
Abstract
This study investigated the associations of relationship satisfaction, depression, and anxiety post-acute coronary syndrome in a sample of men having completed an early, couple-focused, and men-tailored psychoeducation intervention. A baseline sample of 50 male patients were followed over a 12-month period and completed the Couples Satisfaction Index and the Depression, Anxiety and Stress Scale. Results revealed a significant improvement in depression symptoms from T0 to T1, during which all participants completed the MindTheHeart® psychoeducation intervention. In addition, a hierarchical regression analysis showed that relationship satisfaction is an important predictor of this improvement in depression symptoms. Our preliminary findings point to the consideration of life partners in post-ACS interventions and encourage the exploration of this clinical approach in future research.
Introduction
Labelled the second leading cause of death in Canada, acute coronary syndrome (ACS) comprises a group of cardiac conditions in which a reduction or blockage of blood supply to the heart occurs (University of Ottawa Heart Institute, 2022). Unstable angina (UA), non-ST segment elevation myocardial infarction (NSTEMI), and ST segment elevation myocardial infarction (STEMI) are the main pathologies constituting ACS (Cojocariu et al., 2021). Recent clinical literature signals a high prevalence of psychological disorders in patients recovering from ACS. According to Greenman et al. (2018), post-ACS depression and anxiety have reported rates as high as 20% and 16% respectively. For myocardial infarction (MI) alone, Reid et al. (2013) stated that the condition often causes major depressive disorder and anxiety, with these two reaching rates of around 20% and 30–40% each. Additionally, there is a well-documented link between depression and anxiety on one hand, and higher cardiac morbidity and mortality on the other hand (Greenman et al., 2018; Reid et al., 2013; Tulloch and Greenman, 2018). It is important to consider that men and women are affected differently by the psychological effects of ACS. For instance, women are more likely to experience depression after a coronary event, however, men’s depression is more likely to predict recurrent events and mortality (Doyle et al., 2015).
This context is particularly concerning given that men are twice as likely to suffer an MI and are generally a decade younger than women when they are first diagnosed with an ACS (Public Health Agency of Canada [PHAC], 2017). Although the incidence of heart disease has declined by about 50% between 2000 and 2010 in New Brunswick, a large sex gap persists through years (New Brunswick Department of Health, 2013). For acute MI, the sex gap is steadily increasing over time. Indeed, PHAC reports that in 2000–2001 men had about 80,000 more acute MI diagnoses than women, while in 2012–2013 they had more than 200,000 more diagnoses (2017). Moreover, not only is the mortality risk of heart disease 20% greater in men, but they are also more likely to die prematurely from heart disease (i.e. before the age of 75) (PHAC, 2017). The high prevalence of ACS in men paired with the frequent occurrence of psychological disorders post-SCA is alarming considering that consultation rates and help-seeking behaviours are significantly lower in men than in women. To make matters worse, Covid-19 has caused the closure of many cardiac rehabilitation (CR) programs due to concerns of virus transmission (Chindhy et al., 2020). As is often the case, individuals prone to psychological problems are disproportionately affected by the current pandemic.
A key protective factor identified in post-ACS recovery is the presence of a life partner (Hayes et al., 2016; Manfredini et al., 2017). Being in a marital relationship is associated with decreased risk factors and better chances of survival in patients with a cardiovascular disease (Manfredini et al., 2017). Being married, compared to being single, is also associated with increased longevity of life in patients who have had a heart transplant (Manfredini et al., 2017) and lower ACS mortality rates (Tulloch et al., 2020). One intrinsic aspect of relationships, namely relationship satisfaction, has been explored by a small number of researchers. Often used interchangeably, the terms relationship satisfaction and relationship quality refer to an individual’s subjective evaluation of their relationship, no matter the status of this relationship (i.e. marital, or not) (Keizer, 2014).
