
Abstract
The unparalleled speed of COVID-19 vaccine development has necessitated an expansion of existing knowledge on vaccination decision-making. The current study explored (1) how cognitions and emotions shaped college students’ COVID-19 vaccination decisions, and (2) where vaccination-inclined and vaccination-hesitant students converged and diverged in their decision-making process. Seventy-seven students participated in 26 focus groups to discuss their complex thoughts and feelings regarding COVID-19 vaccination, offering a more nuanced understanding of COVID-19 vaccination decision-making that has not been fully captured by quantitative studies. Thematic analysis found that vaccination-inclined participants and their hesitant counterparts reported differential patterns of positive and negative emotions, systematic appraisals, and heuristics in decision-making. Future research should investigate the roles of hope and relief, non-health-related benefits of vaccination, social trust, and interpersonal influence in vaccination decision-making.
Keywords
Introduction
Among adults in the United States, young adults aged 18–24 years have the lowest vaccination coverage against COVID-19 compared to the other age groups (CDC, 2022). One place where young adults congregate is the campus of a higher education institution. Research suggests that college campuses can become hotspots of the COVID-19 pandemic when in-person classes are held without a vaccinated student body and rigorous disease control measures (Lu et al., 2021b). Furthermore, on-campus outbreaks can spread rapidly to nearby communities and other population segments (Leidner et al., 2021; Walke et al., 2020). It is therefore critical to develop strategies to encourage COVID-19 vaccination among college students in order to address the ongoing pandemic, and an essential first step to accomplishing this goal is to understand what shapes their vaccination decisions.
Research on COVID-19 vaccine acceptance among college students has been growing. To date, most studies on this topic rely on survey instruments developed based on a review of research conducted during previous outbreaks or in relation to vaccination against other diseases (e.g. seasonal influenza, HPV infection) (Graupensperger et al., 2021; Kecojevic et al., 2021). However, these predetermined instruments might not fully capture the complex, novel, and unique thoughts and feelings elicited by an unprecedented pandemic. While valuable insights from extant research should be acknowledged, it is helpful to reconsider their application to COVID-19, given the extraordinary scale, duration, and impact of this pandemic, as well as the unparalleled speed with which the COVID-19 vaccines have been developed and authorized for large-scale use. To this aim, the current study explores the most salient thoughts and feelings underlying college students’ COVID-19 vaccination decisions through 26 semi-structured focus group discussions. Using research protocols informed by established theories on health decision-making and through a thematic analysis approach, this research also seeks to identify where vaccination-inclined and vaccination-hesitant college students converge and diverge in their decision-making process.
Social cognition and COVID-19 vaccination
Social cognitive factors are key to shaping health decisions according to prominent theories, such as the Health Belief Model (HBM) (Rosenstock et al., 1988), Theory of Planned Behavior (TPB) (Ajzen, 1991), and Protection Motivation Theory (PMT) (Maddux and Rogers, 1983). According to these frameworks, the decision to engage in a preventive behavior results from an elaborate but subjective analysis (Conner and Norman, 2015). Central to this analysis are the benefits and costs associated with an action. In studies conducted during previous pandemics (e.g. H1N1 and SARS pandemics), perceived benefits of a mitigation measure were often conceptualized in terms of its “response efficacy,” or how far individuals felt that acting this way would protect them from disease (Bish and Michie, 2010). However, when it comes to the preventive behavior of vaccination, research has suggested that individuals’ decision-making might be motivated by the belief that vaccinating themselves would also help safeguard the health of their loved ones (Huang and Li, 2021) or the community at large (Trueblood et al., 2021; Chu and Liu, 2021). In relation to COVID-19 vaccination, an additional layer of consideration is the possibility of returning to a less restrictive and more normal life once higher vaccination coverage and greater community resistance to the disease have been achieved. Informed by these observations, the current project delved into what types of benefits (e.g. self- or other-related benefits; health or non-health benefits) were most frequently reported by college students as part of their vaccine decision-making process.
In health decision-making, the benefits of a preventive behavior are typically weighed against its costs (e.g. physical, psychological, and financial barriers that prevent an individual from taking action) (Conner and Norman, 2015). Closely related to perceived costs are the concepts of “self-efficacy” (Rosenstock et al., 1988; Maddux and Rogers, 1983) and “perceived behavioral control” (Ajzen, 1991), both referring to people’s beliefs in their own capability to overcome obstacles and find the necessary resources to perform a behavior. Regarding COVID-19 vaccination, research conducted during the early stages of the pandemic indicated that safety concerns or concerns over adverse effects, would constitute a strong predictor of hesitancy (Al-Amer et al., 2021; Chu and Liu, 2021). On the other hand, acceptance is associated with the beliefs that getting vaccinated against COVID-19 is within one’s control, and that one can overcome the barriers to vaccination (Guidry et al., 2021). The current study explored whether college students’ perceptions of major barriers to COVID-19 vaccination a year into the pandemic were similar to the concerns identified through general population surveys early on. It also offered an opportunity for young adults to articulate their sense of self-efficacy (or the lack thereof) in overcoming barriers to get vaccinated.
