
Abstract
This study aimed to identify the variables (i.e., internalizing, and externalizing problems, self-control, emotion dysregulation, and alexithymia) relevant for Smartphone Addiction and non-suicidal self-injury (NSSI), conceptualized as emotion-regulation strategies, also assessing age and gender differences. Based on power analysis, N = 78 Italian adolescents (11–19 years; Mage = 14.24; SD = 1.56; 73.1% females) were considered. Step-wise multivariate linear regressions evidence a mutual association between NSSI and Smartphone Addiction, particularly relevant in pre-adolescence. Low self-control is significantly associated with the Smartphone Addiction, while emotion dysregulation and alexithymia with NSSI. This study supports NSSI and Smartphone Addiction conceptualization as emotion-regulation strategies and the importance of prevention interventions.
Keywords
Adolescence is a critical period characterized by changes in different areas of development related to physiological and psychosocial functioning (WHO, 2019). This developmental period is characterized by several vulnerabilities (Cicchetti and Rogosch, 2002) particularly associated with the still-developing neural structures. The period of adolescents’ neuro-development is considered a vulnerability toward the put in action of risk-taking behaviors (Ahmed et al., 2015) which might lay the bases for the development of mental health problems (Cicchetti and Rogosch, 2002). Indeed, half of lifetime mental health concerns occur by the age of 14 (Kessler et al., 2005) further accounting for a great prevalence of adult psychopathology, as often left untreated or unrecognized in adolescence (Cicchetti and Rogosch, 2002; Kessler et al., 2005).
Emotional development is one of the goals of this transition period together with identity formation (Kim et al., 2012), yet it is also characterized by low self-control and a strong desire for novelty-seeking (Herpertz-Dahlmann et al., 2013). Self-control can be defined as the capacity to control one’s impulses in favor of one’s priorities and greater goals (Milyavskaya and Inzlicht, 2017). As such, high self-control can be considered as protective (Kim et al., 2018) as it is associated with a greater capacity for both emotional and behavioral self-regulation (De Ridder et al., 2012), while low self-control is associated with risk-taking and addictive behaviors as well as with the development of emotional problems (Oliva et al., 2019).
In this regard, the importance of self-control is recognized referring to two spreading phenomena among adolescents, namely, Smartphone Addiction (Kim et al., 2018; Billieux et al., 2007; Cho et al., 2017; Jeong et al., 2019; Zhang et al., 2019; Pavia et al., 2016; Olson et al., 2020) and Non-Suicidal Self-Injury (NSSI) (Abi-Jaoude et al., 2020; Castaldo et al., 2020; Lockwood et al., 2016; Yusainy and Lawrence, 2014).
Smartphone Addiction
Recent prevalence studies show that, in Italy, between 85.5% (ISTAT, 2019) and 87% (Ipsos, 2017) of adolescents aged between 11 and 17 years have regular access to a smartphone, with over 72% of them accessing the internet through their smartphone. Accordingly, a 2015 study reports greater problematic smartphone use between the age of 15 and 16 years. Moreover, women (85.7%) present a greater use of the device compared to men (ISTAT, 2019) with female adolescents showing a greater risk of developing addictive tendencies toward the smartphone (Fischer-Grote et al., 2019; van Deursen et al., 2015). Smartphone Addiction refers to the potentially negative consequences associated with the excessive and maladaptive use of the smartphone, sharing aspects relevant for behavioral and substance addictions (Panova and Xavier, 2018), thereby considered by some as an impulse-control disorder (Pavia et al., 2016; Yau et al., 2012). It associates with a compulsive desire for smartphone use, craving, interpersonal problems, and an incapacity to recognize the behavior as problematic (Cha and Seo, 2018; Mahapatra, 2019; Panova and Xavier, 2018). Still, Smartphone Addiction has not been recognized as a diagnostic label since the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013) only recognizes Internet Addiction (IA) as a disorder. As regards gender difference, it is shown that women spend a greater amount of time using the smartphone compared to men (Roberts et al., 2014), which is relevant considering that the duration of smartphone use is reported by the literature as a factor predicting Smartphone Addiction.
