
Abstract
Keywords
Introduction
Being overweight (Body Mass Index, BMI, between 25 and 29.99) and obesity (BMI ≥ 30) are recognized as major health problems that are associated with adverse outcomes throughout the life course, such as the risk of several chronic diseases, reduced lifespan and poorer quality of life (Masocco et al., 2023). In the report on obesity in Europe, the World Health Organization (2022) highlighted that 59% of European adults and nearly one in three children (29% of boys and 27% of girls) are overweight or obese. Italy, the context in which the current study was conducted, mirrors this trend. Data for 2021–2022 (EpiCentro, 2023) indicate that 43% of the Italian population is overweight; specifically, 33% is overweight, and 10% is obese. Overweight and obesity also affect 27% of 18–24-year-olds (Masocco et al., 2023) and 11.2% of university students (Teleman et al., 2015).
Susceptibility to overweight and obesity “can be understood at various levels ranging from genetic, physiological, and metabolic to behavioral and psychological” (Cebolla et al., 2014: 58). At the behavioral and psychological levels, three main theories have been proposed to explain why some people gain weight and lose control of their eating behaviors: psychosomatic theory, theory of externality, and theory of restriction. Psychosomatic theory (Bruch, 1973) focuses on the role of emotional eating in response to emotional arousal states (e.g., anger, fear, and anxiety) instead of internal signals of hunger or satiety. External theory (Rodin, 1981) emphasizes eating in response to food-related stimuli (e.g., sight, smell, and taste). Restriction theory (Herman and Polivy, 1975) reflects the degree of conscious food restriction required to lose or maintain a certain weight. To explain overeating, this theory focuses on the possible side effects of dieting, specifically, the disinhibition effect. When restrained dieters decrease or abandon their cognitive decision to eat less, especially in response to distress, they tend to eat more than non-dieters (Polivy and Herman, 2020). Identification of these three eating patterns is vital for a deeper comprehension of individual differences in overeating.
The Dutch Eating Behavior Questionnaire
Based on the aforementioned theories, Van Strien et al. (1986) described three eating styles: emotional, restrained, and external eating. Emotional eating refers to the tendency to eat in response to negative emotions and distress; external eating corresponds to eating in response to environmental food cues, such as sight and smell; and restrained eating implies conscious attempts to reduce food intake to control body weight. These eating styles can be measured simultaneously using the Dutch Eating Behavior Questionnaire (DEBQ; Van Strien et al., 1986).
The DEBQ consists of 33 items with responses rated on a 5-point Likert scale (ranging from never to very often) covering the three domains: emotional eating (13 items; e.g., “Do you have the desire to eat when you are irritated?”), restrained eating (10 items; e.g., “Do you deliberately eat less in order to not become heavier?”), and external eating (10 items; e.g., “Do you eat more than usual when you see others eating?”). The original Dutch version was validated for adult women and men and showed good psychometric properties regarding factor structure, convergent and discriminant validity, and reliability (Van Strien et al., 1986).
The English translation of the original Dutch version (Wardle, 1987) has been the basis for translations and validations into many languages, such as Turkish (Bozan et al., 2011), French (Brunault et al., 2015; Lluch et al., 1996), Italian (Dakanalis et al., 2013), Spanish (Cebolla et al., 2014), Portuguese (Poínhos et al., 2015), German (Nagl et al., 2016), Maltese (Dutton and Dovey, 2016), Polish (Malesza, 2021; Małachowska et al., 2021), Romanian (Arhire et al., 2021), and Mexican Spanish (Flores-Quijano et al., 2023) on general or specific populations (e.g., overweight or obese persons, pregnant women, higher education students).
The three-factor structure of the DEBQ has been successfully replicated using both exploratory and confirmatory factor analyses (e.g., Barrada et al., 2016; Cebolla et al., 2014; Dakanalis et al., 2013; Malesza, 2021; Małachowska et al., 2021; Nagl et al., 2016). The measurement model proved to be invariant across different groups such as gender, age, and obese vs non-obese individuals (e.g., Dakanalis et al., 2013; Malesza, 2021; Małachowska et al., 2021; Nagl et al., 2016). The DEBQ has good internal consistency (Cronbach’s alphas of the three dimensions are between 0.96 and 0.81) and high test-retest reliability (between 0.92 and 0.94; e.g., Bozan et al., 2011; Dakanalis et al., 2013).
Regarding the correlations between the three dimensions of DEBQ, several studies have found positive associations between emotional and external eating subscales (e.g., Barrada et al., 2016; Cebolla et al., 2014; Dakanalis et al., 2013; Flores-Quijano et al., 2023; Malachowska et al., 2021; Malesza, 2021; Nagl et al., 2016). Although they target different situations, both eating styles correspond to relative insensitivity to internal hunger and satiety signals. Research has also reported positive associations between restrained and emotional eating dimensions (e.g., Barrada et al., 2016; Cebolla et al., 2014; Malachowska et al., 2021; Nagl et al., 2016; Van Strien et al., 1986). This may be due to the side effects of intense dieting, which generates stress and results in emotional instability (Van Strien et al., 1986). The link between restrained and external eating has also been described (e.g., Nagl et al., 2016), although it has not been found in all studies or found to be inverse or negligible (e.g., Barrada et al., 2016; Cebolla et al., 2014; Malachowska et al., 2021; Malesza, 2021).
