
Abstract
This study aimed to examine the role of resilience resources in patients' lifestyle changes after the first Acute Coronary event. 275 Italian patients (84.0% men; mean age = 57.5, SD = 7.9) participated in a longitudinal study. Resilience resources (Self-esteem, Dispositional Optimism, Sense of Coherence – SOC, General and Disease-specific Self-efficacy), and lifestyles (diet, physical activity, and smoking) were assessed twice (at baseline and after 6 months). Path analysis using latent change models was performed to model the combined effect of levels and changes of the resilience resources over lifestyle changes. Patients with strong SOC at baseline were less prone to smoke and more prone to decrease smoking; enhancement in SOC was associated with a smoking decrease. High Disease-specific Self-efficacy at baseline was associated with an improvement in all lifestyles; enhancement in Disease-specific Self-efficacy predicted an increase in physical activity. Findings underline the need to design psychological interventions that promote patients' Disease-specific Self-efficacy and SOC.
Keywords
Introduction
Cardiovascular diseases (CVDs) are among the most common causes of hospitalization in Western countries and are associated with high morbidity and mortality rates. Tackling CVDs is a health issue and a growing economic and societal challenge (Arnett et al., 2019; Timmis et al., 2020). Overall, modifiable risk factors like diet, physical activity, and smoking account for 70%–90% of CVD risk, suggesting that CVDs are largely preventable disorders (Yusuf et al., 2020). The virtuous management of modifiable risk factors has been listed as a primary World Health Organization (WHO) target for 2025 (Global Action Plan for the Prevention and Control of NCDs 2013–2020, n.d.). Nevertheless, a recent report from the European Society of Cardiology (ESC, Timmis et al., 2020) showed that only the reduction in smoking from 28% to 21% over the last 20 years achieves the WHO target. Other behaviors, like unhealthy diet and sedentary lifestyle, still need strong attention. Despite the considerable scientific evidence and the international guideline recommendations, adherence to regimens of a healthy diet and adequate physical activity is poor (Hamer et al., 2017; Yu et al., 2018). In addition, studies focusing on the longitudinal trajectories of healthy lifestyles have shown that patients with established CVD who initially adopt healthier lifestyles tend to drop out within 6 months of hospital discharge (Greco et al., 2021; Kotseva et al., 2019).
The medical community underestimates the role of psychological factors in adopting a healthy lifestyle among patients with CVDs. They are not currently recorded in the ESC Atlas (Timmis et al., 2020), nor are they among the WHO’s targets for management for 2025 (Global Action Plan for the Prevention and Control of NCDs 2013–2020, n.d.).
Prior research has consistently shown that distress symptoms, especially anxiety and depression (Kubzansky et al., 2018; Ossola et al., 2018; Wang et al., 2021), can contribute to CVD risk. Lifestyle is one of the pathways through which the link between distress symptoms and CVDs is expressed (Kubzansky et al., 2018). For example, a previous study showed that patients after the first cardiovascular event experiencing anxiety and depressive symptoms exhibited less healthy lifestyle profiles than patients without these symptoms (Monzani et al., 2018). This finding is coherent with other empirical evidence showing anxiety has a deleterious effect on adopting a healthier lifestyle following myocardial infarction (Kuhl et al., 2009) and a systematic review showing that anxiety and depression represent a barrier to lifestyle changes in patients with CVDs (Murray et al., 2012).
Few studies have focused on the role played by psychological well-being and resilience resources, despite the vast literature demonstrating that positive psychological factors do not overlap with the opposite of negative ones and that the two may play different roles in affecting human behavior (Kubzansky et al., 2018; Ryff et al., 2006).
As regards CVDs, recent reviews have pointed out that psychological well-being may promote healthy behaviors (Kubzansky et al., 2018) and cardiovascular health (Park et al., 2022). Despite this evidence, there is no shared definition of psychological well-being or resilience. Consequently, there is no consensus measure for most aspects of psychological well-being. Our study fits into this context and serves to compare the role of different psychological constructs in contributing to lifestyle changes in patients after the first acute cardiovascular event.
Psychological resilience is generally defined as the capacity to overcome adverse situations and evolve positively despite negative experiences (Fletcher and Sarkar, 2013; Zautra et al., 2010). Resilience has had several operationalizations in literature. Among them, resilience has been characterized as having a positive attitude toward the self (Self-esteem, Rosenberg, 1965) and feeling the confidence to apply the necessary effort to succeed in challenging tasks (Self-efficacy, Bandura, 1977). It is also related to a tendency to appraise life situations as predictable, meaningful, and manageable (Sense of coherence, Antonovsky, 1980), and to have positive expectations about current and future success (Dispositional Optimism, Carver and Scheier, 1998). The psychological constructs mentioned are those most commonly investigated and significant in predicting positive lifestyle changes in patients with CVDs.
For example, previous studies have suggested that low Self-esteem (Rosenberg, 1965) represents an obstacle to lifestyle change for CVD prevention (Mosca et al., 1998). In contrast, high Self-esteem has been associated with a healthy diet, high levels of exercise, and smoking reduction after myocardial infarction (Conn et al., 1992). A recent study confirmed the link between high Self-esteem, health-promoting behaviors and CVD risk in a sample of middle-aged women (Ashgar, 2021).