One of the main themes emerging from the findings of a systematic review of heterosexual couples in which the man has a cardiovascular disease is that the quality of couples’ relationships affects the physical, mental, and emotional response of both partners following diagnosis (Trump and Mendenhall, 2017). More specifically, two articles in this review found a negative correlation between marital quality and distress for both partners (see Rohrbaugh et al., 2002, 2008). This result is consistent with Tulloch et al.’s (2020) assertion that high-quality relationships can strengthen psychological health in the face of cardiovascular disease, and conversely, that low-quality relationships can be a risk factor for the development of psychological disorders (Tulloch and Greenman, 2018). Looking more specifically at depression, Dekel et al. (2014) found that the higher men’s marital satisfaction was at the time of their ACS hospitalization, the fewer depressive symptoms they had at that time, as well as 6 months later. Novak et al. ‘s 2014 study, for its part, does not reveal a significant link between the marital satisfaction of men with a cardiovascular health problem and their depressive symptoms. Nevertheless, the results show that in healthy men, the higher the level of marital satisfaction, the less they experience depressive symptoms (Novak et al., 2014). The researchers therefore argue that some aspects of marital satisfaction appear to be different for heterosexual couples where men have a cardiovascular health problem compared to healthy couples (Novak et al., 2014). However, they do not provide an explanation for these differences.
On the qualitative side, Jbilou et al. (2019) conducted focus groups and one-on-one interviews with men who had had an ACS or heart surgery. The male participants perceived that the support received from their life partner helped them cope with stress and anxiety (Jbilou et al., 2019). More specifically, the attention, compassion and understanding provided by their life partner and loved ones were particularly appreciated; however, overprotection could be perceived as irritating (Jbilou et al., 2019). It should be noted that all studies mentioned thus far have been conducted on heterosexual couples only.
Psychoeducation interventions have demonstrated success in alleviating symptoms of depression and anxiety post-ACS and are even described as an integral component of CR by some clinical researchers (Cojocariu et al., 2021). Indeed, these interventions aim to educate patients on the mental health risks related to ACS and provide information that could correct beliefs and promote patients’ active participation in the recovery and treatment process (Fernandes et al., 2017). However, there are not many psychoeducation interventions that are tailored specifically to men, and of those that do exist, the ones that elicit life partner involvement are virtually nonexistent despite the data that would support this approach. To the best of our knowledge, the MindTheHeart® psychoeducation intervention is the only one to have done this. As a result, the aim of this study was to gain a better understanding of the associations of relationship satisfaction, depression, and anxiety over a 12-month follow-up period in men having completed an early, post-ACS couple-focused and men-tailored psychoeducation intervention. While most studies have explored relationship satisfaction using the couple as the unit of analysis, Barton et al. (2020) indicated that two-partner designs diminish the variability in relationship measures. For this reason, the present study exclusively favours the perspective of the male patient. Based on the literature summarized above, we expected (H1) that relationship satisfaction would be negatively associated with depression and anxiety at all measurement times. We further expected (H2) to find improvements in depression and anxiety over time, particularly post-psychoeducation intervention. Lastly, we hypothesized (H3) that relationship satisfaction would predict better outcomes in depression and anxiety at subsequent measurement times.
Methods
Design
The present study is a secondary analysis of data collected in New Brunswick as part of the MindTheHeart® project. This project was designed as an open-label, single-arm clinical trial (ClinicalTrials.gov Identifier NCT03354351). The MindTheHeart® project used a prospective observational cohort with a nested, stepped-care psychological intervention in three Canadian provinces.