Concerning demographic and anthropometric variables, research reports that: (a) emotional and external eating decrease with age, whereas restrained tends to increase (e.g., Barrada et al., 2016; Cebolla et al., 2014; Dakanalis et al., 2013; Małachowska et al., 2021; Nagl et al., 2016); (b) women score higher than men on emotional and restrained eating (e.g., Arhire et al., 2021; Barrada et al., 2016; Dakanalis et al., 2013; Nagl et al., 2016); (c) BMI status and eating behaviors are significantly and positively related with individuals with obesity and overweight scoring significantly higher than individuals with normal weight on all DEBQ subscales (e.g., Arhire et al., 2021; Barrada et al., 2016; Malesza, 2021; Nagl et al., 2016). Thus, each eating style may be a risk factor for overeating and weight gain (Malesza, 2021).
Some studies have examined the association between DEBQ scores and self-reported measures of eating disorder symptoms as measured by the Eating Attitudes Test (Garner et al., 1982). For example, relationships between emotional eating and bulimia as well as between restrained eating and dieting have been found (e.g., Bozan et al., 2011; Cebolla et al., 2014; Dakanalis et al., 2013). Another eating disorder symptom considered was binge eating, which corresponds to the occurrence of episodes characterized by the consumption of a large amount of food in a brief period and a sense of lack of control on overeating during such episodes. A few studies (e.g., Poínhos et al., 2015; Schulz and Laessle, 2010) found that emotional, external, and binge eating were positively associated with each other.
The DEBQ was originally developed and validated for adults; however, questionnaires shorter than the original 33-item version have been adapted for children (Halvarsson and Sjödén, 1998; Ohara et al., 2020; Van Strien and Oosterveld, 2008) and pre-adolescents in different languages (Wang et al., 2018). Bailly et al. (2012) tested the factorial validity and internal consistency of a short version (16 items) in an older and oldest-old French population. In their study, confirmatory factor analysis supported the hypothesized three-factor structure, which was invariant for gender, age, and BMI status. This short scale had satisfactory psychometric properties and the internal consistency values were adequate.
The current research
The present paper reports two studies to validate the short version of the DEBQ proposed by Bailly et al. (2012) in the Italian context with university students.
The advantages for both clinical and non-clinical assessments associated with the use of short versions of health questionnaires or scales have recently been emphasized in the literature (e.g., Machado et al., 2020; Nilsson et al., 2020). With short scales, the time spent on administration, application, and scoring is saved, and the monitoring of treatment outcomes may become more efficient. Short versions are also useful in multipurpose surveys with the need to use several scales to address different issues. Long questionnaires have a greater risk of measurement error due to mistakes or shortcuts enacted by respondents to complete the questionnaire (e.g., choosing the same response option for all items).
The choice to specifically validate this short version of the DEBQ in university students was anchored in the broad literature, indicating that university students are particularly vulnerable to developing non-adaptive eating styles (Choi, 2020), which are long-term and affect adult life (Poobalan et al., 2014). Furthermore, students are in a crucial period of life when they begin to assume responsibilities related to independence from their families and make autonomous choices in several areas such as consumption and nutrition. Thus, university students can be the recipients of specific educational or awareness programs.
The first study aimed to (a) evaluate the construct validity (factorial structure) of the Italian version of the short form of the DEBQ by Bailly et al. (2012), (b) test the invariance of the factorial structure across genders, (c) to analyze mean gender-based differences associated with the DEBQ dimensions, and (d) examine the relationships between DEBQ dimensions and BMI. Based on previous validations, we expected that the factorial structure would be invariant across genders, that women scored higher than men on emotional and restrained eating, and positive correlations between the three dimensions of the DEBQ and BMI status.
The second study aimed to deepen the criterion concurrent validity of this short version of the DEBQ by exploring the relations with a few relevant variables scarcely considered in previous research. We assessed the relationships with eating self-efficacy (Lombardo et al., 2020), state self-esteem (Heatherton and Polivy, 1991), and habit strength (Verplanken and Orbell, 2003) in consuming hypocaloric and hypercaloric snacks.
Self-efficacy applied to the eating domain can be defined as: “the belief in one’s ability to self-regulate eating” (Lombardo et al., 2020: 295). Lombardo et al. (2020) proposed the Eating Self-Efficacy Brief Scale, which addresses situations that challenge self-regulation of this behavior. Such situations may be social in nature (e.g., the presence of other people and food availability) or emotional (i.e., the presence of negative emotions). In their study, conducted in Italy, eating self-efficacy in social and emotional situations was negatively correlated with measures of disordered eating and emotional eating.
The relationship between self-esteem appraisal and eating styles has scarcely deepened. Markey et al. (2023) surveyed adults in eight countries (n = 6272). Negative correlations emerged among self-esteem, body satisfaction, and emotional and restrained eating scores.
