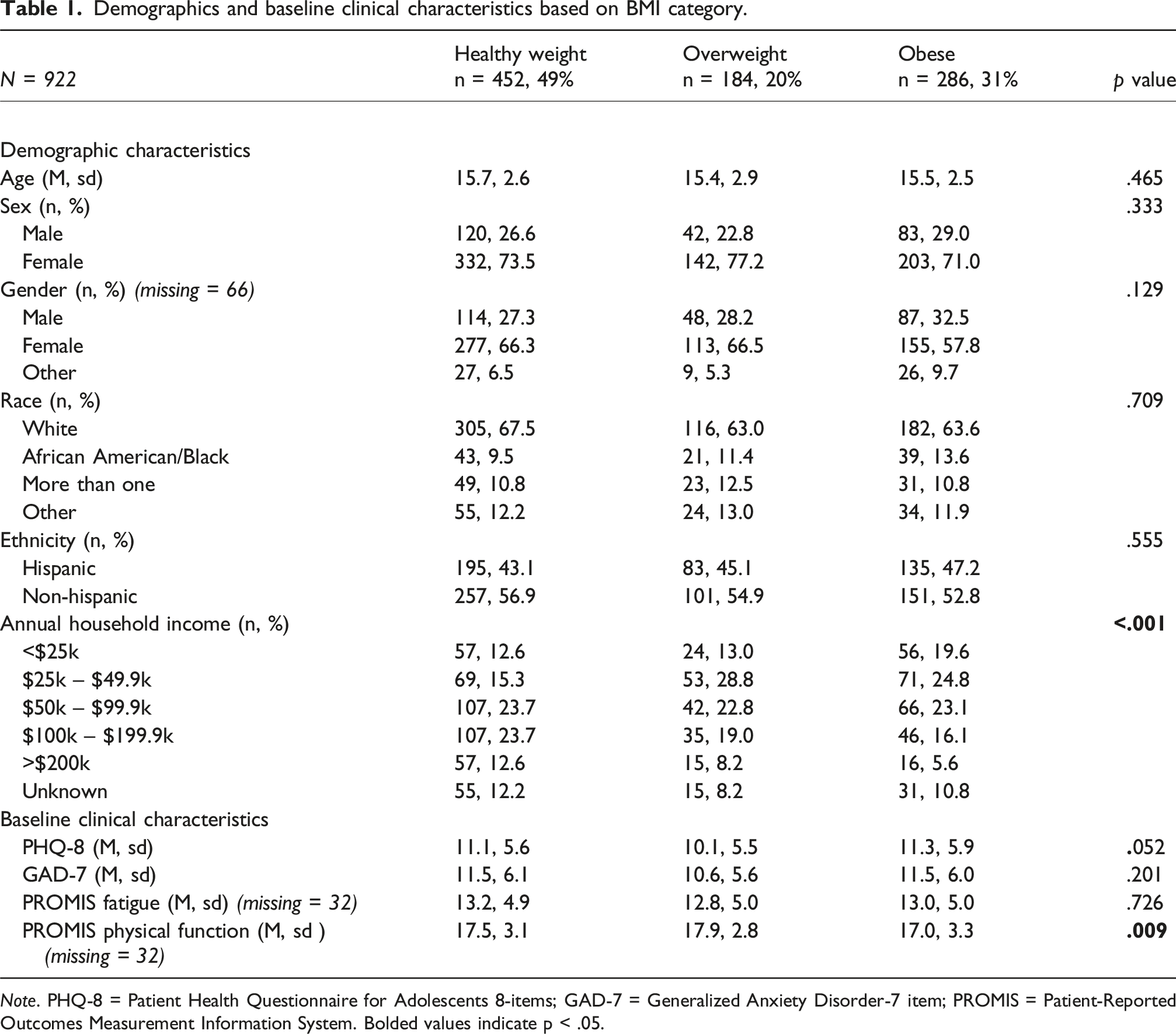
Note. PHQ-8 = Patient Health Questionnaire for Adolescents 8-items; GAD-7 = Generalized Anxiety Disorder-7 item; PROMIS = Patient-Reported Outcomes Measurement Information System. Bolded values indicate p < .05.