Engagement with preventive behaviors can also be motivated by people’s heightened risk perceptions, which are often discussed in terms of “perceived susceptibility” (i.e. how likely one is to get ill), “perceived severity” (i.e. how serious the resulting illness would be), and “perceived threat” (i.e. a combination of the previous two constructs) in extant literature (Maddux and Rogers, 1983; Rosenstock et al., 1988). However, risk perceptions have not consistently served as a predictor of COVID-19 mitigation behaviors (Chu and Liu, 2021; Al-Amer et al., 2021; Guidry et al., 2021; Fullerton et al., 2021). For college students, the relationship between risk perceptions and preventive actions might be further complicated by the fact that young adults tend to underestimate their vulnerability to health threats (Masiero et al., 2018). It is therefore of interest to explore how common such optimistic bias is when college students discuss their COVID-19 vaccination decisions.
How individuals assess the social context for a health behavior can also affect decision-making (Conner and Norman, 2015; Chu and Liu, 2021). To begin with, our social environment is full of “cues to action” (Rosenstock et al., 1988) that motivate us to act, such as vaccination reminders from the mass media or from healthcare providers. Our action can also be shaped by “subjective norms” or approvals of a behavior from close others (e.g. family or friends) (Ajzen, 1991). In the context of COVID-19, it is equally important to consider the abundance of misinformation (i.e. false information shared by people who do not intend to mislead others) and disinformation (i.e. false information deliberately created and disseminated with malicious intent) in one’s surroundings that might result in ample “cues to objection” and messages of disapproval from significant others regarding preventive behaviors (CDC, 2021). Reflective of these opposing forces, research has suggested that individuals tend to be more hesitant toward COVID-19 vaccination when their information sources are dominated by communication from social media and conservative cable news networks (Viswanath et al., 2021; Ruiz and Bell, 2021). On the other hand, when individuals receive and trust information from public health agencies and healthcare providers, they are more likely to get vaccinated against COVID-19 (Purvis et al., 2021). Expanding upon this line of inquiry, the current study examined not only college students’ communication environment regarding the COVID-19 vaccines, but also potential reasons as to why they trusted or distrusted particular information sources about vaccines.
Emotion and COVID-19 vaccination
Emotions can influence information processing relevant to decision-making, and can further influence the extent to which individuals engage in systematic cost–benefit analysis during decision-making (Ferrer and Ellis, 2019). Various models, such as the extended parallel process model (Witte et al., 2001), cognitive-functional model (Dillard and Nabi, 2006), and appraisal tendency framework (Lu et al., 2021a) have been developed to explicate how various emotions are functionally linked with different types of cognitive appraisals (e.g. systematic vs. heuristic) and action tendencies (e.g. approach vs. avoidance), which in turn lead to particular health behavior patterns. In the context of COVID-19, researchers have identified which emotions were likely to be experienced by individuals during a health crisis, and then quantitatively examined the relationships between these emotions and preventive behaviors (Liao et al., 2021; Chu and Liu, 2021; Broodryk and Robinson, 2021). However, there is a scarcity of qualitative studies in which participants could report their emotions freely, or that explore individuals’ emotions regarding a particular mitigation measure (e.g. vaccination) rather than the pandemic itself. These are significant gaps to address, as the unparalleled nature of the COVID-19 pandemic might elicit a greater range of emotions, and the controversy surrounding the COVID-19 vaccines can also arouse many strong feelings. The current study therefore explored how emotions directed at different targets (i.e. pandemic and vaccines) would help shape COVID-19 vaccination decisions.
Given the unprecedented nature of the COVID-19 pandemic, the aims of the current study were to validate and expand upon existing research findings on the role of emotions, cognitions, and information sources in shaping individuals’ preventive behaviors. Specifically, the study explored the following research questions: • How do cognitions and emotions work in tandem to shape college students’ COVID-19 vaccination decisions? • Do vaccination-inclined and vaccination-hesitant students express similar or different thoughts and feelings when discussing their decision-making process? • What are the major sources of COVID-19 vaccine information trusted by college students? • Do vaccination-inclined and vaccination-hesitant students rely on similar or different sources?
Method
Participants
Three-hundred and eighty-one undergraduate students were recruited from two universities, one in California and another in Texas. Institutional Review Board approval was obtained from both universities. The students were recruited via flyers posted on campus or by signing up to serve as research participants through the online SONA participant pool management software from March 22 through April 26, 2021. Students were eligible for the study if they had not received the COVID-19 vaccine and had not been diagnosed with COVID-19. Participants were excluded if they had received the COVID-19 vaccine or were diagnosed with COVID-19, as research demonstrates that having been vaccinated against a disease can change individuals’ evaluation of their disease risk and inclination to engage with preventive behavior (Brewer, 2007). Similarly, having received a diagnosis might considerably change how a person assesses the benefits and risks of COVID-19 vaccination. Therefore, a decision was made to focus on those who have been neither vaccinated nor diagnosed to avoid complexity in interpreting the research findings.
One-hundred and forty-four of the 381 students were eligible to participate, and all participants provided informed consent via Qualtrics. Of the 144 students, partial data were obtained for 67 students because they either had not completed the online survey questions or dropped out before completing the focus group discussion. Hence, the final sample for the analyses was 77 students (34 females, 42 males, and 1 who declined to specify). The mean age of the participants was 23.76 years (SD = 7.05). The sample was ethnically diverse: 42 students identified as Latino(a)/Hispanic, 17 were non-Hispanic Caucasian, 8 were bi- or multiracial, 2 were African American, 2 were Asian, 1 was Native Hawaiian or other Pacific Islander, and 5 specified other or preferred not to disclose. Fifty-two of the participants were from California, whereas the other 25 participants were from Texas.
