
Abstract
Despite the clear utility and transferability, National Health Service (NHS) quality improvement initiatives have yet to benefit fully from what is already known within health psychology. Thus far, evidence from established, seminal behaviour change theory and practice have been ignored in favour of newly developed models and frameworks. Further, whilst there is a growing interest in what is commonly referred to as ‘human factors’ of change and improvement, there is scant transferability of known psychologically informed implementation skills into routine NHS Improvement practice. The science and practice of healthcare improvement is growing, and the behaviour change aspect is critical to sustainable outcomes. Therefore, this paper offers practical guidance on how seminal psychological behaviour change theory and motivational interviewing (a person-centred skills-based approach specifically developed to support people through change) can be combined to better address individual and organisational change within a healthcare improvement context.
Background and context
The current paper is written from a practice-based evidence perspective. The value of informing research and practice from a practice-driven approach (with support from the literature), rather than a wholly research derived, evidence-based approach has been recognised as a valuable method of closing the research-practice gap (Green, 2008). This approach also enhances the likelihood that recommended practice approaches are feasible and sustainably deliverable because such recommendations have been derived from and with practitioners rather than delivered to. The overarching aims of this practical-orientated position paper are to improve the all-important behaviour change component of National Health Service (NHS) improvement initiatives by a better integration of evidence-based health psychology research and practice. Specifically, by utilising seminal behaviour change theory to support programme design (what to do) and also integrating the behaviour change skills and strategies of motivational interviewing (MI) into routine delivery/facilitation (how to do it). Integrating well-established/evidenced behaviour change theory can better address the complexity of change and generate meaningful questions in the change process (e.g., Barley and Lawson, 2016). Amongst other things, MI supports the formulation of such questions.
The paper is comprehensive and organised into key sections that explore this aim. These sections include: quality improvement (QI) methodology, the human factors of improvement and behaviour change, applications of psychological theory to QI, MI (including the foundational, conceptual and core skills, ambivalence, resistance and advice giving), MI and coaching, translating behaviour change theory into practice and broader applications of the practical strategies with implications for practice. Practical examples of MI skills set within the context of general practice QI are also provided although these are highly transferable.
Quality improvement methodology
QI is a global concept, strongly linked with quality assurance (see De Jonge et al., 2011) that has applications to a range of industry settings from engineering to health and social care (e.g., Barth et al., 2022; Batalden and Davidoff, 2007; Clement et al., 2023; Gillam, 2022; Tercan and Meisen, 2022) including health equity (Nundy et al., 2022) and patient satisfaction (e.g., Mbwogge et al., 2022). There is no universal definition of QI although common themes include references to systematic approaches to performance data analysis, a method of improving performance, implementing changes to produce improvements and approaches to improving capacity and capability within organisational systems. Within a healthcare context, QI has been comprehensively described as the continued efforts of a range of people such as healthcare professionals, patients, planners, researchers and educators to implement changes leading to improvement. This may include patient outcomes, system performance and professional development (Batalden and Davidoff, 2007). The need for improvement strategies and programmes has become increasingly more important for healthcare (Portela et al., 2015) and had a critical role to play in supporting healthcare systems during the global Covid-19 pandemic (e.g., Staines et al., 2021). The nature of specific healthcare settings (i.e., primary care, secondary or emergency care) and within industry may prioritise certain elements of QI and approach over others although central to these is human behaviour change.
There is an international interest in QI (Hickey et al., 2017) although the literature largely demonstrates outputs from the UK and the USA (e.g., Marjoua and Bozic, 2012; NHS England, 2016; Royal Collage of General Practitioners, 2018). In broad terms, a range of models and tools are associated with improvement approaches, the most common of which include the Change Model/Model for Improvement (particularly within NHS primary care improvement), Six Sigma and Lean (e.g., D’Andreamatteo et al., 2015; NHS, 2018, 2022). The popularity of the Model for Improvement within healthcare settings has justified a systematic review which highlighted discrepancies in understanding and application and often inadequate depth of reporting which challenged clarity regarding utility (Taylor et al., 2014).
Central to the Model for Improvement is an approach known as Plan (identify the change to be implemented), Do (pilot the change), Study (assess the impact of change from measurable data) and Act (plan the next change cycle). This is often shortened to PDSA and a series of PDSA cycles are encouraged as part of the process of engaging in continued improvement (e.g., Crowl et al., 2015; NHS, 2022). Despite the challenges of implementing a PDSA approach that have been highlighted within the literature (e.g., Taylor et al., 2014), in practice, PDSA cycles offer a simple strategy to avoid what can often be reactive responses to implementing changes. Typically resultant of limited timeframes and what has been identified as unrealistic pressure to deliver outcomes (Maniatopoulos et al., 2020).
