
Abstract
Extensive training, overuse, overexertion, and repetitive movements put Soldiers at increased risk for musculoskeletal injuries (MSIs). The present study investigated the prospective association between psychological strengths, physiological and social factors, and non-combat-related MSI in a sample of 24,746 active duty Army Soldiers. Over a mean follow-up period of 21.07 months (SD = 16.07), 65.42% of the Soldiers examined were treated for an MSI. Applying survival analysis techniques and adjusting for relevant physiological and social factors, we found greater baseline Optimism, Positive Affect, Coping, and Adaptability were each associated with a modest reduction in risk of MSI (4-8%). Additionally, being older, female, married, and having a higher BMI were each associated with an increased MSI risk, whereas being an officer (relative to enlisted) and obtaining post-secondary education were each associated with a decreased MSI risk. Future research should examine the mechanisms through which psychological-based interventions may impact Soldiers’ risk of MSI.
Introduction
Musculoskeletal injuries (MSIs; including injuries to the bones, joints, or muscles) are a leading health problem in the U.S. (Cieza et al., 2021), with annual estimated treatment costs in the United States exceeding $213 billion (American Academy of Orthopaedic Surgeons, 2016).
Within the U.S. Army, occupational demands including extensive training, overuse, overexertion, and repetitive movements put Soldiers at increased risk for MSIs. Indeed, approximately half of all active duty Soldiers experience an MSI in a given year, which substantially impacts the medical readiness of our troops. MSIs account for a combined total of over 10 million limited duty days each year (United States Army Public Health Center, 2021). Importantly, a significant portion of musculoskeletal injuries in the Army are not combat related, with approximately 70% of injuries resulting from cumulative musculoskeletal overuse (United States Army Public Health Center, 2021).
Research has also found that the majority (60%) of overexertion injuries among active duty Army Soldiers result from running, walking, marching, hiking, and playing basketball, with running-related injuries making up 32% of all overexertion injuries (Canham-Chervak et al., 2016). Falls have long been cited among the leading causes of MSI in the military (Jones et al., 1999; Ruscio et al., 2010; Senier et al., 2002; United States Army Public Health Center, 2021). Non-deployment MSIs tend to occur in sports settings (22%), during parachuting activities (20%), and during walking or marching (19%; Hauschild et al., 2016). The number of ambulatory visits related to musculoskeletal disorders (including MSI) among active component service members has increased since 2014 (Armed Forces Health Surveillance Branch, 2017).
In addition to reducing the readiness of Army Soldiers, MSIs are also very costly. Across the Department of Defense, MSIs account for almost 2.5 million medical visits, and cost $548 million in patient care (US Armed Forces, 2010; Rhon et al., 2016). Overexertion injuries are most often addressed through outpatient visits, which significantly contribute to healthcare burden. Differences in non-modifiable risk factors have been documented in outpatient visit rates. For example, higher outpatient visit rates have been observed among females (compared to males), active duty (compared to National Guard and Reserve), younger Soldiers (under the age of 25), junior enlisted Soldiers, and Soldiers with a motor transport service position (Canham-Chervak et al., 2016; Kazman et al., 2015). Better understanding the factors that place Soldiers at greater MSI risk, and developing targeted interventions when possible, has the potential to reduce burden on the Military Health System (particularly outpatient clinics), while also cutting costs and potentially improving Soldier health and well-being.
Physiological and social risk factors of musculoskeletal injury
The association between physiological risk factors and MSI risk in the military has received a great deal of attention. There is strong scientific evidence, for example, that high body mass index (BMI; i.e., ≥25) is a risk factor for MSI (Sammito et al., 2021). Compared to Soldiers classified as meeting body composition standards, Soldiers exceeding the body composition standards experienced a 47% greater chance of MSIs and used health care services 49% more often (Cowan et al., 2011). Another study found that Soldiers classified as overweight, underweight, or obese were at significantly greater MSI risk, compared to those with an average BMI (Hruby et al., 2015). Similarly, in a study measuring fitness and injury among active duty, National Guard, and Reserve women, higher BMI was predictive of physical injury (Kazman et al., 2015).