Measures and procedure
All eligible participants completed an online 10-item survey consisting of sociodemographic questions and an additional item asking what they would do when the COVID-19 vaccine became available to them (see Appendix 1 for a full list of the survey items). Participants were asked to choose from six Likert-scale options ranging from “get any vaccine as soon as you can” to “definitely not get it.” Individuals who chose the first two options were subsequently classified as vaccination-inclined and those who selected the last three options were classified as vaccination-hesitant. For participants who indicated that they would “wait and see” on the screening survey, this sample was further asked to elaborate on their decision about COVID-19 vaccination. Many of them reported a willingness to get vaccinated in the near future or the intention to ultimately get the vaccine, even though they did not have a timeline in mind. A few participants were more ambivalent and expressed a desire to continue to monitor the situation at that time. Because the majority of the “wait-and-see” participants planned on getting vaccinated at some point, a decision was made to classify them as vaccination-inclined.
Composition of vaccination-inclined and vaccination-hesitant focus groups.

Our decision to use focus groups rather than surveys or other quantitative research instruments was based on a desire to acquire an in-depth understanding of “people’s own meanings” (Wilkinson, 1998: 331) and experiences with the COVID-19 pandemic and COVID-19 vaccination, both of which could be considered unprecedented developments for many. As a result, it was appropriate to allow individuals more space to elaborate on their thoughts and feelings in a discussion setting to see if new patterns emerge. Focus groups also allowed the moderator to probe into any interesting comments shared by the research participants. Furthermore, in order to create a more comfortable and less intimidating environment for focus group participants to share their thoughts and feelings candidly, we followed the common practice of separating individuals into different groups (i.e. vaccination-inclined vs. vaccination-hesitant groups) based on similarities in their attitudes or experiences (Wilkinson, 1998).
Each participant was assigned a pseudonym that was recorded with their data and used during the focus group discussion. The focus group discussions were conducted and video recorded via Zoom. Participants had the option to turn off their camera during the focus groups. Each focus group session lasted between 40 to 60 min and included two to five participants and a moderator (one of the investigators). After each focus group, participants were provided incentives. For those recruited through SONA, research credits were granted to fulfill psychology program research requirements. Those recruited through flyers were given extra credit for volunteering their time and effort. Below is a list of the focus group prompts: Think about 3 words that describe your feelings about the COVID-19 outbreak in the United States during the past year, and enter them in the chat. Share your feelings about the COVID-19 outbreak in the United States, and tell us why you feel this way. Think about 3 words that describe your feelings about the COVID-19 vaccine, and enter them in the chat. Share your feelings about the COVID-19 vaccine, and tell us why you feel this way. Tell me what you would do when the vaccine becomes available to you, and the reason behind your decision. What are the top one or two benefits for you to get vaccinated against COVID-19? What are the top one or two concerns that you have about getting vaccinated against COVID-19? Is there anything else about your personal background that is impacting your decision to get vaccinated or not get vaccinated against COVID-19? When I say background, I mean your spiritual or religious beliefs, race, ethnicity, language, gender, being an immigrant, or being a college student, experiences of unfair treatment or discrimination, etc. Think about three sources from which you have most frequently received information about the vaccine. These can be sources that you either agree or disagree with, and they can range from mainstream media outlets to social media platforms or from specific persons to certain organizations. Please enter them in the chat. Tell me your most trusted source for information related to the COVID-19 vaccine. Why do you trust this source of information? Share with me a source that you have little or no trust in when it comes to information related to the COVID-19 vaccine. Why don’t you trust this source of information?
Given our interest in exploring how emotions, cognitions, and information sources shaped college students’ COVID-19 vaccination intention, questions 1 to 4 in our focus group protocol were designed to provide an in-depth understanding of participants’ feelings toward the COVID-19 pandemic and COVID-19 vaccination. Questions 4 to 7 asked participants to elaborate on the cognitions and thought processes beyond their decision to get vaccinated against COVID-19 or not. Question 8 offered an opportunity for discussing additional personal background factors that influenced participants’ vaccination decision-making. Lastly, questions 9 to 11 gave participants an opportunity to share their main sources of information on COVID-19 vaccination and reflect on why they trusted certain sources and distrusted others.
As noted in focus group questions 1 and 3 above, participants were initially asked to type in their feelings toward the pandemic and the COVID-19 vaccine in the chat. The chat responses were then used to facilitate participant discussion about what feelings or words they used, and why. The chat feature was only used for these two questions to help participants gather their thoughts before they were asked to expand on their responses. In order to ensure the originality of participants’ initial responses, they were asked to type in their answers in the chat but hold off pressing the “enter” button until everyone has finished typing in their response. Interaction between participants was then allowed, when they elaborated on their initial responses orally and reflected, agreed, or disagreed with what others had to say.
The focus group discussions were then transcribed by six research assistants. To ensure consistency in transcribing interview sessions, a training session was conducted by one of the authors (H.L.) who has expertise in qualitative methodology. Two research assistants were assigned to transcribe each interview; one assistant completed a transcript, and the other research assistant reviewed whether all interview content was accurately transcribed. If any discrepancy was detected, it was marked with time points so that coders could determine whether the discrepancy affected coding results.