Tools to help implement QI are varied and include cause and effect diagrams (often referred to as fishbone diagrams), driver diagrams (that aim to identify specific routine actions and behaviours that influence the desired improvement/change) and process mapping (visually map out the current and desired operational process) to name just a few. For a comprehensive list of QI tools, the interested reader is directed to NHSE (no date). In addition to the Model for Improvement, NHSE Improvement utilise their self-constructed Change Model (see NHSE, 2018) and Sustainability Model (Maher et al., 2010) to operationalise their approach. A formative evaluation of the Change Model revealed that whilst considered valuable and practically useful, its utility was dependent upon an organisational culture that supported the fidelity of application. Further, that contrary to its intention, the Change Model was sometimes used to delegitimise opposition rather than enhance a shared purpose approach to implementation (Martin et al., 2013). Similarly, whilst the Sustainability Model has been reported as potentially useful within clinical settings (e.g., Silver et al., 2016), it was found to be difficult to understand and apply. Thus, how the models are implemented (i.e., the interpersonal skills utilised) is critical.
Appropriate testing and refinement of such models has been encouraged to gain a more robust, objective and evidence-based understanding of their real-world application (Doyle et al., 2013). It is noteworthy that The Health Foundation have produced a useful QI guide which also refers to the importance of both technical and relational skills (Jones et al., 2021). However, whilst the importance of collaboration and co-production are suggested as important relational factors, there is no reference to specific interpersonal skills or learning from psychology to demonstrate how this might be demonstrated in practice.
Whilst these models are routinely integrated into global QI practice to provide a framework for delivery, they are not specifically designed to address behaviour change. QI design and delivery has yet to benefit from the clear transferability of behaviour change expertise that is routinely integrated into health psychology practice in particular. Specifically, at the time of writing, there has yet to be any reference to, or utility of the seminal theory or evidence-based behaviour change skills (e.g., MI) in NHS QI practice guidance. Indeed, a recent systematic review of QI collaboratives (whereby multidisciplinary teams share learning), specifically indicated the need for greater use of behaviour change and psychology theory/practice to improve QI design, adaption and evaluation (Zamboni et al., 2020).
The value of integrating psychology into QI practice has been recognised by the Institute for Healthcare Improvement (IHI) in the publication of their Psychology of Change Framework white paper (Hilton and Anderson, 2018). There is also growing recognition of the value of integrating behavioural insights and psychology into improvement (e.g., Perry et al., 2015). However, to date, there is yet to be any specific reference to the decades of behaviour change theory research, now considered seminal behaviour change theory. Nor is there evidence of the explicit integration of evidence-based psychological skills that have been consistently demonstrated to facilitate change, into routine NHS improvement practice. Consequently, there is a critical opportunity for health psychology to support the design and implementation of healthcare QI.
The human factors of improvement and behaviour change
Behaviour change is fundamental to QI because the degree to which changes in processes and procedures are implemented are dependent upon the behaviour of those who deliver them. Yet, within routine NHS improvement practice, learning from behaviour change theory and practice is comparatively overlooked at the expense of an emphasis on QI models and tools. Perhaps because it has been suggested that the behaviour change aspect of QI is the most difficult to deliver and underestimated (Kadom and Nagy, 2016). It is also important here to draw the distinction between the practice integration of behaviour change theory and taxonomies (explored in more depth in the next section) and interpersonal behaviour change implementation skills. Whilst there is some evidence that behaviour change strategies to support the design of QI interventions are being integrated into the scientific QI literature (e.g., Lucas and Nacer, 2015; Steinmo et al., 2015), there is comparatively less regarding what psychologically informed skills are useful to support behaviour change. Further, and as mentioned previously, neither the theory nor the practice have been explicitly integrated into NHSE Improvement. This gap in behaviour change skill transfer into practice is elaborated upon later in the current paper.
The need to have a better balance between theoretically informed design and the assessment of the person-centred skill competencies of those who deliver behaviour change interventions, is reflected in the recent development of a competency framework (Dixon and Johnston, 2021). However, in addition to any agreed competencies, proficiency in person-centred approaches to facilitation may be better assessed via ongoing supervision and coaching rather than a competency checklist per se (e.g., Hilton et al., 2016) which would require a paradigm shift in thinking about NHS investment in supporting adequate proficiency in skill development.
A wealth of psychology research has informed our understanding of the complexity of behaviour change. One of the most consistent findings from practice-based behaviour change research is that a lack of knowledge does not always explain why people do not engage in desirable behaviour (Miller and Rollnick, 2012; Rollnick et al., 2010), and that there is a commonly observed disconnect between knowledge and behaviour (e.g., continuing to smoke despite understanding the health risks). However, despite this, it is not uncommon to assume that gaps in knowledge account for behaviours that do not reflect those that are desired (e.g., implementing changes to routine practice/processes). Therefore, in the absence of access to training in more collaborative/person-centred approaches, there is a risk that a typically unhelpful ‘expert driven’ approach to behaviour change (and within a clinical context, the medical model e.g., Elkins, 2009), that relies heavily on educating people regarding why they should change and the consequences of not doing so, is adopted. From the perspective of the behaviour change approach, MI this is often referred to as wrestling with change rather than dancing (as equal and active partners in the change process) and this expert driven approach has consistently been demonstrated as ineffective in supporting people through change (e.g., Rollnick et al., 2010).