Smartphone Addiction might be considered as an emotion-regulation strategy for mood enhancement requiring little cognitive effort (Mahapatra, 2019) and for which low self-control capacities play a relevant role (Jeong et al., 2019; Zhang et al., 2019; Kim et al., 2018; Cho et al., 2017; Billieux et al., 2007). Beyond the predictive role of low self-control (Kim et al., 2018), other relevant risk-factors are the increased use of Social Networks Sites (SNSs; Wu et al., 2013), internet use, female gender, and anxiety (Choi et al., 2015) with the latter also recognized as a consequence of Smartphone Addiction (Hussain et al., 2017; Jeong et al., 2019). Moreover, anxiety, together with depression and stress, associates with different levels of Smartphone Addiction severity (Elhaia et al., 2019), while anger particularly distinguishes those showing a more pervasive addiction (Elhaia et al., 2019). Another relevant variable shown to be predictive of Smartphone Addiction is alexithymia (Gao et al., 2018), a personality trait referred to as a difficulty in recognizing, comprehending, as well as verbalizing feelings and emotions (Sifneos, 1973; Taylor and Bagby, 2012). Alexithymia shows a direct as well as indirect association with Smartphone Addiction (Gao et al., 2018) accounting for the association between Smartphone Addiction and mental health (Mei et al., 2018), and depression, anxiety, and stress more specifically (Gao et al., 2018). Alexithymia can also be considered as an inflexible emotion-regulation strategy, thus referring to a maladaptive emotional-processing and leading to an inadequate reactivity to situations as well as more frequent stress (Taylor and Bagby, 2012; Panayiotou et al., 2019). Coherently, emotion regulation (ER; Gratz and Roemer, 2004) is defined as a multidimensional construct involving four aspects: the awareness, understanding, and acceptance of emotional experience; the ability to engage in goal-directed behaviors and to inhibit impulsive behaviors when experiencing negative emotions; the flexible use of situationally appropriate strategies to modulate the intensity and/or duration of emotional responses; and the willingness to experience negative emotions as part of pursuing meaningful activities in life. In this regard, emotion dysregulation refers to a deficit in any of these ER components (Gratz and Roemer, 2004). Conceptualizing Smartphone Addiction as an emotion-regulation strategy (Kardefelt-Winther, 2017; Mahapatra, 2019), studies show that difficulties in ER are positively associated with problematic smartphone use in adolescents, further underlying the mediating role of depression (Fu et al., 2019), with emotion dysregulation mediating the relation between psychological distress and Smartphone Addiction (Squires, Hollett, Hesson, and Harris, 2020).
Non-suicidal self-injury
NSSI has been included in Section III of the DSM-V among the disorders in need of future research (APA, 2013). Criteria A describes it as “intentional self-inflicted damage to the surface of his or her body of a sort likely to induce bleeding, bruising, or pain (e.g., cutting, burning, stabbing, hitting, excessive rubbing), with the expectation that the injury will lead to only minor or moderate physical harm (i.e., there is no suicidal intent)” (APA, 2013: 803). A 2017 systematic review of studies published between 1998 and 2016 (Cipriano et al., 2017) reports prevalence rates ranging between 7.5% and 46.5% in adolescence. Onset usually occurs during early adolescence, between 12 and 14 years old (Beckman et al., 2018; Cerrutti et al., 2011), albeit observed also in children under the age of 12 (Barrocas et al., 2012). Moreover, a 2015 systematic review focusing on longitudinal studies investigating the NSSI phenomenon (Plener et al., 2015) showed a peak in prevalence rates during mid-adolescence, around 15 or 16 years of age, and declining during late adolescence. Studies also report an association between NSSI and the female gender (Bresin and Schoenleber, 2015; Burton, 2014; Castaldo et al., 2020; Spears et al., 2014; Morey et al., 2017; Schwartz-Mette and Lawrence, 2019) particularly relevant in women showing an internalized symptomatology (Castaldo et al., 2020; Skegg et al., 2004). NSSI is indeed particularly associated with depression (Lee, 2016; Singhal et al., 2014; Latina and Statting, 2018) and anxiety (Moran et al., 2012; Armey et al., 2011; Nock, 2009; Moller et al., 2013; Hughes et al., 2019; Singhal et al., 2014). Moreover, a longitudinal study (McLaughlin et al., 2011) showed that internalizing symptoms significantly mediate the association between emotion dysregulation and NSSI (Kranzler et al., 2016). Relying on the above-mentioned conceptualization of ER (Gratz and Roemer, 2004), NSSI can thus be considered as an emotion-regulation strategy (Bentley et al., 2014; Muehlenkamp et al., 2009; Nock 2009; Chapman et al., 2006). A further association emerges between NSSI and alexithymia (Gatta et al., 2016; Garisch and Wilson, 2015). Alexithymia is associated with deficits related to a cognitive-experiential comprehension of emotions and an incapacity for proper interpersonal-regulation (Taylor and Bagby, 2012). As such, it could be hypothesized that those presenting NSSI behavior externally express their suffering as an attempt at containing their psychological sufferance.