Finally, some studies have shown positive associations between emotional eating and the consumption of energy-dense sweet snacks (e.g., Camilleri et al., 2014). Adriaanse et al. (2011, 2016), employed 7-days snack diaries to examine the extent to which emotional, restrained, external eating (from the DEBQ), and habit strength related to unhealthy snacking were predictors of the consumption of both healthy (i.e., hypocaloric) and unhealthy (i.e., hypercaloric) snacks. Eating habits proved to be important predictors of healthy and unhealthy eating behaviors. They do not simply reflect the frequency of past behavior but are mental constructs denoted by automaticity (Mazar and Wood, 2018). The results of Adriaanse et al. (2011, 2016) revealed positive associations between unhealthy snacking habit strength and emotional and external styles, and negative associations with restrained eating. Unhealthy snack consumption was positively associated with habit strength (targeting unhealthy snacking) and negatively associated with restrained eating, whereas healthy snack consumption was negatively associated with external eating.
Based on these results, we expected negative correlations between the two dimensions of eating self-efficacy, emotional and social, and the emotional and external eating dimensions of the DEBQ. Regarding state self-esteem, which comprises three components (performance, appearance, and social; Heatherton and Polivy, 1991), we hypothesized negative correlations between these three components and emotional and restrained eating styles. Finally, we posited that the habit strength to consume hypocaloric snacks would be positively associated with restrained eating, whereas the habit strength to consume hypercaloric snacks would be positively associated with emotional and external eating and negatively associated with restrained eating.
Study 1
Method
Data collection
Participants were initially recruited among students attending introductory psychology courses at the School of Psychology and School of Human and Social Sciences and Cultural Heritage (Padua University). Participation occurred online via the Qualtrics survey platform through a link sent to the students’ academic email addresses. The Qualtrics survey platform (www.qualtrics.com) allowed researchers to develop, test, and distribute surveys online, and was contracted to implement our Internet-based questionnaires.
Students were asked to personally fill out an online questionnaire and share the link to the survey with male university students from other degree programs at Padua University. First, participants were requested to read an instruction paragraph through which they were familiarized with the aim of the study, the estimated duration of the task, and the possibility of withholding their consent to participate at any time without any consequence. They were also assured that all answers would remain confidential, combined, and presented as a group. Then, they were asked to provide their informed consent by clicking the “I accept” button on the questionnaire web page. The study was conducted according to the guidelines of the Declaration of Helsinki, and the ethical committee of the institution, which supported the research and approved all procedures involving human subjects. All the participants provided informed consent to join the research.
Measures
The translation process of the DEBQ short version by Bailly et al. (2012) included both forward and backward steps by two Italian researchers who spoke fluent English and a native English speaker, and a pilot test to collect feedback on the readability and comprehensibility of the translated items. The instrument was administered to 10 individuals (university students from non-psychological degree courses; six women and four men), and no significant changes were made to the instrument.
The short version of the DEBQ (Bailly et al., 2012) contains 16 items rated on a scale ranging from 1 = never to 5 = very often. The items reflect the three eating styles: (a) emotional eating (6 items; e.g., “Do you have the desire to eat when you are feeling lonely?”), (b) restrained eating (5 items; e.g., “Do you deliberately eat foods that are slimming?”), and (c) external eating (5 items; e.g., “If you see or smell something delicious, do you have a desire to eat it?”).
Finally, sociodemographic questions included gender, age, geographic area of residence, degree program attended, and self-reported height and weight. BMI was calculated using self-reported height and weight using the standard formula: weight (kg)/height (m)2.
Participants
Study 1: Survey sample characteristics (n = 613).

Data analysis
Statistical analyses were conducted using M-Plus 8 (factorial analyses and measurement invariance) and SPSS 27 (descriptive analyses, reliability assessed by means of Cronbach’s alpha, correlations, and differences between men’s and women’s scores). There were no missing data on the DEBQ as participants were prompted to respond to all items. After verifying the univariate normality of item distributions using skewness and kurtosis indices, we checked Mardia’s (1970) coefficients to assess the multivariate distributions. To examine the factor structure of the 16-item-DEBQ, we used a two-step process involving exploratory factor analysis (EFA) in the first step and confirmatory factor analysis (CFA) in the second. Thus, the entire sample was divided into two subsamples using the SPSS 27 random case selection procedure. There were no significant differences between the two random subsamples in terms of gender, geographic area of residence, mean age, and BMI (p s > .39).
We applied EFA (Geomin rotation) on the first subsample (n = 294) and CFA (Robust Maximum Likelihood estimation, MLR), with the covariance matrix as input, on the second subsample (n = 319). Based on Bagozzi (1994), the second subsample size for the CFA was deemed adequate, as it exceeded the recommended 5:1 cases-to-parameter ratio. Model fit was determined following the indices recommended by Hu and Bentler (1999): Root Mean Square Error of Approximation (RMSEA), Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), and Standardized Root Mean Square Residual (SRMR). Specifically, RMSEA values equal to or lower than 0.06, CFI and TLI values equal to or higher than 0.95, and SRMR values approximately equal to 0.08 or lower were considered satisfactory.
Cronbach’s alpha and composite reliability (CR) coefficients were determined to estimate reliability. Values higher than 0.60 were considered appropriate (Bagozzi and Yi, 1988).