It is recognised that there are examples of local/regional change initiatives that attempt to integrate behavioural change into their implementation. However, the emphasis is typically on design rather than delivery. This is potentially limiting the impact of QI and may also account for the challenges with engaging clinicians in QI (e.g., Davies et al., 2007). Moves towards a more collaborative/participatory approach to healthcare QI design have been proposed (Mitchell and Jun, 2019) although once again, we see no recognition of how fundamental aspects of a participatory approach such as co-development/production are implemented – what interpersonal skills could be utilised and in what way? How can behaviour change counselling skills support this aim?
Within NHSE Improvement, a common attempt to integrate psychological theory into QI is Kotter’s (1996) change model (e.g., Aziz, 2017). However, there is sparse empirical support for the model and a review of 15 years of literature indicated that there was limited evidence for its validity despite its popularity (Appelbaum et al., 2012). Where psychology-informed strategies are considered, their emphasis is upon behaviour change taxonomy/techniques (Abraham and Michie, 2008) or persuasion (Perry et al., 2015). Taxonomies are perhaps best described as a ‘list of ingredients’ (i.e., brief descriptions of what to do/include) and have been criticised for their limited emphasis upon interpersonal process (Hilton and Johnston, 2017). Persuasion has also been consistently demonstrated as an ineffective approach to supporting people through change. Particularly for those who feel uncertain, persuasion may serve to increase resistance to change (e.g., Gabarda and Butterworth, 2021).
These limitations are arguably demonstrative of the challenges of applying theory to practice more generally without also supporting the development of the relational/interpersonal skills needed for implementation. Similar limitations are observed in the increasing popularity of leadership models and approaches such as appreciative inquiry (AI; Barrett and Fry, 2005) and experience-based design (EBD; Bate and Robert, 2007) that provide guidance on what to do but again, lack attention to the interpersonal skills needed to deliver such approaches (how to do it). Indeed, a recent study determined that successful QI projects needed both the technical and the relational skills and that without the latter, projects are likely to fail (Wright et al., 2022).
There is evidence to suggest that healthcare and the NHS are largely outcome and performance focused (e.g., Downing et al., 2007; Ivers, et al., 2012; NHSE, 2015). If we use a cooking analogy previously utilised by Hilton and Johnston (2017) this lack of attention to implementation processes is somewhat like having all the ingredients for a recipe (what is needed) without the method (how to mix the ingredients together - in what order, how long to cook for, how to cook them etc.) Arguably, QI currently has a comprehensive list of ingredients (tools) but comparatively less guidance and training on best-practice approaches to integrating them (the skills required to deliver). Psychology offers valuable insights into not just what to do (evidence-based and theoretically informed approaches) but also how to do it (specific interpersonal skills to support the collaborative engagement of participants and the change process). There is an innovative opportunity to apply this highly transferable theoretical and practical evidence into the context of QI design and delivery.
Applications of psychological theory to quality improvement