Stepped-care psychological intervention
A stepped-care intervention model was used for early detection and treatment of mood disorders (MD), anxiety disorders (AD), and trauma-related stress (TRS) in men with ACS. During the baseline and follow-up data collections (more details below), participants were evaluated and referred to the appropriate step of the stepped-care intervention model. Any participant showing signs of suicidal intent was immediately referred to a qualified health professional. Step 1 consisted of individual psychoeducation and skills development and was completed, by all participants, within the T0 to T1 time interval. The objective of Step 1 was to provide patients with the necessary tools to self-educate on the mental health risks related to ACS. Step 2 consisted of group therapy for skills reinforcement and support. Qualifying patients were invited to eight two-hour group therapy sessions based on men-tailored cognitive-behavioural therapy (CBT) and emotionally focused therapy (EFT) for MD and/or AD. Patients had the opportunity to invite their life partner (or family member or close friend) to the last four group therapy sessions. Patients presenting TRS symptoms were referred to five individual sessions of trauma-focused CBT. Step 3 consisted of couple or individual therapy for skills reinforcement and support. Qualifying patients were invited to eight to 12 individual or couples therapy sessions (depending on preference and marital status) based on men-tailored CBT and EFT for MD and/or AD, or to 10 to 15 individual trauma-focused CBT sessions for TRS.
Participants and procedure
Men having experienced an ACS were recruited for participation (n = 61) at hospital discharge from cardiac wards and CR centres in the province of New Brunswick, Canada. Additionally, patients were referred by their family doctor or cardiologist. Those who accepted to participate were contacted by a research assistant to schedule in-person meetings. Baseline data were collected between 1- and 8-weeks post-ACS and follow-up data were collected at 3-, 6-, 9-, and 12-months post-ACS. Inclusion criteria for participation in the MindTheHeart® project were being over the age of 19, having an ACS diagnosis or having undergone cardiac surgery in the last 3 months, ability to speak or write in English or French, having a treating health professional (cardiologist, family doctor or nurse practitioner), and being available for follow-ups for a minimum of a year. ACS diagnosis includes MI (NSTEMI and STEMI), UA, angioplasty (with or without a stent or coronary bypass) or having been a congenital heart patient in the last 3 months. Cardiac surgery includes but is not limited to coronary artery bypass graft (CABG), percutaneous valve procedures, valve graft or cardioverter-defibrillator implantation. An additional inclusion criterion for the present study was being in a relationship. Exclusion criteria for participation in the MindTheHeart® project were abuse of substance in the last year, history of psychotic disorders or bipolar disorders, and not having received psychotherapy or pharmacological treatment for MD, AD, or TRS in the last 3 months. An additional exclusion criterion for the present study was having participated in Step 2 and/or Step 3 of the stepped-care psychological intervention. Prior to participation in the MindTheHeart® project, participants provided written informed consent for their data to be used in secondary analyses. The present study has been approved by the research and ethics committee of the Université de Moncton (approval #2122-065).
Measures
Relationship satisfaction
The complete 32-item version of the Couples Satisfaction Index (CSI-32, Funk and Rogge, 2007) was used to assess self-reported relationship satisfaction. The first item, “Please indicate the degree of happiness, all things considered, of your relationship”, is answered on a seven-point Likert scale ranging from 0 (“extremely unhappy”) to 6 (“perfect”). The following 24 items are answered on a six-point Likert scale ranging from 0 (ex. “always disagree”) to 5 (ex. “always agree”), and the final seven items require the participant to describe how they feel about their relationship using a six-point semantic differential scale ranging from 0 (ex. “boring”) to 5 (ex. “interesting”). Total marital satisfaction is calculated by summing the scores of all 32 items and can range from 0 to 161. Higher scores indicate higher levels of relationship satisfaction while lower scores indicate lower levels of relationship satisfaction. A CSI-32 total score of less than 104.5 indicates notable relationship dissatisfaction. The CSI has demonstrated strong psychometric properties and convergent validity with other relationship satisfaction measures (Funk and Rogge, 2007). Cronbach’s alpha coefficients of the CSI-32 in this study vary from 0.97 to 0.99 depending on data collection times. These values are similar to those of previous studies.