There is also strong evidence that being female is a risk factor of MSI in the military (Sammito et al., 2021). One study found that military women were generally less fit and suffered MSIs at greater rates than men during physical training (Kazman et al., 2015). These authors also found that active duty women were more likely to have experienced an MSI in the past 6 months (Kazman et al., 2015). Similarly, a study examining injury in the context of Army military police training found that 34.2% of men and 66.7% of women experienced an MSI during the training (Knapik et al., 2013).
In addition, there is moderate scientific evidence for age as a risk factor (Sammito et al., 2021). Many studies examining the relation between age and MSI, including those in the review conducted by Sammito et al., observed higher rates of MSI among older Soldiers, compared to younger Soldiers (e.g., Grier et al., 2010; Hill et al., 2013; Knapik et al., 2013). One study of Soldiers undergoing initial entry training (IET), for example, found that older age was associated with a greater likelihood of having an acute MSI (Sefton et al., 2016). Other studies, however, have failed to identify a statistically significant association between age and MSI risk in multivariate models (e.g., Skeehan et al., 2009).
Beyond physiological risk factors for MSI, several social factors have also been examined in military populations. There is weak evidence, for example, that lower levels of education are a risk factor for MSI (Sammito et al., 2021). A small study of Marines (n = 356) found that lower education was associated with a greater risk of incurring a foot injury during mountain training exercises (Reynolds et al., 2000). In contrast, Knapik et al. (2007) did not find a statistically significant relationship between education and injury risk. There is also weak evidence that lower rank is associated with MSI risk in military samples. Injuries have also been more commonly observed among enlisted Soldiers, relative to officers (Hill et al., 2013). A study on altitude injuries sustained by parachutists also found lower ranking personnel to be at greater risk of injury (Craig and Lee, 2000). However, other smaller studies examining the relationship between rank and injury risk have failed to detect a statistically significant association (Lauder et al., 2000; Roy et al., 2012). Associations between race/ethnicity have proven inconclusive, with different racial/ethnic groups being identified as being at greater MSI risk in different studies (Sammito et al., 2021). Additionally, in their recent review, Sammito and colleagues (2021) found insufficient evidence to determine whether marital status is a risk factor for MSI.
Psychological correlates of musculoskeletal injury risk
The association between psychological factors and MSI risk has been studied across many different civilian populations. A positive association has been found between MSI and psychological factors amongst construction workers, teachers, athletes, and hospital patient care workers (Goldenhar et al., 2003; Ng et al., 2019; Reme et al., 2014; Sobeih et al., 2006). Some of the psychological factors that have been linked to MSI risk in these populations include job satisfaction, perceived job stress, job demands, job certainty, and supervisor support. Recent research examining the effects of dispositional optimism in athletes, for example, found that high levels of optimism were associated with a decreased likelihood of injury over a two-year follow-up period (Wadey et al., 2013). Additionally, both worry and negative life-event stress were positively associated with time to first injury. This suggests that those with more worry and negative life-event stress remained injury-free for a longer time, possibly as a result of engaging in fewer aggressive and risk-taking behaviors (Sibold and Zizzi, 2012). Greater negative life event stress among collegiate athletes has also been linked to greater numbers of musculoskeletal injuries (Anderson and Williams, 1999). The ability to cope with life’s challenges has also been linked to injury risk. A study of professional soccer players, for example, found that a lower ability to cope with adversity was predictive of injury occurrence (Devantier, 2011). Greater coping skills have also been associated with better injury recovery (Fernandes et al., 2014).
While well established in civilian populations, studies examining the association between psychological factors and MSI in the military have proven far more elusive (Sammito et al., 2021). Roy et al. (2016) explored various risk factors for MSI in a sample of 160 deployed female Soldiers but did not observe a statistically significant association between the psychosocial factors examined (sleep, coping, and work stress) and MSI risk. A more recent study of 2275 U.S. Army trainees, however, found that high scores on grit and positive hardiness at baseline were associated with a 20–30% lower odds of reporting an injury during training (Heaton et al., 2022).