The increased interest in developing QI delivery models is perhaps driven by the understanding that interventions that are theoretically underpinned are more likely to be effective (e.g., Glanz and Bishop, 2010). Further, the need to include clear and established theories of change has been identified as an indicator of QI programme success (Aveling et al., 2012). However, the limitations of only integrating theory into QI (and other) contexts in an effort to enhance the evidence-based rigour, also increases the risk of an overly expert-driven and rigid approach (Ogden, 2016). This exemplifies why the combination of design theory and implementation skills is so important. There is extensive published work including systematic reviews demonstrating the utility and impact of the behaviour change theory presented below (e.g., Cooke et al., 2016; Hashemzadeh et al., 2019; Tang et al., 2020).
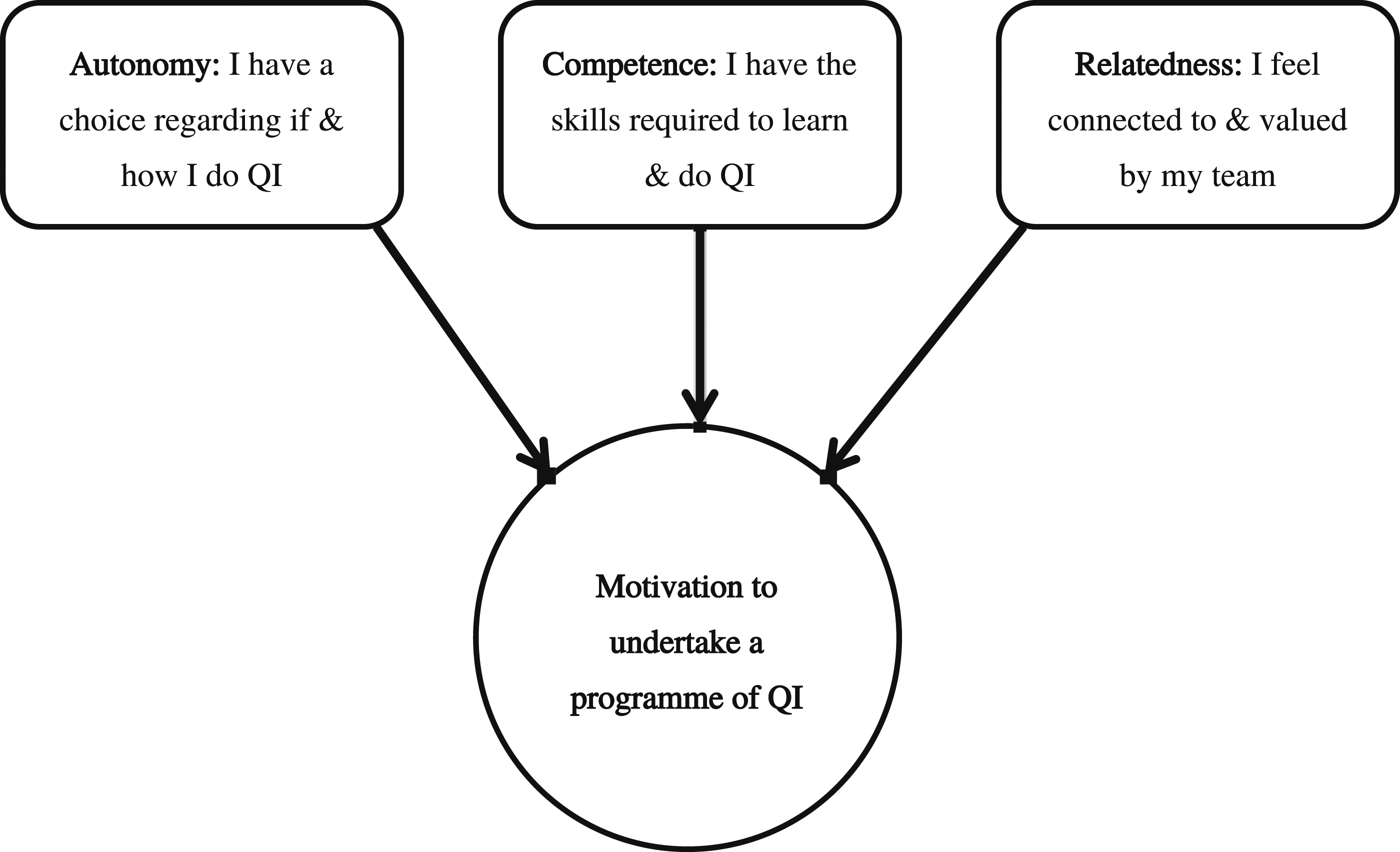
This seminal behaviour change theory is synonymous with health psychology in particular. It is typical that these theories comprise a central part of health psychology teaching and training (i.e., taught university programmes such as MSc) and have common applications as the theoretical underpinnings for behaviour change intervention studies. Therefore, it is recognised that a health psychology audience are typically very familiar with their design (including the capability, opportunity, motivation; COM-B model described below). Learning from this seminal work may be integral to health psychology, but it has yet to be formally integrated into routine NHSE Improvement initiatives. Therefore, for succinctness, context and clarity, rather than a written summary, Figures 1–4 present a visual representation of how the Health Belief Model (Becker, 1974), the Theory of Planned Behaviour (TPB; Ajzen, 1991), the Transtheoretical model (TTM; Prochaska and DiClemente, 1983) and Self Determination Theory (SDT; e.g., Ryan and Deci, 2018) can be utilised in a novel way within a QI context. Applications of The Health Belief Model to Quality Improvement. Applications of the Theory of Planned Behaviour to Quality Improvement. Applications of the Transtheoretical Model to Quality Improvement. Applications of Self Determination Theory to Quality Improvement.


It is perhaps somewhat ironic that much greater attention has been given to the stages of change component of the TTM (i.e., precontemplation through to maintenance including relapse). Further, the literature demonstrates an emphasis on progression through the earlier stages and often neglects the all-important self-efficacy and decisional balance components of the model which are critical influencers of a persons’ progression through the stages. Indeed, it is common that the TTM is incorrectly referred to as the Stages of Change Model/Cycle. Moreover, the accompanying 10 processes of change of the TTM (i.e., consciousness raising, dramatic relief, self-re-evaluation, environmental re-evaluation, social liberation, self-liberation, helping relationships, counter-conditioning, reinforcement management and stimulus control) that predict how people engage in a process of change and what influences the stages, are commonly omitted from research that utilise the model. This is perhaps a further demonstration of a historical emphasis within research and healthcare practice on outcome rather than process. It may also demonstrate a related problematic emphasis upon evidence-based practice (derived from research to inform research and practice) rather than practice-based evidence (derived from practice to inform research and practice). This historical emphasis is likely to have contributed to commonly experienced gaps between research and practice (e.g., Green, 2008).
Key psychological theories mapped onto motivational interviewing four tasks and skills – the what and the how.
