
Abstract
Using data from 148 middle-aged and older adult spouses whose partners had type 2 diabetes, we sought to examine spouses’ motives for involvement in their partners’ diabetes management and whether these motives were related to common types of diabetes-related spousal involvement; we also sought to understand gender differences in these dynamics. Spouses indicated being motivated to be involved in their partners’ diabetes management due to altruistic motives to the greatest extent and egoistic motives to the least extent. Results from multivariable regression analyses that controlled for gender, marital quality, and spouses’ own conditions requiring dietary changes revealed that all types of motives were related to the frequency of providing diet-related spousal support, whereas only egoistic motives were related to the frequency of exerting diet-related spousal control. We did not find gender differences in any motives nor in associations with spousal involvement. Findings have potential implications for couples-oriented chronic illness interventions.
Type 2 diabetes is a serious health issue that increases in prevalence with age (Centers for Disease Control and Prevention [CDC], 2022). Although there are several behaviors that individuals with diabetes need to engage in to successfully manage their condition, eating a healthy diet is a critical aspect of diabetes management (Mayo Clinic, 2020). Yet individuals with diabetes often report that eating a healthy diet is one of the most difficult aspects of their diabetes regimen and often do not follow recommended guidelines (Beverly et al., 2008; Broadbent et al., 2011). Spouses therefore are often involved in promoting better dietary behaviors in their partners with diabetes by supporting or regulating (controlling) their diet (August and Sorkin, 2011; Stephens et al., 2013).
Little is known, however, about spouses’ motives for involvement in diabetes management and whether these motives can help explain why spouses are involved in different ways and at different frequencies in their partners’ diabetes management. In this study, Batson et al.’s (1991) framework of altruistic versus egoistic motives for helping was used to examine the motives for spousal involvement in a partner’s diabetes management. We also examined whether those motives were associated with spouses’ reported frequency of diet-related spousal involvement in the form of support and control. Given gender differences in diet-related spousal involvement in the context of diabetes (August et al., 2020; Dimova et al., 2021), we further sought to examine gender differences in these motives as well as in the associations between motives and frequency of involvement.
Spousal involvement in a partner’s disease management
Among married individuals, spouses are the social network member most often involved in disease management (Revenson et al., 2016), particularly the dietary component (Dimova et al., 2021). In the context of type 2 diabetes management, spouses are involved in providing emotional support to their partners (Helgeson et al., 2016; Iida et al., 2010) as well as helping with the day-to-day tasks of diabetes management such as facilitating adherence to a healthy diet. Two specific ways spouses are involved in promoting a healthy diet are by providing diet-related social support or exerting diet-related control. Diet-related social support involves providing encouragement and positive feedback to individuals who are attempting to engage in healthy dietary behaviors (Franks et al., 2012; Williams and Bond, 2002). Among couples managing type 2 diabetes, this type of support has been shown to be related to better dietary behaviors and positive psychological outcomes as well as positive psychological and relational outcomes for both members of the couple (August et al., 2013; August and Sorkin, 2011).
Another way spouses can be involved in facilitating their partners’ adherence to healthy dietary behaviors is by exerting diet-related social control (Lewis and Rook, 1999; Stephens et al., 2013). Two types of social control have been distinguished in the literature: pressure and persuasion. Pressure (sometimes referred to as “negative” social control tactics) refers to strategies that typically elicit negative emotions in the recipient and can include nagging and criticism; persuasion (sometimes referred to as “positive” social control tactics), in contrast, refers to strategies that typically elicit positive emotions in the recipient and can include gentle reminders and expressions of worry (Stephens et al., 2009). Similar to investigations of diet-related support, most research has focused on whether social control is beneficial or detrimental in promoting better dietary behaviors and emotional well-being in the recipient; it appears these effects may differ depending on which tactic is used. In studies that have examined diet-related social control in the context of type 2 diabetes, researchers have found that persuasion is related to more positive outcomes and pressure is related to more negative outcomes (August 2021; Helgeson et al., 2016; Stephens et al., 2013).
Not all spouses engage in this type of support or control, however. Efforts to understand potential motives spouses may have for being involved in their partners’ disease management may help explain some of the variability in support or control attempts directed toward an important component of their partners’ treatment regimen.