Analysis
An initial reading of transcripts was conducted to extract coding schemes based on the theoretical framework of thematic analysis provided in Braun and Clarke (2006), Joffe (2012), and Terry et al. (2017). Three coders with expertise in clinical psychology (K.K., B.V.) or health communication (N.C.) read all 26 transcripts (i.e. familiarization) and extracted initial coding items for each interview question (i.e. generating codes). These items were then examined to detect systematic patterns for coding schemes (i.e. data reduction). Once three experts agreed on an initial code book consisting of coding schemes for all interview items (i.e. definitions of terms, instructions on relevant/irrelevant statements, and detailed examples), a coding facilitator with expertise in methodologies (H.L.) assigned two randomly selected transcripts to the three coders to check the following criteria: (1) whether all coders were on the same metric when analyzing interview data and interpreting the code book identically (i.e. coder reliability), and (2) whether there was any further need to revise coding schemes. After all three coders reached agreement on initial coding results from the two transcripts, the main coding process was subsequently conducted with a fourth coder (M.O.) to ensure rigor in analyses of interview data and minimize investigator bias as suggested in Elliott (2018). While the three primary coders were involved in the entire research process, including serving as a facilitator for focus group discussions, the fourth coder, with expertise in clinical psychology, was neither involved in any of the focus groups nor informed of the purposes of these discussions.
The final coding results were reached through a discussion about discrepancies in coding among four coders. If agreement was not obtained, averaged frequencies for corresponding coding items (e.g. behaviors/statements found in interview data) from the four coders were used. For intercoder reliability, Fleiss’ Kappa (Fleiss, 1971) was employed. Although percent agreement rates appear to be more intuitive, they lead to the overestimation of the true agreement because they do not consider random chance (guessing). Thus, Fleiss’ Kappa, a statistical measure that incorporates chance agreement was utilized to more accurately evaluate interrater reliability. The intercoder reliabilities, Fleiss’ Kappa values, showed fair to almost perfect agreement based on the criteria from Landis and Koch (1977), with positive Kappa coefficients ranging from 0.31 to 1.00 and the average was 0.81 across 324 coding items. Approximately 3% of coding items showed negative Kappa values. This typically occurs when only one coder identifies a relevant case, whereas the other coders do not. We emphasized consistency in coding as in all scientific investigations; however, the negative Kappa values should not be viewed as a flaw because researchers’ subjectivity should also be valued in qualitative paradigms and coder consistency should not be interpreted as “accuracy” in coding, as noted in Braun and Clarke (2006). Kappa coefficients were not available for some items due to nearly perfect or perfect agreement. Therefore, simple agreement rates were also reported (see Appendix 2 for intercoder reliability values and agreement rates for each coding item). The R package, irr (Gamer et al., 2019) was used for the interrater reliability analysis (see Appendix 3 for the R code).
The focus of the current study was to identify potential factors affecting an individual’s decision making on receiving a COVID-19 vaccine. Therefore, final themes were explored based on final coding results and an early thematic map was created (i.e. developing themes) (see Figure 1). Finally, a conclusion was provided with a final thematic map. The final thematic map was proposed by triangulating the quantitative patterns and qualitative responses supporting the patterns (i.e. reviewing and defining themes). Development of thematic maps.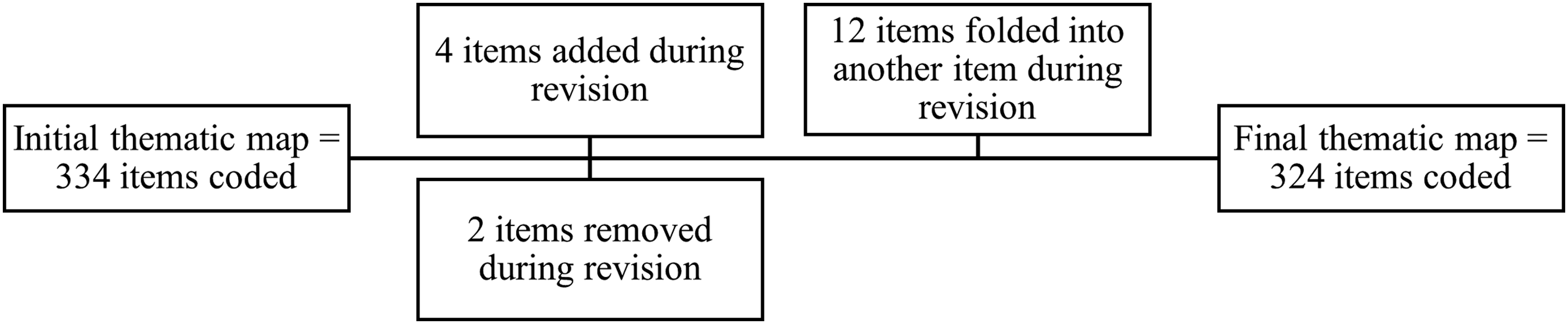
Results
The average frequency for each theme coded per focus group was computed. Further analysis was conducted to identify average frequencies per inclined focus group vis-à-vis per hesitant focus group in order to assess the similarities and differences between vaccination-inclined and vaccination-hesitant individuals (see Appendix 4 for a table summarizing average frequencies overall, and by vaccination inclination). Additional details are provided in the sections below to highlight and contextualize information in the summary table in Appendix 4.