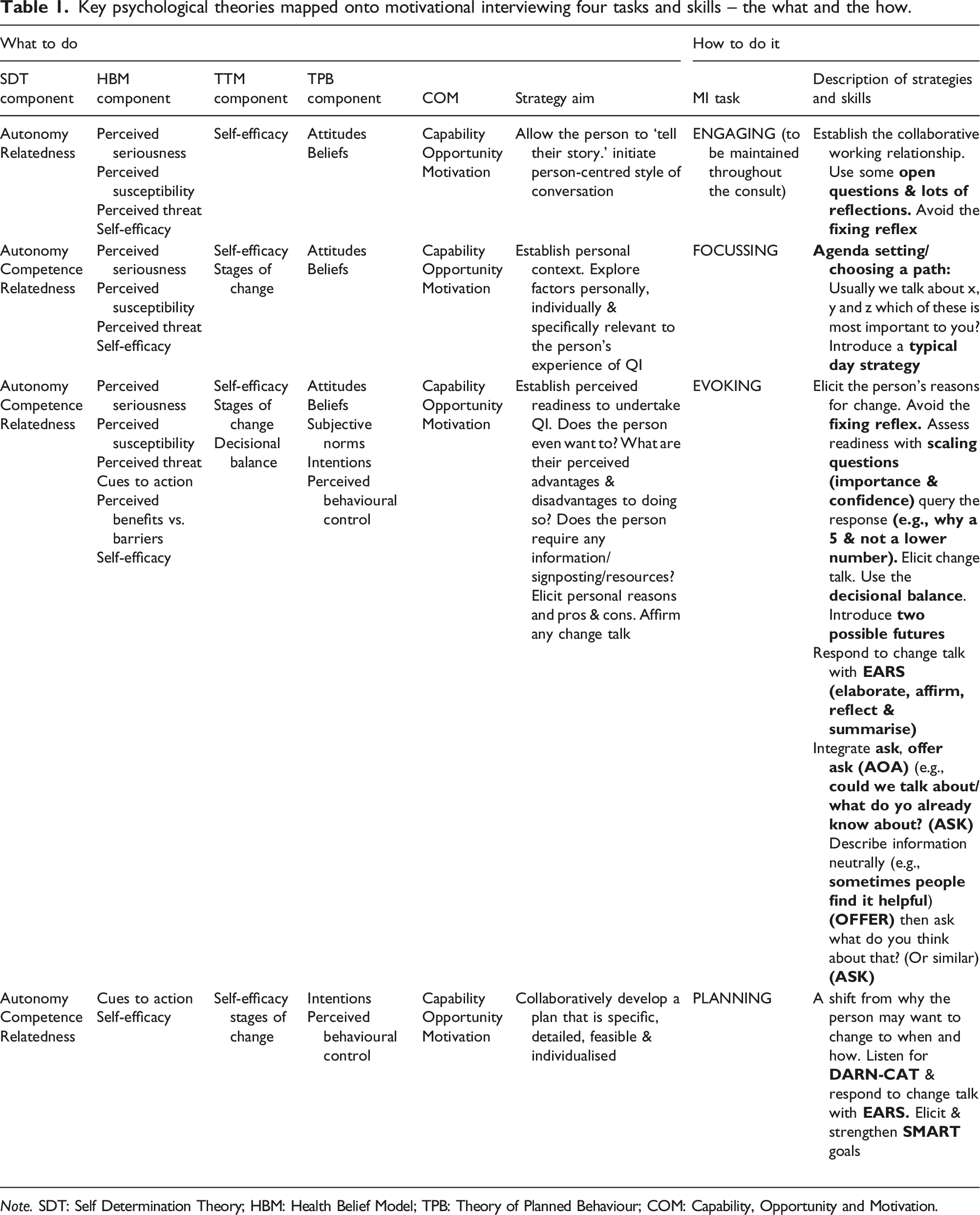
Note. SDT: Self Determination Theory; HBM: Health Belief Model; TPB: Theory of Planned Behaviour; COM: Capability, Opportunity and Motivation.
One of the more recent additions to the literature is the COM-B model (Michie et al., 2011). The model was formulated with the aim of improving the design and implementation of behaviour change interventions. In addition to the core conditions of capability, opportunity, and motivation, the model offers a practical approach of utilising a behaviour change wheel (BCW) comprising nine functions aimed to address deficits in these conditions and seven categories of policy that enable interventions. Such is the popularity of the COM-B model, that a COM (capability, opportunity and motivation) components questionnaire has recently been developed and the psychometric properties assessed, to further encourage the integration of COM-B into the design of behaviour change interventions (Keyworth et al., 2020). Similar attempts to provide an implementation framework of typical barriers and facilitators of change have been made by the formulation of the Theoretical Domains Framework (TDF; Atkins et al., 2017). Indeed, the TDF has been combined with PDSA cycles in an effort to reduce sepsis mortality although the primary outcome of this research was the modification of an existing taxonomy rather than any attention to the all-important interpersonal skills needed to operationalise it (Steinmo et al., 2015).
Consequently, the desire to offer some level of standardisation and replication via the application of the COM-B model and related behaviour change taxonomies/frameworks (e.g., the BCW) has been discouraged in favour of recognising the value of responding appropriately to variability and operating as practitioners rather than technicians (Ogden, 2016). In a similar way, it is noteworthy that the limitations of transferring COM-B into the skills needed to operationalise it have also been recognised in a recent systematic review (Kumar et al., 2021). Despite these limitations, the model does offer practical guidance for intervention design (including QI).
In general terms, the aforementioned seminal behaviour change theories differ to the more recent development of taxonomies because they offer a broader theoretical understanding of factors that influence change whereas COM-B provides a list of behaviour change components (or ingredients to choose from) and the TDF aims to consolidate key theories into domains and constructs. To address the interpersonal skills-based limitations described, the capability, opportunity and motivation components are also included in a summary of MI skills mapped onto the relevant theory in Table 1.