Associations of BMI categories with acute appetite and weight changes
Associations between changes in appetite and weight with BMI categories.

Bolded values indicate p < .05.
BMI, weight, and appetite changes’ impacts on depression, anxiety, fatigue, and physical function
To analyze potential interactions between BMI and other factors, we created four models with depression, anxiety, fatigue, and physical function as dependent variables, BMI categories as the independent variable, and acute weight and appetite changes as covariates while controlling for demographic variables.
Depression
PHQ-8 ANCOVA.

Bolded values indicate p < .05.
Anxiety
GAD-7 ANCOVA.
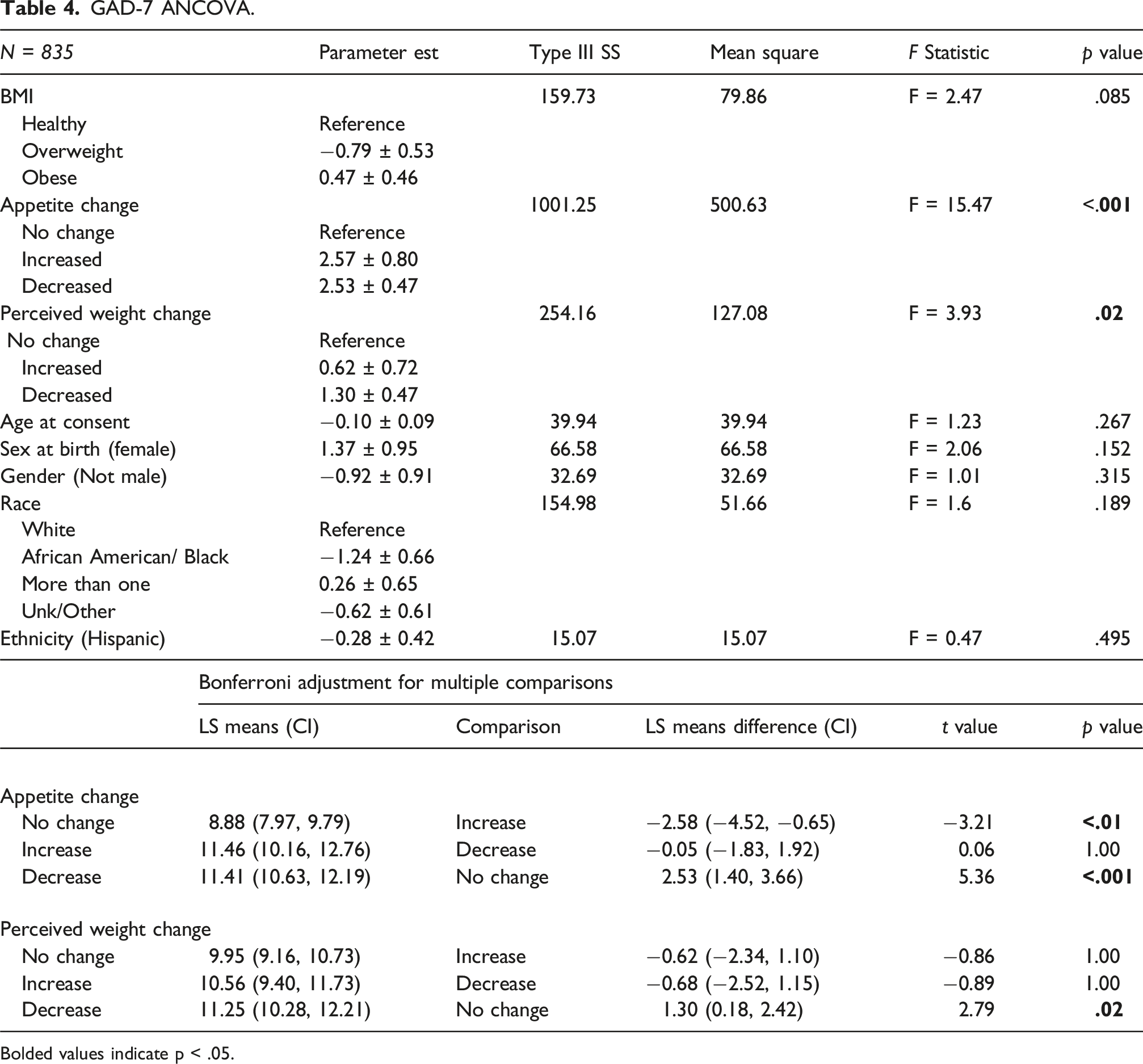
Bolded values indicate p < .05.