Potential motives for spousal involvement in disease management
Although little empirical research has examined why spouses might be involved in their partners’ disease management, types of motivations delineated in the helping literature by Batson et al. (1991), can provide some guidance. According to Batson and colleagues, there are altruistic and egoistic motives for helping, whereby altruistic motives involve helping for the sake of benefitting another individual, whereas egoistic motives involve helping as a way to provide benefit to oneself. Variability in the extent to which individuals have altruistic versus egoistic motives for helping have been reported – even among couples in close relationships (Feeney et al., 2017; Feeney and Collins, 2001, 2003; Park et al., 2011; Sprecher and Fehr, 2005). Yet few studies have examined the usefulness of this distinction among longer-partnered couples in the context of disease management. One of the goals of our study therefore was to understand whether this distinction is indeed valuable in this population and in this context. In the current study, we adapted a measure from a study by Feeney and Collins (2003) of 194 young adult couples that validated a measure of motives for caregiving.
Altruistic motives
The extent to which spouses love, are concerned for, and feel interdependent with their partners may be altruistic motives to be involved in their partners’ disease management. Close relationships, such as marriage, are often interdependent (Arriaga, 2013); this level of interdependence, or feeling an overlap between one’s self and another, has been found to be related to helping (Cialdini et al., 1997). Researchers have posited that as a result of this interdependence, efforts by spouses to facilitate healthy behaviors in their partners may be perceived as reflecting spouses’ caring and concern (Lewis et al., 2004; Rook et al., 1990). Other lines of research have likewise found that empathic concern is a motive for helping (Batson et al., 1991). Finally, feelings of love also have been described as an altruistic, or “otherish,” motive for helping (Crocker et al., 2017).
Positive strategies to facilitate healthy behaviors such as support and persuasion are more likely to be attributed to such altruistic motives (Lewis et al., 2004). Consistent with this idea, Feeney and Collins (2003) found that feelings of love, concern, and interdependence were positively associated with responsive types of caregiving (e.g., provision of support) and negatively associated with controlling types of caregiving. Other research has likewise found that altruistic goals, or motives, are associated with an increase in the level of support in close relationships (Crocker and Canevello 2008). These types of motives are therefore expected to be particularly relevant to support provision (and possibly also relevant to persuasion, which despite being a type of social control, is considered a more positive type of interaction; Lewis and Rook, 1999; Stephens et al., 2009). No studies to our knowledge, however, have examined how these motives are related to specific types of involvement in the disease management context.
Egoistic motives
Feeling obligated to help one’s partner is considered an egoistic motive. Spouses may perceive such an obligation to avoid negative personal consequences – for example, feelings of guilt, concern about “looking bad” to others, or their partners’ dissatisfaction with their lack of help (Crocker et al., 2017; Feeney and Collins, 2003). Researchers have proposed that in some cultures (e.g., Asian and Latinx cultures), familial obligation is an important component of diabetes management (Peyrot et al., 2018), and may extend to spousal diet-related involvement in this context (August and Sorkin, 2011). Though researchers have found greater obligation to be associated with more controlling and overinvolved types of caregiving (Feeney and Collins, 2003), there is a need for more empirical evidence to understand whether this motive is also relevant to the type and extent of involvement in disease management.
Self-benefit is seen as an egoistic motive in which spouses expect something for helping their partner (Feeney and Collins, 2003). Similar to findings for obligation, this type of motive has been found to be related to controlling and overinvolved types of caregiving (Feeney and Collins, 2003). Other research suggests that individuals with more egoistic motives tend to provide little support to their partners (Crocker et al., 2017). In line with these findings, spouses might engage in more coercive (controlling) tactics to ensure their partners are eating a healthy diet to benefit themselves; these benefits could include shared eating habits in the household or other potentially desirable consequences associated with their partners’ healthy eating (e.g., weight management).