Emotion and COVID-19 vaccination
Feelings toward the COVID-19 pandemic
Across the 26 focus groups, participants’ sentiments toward the COVID-19 pandemic were overwhelmingly negative (i.e. an average of 2.79 negative sentiments mentioned per focus group across all groups). Words related to the emotions of fear, worry, anxiety, and stress received the largest numbers of mentions, closely followed by terms related to the feelings of sadness, confusion, isolation, and frustration. When asked why they felt this way, three major explanations offered by participants were the human costs of the pandemic (1.19 mentions per focus group overall), its unprecedented nature (1.14 mentions), and uncertainty about the future (1.04 mentions).
Feelings toward COVID-19 vaccination
Regarding their feelings toward COVID-19 vaccines, inclined and hesitant groups demonstrated notable differences. On average, participants from the inclined groups expressed positive emotions at a greater frequency (2.25 mentions per inclined focus group) than negative emotions (2.12 mentions), whereas the reverse was true for participants from the hesitant groups (2.19 mentions of negative emotions and 0.93 mentions of positive emotions per hesitant focus group). Hope and relief were the most frequently mentioned positive emotions, whereas fear and confusion were the most commonly stated negative emotions. When elaborating on why they felt this way, many reported the benefits of COVID-19 vaccination for their positive feelings (2.00 mentions per inclined focus group; 0.63 mentions per hesitant group). Such benefits were mentioned relatively more than trust in the vaccine development process (0.53 mentions per inclined group; 0.04 mentions per hesitant group). On the other hand, risk associated with vaccination side effects (1.02 mentions per inclined group; 1.44 mentions per hesitant group) and distrust in the development process (1.06 mentions per inclined group; 0.89 mentions per hesitant group) constituted the most common themes when participants explained their negative feelings toward COVID-19 vaccination.
Social cognition and COVID-19 vaccination
General decision-making rationale: Appraisals of perceived benefits, costs, vulnerability of others, and uncertainty
Among vaccination-inclined participants, most stated that they would get any vaccine as soon as they can (1.71 mentions per inclined focus group), followed by those who said that they would wait and see how the vaccine is working for other people (0.84 mentions). Very few participants in this group (0.06 mentions) expressed a strong brand preference (i.e. they would only get their preferred brand of vaccine as soon as they can). In discussing their decision-making rationale, benefits associated with vaccination was the most frequently mentioned reason (0.98 mentions per inclined group by participants who would get any vaccine; 0.06 mentions by participants with a strong brand preference; 0.16 mentions by participants who would wait and see). The second most commonly expressed reason was perceived vulnerability of others (i.e. loved ones or community at large), with 0.55 mentions per inclined group by participants who would get any vaccine, 0 mentions by participants with a strong brand preference, and 0.14 mentions by participants who would wait and see.
Among the participants from the hesitant groups, most stated that they would get vaccinated only if required (1.37 mentions per hesitant focus group), followed by those who would definitely not get it (0.56 mentions), and then those who don’t know if they would get it (0.33 mentions). Risk associated with side effects was the most commonly stated rationale (0.33 mentions per hesitant group by participants who would get vaccinated only if required; 0.33 mentions by participants who would definitely not get vaccinated; 0 mention by participants who don’t know if they would get vaccinated). A general sense of uncertainty about currently available vaccines (e.g. “because it’s not approved yet” or “being unknown about what we’re taking in”) was the next commonly expressed reason (0.26 mentions per hesitant group by participants who would get vaccinated only if required; 0.26 mentions by participants who would definitely not get vaccinated; 0.26 mentions by participants who don’t know).
Perceived benefits and costs: Similarities and differences between vaccination-inclined and hesitant individuals
When prompted about the main benefits of COVID-19 vaccination, health-related benefits to oneself constituted the most popular theme in conversations with vaccination-inclined individuals (1.82 mentions per inclined focus group), closely followed by non-health-related benefits to oneself (e.g. “being able to go back to school,” “to start working again” or “have the ability to do things that we are restricted to do at the moment”; 1.51 mentions). Health-related benefits to family and friends were the third most common reason (1.14 mentions). For the hesitant participants, non-health-related benefits to oneself received the highest number of mentions (1.70 mentions per hesitant focus group), and this frequency was relatively high compared to the next recurrent theme, health-related benefits to oneself (0.78 mentions). Health-related benefits to family and friends were the third most popular reason (0.56 mentions).
When elaborating on their main concerns regarding the COVID-19 vaccines, risk associated with short-term or long-term side effects was the most common theme across inclined and hesitant individuals (2.54 mentions per inclined group; 1.93 mentions per hesitant group), followed by doubts over the effectiveness of the vaccine (0.50 mentions per inclined group; 1.00 mention per hesitant group). While the perceived costs and response efficacy of the COVID-19 vaccines appeared to be major barriers to receiving vaccination among college students, they as a group demonstrated a relatively high level of self-efficacy and only occasionally expressed concerns about logistic barriers (e.g. availability, financial costs) to getting inoculated (0.13 mentions per inclined group; 0.41 mentions per hesitant group).