The present study
Musculoskeletal injuries represent a significant health problem for the Army. Reducing the incidence of both combat and non-combat injuries, and finding novel ways to mitigate the associated costs, represent major objectives of current Army medical strategic thinking (Army Medical Department Civilian Corps, 2017; Nindl et al., 2013; Reivich et al., 2011). Toward this end, the present study has two goals: (1) Leverage existing Army data to test the association between baseline psychological factors and subsequent MSI risk in a large sample of active duty Army Soldiers. Although numerous studies have examined this association in civilian samples, very few studies have examined this association in a military context. We hypothesize that the association between greater positive psychological strengths and lower MSI risk routinely observed in civilian samples will also be observed among active duty Army Soldiers. Psychologically strong Soldiers, for instance, those with strong coping skills, the ability to adapt to changing circumstances, who hold positive expectations for the future and who generally feel positive emotions, may have a reduced risk of injury, compared to Soldiers absent these qualities. If the linkage between psychological strengths and injury risk is robust and the psychological strengths identified as protective factors are modifiable, boosting Soldiers’ psychological strengths has the potential to also help preserve the fitness of the force. (2) Leverage the very large sample size in this study to enhance our understanding of physiological and social MSI risk factors in the military. We hypothesize that given sufficient statistical power, we will be able to identify risk factors with small, but reliable, effects.
The present study leveraged existing data in the Person-Event Data Environment (PDE), a secure virtual data repository and analysis environment (Vie et al., 2013, 2015). Based on the established associations between psychological strengths and injury risk, we selected four Global Assessment Tool (GAT) scales for inclusion in this study (i.e., coping, adaptability, optimism, and positive affect). Together, we define these constructs as “psychological strengths”. Coping and adaptability were selected because they are tools individuals use to process and deal with stressors. Additionally, both optimism (holding positive expectations for the future) and current positive emotions (positive affect) were selected to capture Soldiers’ subjective well-being in the context of a stressful and physically demanding occupation. Given that the extant literature suggests most MSIs sustained by Soldiers are non-combat related, the present study focused on MSIs occurring outside of combat situations.
The project was reviewed and approved by the Army Human Research Protections Office and determined to be research not involving human subjects. Per U.S. Army policy and regulations, individual de-identified participant data may not be extracted from the secure PDE analysis environment. Vetted researchers working on DoD-funded projects can, however, access the data used in this study in the PDE.
Participants
The present study examined active duty Army Soldiers who completed a GAT in 2010, the first full year that the GAT was administered. We limited the study to Soldiers ages 17-54 who had joined the Army in the year leading up to their GAT, to limit the variation in overexertion and Army training that participants would bring into the study. We also excluded Soldiers with a primary MSI diagnosis before their baseline GAT, so that we could capture new MSIs, rather than the recurrence of an existing injury. Finally, this study was limited to participants who indicated through an electronic “opt-in” procedure that their GAT responses could be used for research purposes. These inclusion criteria resulted in an analytic sample of 24,746 active duty Army Soldiers.
Measures
The GAT (later revised and renamed the Azimuth Check) is a psychological strengths inventory that Soldiers complete annually (Peterson et al., 2011). Four GAT scales were examined in this study, and responses from within each GAT scale were averaged. Higher scale scores indicated higher levels of the specified psychological strength.
Optimism
Optimism was measured using four items adapted from the revised Life Orientation Test (Scheier and Carver, 1985; Scheier et al., 1994). A sample item includes, “In uncertain times, I usually expect the best.” Item responses could range from strongly disagree (1) to strongly agree (5). Cronbach’s α for this scale was 0.69.