Depression and anxiety
The Depression, Anxiety and Stress Scale (DASS-21, Lovibond and Lovibond, 1995) was used to assess self-reported depression and anxiety symptoms. The DASS-21 requires participants to indicate how much the 21 statements applied to them over the past week (ex. “I tended to over-react to situations”), with answers being measured on a four-point Likert scale ranging from 0 (“Did not apply to me at all”) to 3 (“Applied to me very much or most of the time”). The DASS-21 measures symptoms of depression and anxiety as well as symptoms of stress. For that reason, it is divided in three subscales of seven items each, and a total score is calculated for each respective subscale. In this study, the stress subscale was not used. The DASS-21 scores are multiplied by two so that they can be compared to the complete, 42 item version of the scale. Total scores allow researchers to differentiate between normal (depression: 0–9, anxiety: 0–7), mild (depression: 10–13, anxiety: 8–9), moderate (depression: 14–20, anxiety: 10–14), severe (depression: 21–27, anxiety: 15–19), and extremely severe (depression: 28+, anxiety: 20+) levels of symptomatology. The DASS-21 has been widely used in clinical settings and has shown excellent validity and reliability (Osman et al., 2012). Cronbach’s alpha coefficients of the DASS-21 in this study vary from 0.84 to 0.93 depending on data collection times.
Socio-demographic characteristics
At the baseline data collection, participants were required to complete a short socio-demographic questionnaire with items relating to age, ethnicity, sexual orientation, marital status, level of education, household income, and employment status. Moreover, at each data collection, participants were required to answer questions relating to health behaviours (smoking, physical activity, eating habits, and drug and alcohol use), insurance coverage, participation in a CR program, and overall health state.
Statistical analyses
All statistical analyses were conducted using SPSS version 27.0. Descriptive statistics were used to present socio-demographic and clinical characteristics. A multivariate analysis of variance was conducted to compare the participants who dropped out of the study to those who remained in the study. Pearson’s correlation analysis was used to test correlations among the main study variables (relationship satisfaction, depression symptoms, and anxiety symptoms). Following these analyses, we conducted a series of paired-sample t-tests to compare levels of depression and anxiety symptomatology throughout the data collections. Time intervals demonstrating significant changes in symptomatology were further analyzed using hierarchical linear regression. A two tailed p-value smaller than 0.05 indicated the presence of statistical significance for all the above-mentioned statistical analyses.
Data sharing statement
The current article includes all research data collected in the study including SPSS raw dataset, SPSS syntax files, SPSS output files, and an explanatory memo. All of the files will be uploaded to the Figshare repository.
Results
Evolution of the sample
Participants’ socio-demographic and clinical characteristics (n = 50).

Note. Surgical treatments included coronary artery bypass graft (CABG) and non-surgical treatments included angioplasty (with or without stents) and cardioverter-defibrillator implantation.

Participants flow chart.
Sample characteristics
Table 1 displays a summary of the socio-demographic and clinical characteristics of the baseline study participants (n = 50). The mean age for participants is 64.90 years (SD = 9.52 years) and all participants are in a heterosexual relationship. Ninety-two percent reported being married and the other eight percent reported living common law. Most participants (96%) had been diagnosed with an ACS while the remaining two had an aortic dissection or a ventricular tachycardia. All participants completed Step 1 of the stepped-care psychological intervention and did so within the T0 to T1 time interval.
Correlations among study variables
Descriptive statistics and Pearson’s correlations for study variables.