Other decision-making factors: the role of interpersonal influence and personal health history
When asked about any other personal considerations that might impact their vaccination intention, interpersonal influence from significant others was a commonly stated factor (0.69 mentions per inclined group; 0.81 mentions per hesitant group). Sometimes, such influence was revealed to be based on others’ beliefs about the COVID-19 vaccines specifically. Other times, it was grounded on loved ones’ attitudes toward vaccination in general, broader views on science and medicine, or political and religious convictions. Another deciding factor mentioned by a considerable number of participants pertained to personal health history (0.43 mentions per inclined group; 1.00 mention per hesitant group), with some citing their perceived good health as a reason against COVID-19 vaccination, while others sharing negative experiences with previous vaccines or medications as a source of hesitancy.
Sources for COVID-19 vaccine information
Most trusted information sources
Domestic public health agencies (e.g. CDC, local public health departments) constituted the most trusted source of COVID-19 vaccine information for the inclined participants (1.24 mentions per inclined focus group), followed by interpersonal communication with family, friends, or acquaintances (0.82 mentions). For the hesitant counterparts, it was interpersonal communication that received the highest number of mentions as a trusted channel (1.52 mentions per hesitant focus group), followed by public health agencies (0.67 mentions). When prompted as to why they trusted these sources, expertise was the most frequently cited reason for public health agencies (0.39 mentions per inclined group; 0.22 per hesitant group), followed by the fact that they were government affiliated (0.47 mentions per inclined group; 0 mentions per hesitant group). For interpersonal communication, most participants explained that they found other people’s personal experiences or testimonials trustworthy (0.39 mentions per inclined group; 0.67 per hesitant group). The second most cited reason was the simple existence of personal relationships and goodwill (e.g. “they’re closely related to me, there’s that bond that we have,” with 0.18 mention per inclined group and 0.63 mentions per hesitant group).
Most distrusted information sources
Social media topped the list for distrusted information sources for both vaccination-inclined and hesitant individuals, followed by mass media (1.53 mentions per inclined group; 1.67 mentions per hesitant group). The most cited reason for not trusting social media was their unregulated nature (e.g. “there’s a lot of misinformation being spread and a lot of lies and whatnot”) (1.20 mentions per inclined group; 1.22 mentions per hesitant group). Lack of expertise was the second most cited reason for not trusting social media (0.43 mentions per inclined group; 0.22 mentions per hesitant group). Mass media ranked second as an untrustworthy information source (1.00 mention per inclined group; 1.11 mentions per hesitant group). Perceived bias was the most frequently stated reason for distrust in mass media (0.27 mentions per inclined group; 0.70 mentions per hesitant group). In addition, a number of participants perceived mass media as unregulated (0.41 mentions per inclined group; 0.11 per hesitant group) and considered them similar to social media (e.g., “those are both really on the same level…because you can get fake news from both of them”). To conclude, Figure 2 presents a graphical comparison of major findings from the vaccination-inclined versus vaccination-hesitant groups. Thematic maps for vaccination-inclined and vaccination-hesitant focus groups.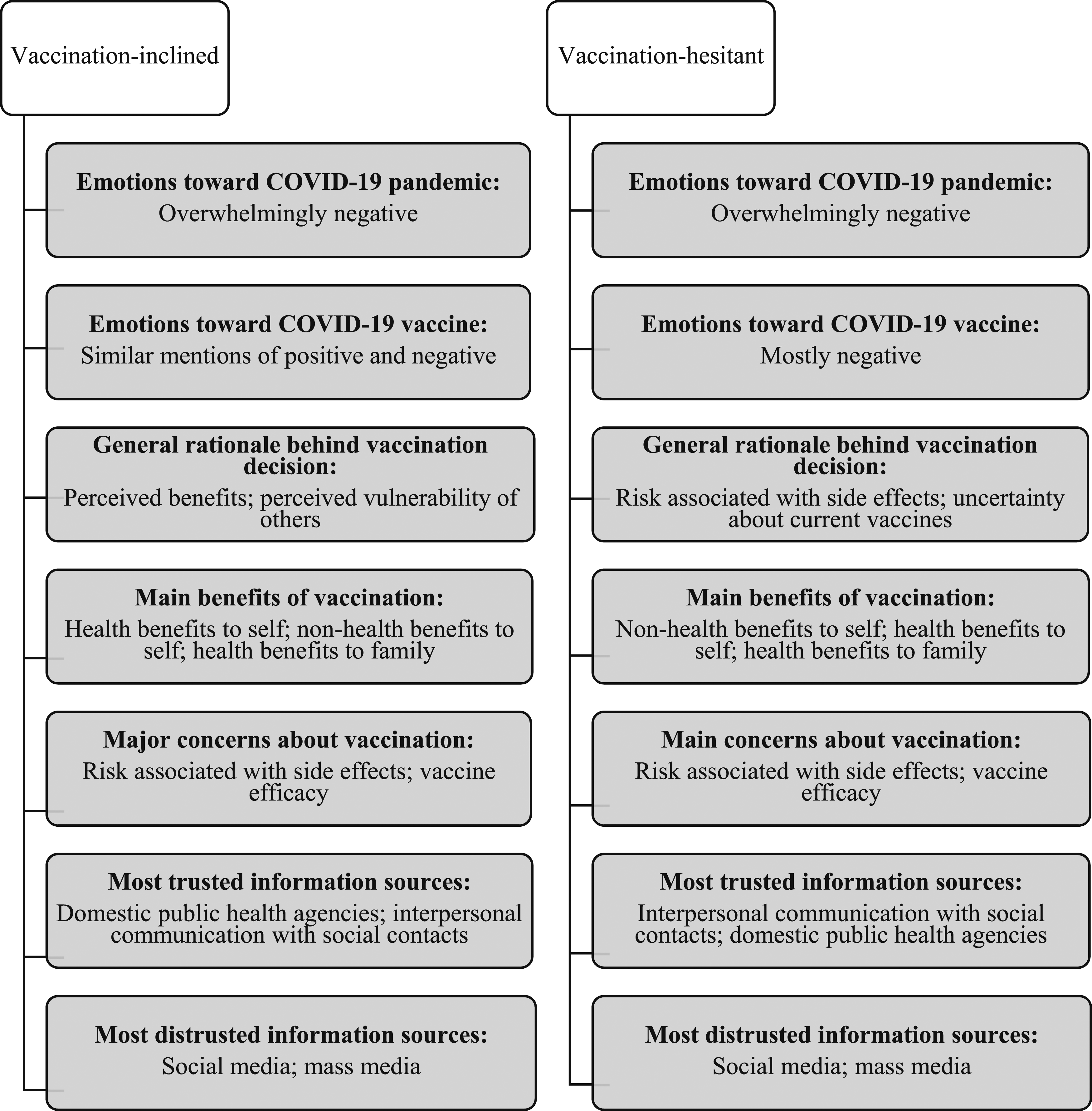
Discussion and conclusion
The purpose of this study was to explore cognitive and emotional factors that motivate or hinder the intention to receive COVID-19 vaccine in college students using 26 focus group discussions. Our findings not only corroborated with those from extant research, but also offered new insights regarding the role of emotions, systematic appraisals, and heuristics in shaping vaccination intention. Specifically, emotions such as fear, worry, anxiety, stress, and sadness were most frequently associated with the COVID-19 pandemic by our focus group participants, which is consistent with results from previous studies in this area (Broodryk and Robinson, 2021; Chu and Liu, 2021; Lu et al., 2021a; Liao et al., 2021). Findings from this study further revealed that the feelings of confusion, frustration and isolation were prevalent. These emotions merit greater attention in future investigations seeking to assess the impact of affect in cognitive appraisals, action tendencies, and behavioral patterns during the COVID-19 pandemic, or during other large-scale outbreaks.
