
Abstract
This study examined the cardiovascular disease (CVD) risk profiles of male law enforcement officers (LEOs) and civilians. CVD risk profiles were based on data collected using traditional objective (e.g., resting BP, cholesterol), novel objective (e.g., ambulatory BP) and self-report measures (e.g., EMA social vigilance). A subset of male LEOs (n = 30, M age = 41.47, SD = 8.03) and male civilians (n = 120, M age = 40.73, SD = 13.52) from a larger study were included in analyses. Results indicated LEOs had significantly higher body mass index [BMI], 31.17 kg/m2 versus 28.87 kg/m2, and exhibited significantly higher trait and state social vigilance across multiple measures, whereas perceived stress was higher among civilians. Findings highlight the need for future research examining CVD risk associated with occupational health disparities, including attributes of individuals entering certain professions as well as experiential and environmental demands of the work.
Keywords
Introduction
In the United States [US], cardiovascular disease (CVD) was responsible for approximately 928,741 deaths in 2020 (Tsao et al., 2023), making it the leading cause of death among men and women. Although CVD mortality rates have declined somewhat since peaking in 1968, the prevalence of key CVD risk factors such as obesity (CDC, 2021), hypertension (Dorans et al., 2018), and type II diabetes (Bhupathiraju and Hu, 2016) have continued to rise. Recently, additional risk factors have been identified including elevated levels of inflammation (Held et al., 2017; Ridker, 2016).
Law enforcement officers (LEOs) as an occupational group in the US, compared with the general population, experience higher rates of CVD morbidity and mortality (Franke et al., 1998; Hartley et al., 2011; Violanti et al., 2017, 2021; Zimmerman, 2014). Some work has suggested that the increased mortality among LEOs is as a result of high prevalence in CVD risk factors such as obesity, metabolic syndrome, shorter sleep (<6 h), hypercholesterolemia, and tobacco use (Franke et al., 2002; Hartley et al., 2011; Violanti et al., 2021; Zimmerman, 2012). Yet, these risk factors for CVD are observed at high levels in the general population, consequently making it unclear to what degree, or on what risk factors, LEOs may be distinct from the general population of the US.
Psychosocial factors contributors to cardiovascular disease
LEOs belong to a distinct occupational population in which their sworn duties may expose them to potentially traumatic and life-threatening situations. Occupational exposure to violent events, in combination with organizational factors (e.g., high demand/low control, shift work, increasing societal and cultural pressure), has the potential to result in increased exposure to psychosocial stressors. If police work leads to frequent and/or persistent exposure to stressors, this in turn may result in prolonged activation of physiological systems that respond to such events, and result in homeostatic disturbances (e.g., Smyth et al., 2013). Additionally, prospective work has found that the severity in which an individual perceives or experiences social stress is associated with accelerated progression of atherosclerosis and adverse cardiac events (Mathur et al., 2016; Yao et al., 2019).
Many factors that exacerbate perceived stress have been identified, including shift work, the possibility of witnessing and/or experiencing violent events, increasing cultural and societal pressure, and organizational pressure (e.g., lack of supervisor and coworker support, insufficient manpower, job insecurity, insufficient pay and excessive paperwork; Hartley et al., 2011; Poirier et al., 2023). Additionally, factors influencing how one interacts with the environment may also be present. Vigilance for social threats may be particularly common especially for caregivers, military, and LEOs who are charged with the safety of others. Prior research has shown that vigilance for non-social (dot-probe tasks, mirror tracing, Stroop tasks) and social stimuli (watching potential debate partners, social observation) evokes heightened cardiovascular reactivity including sustained increases in blood pressure that are hypothesized to increase CVD risk (Smith et al., 2000). Given their occupational demands, levels of vigilance would presumably be high among LEOs; therefore, this may result in more frequent and/or higher levels of stress. Health consequences significantly associated with persistently elevated levels of stress symptoms include anxiety, depression, burnout, chronic back pain, alcohol abuse, and hypertension (Gershon et al., 2002; Sara et al., 2018).
Seeking to expand upon previous work, the aim of this paper was to evaluate the cardiovascular risk profiles of male LEOs and civilians, comparing traditional and novel objective and self-reported CVD risk factors. For comparison, risk profiles are established using demographic, cardiometabolic, psychosocial stress, ecological momentary assessment (EMA), and ambulatory measures.