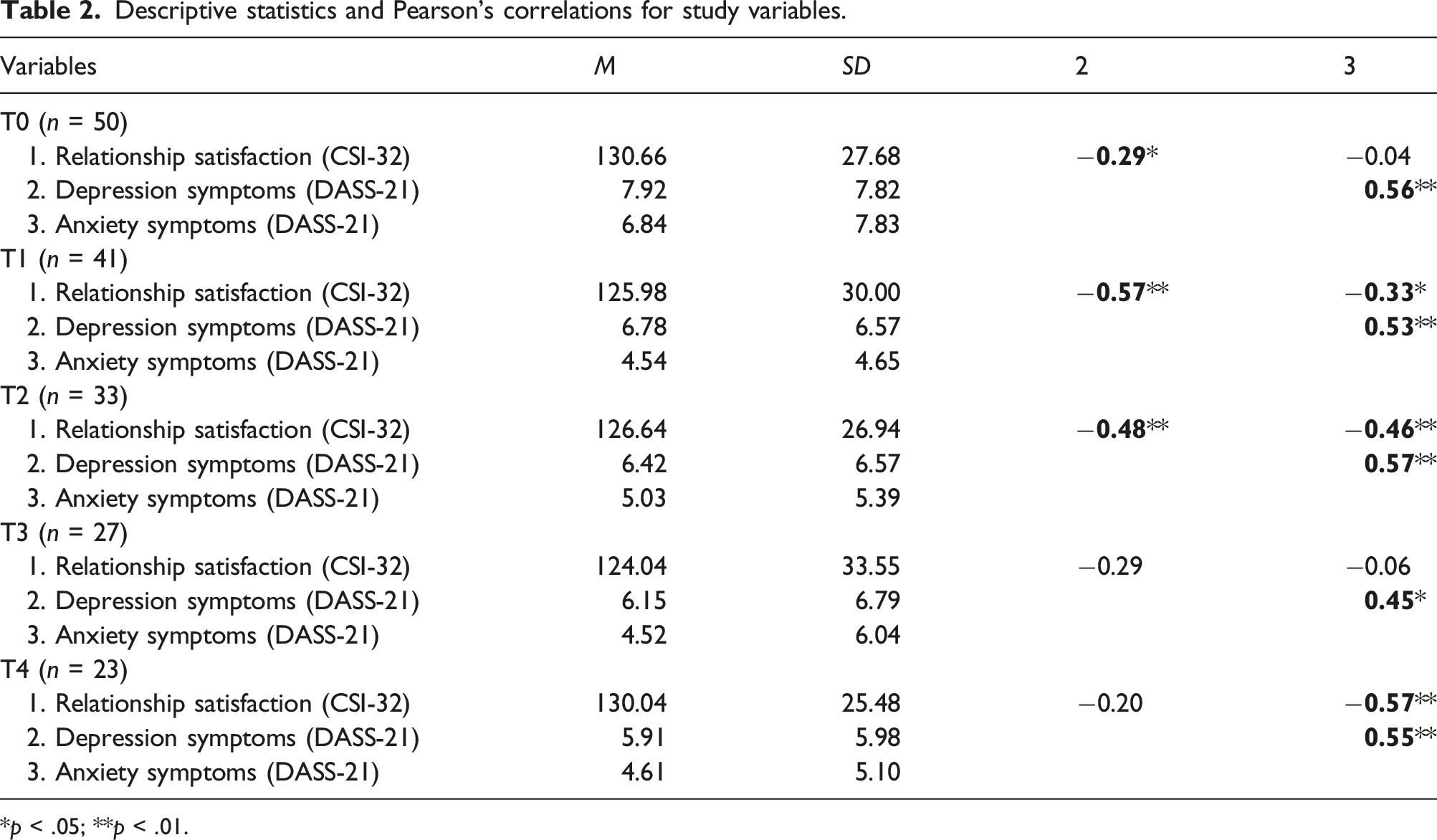
*p < .05; **p < .01.
Changes in depression, anxiety, and relationship satisfaction throughout the 12 months of follow-ups
A series of paired-sample t-tests were conducted to compare depression, anxiety, and relationship satisfaction between each follow-up measure (i.e. T0-T1, T1-T2, T2-T3, T3-T4) as well as between the first and last measures (i.e. T0-T4). For depression, there is a significant improvement in symptoms from T0 (M = 8.63, SD = 8.28) to T1 (M = 6.78, SD = 6.57); t (40) = 2.20, p = 0.03. More specifically, 22 participants (54%) had an improvement in symptoms of depression from T0 to T1. This improvement resulted in a change of clinical category for 11 participants (moderate to normal: 2, mild to normal: 4, severe to mild: 1, severe to moderate: 3, and extremely severe to moderate: 1). The other 11 participants remained in the same clinical category from T0 to T1 despite their improvement in symptoms (normal: 10 and moderate: 1). For the remaining 19 participants, changes in levels of depression were non-significant. For anxiety and relationship satisfaction, there are no significant changes in scores between any of the follow-up measures and between the first and last measures. However, there is a notable decrease in mean scores of anxiety from T0 (M = 6.29, SD = 1.14) to T1 (M = 4.54, SD = 0.73), as well as between T0 (M = 6.17, SD = 1.67) and T4 (M = 4.61, SD = 1.06).