Regarding Dispositional Optimism (Carver and Scheier, 1998), a longitudinal study found that 12 months after acute coronary syndrome, patients with high Optimism reduced smoking and improved their diet (Ronaldson et al., 2015). Coherently, a recent meta-analysis showed that a high level of Optimism was associated with more physical activity, nonsmoking, and a healthy diet in different samples of people from the general population and patients with CVD, leading to the conclusion that a high level of Optimism can indirectly reduce the risk for CVD through healthy behavioral choices (Boehm et al., 2018).
Associations between a strong Sense of Coherence (SOC, Antonovsky, 1980) and healthy lifestyles have commonly been reported among the general population (Binkowska-Bury et al., 2016; Wainwright et al., 2007) and can also be traced among patients after myocardial infarction. For example, previous studies have found that patients after myocardial infarction with a strong SOC tended to be more physically active (Bergman et al., 2009; Myers et al., 2011), were more likely to quit smoking (Gerber et al., 2011), and tended to eat a healthier diet (Nachshol et al., 2020) than patients with a weak SOC.
Regarding Self-efficacy (Bandura, 1977), a clarification must be made. Self-efficacy beliefs can be general or specific. General Self-efficacy concerns the overall confidence level in one’s coping strategies throughout a broad range of situations (Luszczynska et al., 2005; Schwarzer and Jerusalem, 1995). Specific Self-efficacy beliefs regard the feeling of having the capacity to reach an aim in a specific context or condition. Previous studies have shown that higher general Self-efficacy is related to lower levels of smoking in patients with Acute Coronary Syndrome (ACS) (Bekke-Hansen et al., 2014) and better responses to cardiovascular rehabilitation, particularly regarding physical activity (Fleig et al., 2013; Slovinec D’Angelo et al., 2014). Alharbi et al. (Alharbi et al., 2016) found that Disease-specific Self-efficacy was one of the factors affecting exercise capacity, its duration, and, therefore, decreased body mass index (BMI) and waist circumference in a sample of patients diagnosed with coronary heart disease. Again, Sol et al. (Sol et al., 2011) showed that improvements in Disease-specific Self-efficacy were associated with enhanced adherence to the guidelines for good physical activity and a healthy diet in a sample of patients with different CVDs. This result was not replicated for smoking or alcohol consumption (Sol et al., 2011).
As mentioned above, very little is known about which resilience resources are more relevant and how they act together to improve the lifestyle of patients with CVDs. All of the studies cited focused on the effects of a single resilience resource. Furthermore, to the best of our knowledge, no study has investigated the specific link between resilience resources and lifestyle changes in patients after the first acute coronary event. The period immediately following the first acute event is critical because patients are asked to cope with a very stressful situation and are requested to undertake multiple lifestyle changes. It is, therefore, crucial to understand which specific resilience resources can promote positive changes in this critical circumstance. Findings will help to clarify the role of different resilience resources and develop more targeted and effective interventions aimed at fostering individual resources and promoting correct behaviors.
The main aim of this study was to analyze the predictive role of resilience resources over time and assess the role that changes in resilience play in baseline levels and changes in lifestyle. This aim was accomplished by adopting a two-wave longitudinal design with 6-month intervals.
All the resilience resources measured after the cardiovascular event (the baseline) and the 6-month follow-up were considered predictors. In addition, non-modifiable (age, gender, and family history for CVDs) and modifiable (body mass index - BMI) risk factors of clinical relevance to CVDs (Yusuf et al., 2020) were taken under consideration in the analyses.
Specifically, the present study tested three hypotheses. The first hypothesis concerned the association among Self-esteem, Dispositional Optimism, SOC, and Self-efficacy (general and Disease-specific) soon after the first acute event (the baseline). We hypothesized strong correlations among these variables, as they all are facets of psychological resilience. The second hypothesis concerned how diet, physical activity, and smoking behavior changed between the baseline and the 6-month follow-up. We hypothesized an increase in healthy behaviors, as patients are generally likely to adopt healthier lifestyles soon after an acute event (Steca et al., 2017b). Steca et al. (2017) the third hypothesis concerned the role of resilience factors, assessed in terms of baseline levels and changes over time, on patients' lifestyle changes in the period between the acute coronary event and the 6-month follow-up. Based on prior literature, we hypothesized that resilience resources would positively impact lifestyles. We further hypothesized a positive effect of increased Self-efficacy on diet and physical activity (Sol et al., 2011). However, we did not have any other specific hypothesis, as this is a neglected area of research, and existing data are limited.
Methods
Participants and study design
Patients with ACS were enlisted prospectively from two metropolitan hospitals. One was a medium size hospital with a large Cardiology and Pneumology rehabilitation unit in the north of Italy; the other was a large hospital integrated with a university located in the center of Italy.