Fatigue
PROMIS fatigue ANCOVA.
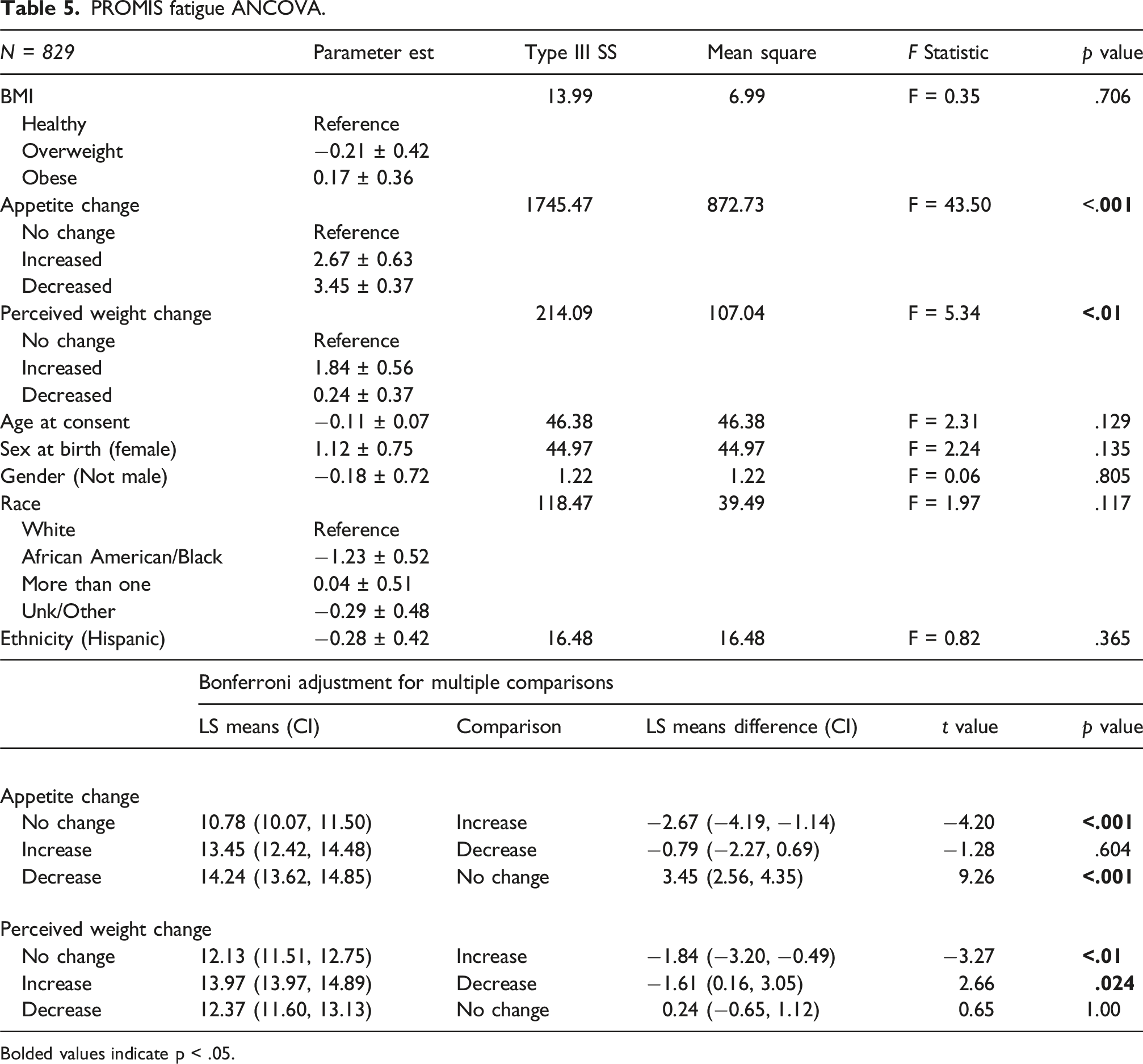
Bolded values indicate p < .05.