Relationship satisfaction as a predictor of improvement in depressive symptoms in men having received an early, post-ACS couple-focused and men-tailored psychoeducation intervention
Results of the hierarchical regression predicting depression at T1 (n = 41).

*p < 0.05; **p < 0.01; ***p < 0.001.
Participants depression symptoms at T0 significantly predict their depression symptoms at T1 F (1, 39) = 53.12, p = 0.00, R2 = 0.58, R2 Adjusted = 0.57. Adding socio-demographic and clinical variables in the second step does not improve the prediction of depression symptoms at T1 F sequential (6, 33) = 1.30, p = 0.28. In the third step, we do observe an improvement of the prediction of depression symptoms at T1 F sequential (1, 32) = 7.84, p = 0.01. Relationship satisfaction at T0, beyond depression symptoms at T0 and a variety of socio-demographic and clinical variables, explains 7% of the variance in depression symptoms at T1. In the final model, three of the variables (depression symptoms at T0, education level and relationship satisfaction at T0) significantly account for the variance in depression symptoms at T1. In terms of the unique variance accounted for by each variable, depression symptoms at T0 accounts for 58% (part r2 = 0.576), education level for 5% (part r2 = 0.049) and relationship satisfaction at T0 for 7% (part r2 = 0.067). In sum, the linear combination is significant with the insertion of relationship satisfaction at T0 in the third step F (8, 32) = 10.55, p = 0.00. The final model explains 73% of the variance in depression symptoms at T1 (R2 Adjusted = 0.66).
Discussion
The purpose of this study was to gain a better understanding of the associations of relationship satisfaction, depression, and anxiety over a 12-month follow-up period in men having completed an early, post-ACS couple-focused and men-tailored psychoeducation intervention. The first key finding is the significant improvement in depression symptoms from T0 to T1, that is, from approximately one to 8 weeks post-ACS to 3 months post-ACS. As previously mentioned, all 50 study participants completed the MindTheHeart® psychoeducation intervention within the T0 to T1 time interval. It is possible that the initial improvement in depression symptoms may have been a result of participation in the intervention, however, the design of the current study prevents us from drawing such conclusions.
Despite this limitation, research indicates that many psychoeducation intervention programs are successful in reducing post-ACS anxiety and depression (Cojocariu et al., 2021; Fernandes et al., 2017). Unique benefits of the MindTheHeart® intervention are that it is structured to meet the needs of male patients specifically, and that it strongly encourages life partner involvement. In fact, during the second psychoeducation session, life partners received their own guide containing strategies on how to positively influence their partner’s post-ACS rehabilitation. Of note is that Fernandes et al. (2017), using a control group, concluded that patients having undergone an in-hospital psychological intervention had significantly lower levels of anxiety and depression at hospital discharge. While such patients showed a linear decrease in anxious and depressive symptoms over time, the patients in the control group presented higher levels of anxiety and depression with time, especially 2 months after hospital discharge (Fernandes et al., 2017). Despite Fernandes et al.’s slight structural differences in the psychological intervention (i.e. two one-hour sessions and one follow-up 2 months later), the early improvement of depression in the experimental group is consistent with our findings. Representing greater mental stability in patients, the gradual improvement in depression scores could explain why we did not identify any significant changes in symptomatology beyond T1.