Physicians involved in the study recruited patients who met the inclusion criteria based on their medical records. The inclusion criteria were a diagnosis of first ACS (NSTEMI myocardial or STEMI myocardial infarction, and unstable angina), age between 30 and 75, fluency in Italian, no cognitive deficits, and no comorbidity with other significant pathologies such as cancer. Participants were informed about the characteristics of the study through informative documents and were asked to sign an informed consent form. The study design was longitudinal. Data were collected through self-reported questionnaires completed during the cardiovascular rehabilitation program between 2 and 8 weeks after hospitalization (the baseline - t0; mean = 33 days after the cardiovascular event; SD = 16.35) and 6 months later (the follow-up - t1), during regular checkups. A trained psychologist administered the questionnaires to the participants in both situations, and physicians reported a set of clinical data regarding cardiovascular risk factors.
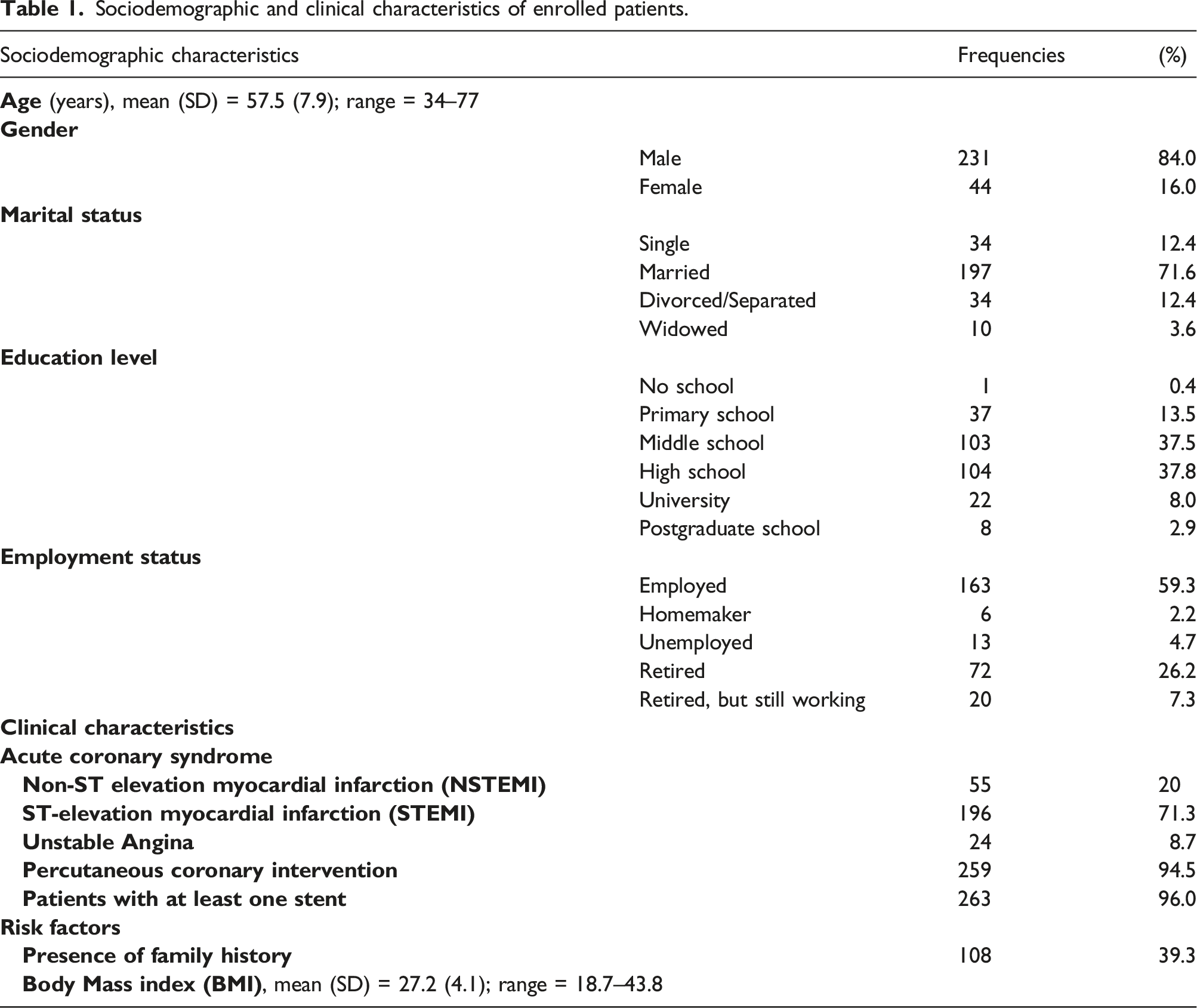
Sociodemographic and clinical characteristics of enrolled patients.
The sample size adequacy was established by resorting to power analysis (Cohen, 1988) using G*Power Version 3.1.9.2 (Faul et al., 2007). We calculated the sample size required to perform bivariate correlations with the following parameters: ρ = 0.30 (medium effect size), α = 0.05, two tails, power = 0.95. The sample size calculated was 134 individuals. Moreover, we calculated the sample size required to perform paired-sample t-tests with the following parameters: dz = 0.30 (medium effect size), α = 0.05, power = 0.95. The sample size calculated was 147 individuals. Based on these considerations, the study’s sample size was sufficient to detect medium-sized effects.