Finally, the perception that one’s partner is needy or incapable of handling problems on their own can be considered another egoistic motive for involvement in a partner’s disease management. Although it may appear to be an altruistic motive, other researchers have argued that it actually may be egoistic, as perceiving one’s partner as incapable or needy may be viewed by the spouse as burdensome and elicit a sense of obligation; alternatively, it can elevate the spouses’ status by making them feel their partner is dependent on them. As such, this motive has been found to be correlated with other egoistic motives (Feeney and Collins, 2003). In a qualitative study of 146 young adults, researchers found that support recipients thought that their partners viewed them as incapable based on the type of support their partners provided (Zee et al., 2018). According to support and control theorists (Rook et al., 2010), health-related social support is provided when providers perceive the recipient to be able to self-regulate their own behaviors, whereas health-related social control is exerted when providers perceive the recipient to be unable to self-regulate their own behaviors. It therefore would be expected that this type of motive would be particularly relevant to exerting control.
Taken together, inferences can be made from the overall caregiving and support (and when available, health-related support and control) literature about different motives spouses may have for being involved in their partners’ disease management. Whether these same motives are more or less important in understanding spouses’ involvement in the dietary component of a partner’s diabetes management is unknown.
Role of gender in motives for spousal involvement in disease management
There may be gender differences in spouses’ motives for being involved in their partners’ disease management as well as gender differences in associations between motives and diet-related spousal involvement. For example, women might be more motivated to care to for their spouses as they tend to be more health-oriented (Reczek and Umberson, 2012), take on a caregiving role in the relationship (Revenson et al., 2016), and are more involved in their partners’ diabetes, particularly the dietary component (Dimova et al., 2021; Mathew et al., 2012), than men. This idea is reflected in evidence that women engage in specific attempts to facilitate better dietary behaviors in a partner with diabetes through diet-related support and control (August et al., 2020; August and Sorkin, 2010; Rook et al., 2011).
Women have been found to generally be more altruistic, empathic, prosocial, and interpersonally-oriented than men (Andreoni and Vesterlund, 2001; Eagly and Koenig, 2006; Kamas and Preston, 2021; Umberson and Kroeger, 2016). In addition, women are more likely to have personality characteristics that make them more heavily invested in relationships, including their partners’ diabetes management (Helgeson et al., 2016). Yet little prior research has examined whether gender differences in these characteristics extend to gender differences in motives for being involved in a partner’s health. In the one available study on this topic, researchers found that men were more likely than women to care for their partners out of obligation or in hopes of receiving something in return (self-benefit) and less likely to care for their partners if they deemed their partner too difficult to help or they perceived their partner to be needy (Feeney and Collins, 2003). No research to our knowledge has examined gender differences in the association between spouses’ motives for involvement and their frequency of involvement in disease management.
The current study
This study addresses a gap in the literature by examining altruistic and egoistic motives spouses have for being involved in their partner’s diabetes management and whether these motives are related to how much spouses are involved in one important aspect of diabetes management, eating a healthy diet. Given gender differences in motives for caregiving (Feeney and Collins, 2003) and in diet-related involvement in the context of diabetes management (August et al., 2020; Dimova et al., 2021), this study attempted to further understand if these dynamics differed by gender.
Our first aim (Aim 1) was to examine the motives spouses reported for being involved in their partners’ diabetes management. We also sought to examine gender differences in motives for spousal involvement (Aim 1a). Consistent with past research, we predicted that the most common reasons cited for being involved were altruistic and that the least common reasons cited for being involved were egoistic (Hypothesis 1). We also predicted that women were more likely than men to cite altruistic motives for being involved in their partners’ diet, whereas men were more likely to cite egoistic motives for involvement (Hypothesis 1a).
Our second aim (Aim 2) was to examine whether motives for spousal involvement were related to spousal reports of the type and frequency of spousal support and two types of control (pressure and persuasion). We further sought to examine how the associations between motives for involvement and diet-related support and control differed as a function of spouses’ gender (Aim 2a). As there is limited research available to guide these hypotheses, these aims were exploratory.
Method
Design
This study involved a quantitative, cross-sectional design.
Participants
Participant characteristics by gender (N = 148).