The current study
In today’s time, a strong increase worldwide in smartphone use has occurred (Olson et al., 2020) and in Italy the forecasted smartphone users are expected to double by 2025 compared to 2017 (Statista, 2020). Concurrently, a significant increase in NSSI has also occurred favored by the greater reliance on the Internet, SNSs, and the smartphone (Abi-Jaoude et al., 2020; Arendt et al., 2019; Castaldo et al., 2020; Dyson et al., 2016; Lewis et al., 2014; Memon et al., 2018; Purington & Whitlock, 2010). As previously reported, the smartphone entails great possibility of use allowing to access multiple platforms and means of communication taking advantage of the continuous possibility to access the internet wherever and whenever. It was shown that around 42 million NSSI-related searches are made on Google per year (Lewis et al., 2014) while in a “Yahoo! Answers” database analysis, 33.6% of the questions regarding NSSI were asked to receive some form of validation for the behavior, which accounted for the reasons underlining the posting of NSSI-related contents (Lewis et al., 2012). Recent systematic reviews, which had focused on the role of social media in the context of NSSI (Dyson et al., 2016; Memon et al., 2018), support the notion for which NSSI adolescents actively share and search for such content as perceiving some form of social support and comradeship that foster a sense of belonging (Dyson et al., 2016) and that can lead to an increased frequency of NSSI behavior (Memon et al., 2018) to the point of antagonizing its interruption while favoring relapse (Dyson et al., 2016). Moreover, NSSI has also been considered in association with SNSs (Abi-Jaoude et al., 2020; Arendt et al., 2019; Memon et al., 2018) as the spreading of the NSSI phenomenon has been observed to associate with greater SNSs use (Memon et al., 2018; Whitlock et al., 2006, 2009) as well as with Internet Addiction (Abi-Jaoude et al., 2020). Moreover, NSSI was shown to associate with nocturnal smartphone use (Oshima et al., 2012) which in turn associated with both sleep problems and depressive symptoms (Dewi et al., 2018), the latter being strongly associated with NSSI behavior (Castaldo et al., 2020; Lee, 2016; Singhal et al., 2014; Latina and Statting, 2018). Yet to present knowledge, no study has considered NSSI in association with Smartphone Addiction specifically, instead potentially relevant among adolescents performing NSSI (Abi-Jaoude et al., 2020). As previously mentioned, because of their bio-psychosocial immaturity, adolescents already present difficulties in emotion regulation and then further compromised when faced with psychological disturbances (Ahmed et al., 2015). The joint investigation of NSSI and Smartphone Addiction within an already vulnerable sample of adolescents is thus expected to provide insights relevant to the domain of emotional regulation since the psychological consequences that might result from the presence of both NSSI and Smartphone Addiction might add up and further limit adolescents’ capacities to acquire more adaptive emotion-regulation capacities and strategies, instead important to improve and support mental health in adulthood (Ahmed et al., 2015).
Thereby, the purpose of the present study is to identify the variables that better account for NSSI behavior and Smartphone Addiction, both considered as ER strategies (Bentley et al., 2014; Chapman et al., 2006; Kardefelt-Winther, 2017; Mahapatra, 2019; Muehlenkamp et al., 2009; Nock, 2009), in a sample of adolescents showing NSSI behavior. Age and gender differences will be also assessed. Based on the reviewed literature, it is expected that (i) self-control will significantly associate with both NSSI and Smartphone Addiction and that (ii) internalizing symptoms versus externalizing symptoms will show a different relevance toward NSSI and Smartphone Addiction. Moreover, it is expected that (iii) being female will significantly associate with both NSSI and Smartphone Addiction as both behaviors are widely reported to be more prevalent in women (Abi-Jaoude et al., 2020; Bresin and Schoenleber, 2015; Burton, 2014; Spears et al., 2014; Morey et al., 2017; Schwartz-Mette and Lawrence, 2019; Skegg et al., 2004; Fischr-Grote et al., 2019; van Deursen et al., 2015; Roberts et al., 2014; Choi et al., 2015).
Method
Participants and procedure
The present Italian community sample is composed of N = 78 adolescents not yet subject to clinical attention and performing NSSI behavior. Mean age is 14.24 (SD = 1.56); 73.1% are women. Moreover, N = 27 (11–13 years; 34.6%) attend middle school and N = 51 (14–19 years; 65.4%) high school.
Participants’ data belong to multiple pre-test phases of the broader LOOK@ME research-intervention project (The Net-ONLUS, 2017). This project has started in 2017 and more than 1000 adolescents have taken part in it since then. It is aimed at supporting community samples of adolescents and to develop ad hoc interventions and focus groups to improve their self-control, emotion-regulation capacities, and well-being. The data considered in the present study were collected between 2019 and 2020 via an online battery of questionnaires administered through the schools’ computers during school hours by psychologists and trained psychology students. Parents of minors or adolescents over the age of 18 years signed informed consent that were collected before questionnaires administration. Subjects further provided oral consent before participation and were informed that they could retrieve from the study at any moment without any repercussion. Participants considered in the present study satisfied the following inclusion criteria: (1) being aged between 11 and 19 years and (2) having fully completed the self-report measures and both modules of the self-injurious self-report measure in particular. Data were collected in compliance with the Declaration of Helsinki (Italian law 196/2003) and protected under the UE GDPR 679/2016 law for the protection of personal data. This study was approved by the Ethical Committee of Psychology of the University of Padova (number 2322, June 6th, 2017).
Measurement tools
Brief Self-Control Questionnaire
The Brief Self-Control Questionnaire (BSCS) is a self-report measure developed by Tangney and colleagues (Tangney et al., 2004) and validated in Italy by Chiesi and colleagues (2020). It is composed of 13 items measured on a 5-point Likert scale (from 1 = “not at all like me” to 5 = “very much like me”) and is aimed at assessing the level of self-control capacities referred to the domains of achievement and task performance, impulse control, adjustment, interpersonal relationships, and moral emotions. BSCS provides a total final score with lower scores indexing lower self-control capacities. The internal consistency for the present study is α= .68.
