
Abstract
This study aimed to assess the relationships between socioeconomic position, perceived stress and Health Related Quality of Life (HRQoL) of patients with hypertension. Data were obtained using the baseline survey of 258 patients from the Social Determinants and Inequities in the Control of Blood Hypertension Program (ProDSICHA). HRQoL was measured with SF-8 Health Survey. Socioeconomic position was measured using education, and the MacArthur Scale. Stress was measured with Perceived Stress Scale. A higher educational level was associated with a higher perception of stress (Coeff = 0.78, p = 0.019). Also, a lower position in the community was associated with a higher perception of stress (Coeff = −0.56, p = 0.027). A higher level of perceived stress was associated with a higher level of mental health (Coeff = 0.64, p = 0.000). No statistical differences were found in the relations between socioeconomic position and physical HRQoL. These findings warrant further research to understand the role of socioeconomic position in physical HRQoL.
Introduction
Hypertension is a major health problem worldwide, and the main cause for cardiovascular disease (World Health Organization, 2013). Its occurrence globally is increasing, and projections estimate a 30% increase in its prevalence by 2025 (Kearney et al., 2005). Low and middle-income countries like Colombia are at higher risk for hypertension (Sánchez et al., 2009), possibly due to factors such as socio-economic inequalities, poor environmental conditions, increasing trends in unhealthy behaviors, and excessive body weight, aging population, and deficient primary health care strategies (Lucumi et al., 2016, 2017; Sánchez et al., 2009; Sarki et al., 2015). In Latin America countries, hypertension prevalences are high, being the countries with the highest prevalence: Brazil (25–35%), Paraguay (34%), Chile (33.7%), Uruguay and Venezuela (33%) (Sánchez et al., 2009). In Colombia, studies estimate a prevalence of 25% for hypertension (Lucumi et al., 2017), and low levels of treatment adherence and control of the disease (Herrera, 2012; Salcedo and Gómez, 2014).
Despite the relevance of hypertension to morbidity and mortality in countries such as Colombia (Lucumi et al., 2017; Sánchez et al., 2009), there is a paucity of research on social factors associated with hypertensive patients’ health-related quality of life (HRQoL), and the potential mechanisms through which these factors can act. Research, mainly in high-income countries, suggests that socioeconomic position is associated with HRQoL, and that perceived stress might be a potential mediator in the relationship between socioeconomic position and health (e.g. Zahran et al., 2005). What has not been so broadly studied is how perceived stress mediates the relationship between socioeconomic position with HRQoL in patients with hypertension in lower income countries. Figure 1 proposes a conceptual model that guides this research, and in the sections below, we further analyze the relationship between socioeconomic position, perceived stress, and HRQoL.

Mediation model with variables in the study.
Socioeconomic position and perceived stress
Socioeconomic position has been reported in the literature as a concept related to “numerous exposures, resources, and susceptibilities that may affect health” (Galobardes et al., 2006: 7). Studies have consistently found that a low socioeconomic position is associated with poorer health outcomes overall (Marmot, 2004; Whitehead, 1992) such as higher risk for hypertension (James et al., 2006) or higher mortality rates (Stringhini et al., 2010). Low socioeconomic position has been related to a poorer subjective health status (Read et al., 2016) and risky health behaviors such as physical inactivity, smoking, and poor nutrition (Pampel et al., 2010; Stringhini et al., 2010).
Educational level -an indicator of socioeconomic position (Galobardes et al., 2006) - has been linked to health outcomes, whereby studies have shown that higher levels of education are associated to a reduction of risky behaviors (smoking or heavy drinking) and declining obesity, whereby for each extra year of study, the risk for obesity reduces by 1.4% (Cutler and Lleras-Muney, 2009). A study in Cuba showed that lower levels of education increase the risk for hypertension by about 24% in women (Orduñez et al., 2005). Similar findings were found among Colombian women with a gradient in the association between low levels of education and hypertension (Lucumi, 2014).
Regardless of socioeconomic position, subjective social status (SSS) described as “a perception of rank on the social hierarchy” (Shaked et al., 2016: 1) has been associated with an increased likelihood of the development of several chronic diseases such as obesity, diabetes, and hypertension (Tang et al., 2016).