Physical function
PROMIS physical function ANCOVA.

Bolded values indicate p < .05.
Discussion
The present study explored the relationships between BMI categorization and depression, anxiety, fatigue, and physical function while assessing the impact of acute changes in appetite and weight on those relationships among youth between 8 and 20 years of age enrolled in the TX-YDSRN registry study. Our sample had higher proportions of overweight and obese youth than the national rates, which were 16.1% and 19.3%, respectively, of youth aged 2-19 (Fryar et al., 2020), and the obesity rate in the state of Texas, which was 20.7% of youth aged 10-17 (Michael & Susan Dell Center for Healthy Living, 2023). While there is no available data outlining overweight and obesity rates among youth seeking treatment for depression, these findings align with reports suggesting that depressed youth might be at a higher risk for developing obesity (Harriger and Thompson, 2012; Mannan et al., 2016). BMI groups varied by annual household income; a finding consistent with recently developed literature on the obesity-income link which demonstrates that excess weight tends to be more prevalent among individuals belonging to the lower socioeconomic class (Bentley et al., 2018; Kim & von dem Knesebeck, 2018). Interestingly, no significant differences between BMI groups in sex, gender, race, and ethnicity were observed in our sample despite frequently reported associations in the general population (Fryar et al., 2020; Ogden et al., 2018). Considering BMI groups alone, physical function significantly differed by BMI category, with depression severity trending toward significance and no differences in anxiety severity and fatigue. These findings are somewhat surprising, especially given the common comorbidity of anxiety in youth with depression (Alaie et al., 2021; Costello et al., 2003). We next sought to determine how common acute changes in appetite and weight were within each BMI category.
To assess whether being overweight or obese impacts acute appetite and weight changes, the percentage of participants in each BMI group reporting increased, decreased, or no change in appetite and weight were compared. While a third of the participants reported no change in appetite and over half did not report any perceived weight changes, we found that the proportion of the youth reporting increased appetite and perceived weight gain closely followed the BMI categories. Obese youth, in particular, were more likely to report acute increases in appetite and perceived weight gain. A Mendelian randomization study by Pistis et al. (2021) argued that obesity could be a cause of increased appetite in depressed participants with atypical clinical presentations. Another study suggested that excess adiposity in youth results in chronically increased appetite regardless of clinical status (Truby et al., 2020), providing another possible explanation of the present findings. Across all three BMI categories, however, the decrease, rather than increase, in appetite and perceived weight loss remained a more frequent change, which might be explained by the generally lower prevalence rates of atypical depression (Paing et al., 2008; Quitkin, 2002), of which both appetite increase and weight gain are symptoms.
Accounting for acute changes in appetite and weight while controlling for age, sex, gender, race, and ethnicity did not result in any meaningful changes in the BMI-clinical measure relationships, with BMI still only playing a role in depressive and physical function symptoms. Interestingly, overweight youth demonstrated lower depression severity compared to obese youth, but given neither group differed from healthy-weight youth, the clinical implications of this difference may be limited. Still, this finding may suggest being overweight, compared to obese, may be linked to less severe clinical symptomology for youth with depression. Physical function was also worse in the obese group, indicating poorer outcomes for youth with obesity. The lack of a relationship between BMI and fatigue is consistent with the other observations in youth (Guerrini Usubini et al., 2023; Viner et al., 2008), despite being reported in adults (Resnick et al., 2006), with these findings helping to confirm this interesting developmental nature.