Strength and Difficulties Questionnaire
The Strength and Difficulties Questionnaire (SDQ; Goodman et al., 2010) is a self-report questionnaire composed of 25 items measured on a 3-point Likert scale (1=“Not True”; 2= “Somewhat true”; 3= “Certainly true”) and aimed at identifying people at risk for psychological problems by collecting information related to their emotional, interpersonal, and behavioral profile with higher scores indexing the presence of more negative attributes, while lower scores greater positive attributes. The European validation (Marzocchi et al., 2004) was performed on a sample of healthy and low-risk adolescents age ranging between 11 and 17 years. The instrument provides a Total difficulty score composed of the sub-scales Internalizing problems and Externalizing problems, which will be considered separately in the present study. The SDQ further provided a Prosocial behavior score. In the current study, internal consistency is α = .68 for the Internalizing problems scale and α = .75 for the Externalizing problems one.
Smartphone Addiction inventory—Italian version
The Italian version of the Smartphone Addiction Inventory (SPAI; Pavia et al., 2016) comprises 24 items measured on a 4-point Likert scale (1 = “Strongly disagree”; 4 = “Strongly agree”) and is aimed at measuring smartphone addiction. Higher scores index greater smartphone addiction, while lower scores index poorer or absent addictive tendencies. The SPAI provides a total final score referred to the level of difficulty in stopping smartphone use as well as the amount of time and resources devoted to its use, the distress experienced when deprived of its use, and the associated feelings of anxiety, irritation, and tension. It further considers how pervasive is the need for smartphone use during daily life activities while also measuring the presence and level of interpersonal problems it may cause. Additional domains refer to the compulsivity and persistence associated with the use of smartphones comprising items investigating withdrawal and avoidance related behaviors, the level of sleep disturbance, and the relation between smartphone use and reduced sleeping time. In the present study, internal consistency is highly satisfactory (α= .91).
Self-Injurious Thought and Behavior Questionnaire-Non Suicidal
The Self-Injurious Thought and Behavior Questionnaire-Non Suicidal (SITBQ-NS), derived from the original interview version (Nock et al., 2007), is a self-report measure validated in Italy by D'Agostino and colleagues (2018) on a sample of self-harming adolescents. It comprises 28 items measured on a 5-point Likert scale, half referring to self-injurious thoughts and the other half investigating self-injurious behavior. For those answering to this second set of items, beyond self-harming thoughts and behavior, the questionnaire further investigates if the person has received medical treatments. The tool specifically aims to measure self-injurious thoughts and behaviors related to self-harming acts without suicidal intent. It provides three final scores referring to “Self-Injurious Thoughts,” “Self-Injurious behavior,” and the “Self-Injurious Spectrum”; the present study will solely consider the latter. Lower scores index less frequent and pervasive self-harming thoughts and behavior, while higher scores refer to a more critical and pervasive situation. Internal consistency is α= .91.
Toronto Alexithymia Scale
The Toronto Alexithymia Scale (TAS; Bagby et al., 1994a, 1994b) validated in Italy by Bressi and colleagues (Bressi et al., 1996) is a self-report measure composed by 20 items rated on a 5-point Likert scale (1 = “strongly disagree”; 5= “strongly agree”). Higher scores index greater alexithymia traits. It is aimed at assessing alexithymia in a continuum going from the absence of alexithymia-related aspects to being alexithymic. The TAS provides a final total score, which will be considered in the present study, comprising three sub-scales, namely, Difficulty Identifying Feelings, Difficulties Describing Feelings, and Externally Oriented Thinking. Internal consistency is α= .80.
Difficulties in Emotion Regulation Scale
The Difficulties in Emotion Regulation Scale (DERS; Gratz and Roemer, 2004) is a self-report measure aimed at measuring difficulties in the capacity for emotion regulation. It comprises 36 items rated on a 5-point Likert scale (1= “almost never”; 5 = “almost always”), with higher scores indexing greater difficulties in emotion regulation. The Italian validation (Sighinolfi et al., 2010) shows a highly significant internal consistency α = .90. The instrument provides a final total score comprising six sub-scales germane to impulse control difficulties, lack of emotional awareness, limited access to emotion-regulation strategies, lack of emotional clarity, and difficulties engaging in goal-directed behaviors. In the present study, internal consistency is α= .91.
Data analysis
Descriptive statics and pair-wise Pearson r’s correlations (p-value > .05) were assessed through SPSS v20.0 (IBM Corp., 2011). Correlations and the graphical representation of paired-variables association were performed to assess multicollinearity among variables. Multiple regression power calculations and regression analysis were performed through R (R Core Team, 2019).
Multiple regression power calculation was performed using R package pwr to define the minimum sample size necessary to maintain a power of at least .80 for hypotheses testing. Results yield that the multivariate regression models should have a sample size of at least 67 participants. The hypothesized proportion of variance explained by the regression models was set at 30%, for a number of predictors ranging from 8 to a maximum of 20. The significance level was set at .05.