Socioeconomic position has also been related with stress. For example, socioeconomic disadvantage has been linked to higher levels of stress hormones in the blood stream (Cohen et al., 2006). Also, belonging to a low socioeconomic status (SES), has been linked to an increased risk of exposure to psychosocial stressors (Williams et al., 2016). In the association between SES and health, there is evidence that one of the mechanisms through which socioeconomic level affects health is its impact on perceived stress and health risk behaviors (Senn et al., 2014).
Perceived stress and quality of life
Perceived stress has been linked to negative impacts on HRQoL in the general population (Ames, 2001) and in groups with specific chronic health conditions (Miftari and Melonashi, 2015). Specifically, perceived stress has been related with lower levels of quality of life in patients with hypertension (Baune and Aljeesh, 2006; Santos et al., 2013).
To date, several studies have established a relationship between psychosocial stress and hypertension (Liu et al., 2017; Spruill, 2010). It has been shown that stress can either have a direct or an indirect influence on hypertension. Direct effects include a greater activation of the hypothalamus-pituitary-adrenal axis (HPAA) (Liu et al., 2017). Allostatic load, a “composite measure of physiologic response to chronic exposure to stress” (Zota et al., 2013: 1), has been mentioned as a possible mechanism between perceived stress in adverse psychological and physical situations, and poor health in individuals including hypertension (Mattei et al., 2010). Indirect effects of stress on hypertension are mainly linked to a higher prevalence of health risk behaviors (Cohen, 2004; Park and Iacocca, 2014). HRQoL can be further compromised in hypertensive patients, as physiological changes due to illness or hypertensive treatment can influence their wellbeing (Ogunlana et al., 2009).
Building on previous literature, we hypothesize that in patients with hypertension in Colombia, a middle-income Latin American country, (a) a lower socioeconomic position is associated with higher perceived stress; and (b) that perceived stress mediates the relationship between socioeconomic position and HRQoL of hypertensive patients.
Method
Study design and inclusion criteria
The Social Determinants and Inequities in the Control of Hypertension Program (ProDSICHA for its Spanish acronym) is a longitudinal study aimed at furthering our understanding of the effects of social determinants on hypertension in three Colombian cities. The inclusion criteria were as follows: adults aged between 45 and 70, with diagnosed hypertension, participants of ProDSICHA at the selected institution, and managed as outpatients. Participants with cognitive, neurological, psychiatric, or motor impairment that hinder response capacity to psychological tests were excluded. We used data from the first wave of ProDSICHA.
Population and sample
We designed the sample using a multi-stage sampling strategy (cities, institutions, and participants). In phase one, we selected three cities using heterogeneous criteria to examine the variations and similarities that the phenomenon may present in different contexts (Patton, 1990). We selected Bogotá, Medellín and Quibdó, considering differences in poverty levels and health service infrastructure. In phase two, we selected health insurance institutions with a hypertension control program. These health institutions provided patients with clinical consultation, as well as hospital services. In some institutions the majority of affiliates belonged to the subsidized health regime; and in other where the majority belonged to the contributory regime. Other selection criteria included coverage equal to or greater than the pre-determined sample size of each city, the existence in these institutions of an updated record of their service users and the institution agreement to participate in the study. In phase three, we selected the participants from a list obtained from each institution. Participants did not present any comorbidity, as a criterion to be part of the study. A stratified probability sampling strategy was used based on age and gender distribution.
Instruments and measurements
HRQoL
We used a four-point Likert scale including questions on eight health dimensions: general health status, pain, physical aspects, mental health, functional capacity, and emotional and mental, and social issues, known as the SF-8 Health Survey (SF™ Health Surveys) (Turner-Bowker et al., 2003). A higher score on this scale equals a better perception of HRQoL. Validation of the scale in Colombia showed good internal consistency and a Cronbach’s alpha of 0.85 (Ramirez-Velez et al., 2010).
Socioeconomic position
Objective socioeconomic position
To assess objective socioeconomic position, we used the variable education asking participants “What is the highest degree of education acquired by you?.” Responses ranged from No studies to Postgraduate studies.