Coping
Five items adapted from the Brief COPE assessed problem-focused coping skills, such as planning or taking direct action, positive reframing, and acceptance (Carver, 1997; Carver et al., 1989). A sample item includes, “When something stresses me out, I try to solve the problem.” Item responses ranged from “Not like me at all” (1) to “Very much like me” (5). Cronbach’s α for this scale was 0.71.
Adaptability
Three items written specifically for the GAT assessed adaptability. Items include “I am good at changing myself to adjust to changes in my life,” “It is difficult for me to adjust to changes” (reverse scored), and “I can usually fit myself into any situation.” Item responses ranged from “Not like me at all” (1) to “Very much like me” (5). Cronbach’s α for this scale was 0.74.
Positive affect
Nine items adapted from the Positive and Negative Affect Schedule Expanded Form (PANAS-X; Watson and Clark, 1994) assessed general positive affect such as joviality (e.g., “happy”), self-assurance (e.g., “proud”), and serenity (i.e., “calm”). A tenth item assessing “love” was removed during a revision to the GAT and excluded from the present analyses. Cronbach’s α for this scale was 0.91.
Physiological and social factors
Physiological and social factors were obtained from electronic administrative records maintained by the Defense Manpower Data Center (DMDC). Physiological factors included gender (male vs female), age (years), and BMI. BMI was calculated based on the height (inches) and weight (pounds) data obtained from the Medical Data Repository (MDR), the Periodic Health Assessment, or the Digital Training Management System Army Physical Fitness Test (APFT). We removed values that were more than three standard deviations above or below the sample mean height or weight (i.e., outliers). Social factors included race/ethnicity (White vs other), educational attainment (high school diploma or lower vs more than high school diploma; HSD), marital status (married vs not currently married), and rank (enlisted vs officer).
Musculoskeletal injury
Data on MSI were obtained from military electronic health records compiled in the Military Health System MDR. The MDR records all outpatient and inpatient medical encounters and medications dispensed to Soldiers and reimbursed by TRICARE, the military health insurer. We included data on MSI encounters treated at military treatment facilities (MTFs) and non-military facilities, if reimbursed by TRICARE. Musculoskeletal injury cases were identified according to whether a Soldier received a primary diagnosis of musculoskeletal injury following their latest GAT and before the end of 2012. MSI cases were identified using the International Classification of Diseases, Ninth-Revision, Clinical Modification (ICD-9-CM; ICD.Codes, 2015) codes identified by Hauret et al. (2010).
Statistical analyses
Statistical analyses were conducted using SAS Enterprise Guide 7.12. Cox proportional-hazards models estimated the hazard ratios (HR) and 95% confidence intervals (CIs) for associations between baseline psychological strengths (i.e., Optimism, Coping, Adaptability, and Positive Affect) and incident musculoskeletal injury. We followed Soldiers until one of the following events occurred: first diagnosis of musculoskeletal injury, separation from Army service, or the end of follow up (a fixed censoring date of December 31, 2012). All models were adjusted for physiological factors (gender, age, and BMI), as well as social factors (race/ethnicity, education, marital status, and rank).
The assumption of proportional hazards was tested by examining the Martingale residuals and functions of time in the primary model. Examination of the residuals indicated that the data did not support the Cox proportional hazards assumption. A violation of this assumption suggests that the strength of the relation between our primary predictor variables (Optimism, Coping, Adaptability, and Positive Affect) and MSI could vary over time. A solution to this assumption violation involves adding an interaction effect between time and the primary predictor variable of interest in each model (Allison, 2010).
Results
Physiological and social factors of Soldiers who experienced an MSI compared to those without an MSI (2010).

Predicting incident Musculoskeletal Injury Risk
Over a mean follow-up period of 21.07 months (SD = 16.07), 65.42% of Soldiers (16,188 out of 24,746) were treated for an MSI. The vast majority of MSI’s in this study were caused by inflammation and pain (97.21%). The remaining MSI’s were caused by joint derangement (1.33%), joint derangement with neurological involvement (0.93%), sprain, strain or rupture (0.28%), dislocation (0.15%) or stress fracture (0.10%). Over half of the MSI’s (56.97%) afflicted lower extremities, nearly a quarter (24.10%) afflicted the vertebral column, 16.18% afflicted upper extremities, and 2.76% of MSI body regions were unclassified.