Simple linear regressions were initially performed to assess the association between each independent variable (i.e., Age; BSCS; SDQ-int; SDQ-ext; TAS; DERS) with either SITBQ-NS or SPAI and to assess if SITBQ-NS and SPAI are associated. Multivariate linear regressions were then performed. Two models were assessed through backward and forward step-wise selection. In the first model (M1), the dependent variable was SITBQ-NS total score while all the above-mentioned variables, as well as SPAI, were included in the model as predictors. The second model (M2) considers SPAI as a dependent variable and includes the same predictors used in M1 as well as SITBQ-NS total score. In both models, age and gender differences were assessed by including Age (11–13 years = 0; 14–19 years = 1) and Gender (Male = 0; Female = 1) as dummy variables and also assessing the presence of interactions between either one of the dummies and each independent variable. Age was not included as a continuous variable since through simple linear regression Age does not show an association with SITBQ-NS and, although showing a significant association with SPAI, the sample age is asymmetrically distributed on the left; therefore, Age as a dichotomous variable allows a greater balance among age-groups, untimely better accounting for age differences. Slope analysis was then performed to further investigate the significant interaction effects. Durbin–Watson (Durbin and Watson, 1950, 1951, 1971) and Shapiro–Wilk (Shapiro and Wilk, 1965) tests were also performed to assess the independence and distribution normality of the models’ residuals. Predictors were considered significant at p-value < .05.
Results
Descriptive information.

Note: BSCS = self-control; SPAI = Smartphone Addiction; SDQ_int = internalizing problems; SDQ_ext = externalizing problems; SITBQ-NS = NSSI; TAS = alexithymia; DERS = emotion dysregulation.
Correlations
Pair-wise Pearson correlation.

Note: *p-value< .05; **p-value< .01. BSCS = self-control; SPAI = Smartphone Addiction; SDQ_int = internalizing problems; SDQ_ext = externalizing problems; SITBQ-NS = NSSI; TAS = alexithymia; DERS = emotion dysregulation.
Regression models
Simple linear regressions were initially performed with either SITBQ-NS or SPAI as dependent variable and the following variables as independent variables: Age, BSCS, SDQ_int, SDQ_ext, TAS, and DERS. Simple regressions performed with SITBQ-NS as dependent variable show a significant positive association with SDQ_int (β = 2.46; p = .006; R2 =9.72%), SDQ_ext (β = 2.88; p < .001; R2 = 13.42%), TAS (β = .89; p = .003; R2 = 11.06%), DERS (β = 22.82; p < .001; R2 = 24.95%), and SPAI (β = 11.57; p = .05; R2 = 4.96%). BSCS showed no significant association with SITBQ-NS. Simple regressions performed with SPAI as dependent variable show comparable positive associations (SDQ_ext, β = 0.05; p < .001; R2 = 9.48%; TAS, β = 0.018; p < .001; R2 = 11.87%; DERS, β = 0.28; p < .001; R2 = 10.18%; SITBQ-NS, β = .004; p = .05; R2 = 4.96%) although also showing a negative and significant association with BSCS (β = −0.35; p < .001; R2 = 10.75%). On the other hand, SDQ_int showed no significant association with SPAI. Age as continuous variable does not significantly associate with either SPAI or SITBQ-NS.
Step-wise multivariate linear regression model (M1).
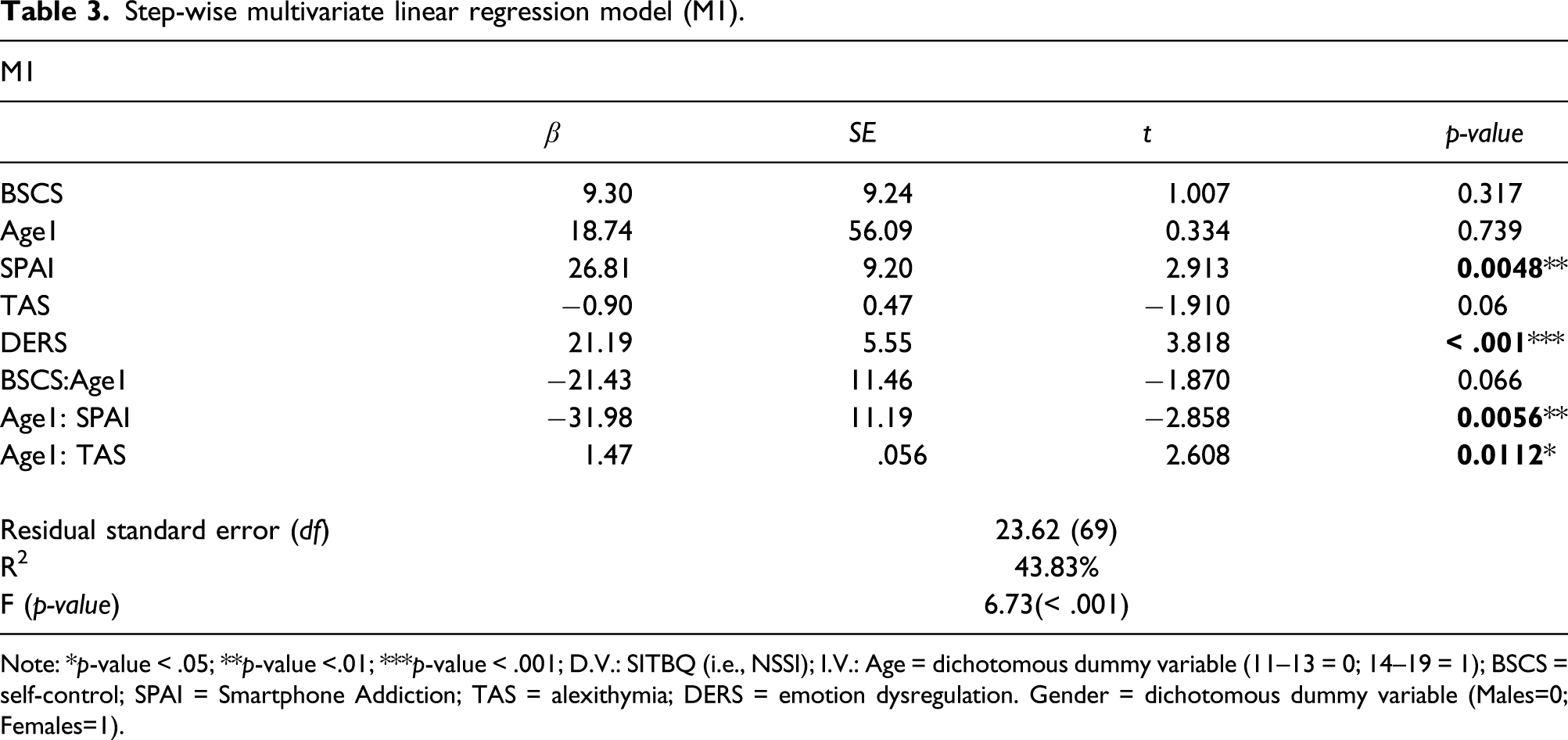
Note: *p-value < .05; **p-value <.01; ***p-value < .001; D.V.: SITBQ (i.e., NSSI); I.V.: Age = dichotomous dummy variable (11–13 = 0; 14–19 = 1); BSCS = self-control; SPAI = Smartphone Addiction; TAS = alexithymia; DERS = emotion dysregulation. Gender = dichotomous dummy variable (Males=0; Females=1).