Subjective socioeconomic position
We obtained participants’ subjective socioeconomic position using the MacArthur Scale of Subjective Social Status (Adler and Stewart, 2007). We showed participants a figure of a ten-rung ladder and asked them to rate their self-perceived status within their community without any reference to socioeconomic status (Fernald and Adler, 2008), followed by their self-perceived status in reference to the country as a whole, this time considering their occupational levels and income. The higher the rung selected, the higher the socioeconomic position perceived. In this paper, we only considered self-perceived status within the community.
Perceived stress scale
We measured stress using the Perceived Stress Scale (Cohen et al., 1983) to assess the degree to which people appraised daily life situations as stressful. Total score is obtained by sum the ten items of the scale and higher scores equal higher perceived stress in the individuals (Cohen et al., 1983). Colombian validation of the instrument showed good internal consistency (Cronbach’s α = 0.86) (Campo-Arias et al., 2009).
Statistical analysis
We performed the statistical analysis in three stages. First, we carried out descriptive analyses with demographic data and variables of interest, followed by correlation analyses to understand the relationship between the variables. Finally, we performed multivariate regression analysis. Significant level used was p ⩽ 0.05.
With respect to statistical mediation analysis, MacKinnon and Dwyer (1993) provided a sufficient approach for testing mediation based on regression equations for the mediation model that remain in common use today:


The difference in coefficients approach compares the relation between the independent variable and the dependent variable before and after controlling for the mediator. The logic behind the estimator is to ascertain whether there is a significant reduction in the effect of the independent variable on the outcome once accounting for the mediator. Conceptualizing mediation in this way does not promote intentionally considering the implied causal direction of variables in the model and may facilitate conflation of mediation effects and confounding effects. This test of mediation has historically been applied in epidemiology and the medical sciences (MacKinnon and Dwyer, 1993) and is commonly used to test mediation hypotheses in clinical nutrition research today (Albert et al., 2015; Jacobs et al., 2015; Jenab et al., 2015; Ma et al., 2016).
Mediation is quantified as the difference between the total effect of the independent variable on the outcome (i.e. c in equation (1)) and the direct effect of the independent variable on the outcome accounting for the mediator (i.e. c′ in equation (2)) by using this method. Statistical significance testing of the parameter estimate is conducted by dividing the ^c–^c′ difference by its corresponding normal theory SE:
The statistical analysis was performed using SPSS version 26 and the macro Process for SPSS.
Results
Demographics are showed in Table 1. Also, for each psychosocial variable, average and standard deviation were calculated as part of the descriptive analysis. We also present data differentiated by each city were information was recollected (Bogotá, Medellín, Quibdó), and show in the same table differences in these locations in regard to the main variables in our model (perceived socioeconomic position, perceived stress, and HRQoL).
Descriptive for perceived socioeconomic position, perceived discrimination, and perceived stress.

SD: standard deviation.
*p ≤ .05; ***p ≤ 0.001.
Results in Table 1 show differences in perceived socioeconomic position in the community, perceived stress and HRQoL by each city. Regarding socioeconomic position in the community, post hoc analysis showed differences between Bogotá and Medellín (Coeff = 1.48, p = 0.000) and between Bogotá and Quibdó (Coeff = 1.71, p = 0.000). For perceived stress, analysis showed differences between Bogotá and Medellín (Coeff = 3.58, p = 0.021) and between Medellín and Quibdó (Coeff = −5.63, p = 0.000). For mental HRQoL, the only significant differences were between Bogotá and Medellín (Coeff = 3.93, p = 0.027).
Mediation analysis
To understand the relations of influence between the variables in the model proposed, we performed two models, with physical HRQoL and mental HRQoL as a dependent variable. Tables 2 and 3 show those results.
Estimates of the effects of selected social indicators on physical HRQoL and perceived stress.