To test DEBQ measurement invariance across genders, the multi-group procedure was applied with three consequential hypotheses: (i) configural invariance (requiring an identical number of factors and the pattern of factor-item relations across the two groups), (ii) metric invariance (invariance of factor loadings across groups), and (iii) scalar invariance (invariance of factor loadings and item intercepts across groups). Model comparisons were based on a chi-square difference test, computing the Satorra-Bentler scaled χ2 (Satorra and Bentler, 2001) (i.e., Δχ2Satorra-Bentler scaled). However, this test is an overly stringent criterion for invariance (Meade et al., 2008). Therefore, Chen (2007) also recommended exploring changes in CFI (ΔCFI), RMSEA (ΔRMSEA), and SRMR (ΔSRMR). If ΔCFI ≤0.010, ΔRMSEA ≤0.015, and ΔSRMR ≤0.030 for tests of factor loading invariance, and ΔCFI ≤0.010, ΔRMSEA ≤0.015, and ΔSRMR ≤0.010 for tests of intercept invariance, then measurement invariance is supported. Partial measurement invariance testing can be conducted if non-invariance is found by allowing problematic items to be freely estimated across groups (Putnick and Bornstein, 2016).
Results
Exploratory and confirmatory factor analyses
Descriptive statistics and factor loadings.

Note. The exact wording of the items could not be presented owing to copyright restrictions. Item numbering refers to the order of presentation in the Italian version.
aFactor loadings are derived from the model with correlated errors.
EFA with three correlated latent factors was performed on the first subsample (n = 294). Parallel analysis indicated that three factors from the actual dataset had eigenvalues greater than the criterion eigenvalue generated from random data (i.e., λ1 5.52 > 1.42, λ2 2.41 > 1.33, λ3 1.84 > 1.26). Moreover, the fit indices for the three-factor model were adequate, χ2 (75) = 209.76, p = .00, RMSEA = 0.08, 90% CI [0.07, 0.09], CFI = 0.94, TLI = 0.91, SRMR = 0.04. Factor 1 included the six emotional eating items, Factor 2 the five restrained eating items, and Factor 3 the five external eating items. Factor loadings ranged from 0.37 to 0.94 on the expected latent factor (Table 2).
The CFA of the three-correlated factor model was performed on the second subsample (n = 319) and indicated an acceptable fit: χ2Satorra-Bentler (101) = 270.55, p = .00, RMSEA = 0.07, 90% CI [0.06, 0.08], CFI = 0.93, TLI = 0.91, SRMR = 0.06. An examination of the modification indices suggested the estimation of error covariances between two pairs of items: items two and three (external dimension), and items 14 and 10 (restrained dimension). Given the high redundancy in wording and meaning, these items could share method effects. The same strategy was used by Bailly et al. (2012), Barrada et al. (2016), Cebolla et al. (2014), and Nagl et al. (2016).