Step-wise multivariate linear regression model (M2).

Note: *p-value < .05; **p-value <.01; ***p-value < .001; D.V.: SPAI = Smartphone Addiction; I.V.: Age = dichotomic dummy variable (11–13 = 0; 14–19 = 1); SITBQ = NSSI; BSCS = self-control; SDQ_int = internalizing problems; TAS = alexithymia; DERS = emotion dysregulation. Gender = dichotomic dummy variable (Males=0; Females=1).
Interaction effect plots are shown in Figure 1, referring to the interaction effects emerged in both M1 and M2. Slope analysis results showed that, in M1, SPAI positively and significantly associated with SITBQ-NS only among pre-adolescents aged 11–13 years (a; β = 26.81; p <.001), while the effect was not significant among older adolescents aged 14–19 years. From the interaction plot showing the interaction effect between Age and TAS (b), it can instead be observed a trend whereby among older adolescents aged 14–19 years, TAS and SITBQ-NS show a positive associative trend, while pre-adolescents significantly differed in that TAS, and SITBQ-NS instead showed a negative associative trend. Moreover, referring to M2, and coherent with M1 results, the interaction effect between Age and SITBQ-NS showed that SITBQ-NS only significantly, and positively, associated with SPAI among pre-adolescents aged 11–13 years (c; β = 0.01; p =.02), while the effect was not significant among older adolescents. Interaction effect plots. Note: Age: 0 = 11–13 years, 1 = 14–19 years.
Discussion
The purpose of the present study is to exploratorily identify the variables accounting for NSSI and Smartphone Addiction in a sample of adolescents performing NSSI. This study is part of the broader LOOK@ME research-intervention project (The Net-ONLUS, 2017), which goal is to develop ad hoc interventions and focus groups to improve self-control, emotion-regulation capacities, and well-being in adolescents showing NSSI idealization and behavior and Smartphone Addiction and addiction tendencies. Both NSSI and Smartphone Addiction are maladaptive behaviors that can be conceptualized as emotion-regulation strategies (Mikolajczak et al., 2009; Chester et al., 2014;Billiewux et al., 2007; Cho et al., 2017; Jeong et al., 2019; Kim et al., 2018; Zhang et al., 2019). By identifying the variables that account for the two behaviors, it might be possible to set some initial bases on the aspects that could lead to greater Smartphone Addiction in adolescents performing NSSI, thus hypothetically dealing with their sufferance through multiple and easy to access maladaptive strategies. Their joint investigation is thus relevant to the study of emotion regulation since “compromised abilities in emotional regulation may confer a further overall risk for all kinds of psychopathology, independently from its clinical appearance” (De Berardis et al., 2020: 2; Young et al., 2019). The increased spreading of the NSSI behavior is largely favored by the use of the Internet and SNSs (Arendt et al., 2019; Dyson et al., 2016; Memon et al., 2018; Purington and Whitlock, 2010), both readily accessible through the smartphone. The current article supports knowledge regarding aspects relevant to both NSSI and Smartphone Addiction in a community sample of adolescents showing relevant clinical symptoms, yet not under clinical attention, and the first which attempts to report a direct association between the investigated behaviors.