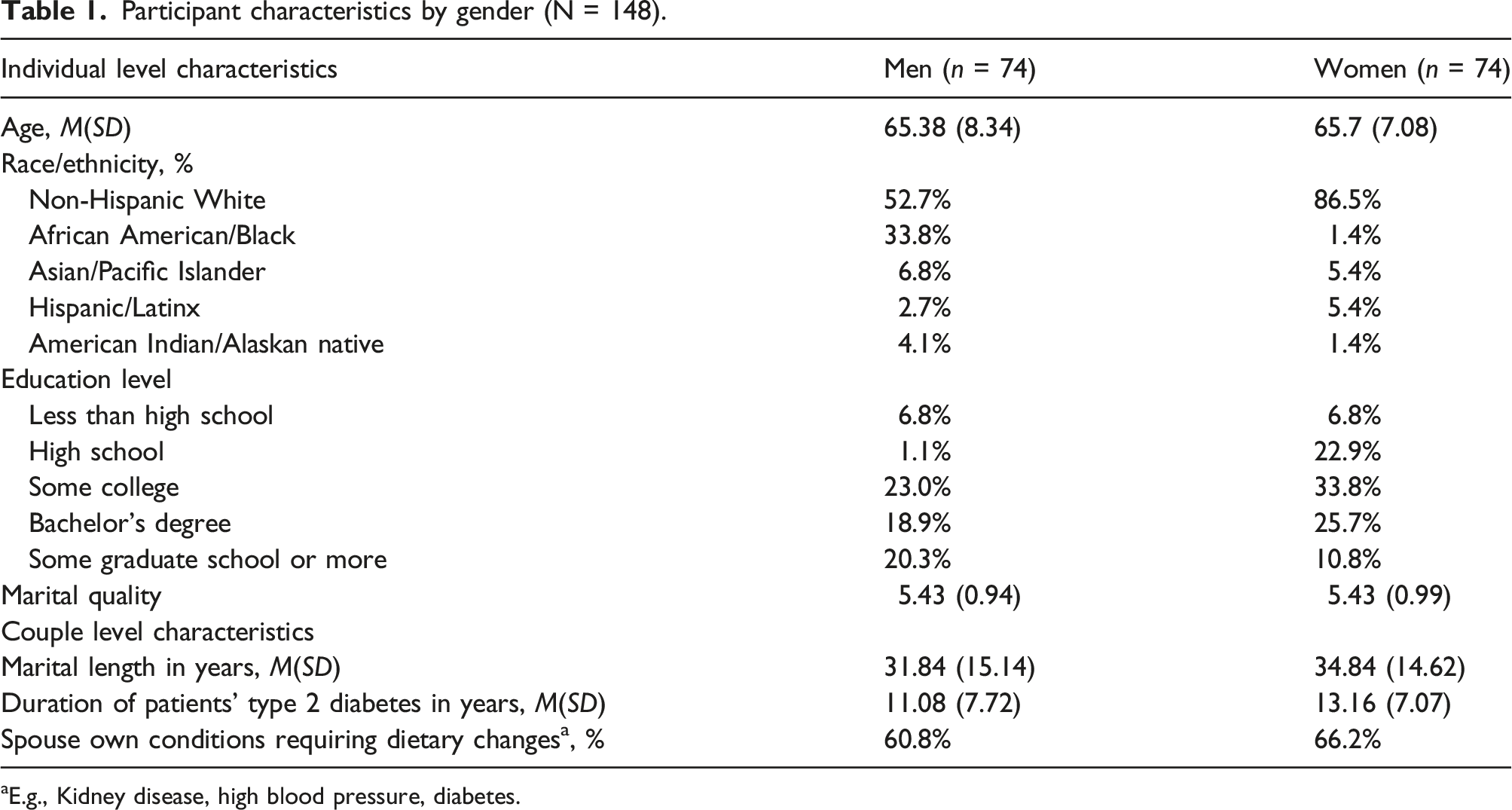
aE.g., Kidney disease, high blood pressure, diabetes.
Procedure
Participants were recruited from the United States via Qualtrics panels (Qualtrics, Provo, Utah) in January 2019. Quota sampling was used to ensure that there was a relatively equal number of men and women, and to ensure that at least 25% of racial/ethnic minorities were included in the study. Qualtrics worked with partner companies to send out anonymous survey links to panel members who might qualify for participation.