It is important to consider that the improvement in depression symptoms may have occurred with the simple passage of time. Notably, researchers have documented that early depressive symptoms resolve, for many patients, within the first few months after hospital discharge (Murphy et al., 2020). Again, the uncontrolled nature of the current study prevents us from determining whether patients’ depression scores simply improved with time, through greater understanding of the implications of ACS, for example. Interestingly, research shows that approximately one third of patients still present symptoms of depression between 6 and 12 months post-ACS (Murphy et al., 2020). Thus, early interventions like the MindTheHeart® psychoeducation intervention may be particularly effective for patients with persistent symptoms or patients at risk of a deterioration in psychological health. This hypothesis would be worth testing in future studies with the use of a control group.
Although not statistically significant, our T0 and T4 measure comparisons (i.e. baseline and 12-months post-ACS) also show an improvement trend in depression and anxiety symptoms. These findings are consistent with Yohannes et al.’s (2010) study that found that the beneficial effects of a 6-week CR program on depression and anxiety were maintained at the 12-month follow-up. As in our study, their CR program included a psychological component targeting coping strategies as well as education about ACS. Our smaller sample size at T4 (n = 23) may have contributed to the absence of statistical significance. Another explanation could be that potential effects of the MindTheHeart® psychoeducation intervention fade over time and thus knowledge reactivation sessions (ie., booster sessions) may be beneficial to help maintain gains. Again, a two-arm clinical trial would be required to confirm this hypothesis.
In addition, we found that relationship satisfaction and depression symptoms were significantly and negatively correlated at T0, T1 and T2 and that the correlation was strongest at T1. A similar pattern of results was obtained in Dekel et al.’s (2014) study indicating that the higher men’s marital satisfaction is at the time of their hospitalization, the fewer depressive symptoms they have at that time, as well as 6 months post-ACS. It is curious that relationship satisfaction and depression symptoms were not significantly correlated beyond T2 in our study. However, we note that relationship satisfaction levels were stable over time, with mean scores ranging from 124 to 131 and median scores ranging from 134 to 137 out of a total of 161. This general stability in patients’ relationship satisfaction may have facilitated their post-ACS adjustment and contributed to their improvement in depressive symptoms over time. From this standpoint, patients could have developed a stronger psychological state that is less dependent of the benefits of relationship satisfaction.
There seems to be very little research on the links between relationship satisfaction and anxiety symptoms in men with ACS. Whereas depression has been considered a risk factor for ACS, researchers cannot agree on anxiety’s role (Ossola et al., 2018). In this study, we found that relationship satisfaction and anxiety symptoms were significantly and negatively correlated at T1, T2 and T4 and that these correlations became stronger with time. Examining the data longitudinally, we did not observe a linear improvement in anxiety symptoms. In fact, mean anxiety scores increased and decreased consecutively throughout follow-up measures (MT0 = 6.84, MT1 = 4.54, MT2 = 5.03, MT3 = 4.52, MT4 = 4.61). Of note, depression and anxiety symptoms were strongly and positively correlated across the study. This is important to highlight as the cooccurrence of depression and anxiety complicates diagnosis and treatment, predicts poorer outcomes, and is associated with a higher rate of treatment resistance (Coplan et al., 2015). Our finding provides further support for the identification of patients at risk of mental health comorbidity in the weeks following an ACS to provide them more complex and appropriate treatment.
The final part of our study looked at whether patients’ relationship satisfaction at T0 could be an important predictor for their improved depression symptoms at T1. We found that relationship satisfaction at T0, beyond depression symptoms at T0 and a variety of socio-demographic and clinical variables, explained 7% of the variance in depression symptoms at T1. This last finding suggests that self-rated relationship satisfaction is an important variable in terms of understanding men’s depression symptoms early on in their ACS recovery process. Our result supports the argument for examining various types of relationships (e.g. same sex couples, younger couples, etc.) as well as the constructs underlying relationship satisfaction. For example, the relationship satisfaction measure used in this study (CSI-32) assessed participants’ degree of happiness in the relationship, the extent of agreement or disagreement with their partner, as well as feelings, perceptions, and thoughts about the relationship. Subsequently, it is plausible that the development of an intervention to target these specific characteristics may be of benefit for male ACS patients. In the case of the MindTheHeart® psychoeducation intervention, an important component of couple relationships that was targeted is sexual intimacy. Indeed, patients and their partner received advice on how to regain a healthy sex life, among other strategies. The degree of success of this approach would need to be evaluated in another study. Moreover, given the potential for a bidirectional association between the variables, additional research should examine the link between initial depression and change in relationship satisfaction. Lastly, it is worth emphasizing that our findings regarding relationship satisfaction as a predictor of improvement in depressive symptoms derive from the male patient’s perspective exclusively, rather than both partners in the couple. We advocate that patient perspectives are key to understanding how patients experience CR programs as well as how treatments in turn affect their psychological health.