The study was conducted according to the World Medical Association Declaration of Helsinki. The ethical committee of the University of Milano-Bicocca approved the research.
Variables and instruments
Sociodemographic and clinical variables
Physicians collected information about sociodemographic (i.e., gender, age, marital status, education, and working status) and clinical (i.e., family history of premature CVDs and BMI) indicators.
Resilience resources
Due to the frail health condition of the patients involved in this study, a brief version of all the questionnaires was used to engage them for no longer than 30 min. The choice of the items of each scale was made based on theoretical and psychometric criteria. Indeed, each set of items has been chosen considering the criterion of the greatest factor loadings (Kelloway, 1998; Schumacker and Lomax, 2004) of the original scales and resorting to a focus group between the study’s authors and the clinical psychologists involved in the project. The rationale was to capture all the psychological constructs in the shortest time possible.
Self-esteem and dispositional optimism
A brief Italian version of the Rosenberg Self-esteem Scale (Prezza et al., 1997; Rosenberg, 1965) was used to assess Self-esteem. Only three of the 10 original items were used. Two were positively worded items (i.e., items for which higher scores denote higher levels of Self-esteem), and one was negatively worded. Responses were on a 4-point Likert scale, ranging from 1 (strongly disagree) to 4 (strongly agree). Self-esteem was calculated as the mean of the answer to all items. The items were: “Sono in grado di fare le cose bene almeno come la maggior parte delle altre persone” (I can do things as well as most other people); “Complessivamente sono soddisfatto di me stesso” (Overall, I am satisfied with myself); “Sono portato a pensare di essere un fallimento” (I tend to think I’m a failure).
Dispositional Optimism was assessed with a brief Italian version of the Revised Life Orientation Test (Scheier et al., 1989; Steca et al., 2017a). Only three of the original items were used. Two were positively worded items (i.e., items for which higher scores denoted high Optimism), and one was negatively worded. Responses were on a 5-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). Optimism was calculated as the mean of the answers to all items. The items were: “In generale mi aspetto che mi accadranno più cose positive che negative” (In general, more good things will happen to me than bad); “Sono sempre ottimista riguardo il mio future” (I am always optimistic about my future); “Se qualcosa può andare per me per il verso sbagliato, sicuramente ci andrà” (If anything can go wrong for me, it surely will).
Standardized estimates, standard errors (SE), and p value resulting from the Confirmatory factor analyses.

Sense of Coherence (SOC)
The Sense of Coherence Scale (Antonovsky, 1993; Barni and Tagliabue, 2005) is a 13-item self-report measure of how people manage stressful situations and stay well. It is composed of three subscales, namely comprehensibility (5 items, for example: “Do you have the feeling that you are in an unfamiliar situation and do not know what to do?”), manageability (4 items, for example: “How often do you have feelings that you are not sure you can keep under control?”), and meaningfulness (4 items, for example: “How often do you have the feeling that there is little meaning in the things you do in your daily life?”), which can be added to a total score. Responses were on a 7-point Likert scale, on which the alternatives were semantically different and ranged from 1: “very seldom or never” to 7: “very often.” In the present study, only the total score was used. The scale showed a good internal consistency (McDonald’s ω t0 = 0.84; t1 = 0.84).
Self-efficacy – general and disease-specific self-efficacy
General Self-efficacy was assessed using a brief three-item version of the Italian adaptation of the Generalized Self-efficacy Scale (Scholz et al., 2002; Schwarzer and Jerusalem, 1995; Sibilia et al., 1995), designed to measure the overall perceived Self-efficacy to cope with various difficulties in life. Responses were on a 4-point Likert scale (from 1: “not at all true” to 4: “exactly true”). General Self-efficacy was calculated as the mean of the answers to all items. The items were: “Grazie alle mie risorse, so come gestire situazioni impreviste” (Thanks to my resources, I know how to handle unforeseen situations); “Rimango calmo nell’affrontare le difficoltà perché posso confidare nelle mie capacità di fronteggiarle” (I remain calm in facing difficulties because I can rely on my ability to deal with them); “Non importa quello che mi può capitare, di solito sono in grado di gestirlo” (No matter what comes my way, I am usually able to handle it).
Disease-specific Self-efficacy was assessed using a brief three-item version of the Cardiac Self-efficacy Questionnaire (CSEQ, Steca et al., 2015a; Sullivan et al., 1998), designed to assess patients’ belief in their ability to identify, recognize and manage the specific symptoms of CVD. For each item, there were five possible choices (from 1: “not at all confident” to 5: “completely confident”), plus the option “never occurred” in the case participants had never experienced the circumstances presented by the item. The items were: “Quanto è capace di riconoscere sempre i sintomi della sua malattia, come edema o gonfiore agli arti?” (How well can you recognize the symptoms of your illness, such as edema or limb swelling?); “Quanto è capace di riconoscere i segni di un peggioramento e capire quando è il caso di rivolgersi ad un medico?” (How well can you recognize the signs of deterioration and understand when it is appropriate to consult a doctor?); “Quanto è capace di riuscire a far capire al suo medico le preoccupazioni che ha riguardo ai suoi disturbi?” (How well can you make your doctor understand your concerns about your ailments?).