Methods
Participants
This paper presents a secondary analysis of data from the North Texas Heart study (see Ruiz et al., 2017), which was an investigation of atherosclerotic risk among a community sample. The Institutional Review Board at the study coordinating institute approved this study. The complete North Texas Heart sample was made up of 300 adults ages 21 to 70 years. Participants were eligible if they were (1) 21+ years of age, (2) residing within Denton County, Texas, and (3) had written and verbal fluency in English. Community members were excluded if they possessed any of the following: (1) cognitive impairment (i.e., dementia), (2) previous history of myocardial infarction or tertiary cardiac interventions (e.g., coronary artery bypass surgery, implanted cardiac defibrillator), (3) pregnancy within last year or anticipating pregnancy during study period, or (4) night shift worker. Ineligibility based on shift work at night may bias the LEO sample by excluding officers who work within the departmental patrol division (uniformed officers working in designated areas). These divisions are staffed 24-h a day and are responsible for most departmental police services.
For this report, the term ‘law enforcement officer’ was operationalized using the definition provided by U.S. Code, Title five in which a law enforcement officer is “An employee, the duties of whose position— (i) are primarily— (I) the investigation, apprehension, or detention of individuals suspected or convicted of offenses against the criminal laws of the United States, or (II) the protection of officials of the United States against threats to personal safety” (2001).
Occupational justification for categorization.

Data collection procedures
Participants screened and found eligible to participate were scheduled for an in-person clinic visit. At their scheduled appointment time, participants met with the study coordinator at the clinic to provide written, informed consent.
Demographic measures
Self-reported demographic information was collected from participants. Information included gender, race, ethnicity, marital status, household income, and educational attainment.
Cardiometabolic measures
Cardiometabolic risk factors within the current study included: body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), high density lipoprotein (HDL), low density lipoprotein (LDL), fasting glucose, triglycerides, high-sensitivity c-reactive protein (CRP), and interleukin 6 (IL 6).
Following consent procedures, participants underwent a brief physical exam and interview with a study nurse. During the interview, participants’ current medications and health conditions, health behaviors, and a detailed cardiac disease history were collected. A phlebotomist performed a fasting (8 h) blood draw to assess inflammatory markers and a complete lipid profile. While at the laboratory session, participants underwent a physical exam that included anthropomorphic measures and three measures of resting BP, which were averaged to determine a baseline clinical measure of blood pressure (Ruiz et al., 2017).
Psychosocial stress measures
A self-report questionnaire package was completed by participants to collect data within four interrelated domains of psychosocial risk. Information used in this analysis focused on data collected within the psychosocial stress domain. This analysis used the following measures.
Social vigilance questionnaire (SVQ)
The SVQ measure is designed to measure the frequency of vigilant behaviors within social contexts using a range of 1 (almost never) to 5 (almost always). The scale includes 16-items, 10 of which are used for scoring purposes. Confirmatory factor analysis (CFA; Ruiz et al., 2017) validated a 3-factor solution: (1) Vigilance for social threats (4-items), (2) vigilance of others’ reactions to self (3-items), and (3) vigilance of self (3-items). A total score (average of 10-items) was also derived. Within the full NTHS sample, the full-scale measure and independent subscales demonstrated good internal consistency; vigilance for social threats (Cronbach’s alpha = .81), vigilance of others’ reactions to self (Cronbach’s alpha = .81), and vigilance of self (Cronbach’s alpha = .81), and overall (Cronbach’s alpha = .84).
Perceived stress (PSS)
The 10-item PSS (Cohen et al., 1983) scale evaluates an individual’s perceptions of the frequency of stressful events within the previous 30 days, using a frequency range of 0 (never) to 4 (very often). Specific items are reverse coded. All items are averaged to generate a total perceived stress score. The measure had good internal consistency (Cronbach’s alpha = .88) within the complete NTHS sample.
