
Abstract
The study compared the effectiveness of Cognitive Behavioral Therapy (CBT) with biofeedback or with emotional expression in individuals with fibromyalgia, and a waiting list control group. 88 women participated in a naturalistic study with random assignment. The Fibromyalgia Impact Questionnaire, SCL-90R, and a visual analog quality of life scale were used. Both intervention groups improved, but differed in physical and emotional control response. Using the reliable change index procedure, clinical improvement occurred in 18.8% of participants, and 4.8% achieved scores comparable with clinical recovery. Greater specificity on therapeutic objectives is warranted.
Introduction
The diagnostic criteria for fibromyalgia (FM), established in 1990 and reviewed in 2010 by the American College of Rheumatology (ACR
From a biopsychosocial perspective, the psychosocial and functional consequences of chronic pain should be evaluated (Kashikar-Zuck et al., 2019; Turk et al., 2016) given its impact in the experience of pain and the response to treatment (Ang et al., 2010; Sil et al., 2014). There are FM patients for whom the severity of symptoms and the absence of response to treatment is associated with high levels of psychopathology, mainly anxiety and depression, and low quality of life (Litt and Porto, 2013; Luciano et al., 2016; Rowe et al., 2019; Yim et al., 2017). The complex and poorly understood etiology of FM (Bazzichi et al., 2011) makes identifying effective therapies particularly difficult, currently lacking consensus on the best treatment modality. In this context, clinical research suggests that interdisciplinary treatments with Cognitive Behavioral Therapy (CBT), as the central ingredient, improve outcomes in FM patients (Lami et al., 2013; Martín et al., 2012; Thieme et al., 2017).
CBT for FM patients often includes three components: (1) education about FM, (2) symptom management skills (behavioral, cognitive and emotional), and (3) life style changes (Janke et al., 2011; Society of Clinical Psychology, 2014), with the objective of decreasing the level of pain and improving general functioning. Several studies and meta-analyses have shown the efficacy of CBT in FM for decreasing negative emotions (anxiety and depression), pain, dysfunction (Bernardy et al., 2013; Gritzner et al., 2012), and for increasing general health (Schöder et al., 2017). Nevertheless, other studies (Bernardy et al., 2010) have questioned the efficacy of CBT. For instance Bernardy et al. (2018), showed non-statistically significant improvements in pain reduction, as did others with dysfunction (Thieme et al., 2005), and somatization symptoms. Others (Van Den Houte et al., 2017) have shown that the effects are limited and often do not persist. Finally, a systematic review (Glombiewski, 2010) also concluded that improvement is very limited.
CBT for FM patients also has been applied with Biofeedback (BF) (Castelnuovo et al., 2016). This is a well-established intervention in which patients' bodily responses are monitored and reported to the patient through an auditory or visual modality. Applied to FM, muscular tension has received most attention, measured through the Electromyographyc-Feedback (EMG-BF) by electrodes applied to the forearm extensors and upper trapezius, to learn to control and to alleviate the muscles’ tension. Diverse meta-analytic reviews (Castelnuovo et al., 2016; Glombiewski et al., 2013; Laevsky et al., 2014; Markozannes et al., 2017; Palermo et al., 2010) indicated that EMG-FB results in a decrease in pain intensity, but not in depression, fatigue or health-related quality of life in comparison with control groups. Other studies, nevertheless, obtained improvement with the EMG-FB also in somatic symptoms (Caro and Winter 2011), anxiety, depression and quality of life (Kayiran et al., 2010), but the best results were obtained when combined therapies were used. For instance, Collado et al. (2001) applying EMG-BF combined with CBT, obtained significant improvements in depression and anxiety. In sum, there is scarce and contradictory knowledge about this treatment option for FM. Thus, the aim of the present study is to gather evidence about the effectivity of EMG-BF for FM, evaluating the effect of two CBTs, a group combined with EMG-FB (T1) and a group without EMG-FB (T2), and comparing them with a waiting list and control normative groups.