A modified version of both scales was used; therefore, CFA was performed. In line with Hu and Bentler’s guidelines (Hu and Bentler, 1999), the results indicated that the two-factor model (general Self-efficacy and Disease-specific Self-efficacy) fit the data adequately and provided a better fit than a one-factor model (χ2 = 7.69, df = 8, p = 0.464, CFI = 1.00, RMSEA = 0.00, WRMR = 0.32). Standardized estimates were all significant (Table 2). The scales demonstrated an adequate internal consistency (regarding general Self-efficacy, McDonald’s ω t0 = 0.75 and t1 = 0.69; regarding Disease-specific Self-efficacy, McDonald’s ω t0 = 0.84 and t1 = 0.84).
Lifestyles
Diet
Diet was measured using the Italian version of the Mediterranean Diet Scale (MDS, Steca et al., 2015b; Trichopoulou et al., 2003). The MDS is a 9-item self-report questionnaire that measures the weekly consumption of nine foods using a 6-point Likert scale (from 1: Never to 6: More than three times per day). The consumption of both beneficial (i.e., vegetables, fruits, whole grains, fish, legumes, olive oil) and detrimental foods (i.e., more than two glasses of wine per day for men and more than one glass of wine for women, butter and margarine or vegetable oil other than olive oil, red or processed meat) was assessed. The sum of the recoded responses yielded the Mediterranean Diet Score, with higher scores indicating a healthier diet. A score of four and above represents good adherence to the Mediterranean diet and has been related to good health outcomes (Trichopoulou et al., 2003).
Physical activity
Physical activity was examined using the Italian version of the Rapid Assessment of Physical Activity Questionnaire (RAPA-Q, Topolski et al., 2006), a 7-item measure of physical activity frequency and intensity. The questionnaire uses a yes/no scale. The total score ranges from one (i.e., sedentary) to seven (i.e., regular and vigorous activity), with higher scores indicating a healthier amount of physical activity. Scores of 6 or 7 (i.e., at least 30 min of moderate to vigorous aerobic exercise five times a week) indicate the target amount of physical activity for cardiovascular prevention.
Cigarette smoking behavior
Participants’ smoking behavior was measured by asking, “How many cigarettes do you smoke per day?”. The scale ratings were 0: “No cigarettes,” 1: “10 cigarettes or fewer per day”, 2: “11–20 cigarettes per day”, 3: “21–30 cigarettes per day”, and 4: “31 or more cigarettes per day”.
Data analysis
IBM SPSS Statistics, version 24 (SPSS, Chicago, IL, USA), and Mplus software, version 7.0 (Muthén and Muthén, 2007), were used to perform data analyses.
CFA was carried out to evaluate the latent structure of the resilience factors. McDonald’s ω was calculated to estimate the internal consistency of the resilience factors (Hayes and Coutts, 2020; McDonald, 2013).
Attrition is common in longitudinal studies (Hansen et al., 1990). Mann-Whitney U and Chi-square tests were used to identify possible dissimilarities between the sample included in the analyses and the participants lost to follow-up. Moreover, we ran a Little Missing Completely At Random (MCAR) test to evaluate if data from patients who dropped at the follow-up were missing at random (Marcoulides and Schumacker, 2013).
Paired sample t-tests were used to examine changes over time in lifestyles. Reliable changes in lifestyles and resilience resources were estimated using latent change models (Hertzog and Nesselroade, 2003; McArdle and Nesselroade, 2019). These models estimate absolute change over two measurements in latent variables. A latent change model restructures the wave-specific factor to the latent level (i.e., mean baseline level, t0) and changes factors (i.e., differences between the follow-up and the baseline, t1-t0). Regression coefficients involving the latent variables were fixed to 1, meaning that the latent variable of a level was equal to the level at t0, and the latent change variable was equal to the difference between the two waves (t1- t0). The model defined in this way has various advantages, as it prevents measurement errors with minimal dissimilarity scores (Rogosa et al., 1982) and the description of the complete change in the latent variable in a factor. Latent variable values were used to analyze a path model, with a maximum likelihood estimation, investigating whether levels and changes in resilience resources predicted lifestyle levels and changes from t0 to t1 (Figure 1). The effects of non-modifiable and modifiable CVD risk factors were controlled for in the analysis model. Hu and Bentler’s guidelines (Hu and Bentler, 1999) for several fit indices were employed to decide whether the expected models were consistent with the data. Conceptual model linking lifestyle and resilience resources. 
All statistical tests were two-tailed, and a p ≤.05 was considered statistically significant.
Results
Preliminary analyses
At the 6-month follow-up, 241 of the 275 initial patients remained. Thus, Mann-Whitney U tests and chi-squared tests were performed on variables measured at t0 to exclude possible dissimilarities between the sample used in the study and the 34 participants lost to follow-up.