The model was revised accordingly, and fit indices turned out to be satisfactory: χ2Satorra-Bentler (99) = 189.8, p = .00, RMSEA = 0.05, 90% CI [0.04, 0.07], CFI = 0.96, TLI = 0.95, SRMR = 0.07. All loadings on the expected latent factors were significant (Table 2; Figure 1). The correlations between factors followed the expected pattern: emotional and restrained eating, r = 0.46, p < .001; emotional and external eating, r = 0.41, p < .001; and external and restrained eating, r = 0.16, p < .05. CR was 0.93 for emotional eating, 0.82 for restrained eating, and 0.74 for external eating. Cronbach’s alpha was .93 for emotional eating, 0.82 for restrained eating, and 0.73 for external eating. Study 1: Three-factor oblique model of the short version of the DEBQ.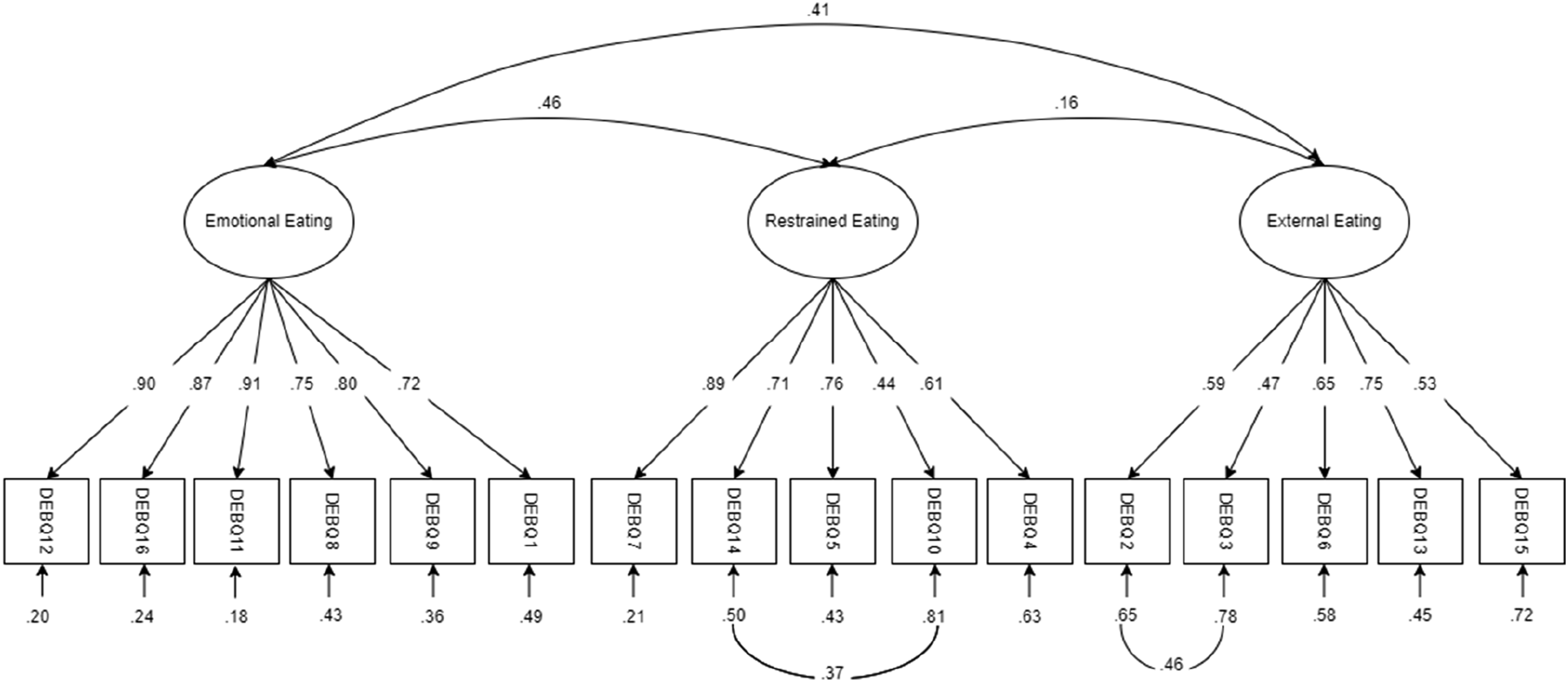
Gender measurement invariance
Results for gender measurement invariance.

Note. *p < .05, **p < .001.
aThe intercepts of items 4, 6, 7, and 15 were freely estimated.
Eating styles, gender, and BMI
Means and standard deviations for emotional, restrained, and external eating in the overall sample and female and male subsamples.
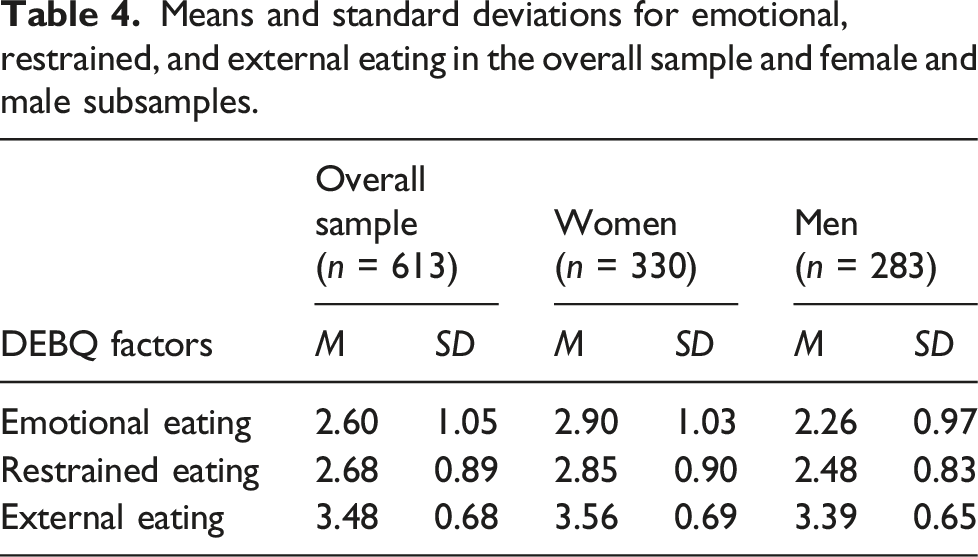
We examined the mean differences associated with the three dimensions of the DEBQ across genders using MANOVA. The main multivariate effect was significant (F3,609 = 23.70, p < .001, η 2 par = .11). The univariate effects were significant for all three eating styles: emotional eating (F1,611 = 61.96, p < .001, η 2 par = .09), restrained eating (F1,611 = 28.06, p < .001, η 2 par = .04), and external eating (F1,611 = 9.63, p < .003, η 2 par = .02). Women scored higher than men for all styles.
Correlations of eating styles with BMI.

Note. *p < .05, **p < .01.
Study 2
Method
Data collection
Participants were initially recruited among students attending introductory psychology courses at two universities: the Padua University and the Salesian University Institute of Venice (IUSVE). As in Study 1, students were asked to personally complete an online self-report questionnaire created through the Qualtrics platform and share the link to the survey with their personal contacts (i.e., university students of other Italian universities) also using social media platforms (e.g., WhatsApp, Instagram, and Facebook). The instructions and modality used to obtain students’ informed consent were the same as those in Study 1. The study was conducted according to the guidelines laid down in the Declaration of Helsinki, and the ethical committee of the institution, which supported the research and approved all procedures involving human subjects. All the participants provided informed consent to participate in the study.
Measures
Dutch eating behavior questionnaire
The short version of the DEBQ tested in Study 1 was used.