Method
Participants
With the support of a local FM patient association, 200 individuals were invited to participate. The Flow Chart in Figure 1 shows that 60 subjects declined and 52 were excluded for not fulfilling the inclusion criteria (to be a female, to have a FM’s diagnosis, not undergoing other psychological treatments, and not suffering other diseases that could influence the evolution of the symptomatology). Of 88 selected patients, 33 were assigned to the CBT with EMG-BF treatment (CBT+BF), 33 to the CBT treatment (CBT), and 22 to the Waiting List (WL) control group. 32, 32 and 20 participants completed their respective treatments. A convenience sample of 47 volunteer women with no FM diagnosis, matched by age and without pain related disorders was recruited as the normative control group. In all, the final sample was constituted by a total of 131 women. Flowchart diagram.
Instruments
A questionnaire including personal data and medical and psychological information was used. It asked about age, marital status, educational level, and occupation, and included five items to assess age of onset, course of symptoms, presence of previous psychopathology, previous treatments, and disability status. It also included the disability index according to Spanish legislation (Spanish Ministry of Social Affairs, 2007). Quality of life was assessed with a single item, using a visual analog scale, where participants have to indicate from zero to 10 their current perceived quality of life. This single item instrument has adequate psychometric properties (Feng et al., 2021).
Psychopathology measures. SCL-90-R - Symptom Checklist-90-Revised (Derogatis, 1977) Spanish adaptation (González De Rivera et al., 2002). This self-report instrument consists of 90 items distributed in 10 scales of which only somatization, depression and anxiety are reported in this study. The instrument yields a global severity index (GSI), which is a measure of the intensity of global mental and psychosomatic suffering, and a positive symptom distress index (PSDI). Participants reported the frequency with which they have experienced these symptoms during the previous month. Results of a study conducted with Spanish samples (González De Rivera et al., 2002) suggested good reliability of the instrument, being consistent with those carried out by the author. Alpha coefficient values ranged from 0.81 to 0.90. Reliability analysis with the sample of this study showed high internal consistency (α = 0.90) and adequate temporal stability (r scores between 0.78 and 0.90) with a test-retest interval of 1 week.
Functional measures. FIQ - The Fibromyalgia Impact Questionnaire (Burckhardt et al., 1991) Spanish adaptation (Monterde et al., 2004). The questionnaire is a brief 10-item instrument developed to assess fibromyalgia patient status, progress and outcomes. In the Spanish version, the value of the total coefficient of intra-class correlation was of 0.81. The Spanish FIQ replicated the properties of the original version and its adequacy was confirmed for Spanish patients with FM (Monterde et al., 2004). In the present study the subscales of pain and fatigue, and total scale score have been used.
Muscle tension. Electromyographic biofeedback, EMG-BF, 77601-EMG Retrainer model (Chattanooga Group, 2020). The EMG Retrainer measures and quantifies muscle movement with the results displayed on a liquid crystal display (LCD), and can be programmed to assess the activity of healthy and damaged muscle. The dual channel unit is designed to continuously monitor muscle movement, provide visual and audio feedback, while allowing achievement of targets set in therapy. EMG Retrainer conditions voluntary control of muscle tension associated with stress, anxiety and pain by applying the electrodes to the forearm extensors and upper trapezius (neck). Participants learn, with the help of visual and auditory BF, to relax the muscles with cognitive and progressive muscle relaxation.
Data collection procedures
At pretest, after participants had given informed consent, we administered the assessment instruments to measure the dependent variables. The assessment was performed by a member of the research team, a graduate in Psychology, who had been trained to administer the assessment in a standardized way. The administration and scoring of the questionnaires was blind. Upon treatment completion, posttreatment assessment was carried out, and the same instruments as at pretest were administered. The control waiting list group included 22 persons and instruments were administered by the same professional.