Demographic-adjusted Hazard Ratios of Optimism and incident MSI.

Demographic-adjusted Hazard Ratios of Positive Affect and incident MSI.

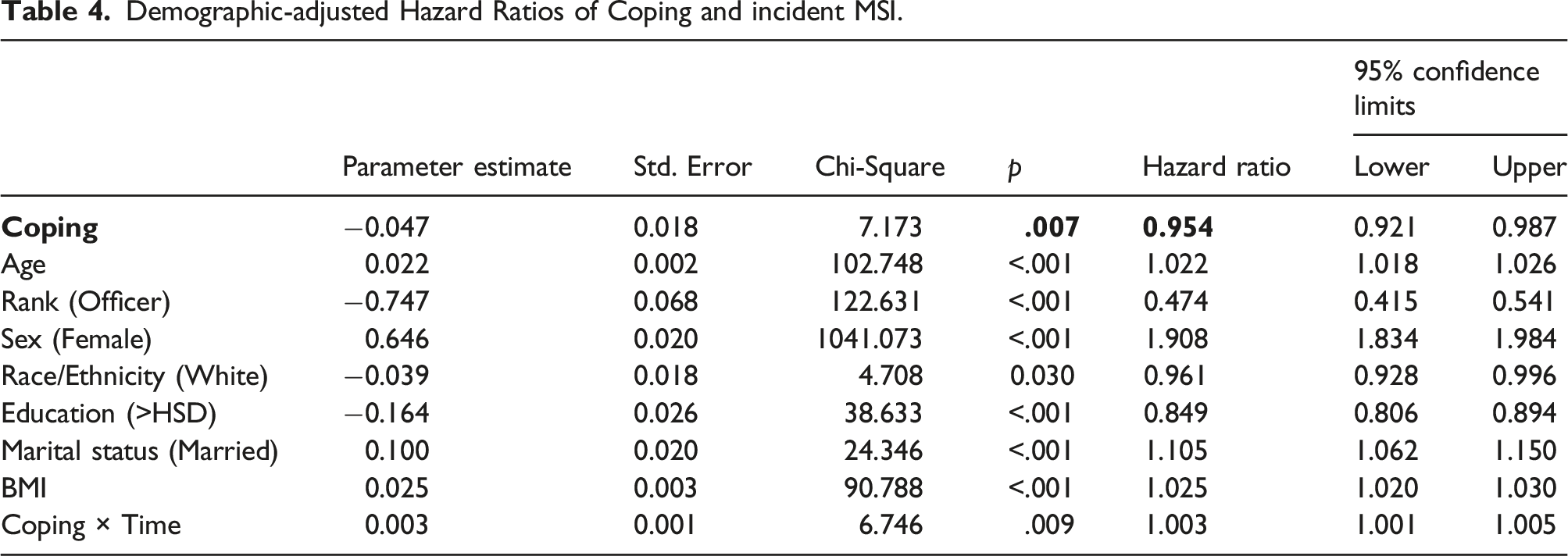
Demographic-adjusted Hazard Ratios of Coping and incident MSI.
Demographic-adjusted Hazard Ratios of Adaptability and incident MSI.

Bold indicates the independent/primary predictor variable in each model.
The association between the physiological and social factors and MSI incidence was also examined (Tables 2–5). MSI incidence risk was higher among female Soldiers (relative to male Soldiers; HR: 1.908-1.914) and among married Soldiers (relative to Soldiers who were not married; HR: 1.104-1.108). Age and BMI were also associated with an increased risk of MSI (HR: 1.022-1.023 and HR: 1.025, respectively). In contrast, MSI incidence risk was lower among officers (relative to enlisted Soldiers; HR: 0.474-0.478) and among Soldiers with more than a high school education (relative to those with a high school degree or less; HR: 0.848-0.852).