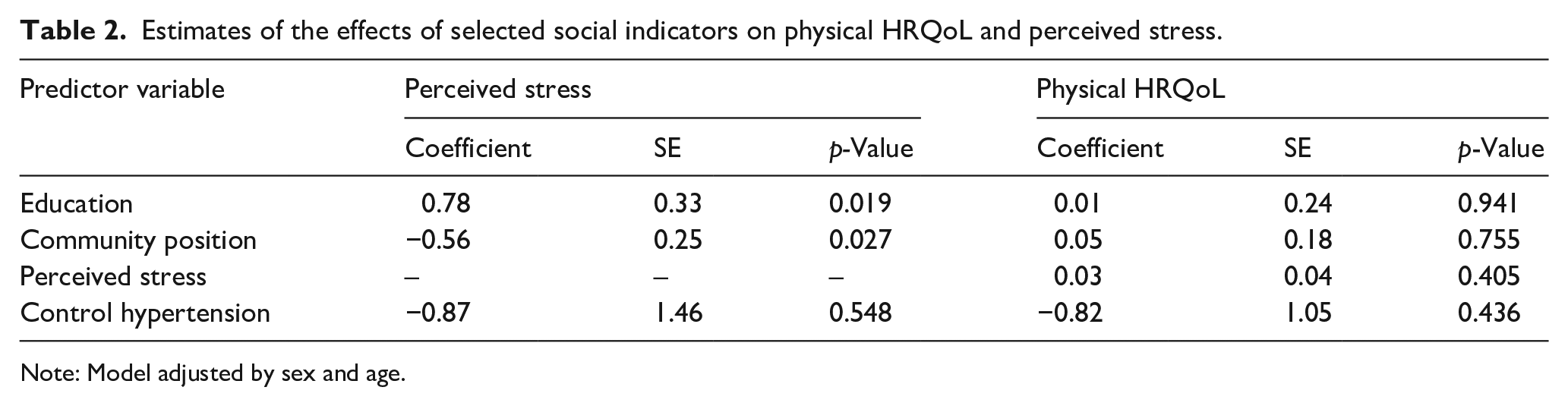
Note: Model adjusted by sex and age.
Estimates of the effects of selected social indicators on mental HRQoL and perceived stress.

Note: Model adjusted by sex and age.
A positive and significant association was found between education and perceived stress: the higher the educational level, the higher the perceived stress reported (Coeff = 0.78, p = 0.019). A person’s position in the community was negatively associated with stress: the greater the perceived position, the lower the perceived stress reported (Coeff = −0.56, p = 0.027). No statistically significant associations were found between predictors and physical HRQoL. On the same way, perceived stress showed no association with physical HRQoL.
In relation to the covariables, the model tested showed no association between sex or age and perceived stress. Also, no association was found between sex or age and physical HRQoL (results not shown).
Table 3 shows the relationships between predictor variables, perceived stress and mental HRQoL. In this model, a positive and significant association was found between education and perceived stress (Coeff = 0.78, p = 0.019). Regarding position in the community, this variable was negatively associated with stress (Coeff = −0.56, p = 0.027).
No statistically significant associations were found between predictors and mental HRQoL. However, differently from the previous model, perceived stress showed a positive association with mental HRQoL (Coeff = 0.64, p = 0.000).
In relation to the covariables, the model tested showed no association between sex or age and perceived stress. Also, no association was found between sex or age and physical HRQoL (results not shown).
Discussion
The aim of this study was to better understand the relationships between the socioeconomic position, perceived stress, and HRQoL of patients with hypertension in the context of a mediation model.
Descriptive results showed average scores for perceived stress just below the median score. Medellín showed the lower levels of perceived stress among the three cities. In relation with the subjective socioeconomic position, results showed that the average was very close to the median score which reflects perceived socioeconomic positions that are neither too high nor too low when participants compare to the other members of the community. Bogotá showed higher levels of perceived socioeconomic position, when compared with Medellín and Quibdó. This result could be explained by the fact that Bogotá, for being the capital, is the region in Colombia were economic, social and cultural capital is higher. Also, when we look to socioeconomic strata, our sample is composed with more high strata participants and at the same time fewer low strata participants in Bogotá, in relation with the two other cities.