The 34 patients who declined to participate at the follow-up did not differ significantly from the respondents in their sociodemographic characteristics, namely age (U = 4125.00; z = 0.104; p = 0.917), gender (χ2(1,275) = 0.518; p = 0.472), marital status (χ2(1,275) = 0.446; p = 0.504), education (χ2(1,275) = 0.025; p = 0.874), working status (χ2(1,275) = 0.185; p = 0.667), and clinical diagnosis (χ2(3,275) = 0.910; p = 0.823). Statistically significant differences were found in Optimism (U = 5073.00; z = 2.276; p = 0.023), Self-esteem (U = 5073.00; z = 2.276; p = 0.023), and SOC (U = 5383.00; z = 3.035; p = 0.002), with higher levels of these factors in patients who participated at the two-time points. In contrast, no significant differences were pointed out for the remaining resilience resources, namely General (U = 4457.50; z = 0.860; p = 0.390) and Disease-specific Self-efficacy (U = 3398.00; z = −1.490; p = 0.136). Finally, no significant differences were found in terms of lifestyle, namely diet (U = 4511.00; z = 0.979; p = 0.328), physical activity (U = 4610.50; z = 1.196; p = 0.232), and cigarette smoking (U = 3712.00; z = −0.899; p = 0.369).
The MCAR test was not significant (χ2(68) = 80.743; p = 0.138). The non-significant effects of the missing data pattern (dropouts vs completers) suggested that all data were missing at random and that the estimates of effects were unbiased by the presence of dropouts (Kristman et al., 2004).
Path model predicting latent lifestyle changes
Standardized regression coefficients of non-modifiable (age, gender, and family history for CVDs) and modifiable (BMI) risk factors taken under control in the path model predicting latent lifestyle changes.

Note: *p < 0.05; **p < 0.01: ***p < 0.001.
Overall, the model explained a high proportion of the variance in lifestyle changes (28.4% for diet, 47.6% for physical activity, and 83.5% for cigarette smoking). However, the model showed a low proportion of the variance of the predicted levels of lifestyles (explained variance: 7.7% for diet, 2.6% for physical activity, and 5.5% for cigarette smoking).
Association among the resilience resources at t0
Correlation coefficients among levels of Self-esteem, Dispositional Optimism, Sense of Coherence, general Self-efficacy, and Disease-specific Self-efficacy from a path model predicting latent lifestyle changes.

Note: N = 241. *p < 0.05; **p < 0.01; *** = p < 0.001.
Changes in lifestyle from t0 to t1
Significant differences were found between the two time points for diet (t(240) = -9.66, p < 0.001; dz = 0.62), physical activity (t(240) = -8.11, p < 0.001; dz = 0.53), and cigarette smoking (t(240) = 13.14, p < 0.001; dz = 0.85). Particularly, diet (mean t0 = 3.42, SD = 1.36; mean t1 = 4.38, SD = 1.46) and physical activity (mean t0 = 4.27, SD = 2.03; mean t1 = 5.48, SD = 1.79) improved over time (patients were engaged in a healthier diet and a higher amount of physical activity from t0 to t1). Cigarette smoking decreased over time (mean t0 = 1.36, SD = 1.40; mean t1 = 0.20, SD = 0.61).
Impact of resilience resource levels and changes over lifestyle changes between t0 and t1
Standardized regression coefficients and explained variance for path model predicting latent lifestyle changes.

Note: *p < 0.05; **p < 0.01: ***p < 0.001.

Standardized regression coefficients for path model linking lifestyle and resilience resources.
Regarding diet, the level of Self-esteem was associated with the initial diet score; in other words, a higher score of Self-esteem at the baseline was associated with a healthier diet at the baseline. Moreover, a higher level (i.e., higher score at the baseline) of Disease-specific Self-efficacy predicted more remarkable improvement in the diet. That is, the higher the Disease-specific Self-efficacy score at the baseline, the more significant the improvement in diet over time.
Regarding physical activity, none of the resilience resources were associated with the initial level of physical activity. However, a higher level (i.e., higher score at the baseline) of SOC and Disease-specific Self-efficacy predicted increased physical activity. In other words, the higher the SOC and Disease-specific Self-efficacy score at the baseline, the more significant the improvement in physical activity over time. Coherently, a change in Disease-specific Self-efficacy was associated with a more significant change in physical activity. In other words, an increase in the Disease-specific Self-efficacy score over time was associated with an improvement over time in physical activity.
Regarding cigarette smoking, a higher level (i.e., higher score at the baseline) of SOC was associated with a lower level of initial cigarette smoking. In other words, the higher the baseline SOC score, the lower the baseline cigarette smoking. Furthermore, higher levels (i.e., higher score at the baseline) of SOC and Disease-specific Self-efficacy predicted decreases in cigarette smoking over time. In other words, the higher the SOC and Disease-specific Self-efficacy score at the baseline, the more significant the decrease in cigarette smoking over time. Coherently, changes in SOC predicted more remarkable changes in cigarette smoking. In other words, an increase in the SOC score over time was associated with a decrease in cigarette smoking.