Discussion
The present study examined the association between psychological strengths and subsequent MSI risk in a large sample of active duty Army Soldiers. An examination of four baseline psychological strengths measures (Optimism, Positive Affect, Coping, and Adaptability), modeled separately, revealed significant associations with MSI risk during follow up. Specifically, Soldiers with high baseline levels of Optimism, Positive Affect, Adaptability, or Coping were at a modest decreased risk of musculoskeletal injury over time (each measure resulted in an approximately 4-8% risk reduction). These findings add to the growing body of literature that suggests that psychological constructs, such as Optimism, Positive Affect, and Coping, are positive or protective health factors (Pressman and Cohen, 2005; Scheier and Carver, 1985; Segerstrom, 2007; Seligman, 2008; Steptoe et al., 2009). The idea that psychological strengths may impact the risk of injury or physical health is in alignment with the biopsychosocial model of health and disease. Furthermore, these findings could hold practical significance as a basis for psychosocial intervention as a growing number of studies point to the idea that psychological interventions focused on improving psychological well-being can result in physical health benefits (Paddon and Kampman, 2023).
The current findings extend our understanding of the association between psychological factors and MSI in two important ways. First, this study replicates the association in a sample of over 24,000 active duty Army Soldiers who were free of an MSI diagnosis at baseline. Second, this study adds Optimism, Positive Affect, Coping, and Adaptability to list of psychological factors that may relate to MSI risk.
The effect of psychological variables on objective physical health outcomes tends to be modest (Boehm et al., 2018; Rasmussen et al., 2009), so the observed risk reduction between 4% and 8% per unit increase in Optimism, Positive Affect, Adaptability, and Coping is reasonable. Results from the current study suggest that a psychologically-based intervention strategy for MSI prevention could potentially play an impactful role in preventing MSI among active duty Army Soldiers. If an intervention targeting enhancing positive psychological strengths were successful, our findings suggest that a reduction in the incident number of MSIs could potentially be seen. Given the high incidence rate of MSI in the military (Molloy et al., 2020), even a 4–8% reduction in incident MSI rates could have an important, real-world impact. Importantly, the Soldiers in the current sample were not given any formal intervention targeted at increasing psychological strengths as part of this study. If, for example, an intervention was able to increase Soldiers’ scores on the Optimism measure by two units, those Soldiers would then have a 17% reduction in MSI risk according to the current findings (assuming a causal relation between Optimism and incident MSI).
Additionally, this study identified several physiological and social risk factors. Consistent with the literature, age and sex (being female) were identified as non-modifiable risk factors (see Sammito et al., 2021 for a review). Although there is mixed evidence for continuous measures of BMI as a risk factor for MSI, a modest risk was observed in this study. Based on recent findings (Sammito et al., 2021), we recommend future studies classify participants as overweight, healthy weight, and underweight, rather than examine BMI as a continuous measure, to more precisely capture any association between BMI and MSI risk. This study also provides additional evidence that lower education and lower rank are risk factors for MSI. We recommend future studies continue to further examine these associations.
In addition, although there is mixed evidence in the literature regarding marital status as a risk factor for MSI, this study found that being married was associated with an increased MSI risk. This finding is consistent with another large study of active duty Army Soldiers study (n = 83,323; Hill et al., 2013), which identified being married as a risk factor for soft tissue knee injuries. It may be that married Soldiers are more likely to receive encouragement to seek treatment for a possible MSI than unmarried Soldiers. Many of the studies that have examined the association between marital status and MSI risk in the military may have lacked the statistical power to reliably measure a small effect size. We recommend that power analyses be performed in future studies examining the association between marital status and MSI risk in the military.