Job content (JCQ)
The Job Content Questionnaire (Karasek et al., 1998) is an instrument used to evaluate psychological dimensions of job environments. The measure includes assessments of both job demand and control characteristics. For the NTHS, methods presented by Schwartz et al. (1988) were used to measure job strain; a construct reflective of a combination of demand and content. For a complete explanation of methods utilized to measure job content see Ruiz et al. (2017). The measure includes 11 items from the JCQ including items like “my job requires a high level of skill” and employed a four-point Likert scale from 1 (strongly disagree) to 4 (strongly agree). The measure scales had good internal consistency (Job Control (averaged) Cronbach’s alpha = .65; Job Demand (averaged) Cronbach’s alpha = .69) within the complete NTHS sample.
Ecological momentary assessment (EMA) and ambulatory data
While attending the laboratory visit, participants were provided with an ambulatory blood pressure monitor (ABPM: Oscar II; Suntech, Inc.) and a cellular phone for the 2-days and 1-night ambulatory/ecological momentary assessment (EMA) study. Blood pressure was measured at semi-random times at approximately 45-min intervals throughout the waking day. This sampling was done to prevent participants from anticipating a measurement and altering their activity as a result (see Ruiz et al., 2017). Participants were instructed to complete the EMA survey immediately following each blood pressure assessment throughout the day. This approach allowed for synchronizing the EMA record to the BP record throughout the ambulatory data capture period. Administration of the Social Vigilance Questionnaire was contingent on the participant reporting having spent time in a social context within the measurement window.
Data analysis plan
Statistical analysis was conducted using the SAS software, version 9.4 (SAS Institute, Cary, NC). Upon confirmation of occupational groupings, descriptive statistics including means (standard deviation) and frequency were calculated for demographics to characterize the study population, both in its entirety and based on occupation. When analyzing group differences, the cardiometabolic, psychosocial, and ambulatory daily experience variable models were run separately. The homogeneity of variance was assessed in each model using Levene’s test for equality of variances. Models found to violate the assumption were evaluated using the Welsh’s adjusted F ratio. Covariates included in each model can be found in respective tables. A p-value of <0.05 was considered statistically significant.
Results
Group differences
Demographic variables
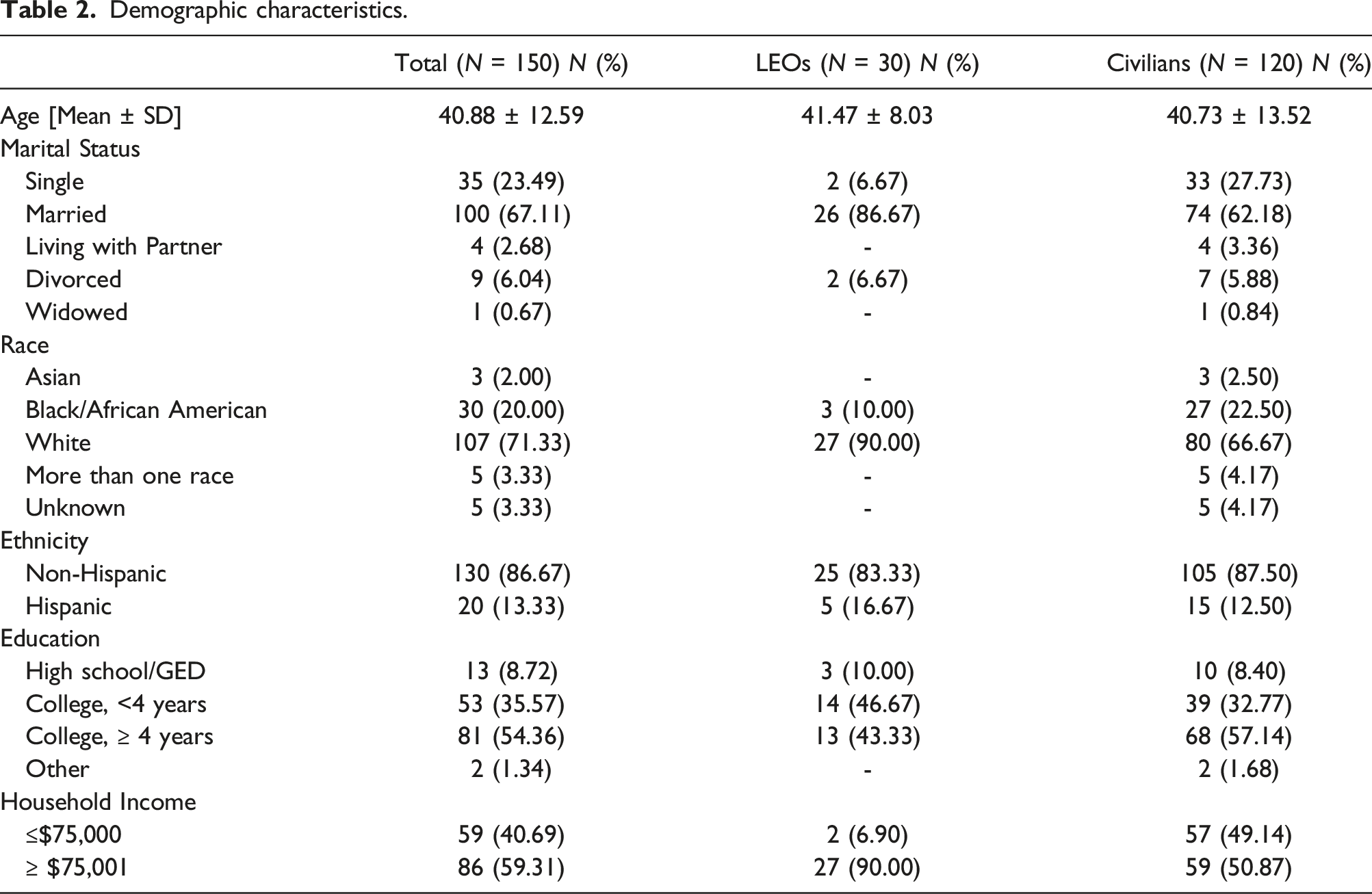
Demographic characteristics.
Cardiometabolic variables
Cardiometabolic variables.

Note. M = mean, SE = standard error of the mean; models control for body mass index [BMI].
aIndicates assumption of variance homogeneity was met.
Psychosocial stress variables
Baseline psychosocial characteristics.

aIndicates assumption of variance homogeneity was met.
bIndicates Welch’s adjusted F ratio.
Groups also differed significantly in perceived stress. Unexpectedly, perceived stress was significantly higher among the civilian group (F (1, 149) = 7.62, p = .01, r2 = 0.05). Based on scale range, scores among both groups indicated moderate mean levels of stress (LEOs = 2.12 vs civilians = 2.47). The assumption of variance homogeneity between groups was met for perceived stress (p > 0.05). Job strain, an assessment of psychological dimensions of a job environment related to increased CVD risk, did not differ significantly between groups.