Eligible individuals completed online consent forms at the beginning of the survey. Participants were given instructions to complete the survey without any help from their partner. Once the participants completed their portion of the survey, their spouse was instructed to complete their portion of the survey immediately after; spouses were unable to go back to see their partners’ responses. Incentives for participants were provided by panel providers. The amount and type varied across providers, but were based on survey length, the panelist profile, and difficulty in acquiring the participant; examples included redeemable points, airline miles, and cash.
Data for the current study are available at https://rucore.libraries.rutgers.edu/research/.
Measures
Gender
Gender was coded as 0 (man) and 1 (woman).
Motives for spousal involvement in a partner’s disease management
We adapted a 15-item measure from Feeney and Collins (2003) in which participants rated their agreement on possible motives for spousal involvement in their partners’ diabetes management on a 6-point scale (1 = “strongly disagree,” 6 = “strongly agree”). Items were shortened from the original scale to be most salient to couples managing diabetes and for online administration. Items were averaged to create 4 subscales: (1) love/concern/interdependence (3 items; e.g., “You love your spouse and are concerned about his/her well-being; ” α = .71); (2) obligation (3 items; e.g. “He/she makes you help; ” α = .75); (3) self-benefit (5 items; e.g., “You will be rewarded [praised, thanked, honored, etc.] for helping your spouse; ” α = .86); and (4) needy/incapable partner (4 items; e.g., “Your spouse really needs your help; ” α = .82).
Diet-related spousal support
We used a 3-item measure adapted from Franks et al. (2012) in which participants rated the extent of their involvement on a 6-point scale (1 = “everyday,” 6 = “not at all; ” e.g., “do something to help your spouse stick with a healthy diet”). Items were averaged to create a composite scale (α = 0.88).
Diet-related spousal control
We used a 7-item measure adapted from Stephens et al. (2013) in which participations rated the extent of their involvement on a 6-point scale (1 = “everyday,” 6 = “not at all”). Items were averaged to create two subscales: (1) persuasion (3 items; e.g., “try to persuade your spouse to do more to follow a healthy diet;” α = 0.91) and (2) pressure (4 items; e.g., “criticize your spouse’s poor food choices;” α = 0.94).
As the focus of this study is on spouses’ own perceptions of their motives and how they are related to their own perceptions of their involvement in their partners’ diet, we chose to examine spouses’ versus patients’ reports of diet-related spousal involvement. We did, however, examine the extent of concordance between spouses’ and patients’ reports of spouses’ diet-related involvement in our descriptive analyses.
Covariates
Potential covariates were selected a priori based on previous literature on spousal involvement in a partner’s diabetes management and included age, race/ethnicity, marital length, marital quality (5-item Marital Quality Index; Norton, 1983; α = 0.98), and whether spouses had their own chronic condition that required dietary changes. Directed acyclic graphs (DAGs) were used to determine appropriate covariates to include in regression analyses (Diemer et al., 2021); gender, marital quality, and spouses’ own conditions requiring dietary changes met this criterion and were thus included in regressions.
Analytic plan
All analyses were conducted using SPSS version 28 software. Data were checked for completeness; there were 0–1.4% missing data; given the small amount of missing data, listwise deletion was used (Graham, 2009). Next, means, standard deviations, and intercorrelations for all key study variables were examined to provide descriptive information and to identify outliers.
Regression assumptions were checked; all assumptions except non-normality of the residuals were met; thus, bootstrapping using 1000 bootstrap samples was used to determine the sampling distribution of the estimates (Pek et al., 2018).
To address Aim 1, we examined means and standard deviations for each of the motives for spousal involvement. We then conducted a repeated measures ANOVA to examine whether some motives were endorsed to a greater extent than others. To address Aim 1a, we conducted independent samples t-tests to examine gender differences in each motive for spousal involvement. To address Aim 2, we conducted a series of multivariable regression models to examine how motives for spousal involvement were related to the frequency of different types of diet-related spousal involvement; separate models were examined for each type of motive and diet-related spousal involvement to determine the extent to which each motive was related to diet-related spousal involvement without accounting for shared variance between motives. To address Aim 2a, we calculated interactions between each (centered) motive and gender and added them to the models in Aim 2 to determine whether gender moderated associations between motives and diet-related spousal involvement; again, separate models were run for each type of diet-related spousal involvement.