What is motivational interviewing?
MI was first introduced as a behaviour change counselling approach to support people with problem drinking (Miller, 1983). However, the utility of MI has expanded to support a range of behavioural changes (Hilton et al., 2016). This also includes leadership to enhance positive organisational culture and productivity (Marshall and Neilsen, 2020; Wilcox et al., 2017). Whilst MI does not have theoretical underpinnings as such, the TTM and SDT described earlier are commonly used to explain why MI may work as it does to support people through change (e.g., Filiz et al., 2020; Vansteenkiste and Sheldon, 2006). As a practical approach with a strong evidence-base and broad utility, MI is highly relevant to health psychology and supports the translation of behaviour change theory into practice. It is the only behaviour change skills-based approach to specifically and actively work with feelings of uncertainty about change (ambivalence) and has most recently been defined by the originators as “a collaborative conversation style for strengthening a person’s own motivation and commitment to change” (Miller and Rollnick, 2012, p. 12).
Developing proficiency in the method alongside other interpersonal skills has previously been highlighted as useful for practicing psychologists - particularly for those undertaking Stage 2 Qualification in Health Psychology (see British Psychological Society, nd; Hilton and Johnston, 2017). Learning MI may be linked to eight distinct stages: (1) openness to collaboration with clients’ own expertise, (2) proficiency in person-centred counselling, including accurate empathy, (3) recognition of key aspects of client speech that guide the practice of MI, (4) eliciting and strengthening client language in favour of change, (5) rolling with resistance, (6) negotiating change plans, (7) consolidating client commitment, and (8) switching flexibly between MI and other intervention styles (Miller and Moyers, 2006). The concept of rolling with resistance is somewhat outdated and in more current MI thinking, resistance has been re-conceptualised as a product of the interpersonal relationship (Miller and Rollnick, 2012). Nevertheless, these eight stages are often considered as a useful guide. In terms of duration, and type of training, it is suggested that a 2–3-day introductory course and attendance at more advanced training with coaching/supervision is a useful approach to developing proficiency (Hilton, 2023).
The interested reader is directed to Britt et al. (2003) for a useful review of MI and Miller and Rollnick’s (2012) and forthcoming (2023) text for a comprehensive overview of the MI approach. What follows is a highly practical presentation, with supporting demonstrations of how MI can be integrated into a healthcare QI context. As mentioned earlier, the examples provided reflect conversations within general practice although they are highly transferable.
The conceptual and foundational skills of motivational interviewing
For ease of understanding, and to assist the reader to cross refer to summary Table 1, MI strategies and skills that are referred to henceforth are presented in
Central to the practice of MI is attention to avoiding an overreliance upon the skills and instead ensuring that the practitioner maintains Conceptual diagram of the motivational interviewing four tasks and spirit.
In contrast to MI-spirit, the
The core skills and strategies of motivational interviewing
There are several texts that provide comprehensive descriptions of the MI approach, skills and strategies. As mentioned earlier, the interested reader is directed to Miller and Rollnick (2012) and Miller and Rollnick (2023) for the two most recent core texts written by the founders of the approach. The core skills that comprise MI are:
Questions that start with ‘how,’ ‘what,’ ‘why,’ ‘tell me,’ ‘explain’ and ‘describe’ tend to be much more open than alternatives (see Hilton, 2023 for practical examples). Figures 1, 2 and 4 present examples of
Coupled with the relational component of MI spirit, these MI core skills (OARS) are incorporated into an MI-consistent conversation alongside additional strategies such as
An Agenda Setting/Choosing a Path Strategy.
A frequent consideration for those who deliver QI initiatives (and arguably supporting anyone through change) is whether an individual/team is even ready to consider implementing changes/improvements. Indeed, the concept of readiness alone has been deemed integral to healthcare delivery (Dalton and Gottlieb, 2003). MI considers that the perception of readiness is culminated by a combination of perceived importance and confidence. The more important and confident someone is to make changes, the greater their perceived readiness and vice versa. As a consequence of this relationship, an additional MI strategy is the use of scaling questions. For example, a QIS may ask a healthcare staff member who is ambivalent about the value of QI:
“On a scale of 1–10 with 1 being not at all important and 10 being very important, how important is it for you to assess your prescription process?”
and
“On a scale of 1–10 with 1 being not at all confident and 10 being very confident, how confident are you to assess your prescription process?”
A curious approach to assessing confidence is also consistent with the self-efficacy component of the HBM (see Figure 1) and the TTM (see Figure 3). Therefore, combining the use of open questions with a scaling question of confidence offers further practical examples of translating theory into practice. In addition, a numerical assessment of perceived importance and confidence not only allows for insights into a person’s readiness but also allows for the introduction of follow-up questions to elicit what is referred to as
Hearing
Conversely,
An increase in change talk is typically an indicator to move into the planning process of MI. Typical responses to change talk that strengthen and support the process have been identified as
As is often the case in healthcare, it can be difficult to identify the area of improvement to focus upon that is likely to result in a large impact without over-burdening staff. Similar to a benefit-effort matrix QI tool (whereby areas of practice that could be worked on are mapped against the relative effort to complete them),
Ambivalence, resistance and advice giving
Perhaps particularly because MI is a person-centred approach, as described earlier, accepting that a person may feel genuinely unsure (or ambivalent) about change is an accepted part of the change process. It is the process of actively working with ambivalence that has been attributed to some of the success of MI (Rice et al., 2017). How a practitioner responds to any observed resistance or ambivalence has a direct impact upon the likelihood of change (Drage et al., 2019). In more general therapeutic terms, this is akin to the importance of therapeutic alliance (or relationship) being critical to predicting favourable outcomes (e.g., Horvath and Bedi, 2002).