EMA and ambulatory assessment variables
Ambulatory and daily experience variables.

Note. M = mean, SD = standard deviation, SE = standard error of the mean; Blood pressure models control for body mass index [BMI].
aRepresents adjusted values after controlling for body mass index [BMI].
bIndicates assumption of variance homogeneity was met.
cIndicates Welch’s adjusted F ratio.
Discussion
Previous research generally documents higher prevalence of CVD and higher rates of CVD mortality in LEOs relative to civilians at a broad level, although factors contributing to this divergence are less clear. In this study, potential contributors to these disparities were explored, encompassing measures based on baseline demographics and traditional self-report scales. More importantly, the present study is novel in the incorporation of inflammatory biomarkers, ambulatory monitoring of blood pressure and daily experiences, and the implementation of a social vigilance measure, gathered both at baseline and during ambulatory assessments.
When comparing groups, demographic information identified several differences. Racial diversity was more limited within the LEO group when compared to the civilian group. Only 10% of officers identified as non-White, whereas 25% of individuals in the civilian group identified as Asian or Black and 4% identified as more than one race. The difference in racial diversity is consistent with existing literature indicating that White non-Hispanics make up 69% of US LEOs (Goodison, 2022), however this sample of LEOs remains less racially diverse than US law enforcement population. To ensure the recruitment of a representative sample in future research, recommendations made by Cunningham-Erves and colleagues (2022) emphasize the development of tailored research recruitment materials for African American and Latino populations. Recommendations include establishing relationships within communities and being physically present, placing recruitment materials in accessible areas (e.g., community social media pages, bulletin boards in parks, libraries, barber shops, churches, stores in Latino communities), and personalizing recruitment to address the beliefs and values of a specific group are achievable and cost-effective. Further, a significant difference was observed in household income between LEOs and civilians; the vast majority (90%) of LEOs reported a household income >$75,001, relative to civilians, of whom 50% reported a household income <$75,000. Given the association between lower household income and adverse health behaviors, outcomes, and health care (Dubay and Lebrun, 2012), it seems unlikely that household income is a prominent contributor to the divergence in CVD risk between groups in the current sample (i.e., the higher income of LEOs should be associated with better outcomes). Previous research suggests the prevalence of disease among adults with a lower income to poverty ratio is significantly greater than adults a higher ratio (Minhas et al., 2023). For example, the percentage of adults with coronary heart disease (CHD) among those with annual family incomes ranging from <$35,000 - $74,999 is 20.9%, whereas 10.2% of adults with family incomes >$75,000 have CHD (Schiller et al., 2012).