Results
Descriptive results
Means, standard deviations, and correlations among key study variables by gender.

Note: Men’s correlations are above the diagonal and women’s are below. Men = 0; Women = 1.
*p < .05. **p < .01. ***p < .001.
For men, the motives, love/concern/interdependence, obligation, and needy/incapable partner, were significantly and positively related to support, whereas there were no significant bivariate associations between any of the motives and support for women. For both men and women, the motive, needy/incapable partner, was significantly and positively related to persuasion and pressure; self-benefit was also significantly and positively related to persuasion and pressure for men, and obligation was significantly and positively related to persuasion and pressure for women.
Results from pairwise intraclass correlations revealed significant, moderate correlations between spouses’ reports of providing and patients’ reports of receiving diet-related support (r = .63, p < .001), persuasion (r = .65, p < .001) and pressure (r = .72, p < .001). This relatively high level of concordance supports the idea that for the most part, spouses and patients are in agreement on the extent of these diet-related interactions.
Finally, as expected, there were gender differences in all types of diet-related spousal involvement, with women reporting greater involvement in their husbands’ diet than men’s involvement in their wives’ diet.
Motives for spousal involvement in diabetes management
In testing Aim 1, love/concern/interdependence was the motive that spouses agreed with to the greatest extent, with 87.8% of men and 91.9% of women endorsing this motive. Self-benefit was the motive that spouses agreed with the least, with 27.0% of men and 16.2% of women endorsing this motive. Findings from a repeated measures ANOVA revealed that participants significantly differed in the extent to which they endorsed different motives (F (3) = 147.35, p < 0.001, ηp2 = 50). Pairwise comparisons with a Bonferroni adjustment revealed that all motives were significantly different from each other (all ps < 0.013). Finally, t-tests that tested Aim 1a did not reveal any significant gender differences in any of the motives.
Associations between motives for spousal involvement and diet-related spousal involvement
Motives for spousal involvement in diabetes management predicting frequency of diet-related involvement.

Note: All models controlled for gender, marital quality, and spouses’ own conditions requiring dietary changes. Models were run separately for each motive. Unstandardized coefficients (B), standard error (SE), and bootstrapped 95% confidence intervals (CI) of the estimates are reported.
*p < .05. **p < .01. ***p < .001.
Finally, in testing Aim 2a, gender did not moderate any of the associations between motives and diet-related spousal involvement. The results are therefore not presented in the table.
Discussion
Not all spouses are involved in their partners diabetes management to the same extent. Variability in this type of involvement may be partially explained by motives spouses may have for involvement, which may be either altruistic or egoistic in nature (Batson et al., 1991; Feeney and Collins, 2001, 2003). Overall, our results suggested that spouses were most motivated to be involved in their partners’ diabetes management for altruistic reasons and the least motivated to be involved for egoistic reasons. In addition, all types of motives were related to engagement in diet-related spousal support, whereas only egoistic motives were related to engagement in diet-related control (persuasion and pressure). Gender did not appear to be important with regard to the extent to which participants agreed with the motives or in the associations between motives and diet-related spousal involvement.
Motives for spousal involvement in diabetes management
Consistent with our hypothesis (Hypothesis 1), the motive for being involved in a partner’s diabetes management that spouses most commonly cited was love, concern, and interdependence. As spouses in this sample were in high quality marriages, on average, it is not entirely surprising that they were motivated to be involved for this altruistic reason. This idea is consistent with findings from Feeney and Collins’ study (2003), in which romantic partners’ perceptions of their relationship quality were related to greater altruistic motives for caregiving. Other research also has found that other-ish goals and motives are related to better relationship quality (e.g., Hadden et al., 2013; Canevello and Crocker, 2010). It is therefore likely that there is a cyclical relationship between relationship quality and being motivated to help one’s partner for these reasons.
Also consistent with our hypothesis, the least commonly cited motives were egoistic motives. Yet, participants still reported that they endorsed these motives to some extent, despite potential social desirability concerns, suggesting that there are other reasons besides love and concern that might drive spouses to be involved in their partners’ diabetes management.