Across the four clinical measures, acute changes in appetite, regardless of the direction of change, were almost always associated with poorer outcomes. Acute percevied changes in body weight were also associated with poorer outcomes in all but physical function, but sometimes only for one direction of change. Given that changes in body weight would likely occur over a longer timeframe than changes in appetite, it is not surprising that changes in appetite may be a better indicator of current clinical symptoms. Weight change was self-reported in this study, so it is likely that this variable reflects perceived weight changes rather than actual fluctuations. However, a previous study showed that perceived weight, and not actual excess weight status, increases the risk for major depression among youth (Roberts and Duong, 2013). Given that obese youth are more likely to have acutely increased appetite and perceived weight gain and these acute changes are generally associated with poorer clinical outcomes, high BMI is still of concern despite minimal direct associations between BMI and clinical outcomes. In some cases, calorie restriction could be used as an effective intervention to reduce depressive symptoms (Patsalos et al., 2021), though for overweight and obese youth, losing weight is difficult, and even the most complex interventions are often unsuccessful (Spiga et al., 2024; Truby et al., 2020). Finally, while statistically significant, the small differences in scores indicated that demographic covariates did not meaningfully impact clinical outcomes, suggesting these findings may be generalizable across demographic groups.
Study limitations
Despite the large sample size and data set, the study has several limitations. First, most of the data were derived from participant self-reports, which could be unreliable compared to objective measures. Second, due to the data’s cross-sectional nature, it was impossible to draw any conclusions regarding causality. Similarly, BMIs and changes in appetite and weight reported in the manuscript are a snapshot of the current state of the participants’ health and might not necessarily represent chronic clinical characteristics. Because the self-report evaluation period for subjective changes in weight and appetite considered the past 2 weeks, this is a particularly important limitation of the study, since BMI may take weeks or months to change (Cheng et al., 2014; Von Hippel et al., 2015). Future studies should consider more time points to better understand these changes and relationships between variables.
Future directions
Future research should focus on the long-term impacts of BMI on clinical outcomes and probe for causal relationships. As BMI is an indirect measure of body composition, investigators should focus on levels of adiposity instead, as it presents a more exact picture of the amount of undesirable weight. Similarly, measuring activity levels using wearable technology would be of great use because, in its relationship to mental health, high BMIs may act as a proxy for a lack of physical activity. Tracking actual changes in caloric intake would also help inform the perception of appetite. While medication status was not reported here, this may be an important variable for future work to consider. Psychiatric medications such as certain anti-depressants or anti-psychotics can lead to increased appetite and subsequent weight gain (Alonso-Pedrero et al., 2019; Berkowitz and Fabricatore, 2005; Virk et al., 2004), which may impact the relationship between excess weight and mental health. While questions remain, these findings provide interesting insights into how BMI interacts with clinical features and changes in appetite and body weight in depressed and/or suicidal youth.
Footnotes
Author note
Vadym Zhyrov is now at the Department of Psychology, University of Houston, Houston, TX, USA. Kendall N. Drummond is now at the Department of Psychological Sciences, University of North Carolina at Charlotte, Charlotte, North Carolina, USA.