The current study also sought to understand college students’ feelings toward the COVID-19 vaccines. It is of interest to note that confusion and fear, two negative emotions commonly associated with the pandemic, were also frequently linked to the vaccines developed to control it. For some individuals, these adverse feelings might be overwhelming, and in order to control them, people might resort to not thinking about any information related to the vaccines. It is therefore important to find ways to help individuals overcome these negative emotions so they can move on to performing a more systematic evaluation of the benefits, costs, and health threats in relation to COVID-19 vaccination. One potential strategy is to stimulate or amplify the feelings of hope and relief through public communication efforts, since these are the two positive emotions most frequently associated with the COVID-19 vaccines by our vaccination-inclined participants.
Once individuals are ready to engage in systematic appraisals, it is important for the provider of public health information to meet people where they are by tailoring its messaging to the existing interests, needs, and beliefs of the target audience. For vaccination-hesitant college students, this means highlighting the non-health-related benefits (e.g. social, economic, or educational) of COVID-19 vaccination. Emphasizing how vaccination would help to protect the health of their vulnerable and loved ones is also likely to be an effective messaging strategy to promote vaccination among young adults. On the other hand, messages focusing on the personal health benefits of COVID-19 vaccination to college students might be discounted by some vaccination-hesitant young adults. To elaborate, a number of hesitant participants in our focus groups perceived themselves as being in good health and not susceptible to serious illness from COVID-19. Messages arguing otherwise could therefore be ineffective and perhaps even counterproductive.
In addition, public health messaging would need to address college students’ concerns about the short-term and long-term side effects of COVID-19 vaccines by clearly dispelling some of the myths that have become widespread (e.g. the unproven association between vaccination and infertility). Government and pharmaceutical companies should also try to provide as much certainty as possible regarding the COVID-19 vaccines. Actions such as granting full approval to the available vaccines as soon as feasible and providing transparent, accessible information about the vaccines (e.g. ingredients and development processes) may be helpful. These lessons are also applicable to promoting pharmacological innovations developed to control future outbreaks.
People’s reception and interpretation of public health messages are inevitably shaped by their social environment. As suggested by results from this research, interpersonal influence from family, friends, and acquaintances could sway participants’ vaccination decisions. Furthermore, interpersonal communication was considered a highly trusted source of COVID-19 vaccination information by both vaccination-inclined and hesitant college students. Thus, we might run into the conundrum that “birds of a feather flock together,” meaning that hesitant individuals are probably surrounded by others with the same reluctance in their social environment. One way to tackle this conundrum and make some gain in vaccination willingness is to capitalize on the strength of the “weak ties” (Granovetter, 1973). Weak ties are people in our social network with whom we have less intimate and frequent interaction, and from whom our opinions are more likely to differ. Capitalizing on this weak tie status, vaccination-inclined or already vaccinated individuals can make a dedicated effort to share their personal experiences with professional affiliates and acquaintances (e.g. colleagues at work, fellow students in the same class) who harbor vaccine hesitancy, as people tend to find such testimonials trustworthy.