Treatment
Based on the standards of the Society of Clinical Psychology (American Psychological Association, Division 12) (2014), we developed a multi-component cognitive behavioral treatment for FM, that combines education, symptom management skills, and life style changes
The main difference between the two treatments was the use of EMG-BF for the relaxation and anxiety reduction techniques in CBT-BF (Glombiewski et al., 2013; Laevsky et al., 2014; Markozannes et al., 2017), and no EMG-BF in CBT. EMG-BF electrodes were applied to the forearm extensors and upper trapezius (neck), for 10 sessions during 25 min, and participants learned, with help from visual and auditory BF, to relax these muscles with cognitive and progressive muscle relaxation, and in every session, measures of muscular tension were registered. Thus, T1 dedicated more time to learning to control muscle tension and to relax using EMG-BF, whereas in T2, more attention was paid to emotional regulation: coping strategies, self-esteem, and acceptance of negative emotions. Each session had three components: a review of the previous session, the CBT intervention and, either the BF or the emotional regulation component. Debriefing was given to all participants and treatment was offered to control participants at the end of the study. Both treatments were supervised by an expert clinician.
Data analysis
For the description of the results, the Mean (M) and Standard Deviation (SD) in the case of quantitative variables, and the frequency (n) and percentage (%) in the case of nominal variables were calculated. For the contrast of averages between groups in the baseline scores the F test of variance analysis was used with application of the Brown-Forsythe robust test in the case of heterocedasticity of variances. In the case of nominal variables, the contrast of proportions was performed through the Chi-square (χ2) test (or the exact test in case of expected low frequency). The contrast of change between post-treatment and baseline as a function of the three clinical groups was carried out by means of a variance analysis of repeated measures, with estimation of within-group, between-group and interaction effects. The effect size of the omnibus test was performed through the eta square (η2) and for the contrast change of each group the d Cohen for related groups.
Following The Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) (Dworkin et al., 2009), we used an alternative methodology to evaluate the effectiveness of these interventions, the Reliable Change Index (RCI) (Jacobson and Truax, 1991). Compared with standard evaluations pre-post treatment, this methodology estimates, besides the statistical significance of the change, its clinical relevance. It provides a more precise indication of clinical changes, allowing individualized decisions for health providers (Montero et al., 2015). Given the great variability of symptoms and course, it seemed advisable to apply and to evaluate interventions in an individualized manner, or at least in clinical subgroups. Consequently, the present study evaluated the effect of two CBTs (a group therapy combined with EMG-BF and a group therapy without EMG-BF), in measures of pain, functioning and psychopathology, using the RCI to estimate clinical changes.
Results
Descriptive statistics and comparison of participants in sociodemographic variables.

Descriptive statistics and comparison of clinical variables at baseline.

Post hoc comparison between groups that reached statistical significance. na: non applicable.
Outcomes based on intention to treat analysis: Pre- and Post-intervention comparison of participants randomized to the group Cognitive Behavioural Therapy (CBT), Cognitive Behavioural Therapy plus bioFeedBack (CBT+FB), and the Waiting List (WL) conditions.