The
Whilst MI is a person-centred approach, the method does allow for exchanging information where this is considered helpful. However, as a general rule, permission to do so is always sought first using a strategy
QIS: “Would it be OK if I shared a strategy with you that might be helpful based upon my experience of working with other practices who have had a similar challenge to you”
Practice Manager: “Yes, that would be helpful”
QIS: “Sometimes when you’re so busy delivering a process it’s very difficult to step away from it and assess whether that process is working efficiently for you. What others have found helpful is that when you process map, whereby you visually map out the process from start to end, it allows you to see what about that process is working well, and also where there might be opportunities for improvement” (
QIS: “How does that sound to you?” (
Motivational interviewing and the rise in coaching approaches
It is noteworthy that in recent years there has been an increased interest in a ‘coaching’ approach to delivering QI and in healthcare interventions more generally (e.g., Calo et al., 2019). It has been previously recognised that the generic use of the term coaching without any specificity regarding the approach used is problematic for assessing reliability and validity (Newnham-Kanas et al., 2010). Further, the literature is typically unclear regarding what the specific interpersonal skills and implementation processes of coaching are (see Ives, 2008 for a comprehensive review).
A popular coaching model is the GROW model (Whitmore, 2009) which refers to: goal, reality, options and will. Similar to the MI
In MI terms, this approach to setting goals early in the process would be considered a
Given the rise in popularity of ‘coaching approaches’ and the GROW model in particular (Passmore and Sinclair, 2020), there is potential for the more therapeutically informed interpersonal skills of MI to complement and extend the implementation of the model, and what in practice are deemed as a coaching approach to behaviour change more generally. Figure 7 depicts how conceptually, the GROW model might fit with the The Four Tasks and Conceptual Links with the GROW Model of Coaching.
Mind the (skills) gap! Translating behaviour change theory into practice
The translation of theory (what to do) into practice (how to do it) reflects an enduring challenge across the social science disciplines. As mentioned earlier, whilst there is a growing interest in translating behaviour change theory into practice, the literature is weighted towards utilising behaviour change theory to influence intervention design rather than skills per se (e.g., Gardner et al., 2010; French et al., 2012; Sremanakova et al., 2021). As a useful demonstration, Fry et al. (2020) unintentionally exemplify why this theoretical weighting is problematic. In their survey of nurses, behaviour change was identified as central to clinician and patient QI engagement. However, the ‘implementation strategies’ that are suggested to support this (and broader processes) were theoretically informed (using the BCW) and offered no attention to the skills needed to deliver. Further, whilst not specifically related to QI, perhaps one of the clearest demonstrations of the skills gap is provided by Reid et al. (2022). In a study that explicitly aimed to improve person-centred conversations about physical activity, there is not a single reference to, suggestion, or example of person-centred conversation skills. Rather, the BCW was utilised to formulate intervention development.
Similarly, with the broad aim of enhancing the translation of behaviour change research into practice, there have been recent innovative calls to better combine health psychology with implementation science (Presseau et al., 2022). However, the role of the interpersonal skills of those who translate such research into practice is not considered. The central aim of translational theory into practice studies is to offer frameworks to categorise and evaluate interventions and attempt to identify the mechanisms that account for observed outcomes (Gardner et al., 2010). Although, without attention to the implementation process skills, better understanding the mechanisms seems an impossible task. This current trend in the literature provides clear evidence regarding common misconceptions regarding the what and the how to of behaviour change.
If not a misconception, perhaps the translation of behaviour change theory/taxonomy strategies into intervention design seems easier than a translation to skills? It is also reasonable to suggest that the academic community is more familiar with the translation of theory into practice in this more intervention design type of approach – as the classic Johari Window would suggest, you cannot know what you do not know (Luft and Ingham, 1961)! What is certain, is that the current trend in the literature reflects a missed opportunity that the MI skills proposed in the current paper have the potential to impact upon within future QI implementation research.
Therefore, with the aim of responding to this current challenge, Table 1 presents a summary of what components of the relevant cited theory presented in the current paper, map onto each of the MI four tasks and how differing MI skills support delivery – the what and the how. It is intended that Table 1 has relevance for any behaviour change intervention that aims to combine theoretical underpinnings with evidence-based implementation skills and not just for the context of QI. However, combining Table 1 as an overview with Figures 1–4 provides a visual reference to help the interested reader to translate evidence-based behaviour change theory and MI skills into routine QI conversations.