In the present study, findings show that Smartphone Addiction and NSSI significantly and positively predict each other, which seems particularly true for pre-adolescents as compared to adolescents, although Smartphone Addiction tendencies seem to increase as age increases. This is a relevant finding as it could signify that the specific neuro-developmental immaturity of pre-adolescents and associated poor ER capacities (Ahmed et al., 2015) might account for the significant association between NSSI and Smartphone Addiction reported in both regression models. Interestingly, findings also show that low self-control is a significant variable only in the Smartphone Addiction model. The non-significance of self-control for NSSI could be imputed to the assessment tool itself (i.e., BSCS) as it provides a unidimensional view of self-control (Tangney et al., 2004). Others have instead proposed a two-dimensional specification of the tool as it better differentiates between inhibitory (i.e., the capacity to refrain from impulse-driven behaviors) and initiatory (i.e., referred to the initiation of goal-directed behaviors) self-control (De Ridder et al., 2011) as NSSI is better explained by low inhibitory self-control (Allen and Hooley 2015). In this regard, initiatory self-control better predicts desirable behavior, while inhibitory self-control undesirable behavior (De Ridder et al., 2011) with the two being interrelated yet different constructs (De Ridder et al., 2011; Lindner et al., 2015). By comparing the two factorial structures (i.e., unidimensional vs two-dimensional), it was observed for De Ridder and colleagues’ (2001) perspective to better predict outcome variables (De Ridder et al., 2011; Lindner et al., 2015) ultimately concluding for BSCS as not satisfactorily accounting for the two distinct self-control facets (Lindner et al., 2015). As such, the non-significance of self-control concerning NSSI might be explained by a lack of proper differentiation between the two self-control facets for which the investigation of NSSI self-control related variables necessitates a more punctual consideration, as supported by the association between NSSI and inhibitory self-control (Allen and Hooley, 2015) or impulse-control difficulties (i.e., impulsivity; Hamza et al., 2015) as well as emotion dysregulation (Emery et al., 2016; Gratz et al., 2017). Coherently, in the present sample, greater emotion dysregulation associated with NSSI increased pervasiveness and severity (Emery et al., 2016; Gratz et al., 2017). Following the line of the above-reasoning, this finding might be explained by the emotional reactivity to negative emotions and physiological arousal typical of pre-adolescents and adolescents (Ahmed et al., 2015; Lucarelli, 2010), which supports the conceptualization of NSSI as an attempt at emotion regulation (Mikolajczak et al., 2009; Chester et al., 2014). The negative affectivity associated with different levels of physiological arousal influences how youth interprets it (Bradley, 2003). Physiological arousal implies an activation of the body that goes beyond the one normally experienced; its association with an unpleasant state is particularly relevant during the developmental period, especially as regards the subjective distress pre-adolescents and adolescents might experience (Bradley, 2003). As such, maladaptive behaviors and regulation strategies such as NSSI and Smartphone Addiction might develop as a consequence of a difficulty in regulating both negative feelings and arousal (Ahmed et al., 2015; Lucarelli, 2010) potentially leading to their mutual reinforcement. The risks arising from this mutual reinforcement, strengthened by some of the smartphone’s usage possibilities (e.g., to access SNSs and Google searches), could lead to a normalization (Arendt et al., 2019; Dyson et al., 2016; Kirsch, 2012) and thus reinforcement of NSSI behavior by sharing NSSI-related content (Arendt et al., 2019; Dyson et al., 2016; Memon et al., 2018) by utilizing the multiple platforms available on smartphones (e.g., SNSs, WhatsApp, Telegram, and SMS). On the other hand, this could, in turn, lead to greater Smartphone Addiction and addiction tendencies, since the smartphone would allow for the satisfaction of social needs (Mohd Suki, 2013) by speculatively gaining emotional and instrumental support, as indeed observed specifically referring to the association between NSSI and SNSs (Memon et al., 2018). Furthermore, it could also be speculated that adolescents rely on the smartphone also as a means for attentional-deployment, which also requires little cognitive effort (Mahapatra, 2019), also favoring the suppression of the unpleasant and overwhelming affectivity associated to NSSI when the behavior cannot be performed, thereby acquiring a regulatory function toward the negative and dysregulated emotionality associated with NSSI. Such mechanism might as well account for the mutual reinforcement among the two behaviors, coherent with a recent study (Rozgonjik and Elhai, 2019) showing that the “process use” of the smartphone (i.e., a non-social use of the tool, thereby referred to media consumption such as watching videos, playing games, browsing online, etc.) totally mediated the association between emotional suppression and Smartphone Addiction severity.
Referring to Gratz and colleagues’ (Gratz and Roemer, 2004) conceptualization of ER as a multidimensional construct, for which alexithymia could be considered as one of its facets (Stasiewicz et al., 2012), results showed also that, although alexithymia per-se was not significantly associated with NSSI when controlling for the effect of all other variables, adolescents and pre-adolescents significantly differed in the direction of effect acquired by alexithymia, thus showing a positive associative trend among adolescents performing NSSI, and a negative one among pre-adolescents. Differently, the more complex emotion dysregulation resulted relevant, and significantly associated with NSSI, regardless of age. These differences in effect significance and age associated influence of alexithymia versus emotion dysregulation might be explained by the specific aspects that are accounted for by the two constructs. Alexithymia is defined as a difficulty in recognizing, comprehending, as well as verbalizing feelings and emotions (Sifneos, 1973; Taylor and Bagby, 2012); yet, the more complex emotion dysregulation refers to dysfunctions in either the understanding and acceptance of emotional experiences, the ability to engage in goal-directed behaviors while inhibiting the impulse-driven ones when experiencing negative emotions, the capacity to flexibly use adaptive regulatory strategies, or the willingness to experience negative emotions as part of pursuing meaningful activities in life (Gratz and Roemer, 2004). By referring to the construct’s conceptualization, it can be speculated for NSSI to be more generally due to a difficulty in properly and more broadly modulating, more than merely recognizing, emotions and feelings and related strategies. By contrast, the influence of alexithymia might acquire a greater influence on NSSI behavior during late adolescence as resulting from a deficit in developing a proper emotional maturity and awareness, thus pointing to the importance of psycho-educational interventions.