State self-esteem scale
The Italian version of the scale by Heatherton and Polivy (1991), validated in Italy by Bobbio (2009), was adopted. This scale consists of 14 items that measure three distinct factors: performance (6 items; e.g., “I feel confident about my abilities”; α = 0.81), social (4 items; e.g., “I feel concerned about the impression I am making”; α = 0.84), and appearance (4 items; e.g., “I feel satisfied with the way my body looks right now”; α = 0.87). The response scale ranged from 1 = completely disagree to 5 = completely agree. For the performance and appearance dimensions, higher scores denoted higher self-esteem; for the social dimension, higher scores denoted lower self-esteem. Consequently, the scores for this dimension were reversed.
Eating self-efficacy brief scale
We used the scale developed and validated in Italy by Lombardo et al. (2020), which aims to capture how easy it would be to resist the urgency to eat in different circumstances: emotional (4 items; e.g., “When you are nervous for personal reasons”; α = 0.88) and social (4 items; e.g., “When you eat outside (e.g., restaurant, bar, pizzeria) with friends”; α = 0.80). The response scale was a 5-point Likert-type scale ranging from 1 = not easy at all to 5 = completely easy.
Habit strength to consume hypocaloric and hypercaloric snacks
Following Adriaanse et al. (2011), we adapted four items from the Self-Report Habit Index (Verplanken and Orbell, 2003), validated in the Italian context by Canova and Manganelli (2016). These items measured habit strength in terms of frequency and automaticity. Hypocaloric vs hypercaloric snacks were defined as the following kinds of food that could be consumed between meals: fresh fruit and vegetables vs sandwiches, potato chips, pastry, chocolate, or a slice of pizza. The items were: “Consuming hypocaloric/hypercaloric snacks is something that…” “I do frequently,” “I do automatically,” “I do without thinking,” “It belongs to my routine.” The response scale ranged from 1 = completely disagree to 5 = completely agree. For hypocaloric, α = 0.91; for hypercaloric, α = 0.90.
Furthermore, sociodemographic questions that dealt with gender, age, geographic area of residence, degree program attended, and self-reported height and weight used to compute BMI.
Participants
Study 2: Survey sample characteristics (n = 856).

Data analysis
A three-factor model with correlated errors between two pairs of items was tested via CFA to check the construct validity of the short DEBQ scale using the same statistical package, analytical procedure, and fit indices as in Study 1. SPSS 27 was used for the descriptive analyses and reliability estimates through Cronbach’s alpha, and Pearson’s correlation coefficients.
Results
Confirmatory factor analysis
The fit indices were satisfactory, as in Study 1: χ2 Satorra-Bentler scaled (99) = 401.59, p = .00, RMSEA = 0.06, 90% CI: [0.05, 0.07], CFI = 0.94, TLI = 0.93, SRMR = 0.07. The factor loadings of items on their own latent factor were all significant and ranged from 0.34 (item 3, external eating) to 0.89 (item 7, restrained eating). The following were the correlations between the latent factors: emotional and restrained eating, r = 0.35, p < .001; emotional and external eating, r = 0.28, p < .001; and restrained and external eating, r = 0.01, ns.
Reliability, gender differences, and correlations with BMI
The CR values were between 0.91 and 0.66 and deemed adequate. The alpha coefficients were 0.91 (emotional eating), 0.83 (restrained eating), and 0.68 (external eating). Gender-based differences were examined using MANOVA. The main multivariate effect was significant (F3,852 = 36.35, p < .001, η 2 par = .11), as well as univariate effects (Fs1,854 > 10.66, p < .001, .01 < η 2 pars < .09), and women scored higher than men on emotional (2.87 vs 2.29), restrained (3.00 vs 2.58), and external (3.52 vs 3.39) eating.
In the entire sample, the correlations between BMI and emotional (r = 0.20, p < .01) and restrained eating (r = 0.17, p < .01) were significant but small in size (Cohen, 1988). The coefficient between BMI and external eating was not significant (−0.06, p < .06). The correlation pattern between BMI and DEBQ scores in women and men mirrored that of Study 1.
Concurrent criterion validity and snack consumption habit
Self-esteem, eating self-efficacy, and habit strength: Descriptive statistics and correlations by gender.

Note. The response scales ranged from 1 to 5. *p < .05, **p < .01.
Regarding the overall sample (n = 865), participants described themselves as moderately worried about other people’s judgments or their public image (social: M = 2.64). Furthermore, they reported considering themselves to be performing (performance: M = 3.55) and of average attractiveness (appearance: M = 3.15). The correlations between the DEBQ subscales and self-esteem scores were in the expected direction: individuals with higher emotional eating scores reported considering themselves as poorly effective (performance: r = −0.29, p < .001), attractive (appearance: r = −0.37, p < .001), and worried about other people’s judgments or their public image (social: r = −0.29, p < .001). The effect size of these correlations was medium. The correlations between self-esteem dimensions and restrained and external eating were negative (between −0.09 and −0.27), significant, but small in size. A strong correlation was observed between the appearance dimension of self-esteem and restrained eating.