Self-benefit was the least endorsed type of egoistic motive. In intimate relationships such as marriage, individuals are usually concerned with the overall well-being of their partner without the expectation of them returning the favor (Väänänen et al., 2005). Other research likewise suggests that in these types of relationships, reciprocation is not direct, but instead, is responsive to the other person’s needs (Crocker et al., 2017). Further, older adults (the age group of which the majority of the current sample is comprised) tend to be less concerned than other age groups with reciprocity in their close relationships (Lang et al., 2013).
Notably, despite significant differences in how much spouses endorsed each motive, there were small to medium correlations between many of the motives. These findings could also reflect the idea that there are varied motives for involvement in a partner’s disease management, given the central role spouses play – and are expected to play – in that regard (Revenson et al., 2016; Rook et al., 2011). Another explanation could be that in longer-term couples in which there are overlapping senses of self, the lines between what is considered altruistic versus egoistic may be blurred.
Contrary to predictions and inconsistent with other studies (e.g., Feeney and Collins, 2003), we did not find any gender differences in these motives. This finding was surprising as men are typically not expected to be, nor are they involved as much as women are, in their partners’ disease management (Rook et al., 2011) – which is further reflected in gender differences in actual spousal involvement (e.g., August and Sorkin, 2010). However, the one study that did find gender differences in motives for caregiving (Feeney and Collins, 2003) examined general caregiving and support that young adults provided to their partner, while the current study explored support and control that middle aged and older adult spouses provide to promote better health behaviors in the context of disease management; thus, it is possible that motives for this type of involvement in mid to late life may differ from caregiving in a younger age group. Additional research is therefore needed to better understand the nature of gender differences (if any) in these motives.
Associations between motives for spousal involvement and diet-related spousal involvement
All types of motives were related to more frequent spousal provision of diet-related support. Although we expected that altruistic motives, such as love, concern, and interdependence, would be related to more frequent support, as it is a more responsive and effective type of involvement, egoistic motives also were related to more frequent support. In fact, the type of motive that had the largest effect size in predicting support was obligation. Given the importance of diabetes management, particularly diet, to a partner’s overall health (Centers for Disease Control and Prevention, 2022) spouses may feel obligated to be involved, and as a result, use support at a greater frequency to ensure their partners are eating healthily. It is important to note, however, that, like the other types of motives, the effect size for this motive was relatively small in predicting diet-related spousal support.
These findings, coupled with significant positive correlations between many of the motives, could suggest that the motives assessed in this study might be tapping into some individual difference factor that reflects a general preference for helping. Additional research that also assesses individual differences as potential predictors of spousal involvement might help further shed light on these findings.
In contrast to findings for support, only egoistic motives - self-benefit, obligation, and perceiving one's partner as needy or incapable - were related to more frequent social control. Other research suggests that egoistic motives are related to controlling and overinvolved caregiving (Feeney and Collins, 2003) and ineffective types of support (Feeney and Collins, 2001). Health-related social control is controlling by nature, but also could be construed as a type of overinvolvement as it is rarely welcome because it can (indirectly or directly) connote that one’s partner is unable to regulate their own behavior and thus threaten that individual’s autonomy (Lewis and Rook, 1999). Further, it is not always found to be an effective form of involvement, although persuasion is typically more effective than pressure (e.g., August 2021; Stephens et al., 2013).
The type of motive that had the largest effect size in predicting both types of control (persuasion and pressure) was perceiving one’s partner as needy or incapable partner. This finding supports the way health-related social control is conceptualized in the literature in which network members, such as spouses, “step in” to help regulate an individual’s behavior when they perceive that individual as being unable to self-regulate their own behavior (Lewis and Rook, 1999). Thus, if spouses perceive their partner to be more needy or incapable of their own disease management, they may be more likely to be involved in controlling their diet at a greater frequency.
The only type of motive that was not associated with how frequent spouses engaged in control was love, concern, and interdependence. As noted above, (lower) relationship quality may be tied to this motive for involvement, and other studies have found an inverse association between social control and relationship quality (e.g., August et al., 2013). Thus, even though love, concern, and interdependence was the most commonly endorsed motive and most couples in the study reported a high level of relationship quality overall, we found evidence that other motives may be related to social control, which (particularly pressure) has been conceptualized as a negative type of interaction (Lewis and Rook, 1999; Stephens et al., 2009).