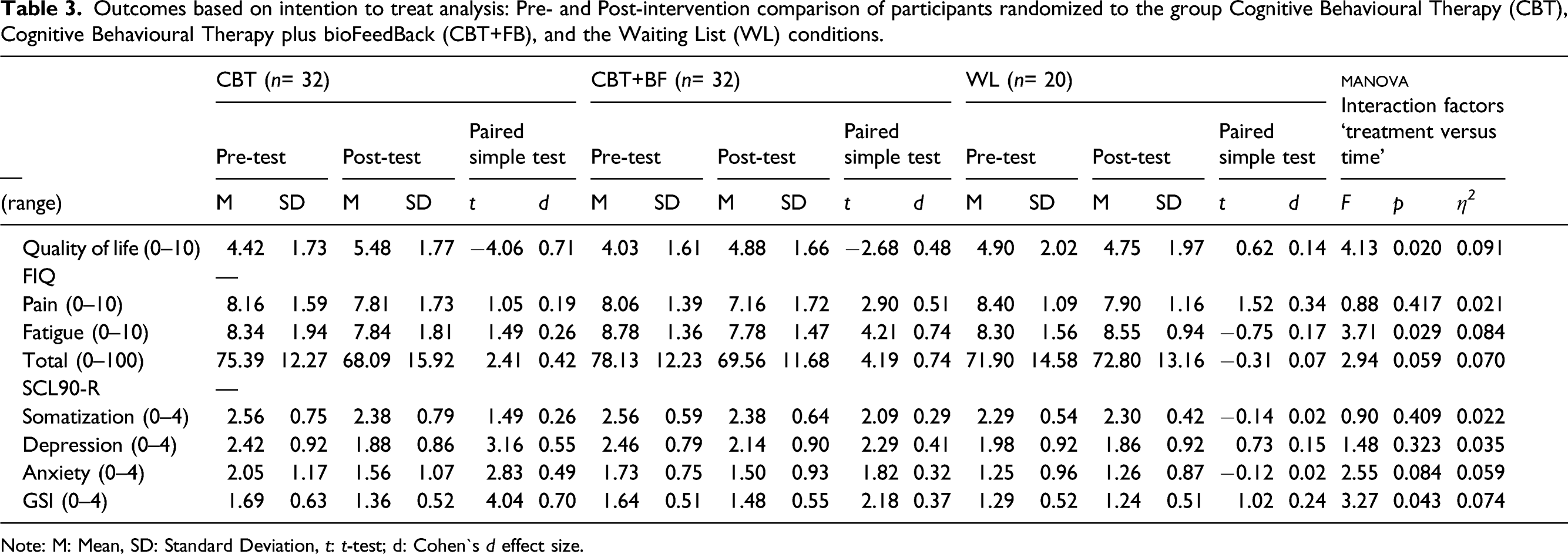
Note: M: Mean, SD: Standard Deviation, t: t-test; d: Cohen`s d effect size.
With regards to the SCL-90-R a statistically significant interaction (p = 0.043) was found for the GSI and approaching significance (p =. 084) for anxiety. While changes observed in the CBT+BF and WL groups are non-significant, there is an evident reduction (d = 0.49) for the CBT group. In terms of the GSI, no changes are found between base line and post-treatment for the WL group, but a reduction is observed in the two treatment groups with a higher effect in the CBT group (d = 0.70) versus the CBT+BF group (d = 0.37). A similar finding was obtained for the quality of life measure: an interaction effect (p =. 020; Ƞ 2 = 0.091) in which the waiting list deteriorated in quality of life, treatment groups showed and improvement, higher for the CBT only (d = 0.71) than for the CBT+BF group (d = 0.48).
Following Jacobson and Truax (1991), a subsequent analysis of the total FIQ score was performed. As can be seen in Figure 2, there is a diagonal central area where no change cases are plotted, cases whose change could be due to chance. In the upper left side, cases with an increase in their scores, that is, a relapse or aggravation in their condition. In the bottom right side there are two areas separated by a cutoff point calculated following Jacobson and Truax (1991) that resulted in a score of 51.38. Scores below this cutoff point show a functionality level similar to the normative population and higher scores indicate non functionality. Applying this cutoff criterion, two improvement groups are identified: one with improvements but still non-functional (12.8% of all cases) and another with reductions but below the cutoff point, moving to functionality levels and therefore showing recovery (4.8%). As it can be seen, most participants (81.2%) are located in the no change area (waiting list 85%, CBT 81.8% and CBT+BF 78.1%). Only one individual of the waiting list group presented deterioration (1.2%), four women showed recovery (4.8%), two from the CBT groups, one from the CBT+BF group and another one of the waiting list group, and the rest had a non-significant clinical improvement (12.8%). The contrast of prevalence was non-significant (χ
2
(6)= 5.45; p= 0.511). Reliable change index.