Furthermore, the eating self-efficacy scores revealed an average level of emotional efficacy (M = 3.27) and a low level of efficacy in social situations (M = 2.35). The pattern of negative correlations between eating self-efficacy and DEBQ dimensions aligned with our predictions. Moreover, higher coefficients were observed for the relationships between emotional self-efficacy and emotional eating (r = −0.75, p < .001), and between social self-efficacy and external eating (r = −0.43, p < .001).
The participants reported a low habit of consuming both hypocaloric and hypercaloric snacks (M = 2.69 and M = 2.28, respectively). As expected, hypocaloric snack scores were positively correlated with restrained eating (r = 0.24, p < .001). For hypercaloric snack scores, positive correlations emerged with emotional and external eating (r = 0.23, p < .001 and r = 0.20, p < .001, respectively), whereas those with restrained eating were negative (r = −0.26, p < .001). As shown in Table 7, the correlation patterns for men and women were largely equivalent.
General discussion
The primary aim of this study was to validate the Italian version of a brief form of the DEBQ (Bailly et al., 2012) in university students. To achieve this, we conducted two studies with two different samples of a total of 1469 students. Our results confirmed the three-factor structure of the DEBQ across both samples. As in previous studies, a few model modifications, such as the estimated error covariance of two pairs of items, were necessary to achieve a good fit. All items in our final model loaded onto the same factors as those in the original DEBQ. The 16-item scale showed satisfactory internal consistency and reliability. Correlations between factors followed the expected pattern: emotional and external eating were positively correlated, as were emotional and restrained eating. The correlation between restrained and external eating was negligible or not significant. The multigroup analysis confirmed the measurement invariance of the three correlated first-order factors structure across genders.
Regarding the relationships between the scale dimensions and gender, women scored higher than men on all three dimensions. The results regarding emotional and restrained eating align with previous studies (e.g., Arhire et al., 2021; Barrada et al., 2016; Dakanalis et al., 2013; Malesza, 2021; Nagl et al., 2016). Women are more prone to use food as a means of coping with psychological distress and internal emotional factors (i.e., fear, anxiety, and anger) than men. With regard to restrained eating, a possible explanation relies on the stronger social and media pressure for a slim body image perceived by women compared to men but also on their greater awareness and concern about food and fear of gaining weight. Concerning external eating, our results differed from those reported in previous literature, in which no significant differences were found between men and women. However, focusing on the university students, we found at least one study in which women scored higher than men on external eating style (Hao et al., 2023). Therefore, further investigation is required.
With respect to BMI, similar to prior studies (e.g., Cebolla et al., 2014; Dakin et al., 2023; Van Strien et al., 2009), the evidence we collected supported the existence of positive correlations of BMI with emotional and restrained eating in the entire sample and in both women and men, thereby suggesting that the higher the index, the higher the tendency to eat following emotional and restrained styles. The positive correlation between emotional eating and BMI has been reported in almost all studies, and eating in response to negative emotions and distress is a risk factor for overeating and weight gain. Concerning restrained eating, our results replicated those of other studies (e.g., Dakin et al., 2023; Warschburger et al., 2023). In the literature, we can find two possible explanations: on the one hand, as a result of disinhibition, increased restraint puts dieters at a higher risk of overeating and, consequently, an increased BMI. On the other hand, people with higher body weights attempt to constrain food intake to lose weight or prevent weight gain. The absence of a relationship between BMI and external eating, which has also been reported in other studies (e.g., Barrada et al., 2016; Van Strien et al., 2009), suggests that responsiveness to food cues may be a general characteristic and not specific to overweight people (Rodin, 1981). Moreover, this reinforces the proofs showing that emotional and external eating refer to separate constructs, although they may often co-occur.
Concurrent criterion validity of the 16-item scale can be considered as achieved. To investigate this, we explored the correlations between the three DEBQ dimensions and self-esteem, eating self-efficacy, and snacking habits. Our results confirmed the expected links. Emotional and restrained eating styles were negatively correlated with appearance and social dimensions of self-esteem in both women and men, restrained eating was negatively correlated with performance dimension only in women, and external eating was negatively correlated only with the social dimension and only in women. The negative correlations of eating styles with self-esteem are consistent with those of previous studies (e.g., Markey et al., 2023). Moreover, it is worth noting that the strongest correlations involved the appearance dimension, both for women and men: individuals with higher scores on the emotional dimension, (and also with restraint in the case of women) considered their silhouette as poorly good and unattractive. These findings further emphasize that maladaptive eating styles are associated with low self-esteem, particularly body appreciation, which may largely depend on socially accepted standards.
We found negative correlations between all DEBQ subscales and emotional eating self-efficacy, and between external eating and social eating self-efficacy. The negative relationship between emotional eating self-efficacy and emotional eating is consistent with Lombardo et al. (2020). Hence, the DEBQ could successfully capture low levels of efficacy in regulating eating behavior in situations that challenge ingestion self-regulation, such as social facilitation (e.g., in the presence of other people and food availability) or emotional activation (specifically negative emotions).