Last but not least, this study highlighted the importance of social trust as a heuristic in shaping college students’ vaccination intention. Social trust refers to individuals’ willingness to rely on a class of people (e.g. scientists) or sanctioned institutions (e.g. public health authorities) to act or decide on their behalf (Siegrist et al., 2000). Unlike the time-consuming and effortful cost–benefit analysis espoused by the HBM, TPB or PMT, social trust is a heuristic that is typically evoked when “the individual lacks the interest, time, abilities, knowledge, or other resources” (Holroyd et al., 2021: 354) to come to a sound conclusion. Research suggests that social trust, especially trust in public health authorities, is highly predictive of acceptance of various vaccines (Holroyd et al., 2021), including the COVID-19 vaccines (Salmon et al., 2021).
While we did not directly ask about the influence of social trust on decision-making, social trust organically emerged as a major theme during the discussions. Specifically, distrust in the vaccine development process was a main reason cited by many participants for their vaccination hesitancy. While this distrust might be partially based on the unprecedented speed with which the COVID-19 vaccines were developed and authorized for large-scale use, it might also be indicative of more general skepticisms toward the institutions (e.g. FDA, CDC, and pharmaceutical companies) involved in the creation, authorization, and recommendation of vaccines and other pharmacological products. It is therefore crucial for these institutions to find ways to build and maintain goodwill and credibility with the public on a long-term basis, as such social trust is likely to facilitate compliance with emergency and exceptional measures during future public health crises. For college students, another important institution involved in making recommendations related to vaccination and other preventive health measures is their school. It is thus important for campus administrations and health centers to engage in ongoing trust-building with students as well.
One limitation of this study is that different meanings can be associated with a “wait and see” response. In the current study, research participants with a “wait and see” response on the screening survey were first classified as vaccination-inclined. When probed about their vaccination decision regarding COVID-19, a significant number of these participants elaborated that they did plan on getting vaccinated in the future, even though they felt a little conflicted at the moment. A decision was therefore made to keep the original classification. However, this pattern could be unique to the current study, and it is of interest for future research to explore if the “wait and see” individuals are leaning more toward acceptance after a short initial pause when it comes to new vaccines or other pharmacological innovations. We also acknowledge that our definition of “vaccination-hesitant” individuals is different from the World Health Organization’s definition of “vaccine-hesitant” individuals, which refers to a heterogeneous group of people between the two extremes of “those that accept all vaccines with no doubts,” and those with “complete refusal [of all vaccines] with no doubts” (MacDonald and the SAGE Working Group on Vaccine Hesitancy, 2015). Compared to our binary approach, future research may yield more nuanced insights from a more refined approach to assigning focus group participants into three or more categories based on WHO’s vaccine hesitancy continuum.
Another limitation is that the participants came from two higher education institutions located in two states in the United States only, so it is not known whether the patterns of findings here would also apply to college students in other parts of the country. Nonetheless, results from this qualitative exploration provide novel insights that can facilitate future experimental studies. For example, future studies can employ our recommendations to create vaccine messages that emphasize particular positive versus negative emotions, highlight testimonials versus information statements by public health agencies, or focus on the benefits of vaccination for loved ones rather than to protect one’s own health. Such research could potentially identify the most effective type of messaging for college students. In fact, this may be useful as the U.S. is considering the need for booster shots among those with prior vaccination against COVID-19.
Additional studies should also identify whether the factors we found to influence vaccine-decision making among college students are similar to those found in a less-than college educated sample, or among older adults. Last but not least, given the social, financial, and physical health related impacts of the pandemic on everyone in our community, it would be noteworthy to also assess the mental health impact of the pandemic on vaccination decision-making. Specifically, it would be of interest to investigate if people who experience depression, anxiety, or posttraumatic stress symptoms in response to the COVID-19 pandemic may become more or less motivated to vaccinate in the future, given the mixed findings from extent literature on the relationship among generalized anxiety, depression, fear, and COVID-19 vaccination inclination (Bendau et al., 2021; Sekizawa et al., 2022). How these more generalized negative emotional states may interact with the object-specific emotions assessed in the current study (e.g. emotions toward a pandemic or a vaccine) in shaping decision-making is a topic that merits further attention.
Supplemental Material
Supplemental Material - Do cognition and emotion matter? A study of COVID-19 vaccination decision-making in college students
Supplemental Material for Do cognition and emotion matter? A study of COVID-19 vaccination decision-making in college students by Nien-Tsu Nancy Chen, Kimmy Kee, Bianca T Villalobos, Miriam Ortiz and HyeSun Lee in Health Psychology Open
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: a Research, Scholarship, and Creative Activity (RSCA) Award from the CSU Office of the Chancellor's and the CSUCI Office of the Provost to support data collection for this article.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical approval
All procedures performed in this study involving human participants received prior approval from the Institutional Review Board at the two universities where the investigators are based, and the study was conducted in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.