Acknowledgements
The authors would like to thank the patients, clinics, staff, and colleagues who made this project possible. We acknowledge the TX-YDSRN teams from the following sites: University of Texas Southwestern Medical Center: Graham J. Emslie, Betsy D. Kennard, and Laura Stone; Baylor Medical Center: Ace Castillo, Emily Bivins, Kendall Drummond, and Eric Storch; Texas A&M University System Health Science Center: Tri Le, Olga Raevskaya, and Jessica Christian; Texas Tech University Health Science Center Lubbock: Jennifer Hudnall, Robyn Richmond, Anuththara Lokubandara, and Victoria Johnson; Texas Tech University Health Science Center El Paso: Sarah L. Martin, Zuber Mulla, Alejandro Fornelli, and Caitlin Chanoi; University of Texas at Austin Dell Medical School: Lexi Hughes, Tyler Wilson, Sophia Syed, Olivia Askew, Santiago Jimenez, Fernanda Pena Lozano, Michelle Lagrone, Eric Gonzales, and Jeffrey D. Shahidullah; University of Texas Health San Antonio: Norma Balli-Borrero, Sofia Ballesteros, Abigail Cuellar, and Presley Pargin; University of Texas Rio Grande Valley: Cynthia Garza, Diana Chapa, Dernay Coley, and Alessandra Rizzo-Esposito; University of Texas Health Science Center Houston: Cesar A. Soutullo, Jair C. Soares, Giovana B. Zunta-Soares, Sofia Galarza-Estrella, and Sydney Solberg; University of Texas Health Science Center Tyler: Jamon Blood, Colten Jones, Kiley Schneider, Pamela Thurman, and Preston Washburn; University of Texas Medical Branch: Michaella Petrosky; University of North Texas Health Science Center: David Farmer, Summer Ladd, Nicki Ahmuada, and Madelyn Guerra. The TX-YDSRN is implemented under the leadership of the central UT Southwestern Hub (Madhukar H. Trivedi, M.D., Principal Investigator; Sarah M. Wakefield, M.D., Medical Director [Texas Tech University Health Science Center Lubbock]; Abu Minhajuddin, PhD, Data/Statistics Lead; Lynnel C. Goodman, PhD, Scientific Lead; and Holli Slater, PhD, Operations Lead).
ORCID iDs
Ethical considerations
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the University of Texas Southwestern Institutional Review Board (STU2020-0665).
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This manuscript was funded by the Texas Youth Depression and Suicide Research Network (TX-YDSRN), a research initiative of the Texas Child Mental Health Care Consortium (TCMHCC). The TCMHCC was created by the 86th Texas Legislature and, in part, funds multi-institutional research to improve mental health care for children and adolescents in Texas. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding organizations.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mr. Zhyrov and Elmore and Ms. Gorman, AlZubi, Drummond, and Ableman do not have conflicts to declare. Drs. Walker, Slater, Ayvaci, Snyder, Goodman, Minhajuddin, and Baughn do not have conflicts to declare. Dr. Wakefield serves as an Executive Committee Member of the Texas Child Mental Health Care Consortium. Dr. Trivedi has provided consulting services to Acadia Pharmaceuticals, Alkermes Inc., Alto Neuroscience Inc, Axsome Therapeutics, BasePoint Health management LLC, Biogen MA Inc, Cerebral Inc., Circular Genomics Inc., Compass Pathfinder Limited, Daiichi Sankyo Inc., GH Research, GreenLight VitalSign6 Inc, Heading Health, Janssen Pharmaceutical, Legion Health, Merck Sharp & Dohme Corp., Mind Medicine Inc., Myriad Neuroscience, Naki Health Ltd, Neurocrine Biosciences Inc., Noema Pharma AG, Orexo US Inc., Otsuka America Pharmaceutical Inc., Otsuka Europe LTD, Otsuka Pharmaceutical Development & Commercialization Inc., Praxis Precision Medicines Inc, PureTech LYT Inc, Relmada Therapeutics Inc., SAGE Therapeutics, Signant Health, Sparian Biosciences, Titan Pharmaceuticals, Takeda Pharmaceuticals Inc, WebMD. He has received grant/research funding from NIMH, NIDA, NCATS, American Foundation for Suicide Prevention, Patient-Centered Outcomes Research Institute (PCORI), Blue Cross Blue Shield of Texas, SAMHSA, and the DoD. Additionally, he has received editorial compensation from Elsevier and Oxford University Press.
Data Availability Statement
TX-YDSRN data collection is ongoing, and data will not be publicly available until after study completion.