The second study also analyzed the relationship between eating styles and snacking habits. Our analyses revealed some associations that have been infrequently investigated in the literature. The restrained eating dimension was positively related to the habit of consuming healthy hypocaloric snacks (such as fruit and vegetables) and negatively associated with the consumption of hypercaloric snacks in the overall sample and in both men and women. This suggests that the participants’ habit of choosing low-calorie foods as snacks was linked to a tendency to consciously limit food consumption. As revealed in previous studies (e.g., Canova and Manganelli, 2016), habit strength regarding the consumption of healthy snacks can be associated with conscious deliberation processes, such as intention development. With regard to emotional and external eating styles, as in previous studies (Adriaanse et al., 2011, 2016), we found positive correlations with habits of consuming hypercaloric or unhealthy snacks. Concerning emotional eating, as suggested by other studies (e.g., Camilleri et al., 2014; Caso et al., 2020; González et al., 2022; Moss et al., 2020), the positive association may imply that individuals who are more prone to eating in response to negative emotions are more motivated to choose unhealthy hyperpalatable energy-dense snacks (such as sweet and savory snacks), which have specific qualities that make them more comforting than others (Gibson, 2012). In line with a study by Zhang et al. (2023), external eating was positively associated with the frequency of hypercaloric snacking. This could be because eating sweet and salty snacks can satisfy the moment’s desire and imply indulging in whims prompted by external food-related stimuli.
Briefly, the validity of the short version of the DEBQ was successfully reproduced in the two Italian samples. Our analyses showed that it could be an effective instrument for measuring the eating behaviors among Italian university students. Our study confirmed that eating styles measured by the DEBQ are associated with higher BMI, lower self-esteem, and lower eating self-efficacy, and that these eating styles can be considered maladaptive as they are consistently associated with an unhealthy diet, particularly snacking habits.
This study makes a valuable contribution to eating style assessment by validating the short version of the DEBQ proposed by Bailly et al. (2012) in a different context and with different age group. In addition, few studies have assessed the relationships between the DEBQ, self-esteem, eating self-efficacy, and snacking habits.
A few limitations of this study should be noted. We used two convenience samples of Italian university students aged 18–30. Therefore, future research should determine whether this form of the DEBQ is valid for the general population and other specific groups (e.g., groups with different ages or patients with eating disorders). Additionally, we did not collect data on test-retest reliability or sensitivity to change; our results were based on self-reported measures, which are susceptible to social desirability and acquiescence effects; and the correlations between eating styles and snacking habits were examined by considering only broad categories such as hypocaloric and hypercaloric snacks. Our study was also limited by its cross-sectional nature; therefore, no conclusions could be drawn regarding the causal direction of the obtained associations. Prospective studies are required to assess the long-term relationships between eating styles, psychological variables, and food habits. Finally, it is worth remembering that our data were collected during the COVID-19 pandemic. It is difficult to determine if and how both the pandemic and lockdown measures impacted our results, although other studies in Italy have shown that lockdown conditions increased indices of emotional eating and the use of food to manage distress (e.g., Cecchetto et al., 2021).
Despite these limitations, it can be concluded that the Italian version of the 16-item DEBQ is a psychometrically sound measure that could be proficiently employed to investigate the three eating dimensions in Italian university students. A brief version of the DEBQ can be advantageous for both non-clinical and clinical screening (Nilsson et al., 2020). Moreover, the administration of a more parsimonious measure can be convenient in the case of large questionnaires assessing several variables that can create fatigue in respondents and, in turn, lead to decreased motivation, withdrawal, or reduced quality of the data collected.
Future studies can provide further evidence for the soundness of the brief Italian version of the DEBQ, for example, by analyzing its test-retest reliability or sensitivity to change. Examining eating styles in representative samples or different age groups could further enhance the generalizability of our findings as the eating habits of university students may differ from those of people of different ages.
Conclusions
This study aimed to validate the 16-item short version of the DEBQ (Bailly et al., 2012) in the Italian context by recruiting convenience samples of university students. Concurrent criterion validity was tested by examining its relationship with gender, BMI, self-esteem, eating self-efficacy, and snacking habits. Owing to the potential advantages associated with time-saving in administration and scoring, as well as the lower risk of inflating measurement error due to mistakes or response set, short scales may be useful for both clinical and non-clinical assessments and in multipurpose surveys that need to use several scales on different issues. University life is a transitional stage for young people between adolescence and adulthood, with poor (if not lacking) parental supervision. Therefore, university students may represent a relevant target for monitoring with ad hoc instruments because they may consolidate eating habits that are potentially decisive throughout future life. The three-factor structure of the short DEBQ received support and can be considered invariant across genders. Correlations among the three eating styles captured by the DEBQ (i.e., emotional, restrained, and external) with gender, BMI, eating self-efficacy, self-esteem, and snacking habits aligned with the expected patterns. The Italian version of the short DEBQ proved to be psychometrically sound and can be used with confidence to explore the possible antecedents and consequences of eating styles among university students.
Footnotes
Author contributions
Study conception and design: AMM, LC, and AB1. Data collection: LC, AB1, and AB2. Data coding and analysis: LC and AB2. Writing of the manuscript: AMM, LC, and AB1. Assistance with revisions: AMM, LC, AB1, and AB2. All authors have approved the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research project was funded by the Salesian University Institute of Venice (IUSVE), “Call di Ricerca IUSVE a.a. 2021–2022.”
Ethical statement
Data availability statement
Data and codes are available on request from the corresponding author.