The participants reported low scores for both physical and mental global health in comparison with normative values for the general population in Colombia, which has been estimated at around 80 on a scale of 0 to 100 using different measurements (Finck et al., 2012; Rojas-Reyes et al., 2017). Bogotá showed better mental HRQoL, in comparison with Medellín, which can be related with a lower intensity in armed conflict in the capital. A study in Colombia showed that in areas were the conflict was higher and permanent, there were more presence of disorders related with anxiety and depression, and higher levels of suicide (Gómez-Restrepo et al., 2016). Also, regarding low mental HRQoL scores, similar results have also been found in other studies. A study that assessed hypertensive patients found that they experienced moderate to extremely severe symptoms of anxiety, stress, and depression (Kretchy et al., 2014). Another study comparing HRQoL in hypertensive and non-hypertensive participants (Xu et al., 2016) found that people with hypertension had a lower score in every domain of HRQoL measured with SF-36 Health Survey, specifically in the mental health domain (Ware and Kosinski, 2005). However, the results in our sample were much lower than those in the cited study, for both physical and mental global scores. Similar results were found in other studies for hypertensive patients in relation to physical HRQoL, with low perceived physical HRQoL as our results also suggest (Trevisol et al., 2011). Emotional role and social functioning were the domains with the lowest average scores, but all scores were, in general, low on the scale. These results are similar to what other authors have previously described regarding the relationship of hypertension diagnosis and low scores in the eight health domains, using SF-36 health scale (Bardage and Isacson, 2001; Trevisol et al., 2011; Xu et al., 2016).
To understand the relationships between variables of interest in this study, we carried out a mediation analysis. In the mediation model that used physical HRQoL global score as an outcome, a higher education level explained higher levels of stress. These results go in a different direction of other results reported in the literature, which found that people with higher educational levels were less affected by stressors, in part, because of its relationship with higher economic or social resources that reduce stress and enable improved coping with disease (e.g. Fărcaú and Năstasă, 2014; Zimmerman and Woolf, 2014). Our results might be related to the fact that higher education levels could be associated with a high-level job demands, which in turn can affect distress, as some studies suggest (e.g. Akbari et al., 2017). Our results also showed that the lower the position in the community, the higher the perceived stress. Similar results were found in other studies, in which a lower subjective social status was associated with higher distress (Sakurai et al., 2010) and higher cortisol levels (Ursache et al., 2015).
In the second tested mental health model, we found a positive relationship between the perceived stress and mental HRQoL. This is an unexpected result of our study, in the sense that it suggests that the higher the perceived stress by the individual, the higher his perception of mental HRQoL. These results go in a different direction of what has been reported in the literature regarding stress and HRQoL (Ames, 2001; Baune and Aljeesh, 2006; Santos et al., 2013). Specifically, studies reported in the literature found a negative relationship between perceived stress and mental health in hypertension patients (e.g. Kretchy et al., 2014). One possible explanation to our results might be that individuals’ expectations play a role in how they interpret and react to adversity (World Health Organization, 2009), which could help buffering the effects of stress. Another study reported in the literature found that people confronted with stressful events or conditions in their lives, might engage in unhealthy behaviors, which in turn seemed to have protector effects on mental health, in the sense that could help to alleviate stress symptoms (Jackson et al., 2010). In our study, we didn’t assess unhealthy behavior in the participants, but this might be an explanation for the results found.
In this study, the mediation models proposed could not be confirmed, for any of the models tested.
Limitations identified in the study were the use of cross-sectional data, sample size, and little variability of the sample. Future studies should include a longitudinal perspective in the analysis so as to expand interpretations of causality.
Conclusions
In our study, the HRQoL of the sample is suboptimal, as all domain scores and physical and mental global scores are low. Perceived stress was not a mediator in this study but rather an independent predictor of mental HRQoL. Socioeconomic position and education predicted perceived stress but did not explain neither differences in physical nor mental HRQoL. A first implication of this study is that it addresses a topic with a lack of research in Colombia since there is not much information regarding the psychosocial and medical variables studied. Also, it provides empirical data to better understand the relationship between social context and individual’s quality of life. This information is important, especially in country with vulnerable economic and social circumstances.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Office of the Vice President for Research of Universidad de los Andes (grant number: P15.853122.009/01).
Ethical statement
This study was approved by the Universidad de los Andes Ethics Committee (Act number 531 of 2015).