Finally, a less healthy lifestyle at t0, in terms of an unhealthy diet, low physical activity, and smoking respectively, was associated with a more remarkable change in the same behavior. It means that the worse the baseline behavior (unhealthy diet, low physical activity, smoking) was, the more significant the Salutogenic change (diet improved, physical activity increased, and smoking decreased, see Table 5).
Discussion
The primary aim of this study was to analyze the association between resilience resources and lifestyle and to evaluate the role that change in resilience plays in lifestyle change in a sample of ACS patients 6 months after their first coronary event. This study is the first to look at five different resilience resources together, providing insight into the individual effect of each variable while controlling for the others.
Association among the resilience resources at the baseline
Our hypothesis that there is an association among the different resilience resources immediately after the first acute event was confirmed, except for the relationship between Disease-specific Self-efficacy and Dispositional Optimism. Moderate positive correlations emerged among General Self-efficacy, Optimism, Self-esteem, and SOC, confirming their common root, but with a different connotation, since resilience can be considered either in terms of a positive attitude towards the self, the confidence to successfully manage different tasks, a tendency to cope with adverse experiences successfully, or positive expectations for the future (Pallant and Lae, 2002). Differently, Disease-specific Self-efficacy was not related to Optimism and was only weakly associated with the other factors investigated. This unexpected result could be explained by the specificity of the Disease-specific Self-efficacy, which refers to the patients’ ability to identify, recognize and manage the symptoms of their illness. This characteristic makes this resource different from the others, which could be considered more generic.
Changes in lifestyle from the baseline to the 6-month follow-up
Our findings demonstrated that patients had healthier behaviors 6 months after the acute event. The results showed improved diet, physical activity, and smoking over time, confirming our hypothesis. These findings are in line with prior research demonstrating that in most cases, patients were able to implement efficacious management and coping strategies (Petrie et al., 1999) and, consequently, were able to adopt a healthier lifestyle after the acute event (Steca et al., 2017b).
Impact of resilience resource level and change over lifestyles change over time
SOC and Disease-specific Self-efficacy had the most relevant link with lifestyle changes when controlling for the effects of modifiable and non-modifiable CVD risk factors.
Results showed that SOC level was strongly associated with smoking behavior. Indeed, patients with higher SOC levels were less prone to smoke at the baseline and more prone to decrease smoking over time than patients with lower SOC levels. Moreover, enhancement in SOC was associated with an improvement in smoking behavior over time. These results are in line with previous findings involving patients with myocardial infarction, suggesting that a higher level of this resource corresponded to a lower percentage of cigarette smoking (Gerber et al., 2011). SOC level at baseline was also associated with physical activity change, in line with previous findings showing an association between a strong SOC and a high amount of physical activity in patients with myocardial infarction (Bergman et al., 2009; Myers et al., 2011). Unlike previous studies (Nachshol et al., 2020), SOC was not related to healthier food choices.
Regarding Disease-specific Self-efficacy, results showed that its level was associated with dietary change; moreover, Disease-specific Self-efficacy level and change predicted physical activity change over time. These results are consistent with prior literature suggesting the role of this variable in promoting a healthier diet and adequate physical activity in patients with CVDs (Alharbi et al., 2016; Fleig et al., 2013; Slovinec D’Angelo et al., 2014). Interestingly, Sol et al. (Sol et al., 2011) found that improvement in Disease-specific Self-efficacy was associated with higher physical activity and a healthier diet in patients with different CVDs. The results of our study are also consistent with those of Sol et al. (Sol et al., 2011), in that they highlight that a change in Disease-specific Self-efficacy did not predict any change in smoking behavior.
Prior research has shown that physical activity and dietary habits can be conceived as behaviors that require an active commitment to promoting one’s health. On the contrary, smoking can be conceived as an addictive behavior requiring restraint or abstinence (De Vries et al., 2008; Noble et al., 2015). In this perspective, our results suggest that a strong SOC and an enhancement of this resource over time may play a significant role in countering addictive behaviors, such as smoking, and a marginal role in improving proactive behaviors like physical activity. Conversely, high Disease-specific Self-efficacy, especially an enhancement of it, may lead to an improvement in proactive behaviors like physical activity.
Regarding the other resilience resources considered in this study, results showed that patients with higher levels of Self-esteem engaged in a healthier diet at the baseline. Similar results were obtained by Conn et al. (Conn et al., 1992), who demonstrated that higher levels of Self-esteem were associated with a healthier diet in patients with myocardial infarction.
No other significant associations emerged. The absence of significant associations between Dispositional Optimism, General Self-efficacy, and lifestyle change may be explained by considering that prior research has generally focused on the effects of a single resilience resource. In contrast, to our knowledge, this study is the first to consider five different resilience resources together, providing information about the individual effect of each variable while controlling for the others. Our findings provide valuable insight into which resilience resources are most relevant to supporting the lifestyle change of patients with CVDs and, therefore, which resources should be enhanced in health-promoting lifestyle interventions.