Despite motives being differentially related to diet-related spousal involvement for men and women in bivariate analyses, gender did not significantly moderate associations between motives and diet-related spousal involvement in regression analyses that controlled for marital quality and spouses’ own conditions requiring dietary changes. Again, this finding is surprising, given existing gender differences in the literature in this type of involvement (e.g., August and Sorkin, 2010; Rook et al., 2011). It is possible then that regardless of gender, if a spouse is motivated to be involved, they will be involved to a greater extent. As noted above, this may be reflected by an individual difference in preference for helping.
Limitations
There are several limitations to this study that need to be considered in interpreting the results. One limitation is the cross-sectional nature of the data, precluding a determination of the direction of effects. It is possible that spouses’ involvement affects their perceptions of their motives for involvement, which is the opposite direction of what we hypothesized. Another limitation is the lack of diversity of the sample, which limits generalizability to other populations. Specifically, most participants in the study were White, of higher socioeconomic status, and in long-term, high-quality marriages. In a related vein, we only examined gender as one possible contextual factor in understanding these relationship dynamics; as gender is not independent of other social identities and heterogeneity in relationship experiences exist as a result of intersectional identities such as race/ethnicity and socioeconomic status, examining these intersectional identities is an important direction for future research.
In addition, the questions used to assess motives for spousal involvement may not have fully captured all of the possible motives for involvement in a partner’s diabetes management. For example, in some couples, one spouse is considered the “health expert” (Reczek and Umberson, 2012) and may be more involved in their partners’ diabetes management due to greater health-related knowledge. For the sake of brevity, we also did not use the full scale developed by Feeney and Collins (2003), nor were their open-ended options for participants to share other possible motives, and thus we may not have captured all potential spousal motives for involvement in this context. Similarly, we only examined spousal involvement in one domain of diabetes management – specifically, involvement in dietary behaviors. Motives were assessed with regard to any type of involvement (up to the interpretation of the participant), however. Although diet is a common component of diabetes management (CDC, 2022), and spouses are commonly involved in their partners’ dietary behavior, in particular, spouses may be motivated to be involved in other aspects of diabetes management (e.g., taking their partner to doctor’s appointments, making sure they were taking medications as prescribed); thus, findings may have differed if motives were only assessed with regard to the dietary aspect of diabetes management. In addition, results may have differed if we assessed spousal involvement in other disease management behaviors (e.g., physical activity and medication adherence). Finally, although the reports of egoistic motives and negative types of diet-related spousal involvement are consistent with relative rates reported in other studies (e.g., August and Sorkin, 2010; Feeney et al., 2017; Stephens et al., 2013), it is possible these are underestimates given social desirability bias; in addition, other factors not reported in this study (e.g., personality traits; August et al., 2020; Helgeson et al., 2016) are important to consider in understanding these motives and behaviors.
Conclusion
Despite these limitations, this study contributes to the literature by providing insight about the motives spouses have for being involved in their partners’ disease management. Spouses are motivated for a number of reasons but seem to be most motivated due to altruistic reasons. These motives, in turn, may “translate” into how often they are involved in different ways in one domain (diet) of their partner’s diabetes management; more research is needed, however, to understand whether motives are important in understanding whether spousal involvement is beneficial for patients’ actual diabetes management. Surprisingly, we did not find evidence of gender differences in these motives nor in how they were related to the frequency of involvement in their partners’ diabetes management.
These findings have the potential to inform the design of couples-focused chronic disease interventions, which have been found to be more effective than patient-only interventions for both disease management outcomes and overall relationship functioning (Martire and Helgeson, 2017). If spouses are not inherently motivated to help their partners, they may be less likely to help their partners with disease management or may engage in ineffective types of helping that are not consistent with their partners’ needs (Feeney and Collins, 2003). Helping spouses frame motives in a more altruistic way may therefore be beneficial in the sense that it could increase spouses’ sense of value and interdependence with their partner (Crocker et al., 2017). In addition, these types of motives also may lead to the type of involvement - support - that has been shown to be the most beneficial for the patient, partner, and relationship (e.g., August et al., 2013; Franks et al., 2006; Stephens et al., 2013).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Rutgers University Research Council Grant.