When comparing risk profiles based on cardiometabolic factors, the prevalence of overweight and obesity was significantly higher among LEOs; 88% of LEOs met the criteria for being classified as overweight or obese, compared to 68% of civilians. Moreover, this difference was particularly evident among those classified as obese. Previous work indicates that high rates of sedentary time and physical inactivity, in addition to poor dietary habits, are significant contributors to the prevalence of obesity among LEOs (Hartley et al., 2011; Lockie et al., 2022; Violanti et al., 2017). Although there are tests available for evaluating officer fitness or occupational readiness, there is no universally accepted standard (for testing or requirements), leaving individual departments to determine their own standards (Dicks et al., 2023).
During medical history reviews, groups had a similar percentage of participants who reported being informed they had high blood pressure, and groups had relatively equal numbers of participants who met criteria for hypertension (LEOs = 56.66% and civilians = 55.04%). Mean values of systolic and diastolic blood pressure, after controlling for body mass index, were only slightly higher among LEOs, a difference found not to be statistically significant. Similar levels of HDL and LDL were found between groups, and these levels were within the normal value range (Arnett et al., 2019; Unger et al., 2020). Biomarkers examined in this study included IL-6 and CRP. IL-6 is an upstream inflammatory cytokine known to contribute to the initiation, and progression, of atherosclerosis (Hartman and Frishman, 2014). CRP, a protein produced by the liver, is induced by the IL-6 action during the acute phase of an inflammatory process (Nehring et al., 2023). Groups were found to differ significantly in mean values of IL-6; however, these levels were well within the normal value range (Said et al., 2021). Although groups did not differ significantly, the mean value of CRP among LEOs (M = 0.46) can be classified as ‘minorly elevated’; an elevation often seen in obesity, whereas the mean value within the civilian group (M = 0.30) is classified as ‘normal’ (Nehring et al., 2023). These results thus did not provide evidence that proinflammatory biomarkers reflect a substantial contributor to greater adverse cardiovascular risk often observed among LEOs, including increased rates of metabolic syndrome, obesity, and hypertension (Franke et al., 2002; Hartley et al., 2011; Ramey et al., 2014; Violanti et al., 2013, 2021; Wright et al., 2011). Thus, this finding from the current study is inconsistent with prior work; rather, we find that there are broadly similar CVD risk profiles when comparing cardiometabolic risk variables (other than BMI).
When comparing psychosocial factors within the current sample, traditional measures of stress (e.g., perceived stress, job control, job demand) seem to be unlikely contributors to CVD risk among LEOs. Instead, findings suggest LEOs have lower perceived stress and higher occupational control (Garbarino and Magnavita, 2015; Kivimäki et al., 2002), which should be associated with better cardiovascular health outcomes. In this particular study, perceived stress was measured using the PSS; a scale that broadly assesses the degree to which situations in one’s life are appraised as subjectively stressful (notably, the PSS does not specifically assess occupational stress). That LEOs report experiencing lower perceived stress may be indicative of the balance between exposure to potential stressors and individual’s perceptions of their capacity to adapt (Lazarus and Folkman, 1984). In particular, LEOs are subjected to occupational training that may be beneficial in the secondary appraisal of stressful situations (e.g., lethal force scenario response training; Baldwin et al., 2022). More specifically, the evaluation of one’s coping resources and options to deal with the stressor (e.g., perceived control) identified in the appraisal process (Lazarus and Folkman, 1984). Work with LEOs to further develop coping resources (e.g., strengthen resilience) is on-going and has been suggested as a promising approach to addressing the underlying physiological mechanisms (Anderson et al., 2023).