These findings illustrate the complexity of the association between Smartphone Addiction and NSSI, which particularly refers to the reported age differences, with implications for treatment and prevention practices. Differently, and contrary to expectations, no gender differences have emerged and gender, in general, did not result as a significant variable in either model. The reported age differences suggest distinct clinical pictures for adolescents and pre-adolescents and specifically referring to the role of emotion-regulation capacities as regards the adoption of maladaptive regulatory strategies and the attempt to compensate for their sufferance by using multiple dysfunctional strategies. As such, the results referring to the association between NSSI and Smartphone Addiction in pre-adolescence seem of particular relevance, since if during the whole adolescence period connectivity among structures does not balance itself out (as happens in clinical populations) (Ahmed et al., 2015) higher-order cerebral areas, although mature, might still not be able to properly modulate physiological arousal nor to properly mentalize it, thus not allowing proper emotion regulation (Ahmed et al., 2015). This might then result in the permanence and/or worsening of emotion dysregulation, and related aspects, as age increases. Results from a recent meta-analysis (Kraiss et al., 2020) indeed highlighted the importance of supporting proper emotion regulation in the context of mental health issues. This would favor greater well-being, which is important to support symptoms remission and overall recovery (De Vos et al., 2017; Mead and Copeland, 2000; Pitt et al., 2007), while also reducing the risk for later psychopathology (De Berardis et al., 2020; Young et al., 2019).
Still, the current findings necessitate replication and the associated speculations deeper investigation.
Limitations and future research
Findings should be considered in light of some limitations as well as potentialities for future research. The present study relies on self-report measures for which bias could occur. The study followed a cross-sectional design; ethnicity and socioeconomic status were not considered, which could limit the generalizability of findings. Moreover, the present study considers a quite small sample, yet the power analysis performed supports the reliance of findings. A further limitation is the unbalanced distribution of gender in favor of females, although it supports past findings reporting a greater prevalence of NSSI among females (Bresin and Schoenleber, 2015; Burton, 2014; Spears et al., 2014; Morey et al., 2017; Schwartz-Mette and Lawrence, 2019; Skegg et al., 2004).
The present study also provides useful suggestions for future investigations. More specifically, as regards self-control, it could be interesting to further investigate how different self-control facets associate with the two behaviors, for instance, by adopting the Adolescent Self Consciousness questionnaire (Li et al., 2015). Moreover, referring to the association between NSSI and Smartphone Addiction, the present findings highlight the relevance of age differences which necessitate deeper consideration and investigation, particularly as regards the hypothetical different role of alexithymia and emotion dysregulation, since it might have significant clinical implication.
Conclusions
To present knowledge, no prior study has ever considered both NSSI and Smartphone Addiction, nor their direct association. Albeit its limitations, the present study provides some initial bases regarding the joint consideration of the two behaviors, in line with past evidence highlighting the association between NSSI and maladaptive use of the smartphone like nocturnal smartphone use (Oshima et al., 2012). Moreover, the joint investigation of NSSI and Smartphone Addiction further highlighted the relevance of age differences for the two behaviors with implications for clinical practice. As such, projects like the LOOK@ME research-intervention project (The Net-ONLUS, 2017) are of paramount importance to limit and counteract the development or worsening of psychological sign and symptoms relevant to both NSSI and Smartphone Addiction, particularly since onset is usually in adolescence (Beckman et al., 2018; Cerutti et al., 2011). Moreover, in light of the increasing reliance smartphones are acquiring in pre-adolescents and adolescents’ lives as well as the increasing possibilities for their use (Abi-Jaude et al., 2020), together with its noxious aspects also its positive ones could be investigated. This could provide new means for psychological support while sensitizing toward the risks resulting from its misuse, particularly among those pre-adolescents that report clinical symptoms in a non-strictly clinical population. Indeed, it is important to make the most of pre-adolescents’ neuronal plasticity (Ahmed et al., 2015) and thus fostering interventions favoring better emotion regulation and the use of more adaptive and flexible regulatory strategies, thereby supporting their mental health in adulthood (Ahmed et al., 2015; De Berardis et al., 2020).
Footnotes
Acknowledgments
Authors are thankful to the “the Net-ONLUS” and the Department of Developmental Psychology and Socialization of the Univeristy of Padova for supporting this research. The “the Net-ONLUS” LOOK@ME research-intervention project won the OPV prize 2017 for innovation in assessment and clinical research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.