Although race/ethnicity has been identified as a risk factor for MSI, there are inconsistencies regarding which groups are considered at elevated risk (Sammito et al., 2021). Considering these inconsistencies and the very modest association observed in this study, more research is needed to better understand whether any race/ethnicity groups are at greater risk of developing an MSI.
Study limitations
Although examination of medical records is both cost- and time-efficient, previously collected data also come with a unique set of challenges. For example, we limited our focus to the ICD-9 codes associated with the Soldier’s chief complaint (i.e., the problem or concern that prompted the Soldier to seek medical attention); in this way, we hoped to identify the primary reason for each medical encounter. It is possible, however, that Soldiers could have been seen for two or more related reasons, and we might have failed to capture the MSI if the diagnosis was listed second or later. Excluding non-primary MSI diagnoses could have also affected the descriptive statistics regarding MSI body region and type in our sample. In addition, because we only had access to medical care reimbursed through Tricare, we excluded Reserve and National Guard Soldiers, who tend to receive coverage through private health insurance. The reliance on existing secondary data also necessitated the analysis of shortened versions of psychological measures, rather than the fuller, more reliable versions of the instruments. Additionally, because of the lack of variation in the causes of MSI in this study (97.2% were caused by inflammation and pain), we were unable to conduct sensitivity analyses to test the association between psychological strengths and MSIs based on different causes, as we originally intended.
Future directions and conclusions
The results from this study reinforce that MSI is a common occurrence among Army Soldiers (65% of the sample developed an MSI during the study follow-up window), and because of this, MSI is a threat to the health and readiness of our force. The current findings also demonstrate that certain psychological strengths are related to a reduced risk of MSI. This raises the question of whether a psychological strengths-based intervention strategy could be effective in MSI prevention. A recent review of positive psychology interventions to improve physical health and psychological wellbeing in police staff provides theoretical support to the notion that a psychological strengths-based intervention to reduce MSI risk may be effective for Soldiers (Kukucska et al., 2023). Additionally, more research is needed to investigate how these psychological strengths may relate to MSI in Reserve and National Guard Soldiers, as well as in the general population. Although it is premature to recommend a psychological strengths-based strategy in MSI prevention, additional research in this area is warranted. Data related to Army Resilience Directorate initiatives to increase Soldier readiness and resilience, combined with the current MSI-encounter data, might provide insight as to whether a psychological strengths-based intervention could be effective in reducing MSI in Soldiers.
The current study provides a foundation for continued research to better understand the relationship between Optimism, Coping, Adaptability, and Positive Affect and musculoskeletal injuries. Future studies could expand the current investigation to include type, severity, and body region of MSI, while examining the impact of additional factors (e.g., physical activity level) on the relation between MSI and psychological factors. Examining whether psychological factors are related to the development or prevention of chronic MSI in Army Soldiers would also add to the scientific literature. Future research protocols should be designed with an eye towards development and testing of psychosocial interventions for reducing the risk of MSI in the Army and the general civilian population.
By leveraging existing data in the PDE to analyze a large sample of active duty Army Soldiers, the current study was able to link baseline psychological strengths to a modest reduction in non-combat-related MSI risk (4-8%) and reinforce and extend what is known regarding physiological and social MSI risk factors in the military. Future research should examine the extent to which interventions designed to increase Optimism, Positive Affect, Coping, and Adaptability can also be effective at reducing Soldiers’ MSI risk, which could improve the readiness of our troops and reduce the Army’s MSI-related health care costs.
Footnotes
Acknowledgments
We thank Dr Doug Bonett (University of California, Santa Cruz) for statistical guidance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Army Studies Program Management Office [funding number HHSN316201200036W_HHSP233201400190W].
Ethical statement
Disclaimer
The U.S. Department of Defense does not exercise any editorial, security, or other control over the information in this article. The authors assume responsibility for the veracity, accuracy, and source documentation of the material, including no use of classified material and conformity to copyright and usage permissions. The views expressed in this article are those of the authors and do not necessarily represent the official policy of the Department of the Army, Department of Defense, or the U.S. government.