It is important to note that the results of this study are preliminary in nature and should be corroborated in future studies, while also considering the following limitations. First, the small sample size and the absence of a control group limit the power of the statistical analyses as well as the reliability and generalizability of the results. More research is needed using larger samples to consolidate the findings of the present study. Additionally, due to the absence of manipulation, results should be interpreted with caution and do not indicate that relationship satisfaction is the cause of improvement in depression symptoms. Second, the sample consisted of predominantly Caucasian men who are all in a heterosexual relationship. Third, the exclusion of patients who were not in a relationship may have created a sample of participants with rather active and involved life partners, thereby leading to a selection bias. A final limitation of the current study is the sole use of a self-report measure to assess relationship satisfaction. Psychosocial research on heart disease commonly assesses relationship quality and satisfaction through self-report measures (Smith and Baucom, 2017), and this may not be the best approach. One explanation for this is that patients of coronary heart disease have a tendency to minimize or deny their emotional struggles (Smith, 2022). The combined use of behavioural observation and experience sampling (Smith and Baucom, 2017) would have been more appropriate for the current study and should be prioritized in future research.
Despite these limitations, this study provides initial data about the way in which relationship satisfaction links to depression and anxiety in men having participated in an early, post-ACS couple-focused and men-tailored psychoeducation intervention. The findings suggest there may be a potential benefit of involving life partners in early, post-ACS interventions and also strengthen the need for future studies to be conducted among female patients, given the current knowledge gap. Given the existing differences between men and women as it relates to the risk and clinical presentation of psychological disorders following ACS, further studies investigating both sexes are needed to determine the most effective and appropriate interventions. Future research could also explore the need for gender sensitiveness within psychoeducation interventions for ACS patients as well as the need for different types of interventions depending on the type of couple (e.g. same sex couples, couples with low relationship satisfaction, couples with high relationship satisfaction, etc.). Studies of this nature could help maximize the psychological and social functioning of a wider range of patients. Given the high prevalence of ACS, its deleterious impact on men’s mental and physical health, and its significant associated costs, improving patient outcomes through early access to men-sensitive psychoeducation can have considerable benefits.
Footnotes
Acknowledgments
The authors would like to thank Mylène Lachance-Grzela for her help with the revision, Marc Harper for his help with the bibliographic research, and Salah-Eddine El Adlouni for his help with the statistical analysis plan. Additionally, we would like to thank the MindTheHeart® research team for data acquisition as well as all the participants who graciously accepted to share their information. Dr. Jbilou received administrative and logistic support from the Centre de Formation Médicale du Nouveau-Brunswick to carry out the MindTheHeart® project.
Declaration of Conflicting Interests
The author(s) declared that there are no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Drs. Jbilou, Greenman, Grenier, and Chomienne received funding for the MindTheHeart® project from the Movember Foundation - Canada (2015) and the New Brunswick Health Research Foundation (Strategic Initiative Grant program - 2016). Mrs. Barriault received a master’s scholarship from the New Brunswick Government (Bourse d’études supérieures du Nouveau-Brunswick) and the University of Moncton (Bourse d’études supérieures de l’Université de Moncton - Campus de Moncton) to carry out the present study. Dr. Jbilou discloses finacial support for publication of this work from the Centre de Formation Médicale du Nouveau-Brunswick.