Implications for practice and broader applications
The seminal behaviour change theory and the practice of MI have broad applications with demonstratable utility and impact across a range of health contexts. However, they have yet to be adopted within routine NHS improvement contexts in favour of the development of comparatively untested models that are not designed to specifically address behaviour change (Doyle et al., 2013). There is also little to no evidence of behaviour change skills training/approaches for those who deliver. The current paper demonstrates how transferrable psychology knowledge and skills support the design and delivery of QI programmes in an innovative, evidence-based and novel way. Adopting this approach responds directly to the need to incorporate a better evidence-base (what), implementation skill-based strategies (how), enhanced engagement of people (who) and their motivations (why) that has been reported as critical to the psychology of change within a QI context (Hilton and Anderson, 2018). Rather than continue to develop untested QI models and frameworks that fail to address behaviour change, it makes much better sense to draw upon what is already known and evidenced within the health psychology literature and practice. It has been previously recognised that the NHS is poor at sharing good practice across services and worse still at benefitting from learning from outside organisations (Moberly, 2016). Therefore, perhaps the greatest challenge of integrating the learning presented here is the requirement of an NHS practice paradigm shift.
As described, as a behaviour change approach, MI is particularly suited to working with individuals who are ambivalent about change (Westra and Norouzian, 2018). Therefore, whilst the examples provided here reflect a general practice context, adopting a MI approach within QI settings may help busy healthcare staff across the system with competing demands on their time to better explore the cost-benefit of QI. Perhaps specifically using the
Similarly, rather than purporting that there are people who are resistant to change and those who are not, MI suggests that resistance is often the product of interpersonal processes (e.g., the relationship/environment/working culture) (e.g., Harakas, 2013). Therefore, adopting a MI approach also presents an opportunity to resolve the underlying causal factors of what is often experienced as staff who are resistant to change such that working relationships and culture are improved. Further, the person-centred approach of MI means that change is driven by staff that are intrinsically motivated, that have their values represented within the change process and therefore any changes implemented are much more likely to be sustainable. These types of courageous conversations have the capacity to recognise not just what people do at work but who they are within that context (Bunniss, 2021).
For healthcare staff that may be interested in adopting a MI-consistent approach as part of their routine practice, MI also has the added value and transferability of improving leadership approaches, staff appraisals that are more collaborative, meetings that are inclusive yet focused, conflict management, reduced clinician burnout, enhanced patient engagement and satisfaction and a values-based working culture (e.g., Marshall and Neilsen, 2020; Passmore, 2007; Pollak et al., 2016; Wagner and Ingersoll, 2012). Integrating the skills provides a practical communication method to encourage patients to become an active participant in QI work which has been identified as a critical component of QI (Andersson and Olheden, 2012). Further, integration of MI skills for staff also supports non-clinical team members who typically facilitate Patient Participation Groups (PPGs), to do so in a manner that enhances group facilitation skills. Whilst MI should not be considered a panacea, it is clear that the person-centred communication element alone has value across a range of healthcare contexts. Developing proficiency in MI can require adequate investment in time and money, although the transferability of skills across such a broad range of scenarios presents a valuable investment for the NHS.
The notion of person-centred care has become synonymous with quality care (Brooker, 2003) although in practice, few approaches claiming to be person-centred are based upon the core conditions identified by Carl Rogers (1980) which makes it difficult to understand in what way they are truly person-centred. This further complicates progressing our understanding on what implementation skills and strategies explain what works for whom, in what way and under what conditions. Integrating MI into routine NHS improvement delivery, offers evidence-based consistency in this regard. However, it is recognised that for the purposes of evaluative/impact research, adequate fidelity testing (i.e., adherence to MI for those who delivered) would need to be an integral part of the design. Indeed, it is lack of attention to MI fidelity or perhaps under reporting due to word limitations which represents a consistent problem within the literature.
The current variability in QI design and delivery poses challenges for evaluation and informing best practice – especially with respect to adequately addressing behaviour change. What is proposed here offers a way of supporting greater global opportunities of cross-comparison between QI interventions and shared learning that is grounded in a comprehensive theoretical and practical evidence base. Utilising the existing diverse skills of health psychologists (who may also have some level of proficiency in MI), creates new and innovative opportunities for health psychologists to collaborate with NHS improvement specialists to enhance the rigour and impact of behaviour change. This would also create new opportunities to make better use of the expertise of health psychologists within the NHS that has been historically underutilised (e.g., Kaplan, 2009; Newson and Forshaw 2009) and remains limited (Hart et al., 2023). To date, NHSE Improvement do not actively advertise for health psychology roles despite the clear utility of their knowledge and skills within this context.
Finally, the purposeful combination of theory and practical skills presented here has relevance for any behaviour change context. It is not uncommon for interventions to utilise behaviour change theory yet, the implementation skills to translate the theory into practice are often lacking or unreported (Hilton and Johnston, 2017; Ogden, 2016). With the intention of supporting efforts to close this gap within the behaviour change literature and practice more generally, Table 1 presents a comprehensive summary of seminal psychological theories mapped onto the four tasks and micro skills of MI – the what and the how. It is anticipated that this will support a better integration of seminal theory and skills into behaviour change interventions for both researchers and practitioners.
Footnotes
Author contribution
C.E.H. is the sole author and conceived, prepared and finalised this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.