The clearest divergence in psychosocial risk profiles was in social vigilance. Scores for all vigilance subscales (except ‘others’ reactions to self’) were significantly higher among LEOs for both baseline and EMA data. The lack of significant difference between groups on the ‘others’ reactions to self’ domain may be reflective of interpersonal power dynamics experienced by LEOs. To our knowledge this is the first use of the social vigilance questionnaire among LEOs and this interpretation is therefore speculative and requires future research to better understand the role of different types of social vigilance in LEOs.
The act of being vigilant involves continuously monitoring an environment for threat; it is possible that occupational training and responsibilities experienced by LEOs may entrain and/or elicit higher rates of vigilance. Although the behavior may be automatic, continuous exposure can lead to heightened cardiovascular reactivity and prolonged activation of physiological systems resulting in homeostatic disturbances (O’Neill, 2022). In addition to health conditions associated with homeostatic disturbance (e.g., diabetes), previous research suggests vascular resistance is a potential byproduct of vigilant behaviors that may manifest as increases in blood pressure, and total peripheral resistance, representing a CVD risk (Panaite et al., 2015; Smith et al., 2000).
Results from the current study also extend those of previous research by incorporating measures of ambulatory blood pressure. Contrary to expectations, ambulatory blood pressure did not significantly differ between groups when controlling for BMI. Nonetheless, the approach provides further evidence for the potential of wearable sensors to assess key health indicators among tactical and first response populations. As wearable sensors (e.g., heart rate monitors) and location tracking technology (e.g., GPS) become more accessible and affordable, researchers are better equipped to capture real time data regarding individual responses to stressors by measuring variables such as stress reactivity and changes in on-shift heart rate. Information collected through these methods could help inform workplace interventions that target key behaviors to improve health outcomes and reduce occupational health disparities within LEOs and other first response groups. For example, work conducted by Andersen et al. (2018) found that a physiologically informed intervention, teaching officers to modulate SNS and PNS activation during scenario-based training, significantly reduced objective errors in lethal force decision-making, and results were maintained over the 18-months study period.
Limitations
The current analysis has several limitations. Foremost, the small sample size of the LEO group reduces statistical power, therefore reducing the ability to detect smaller differences between groups. In addition, the small sample size precluded stratifying the LEO group according to specific work-related exposure that may impact health outcomes (e.g., years of service, departmental rank, shift worked, patrol status, etc.) The current study also utilized a convenience sample that was not representative of the U.S. law enforcement population. As there were no females in the LEO group, we were not able to compare CVD risk profiles between female LEO officers and civilians; this may be important given the association between sex and cardiovascular disease risk indicators (Humphries et al., 2017). Furthermore, the lack of racial diversity among the LEO group (90% White, relative to national average estimated to be 67%; Goodison, 2022) limits the generalizability of our findings. This study excluded participants (in both LEO and civilian groups) with a history of prior cardiovascular disease (e.g., heart attacks); this also limits generalizability. Finally, this was a secondary analysis of a community sample. As such, information on other key demographic, lifestyle, and psychosocial variables that were not collected would be beneficial in providing a more robust comparison of CVD risk profiles between male LEOs and civilians.
Conclusion and recommendations for future research
In the current study, we found that male LEOs had significantly higher levels of both trait and state social vigilance. High levels of social vigilance have been found to evoke heightened cardiovascular reactivity, resulting in sustained increases in blood pressure, thereby promoting greater possible CVD risk. Our findings highlight the need for momentary assessment of cardiovascular reactivity among LEOs as it relates to the onset and development of CVD. Future research should seek to continue this work with larger sample sizes across different states and departments. Furthermore, samples sufficient to stratify LEO populations by factors aside from just occupation (e.g., departmental rank, years of service, sex, etc.) would be highly informative. In addition, research should include measurement tools designed specifically for this population (e.g., scale for measuring vigilance among LEO). Finally, although research has identified the need for health and wellness programs specifically for law enforcement, data is needed to address the barriers to organizing and facilitating these programs (e.g., financial, policy, bureaucratic) within departments.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the the National Institutes of Health, National Heart, Lung, and Blood Institute (NHLBI), R01HL109340.