Regarding the non-modifiable and modifiable risk factors of clinical relevance that were controlled for in the analyses, results showed that older age was associated with a healthier diet and lower smoking levels at the initial assessment, in line with previous studies showing an improvement in these behaviors with advancing age (Mozaffarian et al., 2016; Noble et al., 2015). This result may be due to a growing awareness and risk perception about the effects of unhealthy food and smoking on health. Results also showed that women were less likely to improve their physical activity than men. This result is coherent with prior literature highlighting a gender disparity in interest and participation in physical activity in patients with CVD (Mozaffarian et al., 2016; Timmis et al., 2020).
Limitations
Besides several insights, this study has some limitations. First, the brief self-report questionnaires used to evaluate resilience factors may oversimplify these complex psychological constructs. The same limit could be mentioned regarding the self-report questionnaires used to assess lifestyle. Moreover, information about lifestyle at the baseline was measured retrospectively by asking patients to report their habits before the acute event. This approach may limit the results' reliability because patients may have over- or underestimated their authentic past lifestyle. Moreover, self-report methods are prone to information bias, such as recall bias or social desirability bias. More ecologically valid methods might help evaluate the truthfulness of patients’ reported information about lifestyles. The methodological choice of self-report questionnaires was due to the frail health condition of the patients at the baseline. Despite its inferential limitations, this methodology is widely adopted in the medical and psychological literature (Prince et al., 2008). It provides essential steps in understanding a phenomenon, and it has substantial advantages, such as ease of use and an excellent cost-benefit ratio (Paulhus and Vazire, 2007).
The second limit of our study is its focus on a homogeneous sample of patients at their first cardiovascular event. While this may restrict the generalizability of the results, it ensures that the inferences drawn from the study apply effectively to the population of ACS patients at their first event. Therefore, they assume an essential significance for secondary cardiovascular prevention.
Future studies should consider data from additional time points and more comprehensive samples of patients with a less imbalanced gender distribution to generalize the findings. In this regard, the proportion of men in our sample was a direct consequence of the incidence of ACS, which is more common among men than women (Calabrò et al., 2018).
A further consideration regards dropout motivations. Patients who dropped out of this study had no difference in lifestyle but had lower Self-esteem, Dispositional Optimism, and SOC than patients who participated in the follow-up. This, again, highlights that our results could not be generalized and draws the attention of future studies to dropout motivations.
Finally, some psychological factors that were not investigated in this study, particularly distress symptoms, could play a role in patients' lifestyle changes. However, as pointed out in the introduction, we focused on psychological well-being and resilience resources (in line with what was proposed by Kubzansky et al., 2018) for several reasons. First, these factors are still largely unexplored in the literature, especially compared to distress symptoms, such as anxiety and depression (Kuhl et al., 2009; Monzani et al., 2018; Murray et al., 2012). Moreover, the ultimate aim of this work was to give operational indications for interventions aimed at promoting a healthy lifestyle. As noted above, the results of our study provide valuable insights into which resilience resources should be most stimulated to promote lifestyle change. From a practical point of view, clinical interventions structured around enhancing resilience resources might be helpful for all patients with CVD (Kubzansky et al., 2018). In contrast, interventions structured around reducing distress symptoms make sense only in the case of patients with symptoms of clinical relevance (Kubzansky et al., 2018).
Conclusions
Overall, our study suggests that SOC and Disease-specific Self-efficacy may play an essential role in the active commitment to adopt a healthy lifestyle. These resilience resources can stimulate changes toward healthier behaviors in patients with ACS. Interestingly, Disease-specific Self-efficacy may play the most pervasive role in adopting a healthy lifestyle. Indeed, our results suggested it was the only resilience resource with positive effects over all the behaviors considered.
Dispositional Optimism and General Self-efficacy had no significant impact on adopting a healthier lifestyle over time. These two factors are likely too generic. General Self-efficacy could have lost effect in favor of a more specific resilience resource connected to perceiving the capacity to fulfill a specific task or recognizing one’s value, namely Disease-specific Self-efficacy. Optimism could have lost effect in favor of SOC since, as Antonovsky (Antonovsky, 1980) stated, the latter can be considered a mixture of Optimism and control. All these considerations should be examined more widely in future research. As underlined in the introduction, CVDs represent one of the primary causes of morbidity and mortality in Western countries (Timmis et al., 2020). Modifiable risk factors like diet, physical activity, and smoking account for a large percentage of CVD risk (Yusuf et al., 2020). Therefore, identifying resources to stimulate lifestyle changes is one of the essential aims of cardiac rehabilitation following an acute event.
Clinical implications
In conclusion, this longitudinal investigation represents an original contribution to studying the predictive role of resilience resources for lifestyle change in ACS patients and has important implications for behavioral interventions in patients with CVDs. The general rules for cardiovascular rehabilitation highlight how interventions should focus on psychological topics to stimulate a positive mental perspective and improve patient self-management. Our study underlines the need to design psychological interventions that promote patients’ Disease-specific Self-efficacy and SOC through behavior programs inserted into specific cardiac rehabilitation interventions (Dusseldorp et al., 1999; Kubzansky et al., 2018; Linden et al., 1996; Yeh et al., 2016).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Italian Ministry of Education, University, and Research [grant number RBFR08YVUL].
Data accessibility statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.