Discussion
Psychosocial and functional consequences of chronic pain are a consistent finding in the literature (Litt and Porto, 2013; Luciano et al., 2016; Yim et al., 2017). Our study also confirmed statistically significant differences between the clinical groups with FM and the normative group without FM, showing the clinical groups’ higher prevalence of clinical symptoms like pain, fatigue, (FIQ) anxiety, depression (SCL-90-R), and lower level of quality of life, and with these differences remaining after the treatment.
The major aim of this study was to assess if the treatments applied produced an improvement in the clinical symptoms and quality of life of the groups with FM. In this sense the results were mixed. On the one side, the treatments produced significant improvement in the two groups treated as in other studies (Bernardy et al., 2013; Schöder et al., 2017). But on the other side, clinical symptom scores continued to be higher than those of the normative group, that is, although the improvement was statistically significant, at the clinical level it did not become significant, and did not achieve a sufficient effect to see recovery or normalized functional capacity in people with FM, as other studies concluded (Bernardy et al., 2010; Thieme et al., 2005; Vazquez-Rivera et al., 2009). From this point of view, the methodology applied in this study, called Reliable Change Index (RCI) (Jacobson and Truax, 1991), can help identify effective therapies.
In terms of the differences between the two treatments: CBT and CBT combined with EMG-BF, it was observed that these two different treatment modalities improved different symptoms, showing different specificities: CBT+BF reduced somatic variables like fatigue and general functional capacity (FIQ), showing a significant effect size and a large difference with CBT; however CBT alone resulted in a higher reduction of psychopathological symptoms like anxiety (SCL-90-GSI), and higher improvement of quality of life, while the waiting list group suffered a deterioration. These differences can be explained if we take into account that in CBT alone, more time was spent on coping strategies about the illness, improving psychological and emotional variables (anxiety and quality of life), coinciding with other studies (Thieme et al., 2005; Vazquez-Rivera et al., 2009). Nevertheless, in CBT with EMG-BF more time was spent in the use EMG-BF to control physiological variables like the muscular tension and breathing, thus achieving greater improvement in physiological variables like fatigue, results similar to those obtained by Caro and Winter (2011). The methodology used in this study provided a more precise indication of clinical changes with different treatments (Montero et al., 2015), so as to make individualized decisions about which treatment to choose, given the great variability of symptoms, course, and the patients in FM.
It should also be noted that while CBT and CBT with EMG-BF improved to some degree or maintained the condition of people that received treatment, the waiting list control group showed deterioration. Therefore, although these treatments do not produce a total recovery of individuals affected by this chronic disease, they seem to be a useful resource to prevent further deterioration and to improve quality of life. However, it is necessary to mention, as a study limitation, the short time of follow-up of the participants after the treatment. The follow-up was done 6 months after the completion of the treatment, which does not allow for an understanding of the longer-term development of the participants’ condition and whether there might be differences between the CBT groups with or without EMG-BF. Given the paucity of studies in this regard, it seems important to raise the temporal variable of evolution of people with FM, as a future line of research, posing as a hypothesis, the appearance of a greater deterioration in people with FM who do not receive psychological treatment, and the importance of creating support groups to maintain the learning acquired in the treatments.
Finally, the usefulness of the Reliable Change Index (RCI) (Jacobson and Truax, 1991) is evidenced in this study and others (Montero et al., 2015), allowing us to identify the two fundamental aspects in the therapeutic change: its statistical and clinical significance. The possibility of obtaining relevant clinical information about each individual patient during the course of treatment allows for the design of the treatment based on the idiosyncrasy of each person, thus working from a more person-centered model, and improving the effectiveness of treatments.
Footnotes
Acknowledgments
We would like to thank Bize Bide Association of Gipuzkoa, Basque Country, for supporting this study and to all participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Ethical approval
All procedures in this study were in accordance with the ethical standards of the Bizibide Fibromyalgia Association Research Committee and the 1964 Helsinki Declaration and its subsequent amendments or comparable ethical standards.