
Abstract
This study (N = 780) examines the indirect effects of hardiness—health locus of control (HLOC), health competence (HC), health value (HV)—on past-year healthcare provider visit via attitudes toward seeking and receiving professional healthcare services (ATSRPHS). Across four health domains (dental, general health, mental, vision), ATSRPHS mediated the indirect effect of (1) HV and (2) internal HLoC on past-year healthcare provider visit. ATSRPHS also mediated the indirect effect of external HLoC on past-year visit to healthcare provider visit for general medical, mental, and vision health. ATSRPHS did not mediate any indirect effect of HC on past-year healthcare provider visit. This research contributes to understanding determinants of healthcare service utilization among Black American adults.
Keywords
Non-Hispanic Black Americans utilize healthcare services, including visiting their healthcare providers, less often than non-Hispanic Whites (National Center for Health Statistics [NCHS], 2016, 2018). This underutilization of services—resulting from the lack of health insurance and access to healthcare services (Williams et al., 2019)—is oftentimes cited as a critical determinant of poor dental (e.g. large number of cavities; Feinberg, 2015; Han, 2019), vision (e.g. high rates of glaucoma; Zhang et al., 2012), physical (e.g. high rates of diabetes; NCHS, 2016), and mental (e.g. severe and persistent depression; American Psychiatric Association, 2017) health among Black Americans. These multi-level, multi-factor, determinants of healthcare service utilization, along with their independent and interactive effects are captured conceptually with the Behavioral Model of Health Services Use (Andersen, 1995).
Briefly, the Behavioral Model of Health Services Use incorporates individual and contextual factor to explain healthcare services utilization. The Behavioral Model of Health Services Use is divided into three components that act independently and interactively to influence one’s utilization of healthcare services: (1) predisposing factors, including individual factors such as demographics, psychological factors, and psycho-social factors (e.g. age, health values); (2) enabling factors that influences one’s ability to receive healthcare (e.g. price of healthcare services); and (3) need factors that influences an individual’s perceived need to utilize health services (e.g. current health status; for review see Babitsch et al., 2012). Hardiness, the focus of this paper, constitutes one such predisposing psychological factor.
Hardiness and healthcare services utilization
Hardiness is conceptualized as a personality characteristic that represents “a general quality of an individual to regard stressful life events as amenable, and to consider changes as a normal and interesting part of life” (Gebhardt et al., 2001: 579), comprises three dimensions (Funk, 1992; Kobasa, 1979). The first dimension, commitment, captures one’s perception of stressful situations as meaningful, valuable, and interesting. The second and third dimensions, control and challenge, capture perceptions of stressors as changeable and the tendency to view stressful events as an opportunity for growth, respectively (Funk, 1992; Kobasa, 1979). Hardiness is often implicated in health (i.e. health hardiness) given that it influences behavioral responses to stressful stimuli (Funk, 1992; Gebhardt et al., 2001; Kobasa et al., 1982). Particularly, hardiness is thought to lead to better health outcomes by engendering feelings that one possesses the skills, knowledge, and abilities to overcome the stress of maintaining good health (i.e. perceived health competence; Gebhardt et al., 2001; see Health Belief Model; Janz and Becker, 1984).
Those with a more positive health hardiness orientation—that is, being committed to improving one’s health, believing that one is in control of their health outcomes, and viewing the stresses of maintaining good health as beneficial—are more likely to engage in health-promoting behaviors, including the utilization of healthcare services (Funk, 1992; Kobasa, 1979). For example, the belief that one’s health outcomes result from one’s own actions and will power (i.e. internal health locus of control) is associated with a greater likelihood of visiting a doctor compared to the belief that one’s health outcomes result the actions of others or fate (i.e. external health locus of control; De Jesus and Xiao, 2014; c.f. Kesavayuth et al., 2020; Mautner et al., 2017). In addition, Tromp et al. (2005) found that patients who did not delay seeking medical care reported greater perceived health competence than those who delayed seeking treatment. However, Tromp et al. (2005) also found no difference between the two groups in the extent to which they reported valuing of being healthy (i.e. health value).
Although limited, the aforementioned research is consistent with other work showing that hardiness predicts increased likelihood of engaging in health-promoting behaviors. For example, health value and perceived health competence are associated with greater likelihood of exercising and dieting, and lower odds of smoking and drinking (Bachmann et al., 2016, 2018; Gebhardt et al., 2001; Jackson et al., 2007). Increasing perceived health competence is also associated with greater health information-seeking behaviors (Marks and Lutgendorf, 1999). Other work shows that an internal [health] locus of control orientation is associated with greater reported flossing, exercising, and reported willingness to visit the dentist (Conell-Price and Jamison, 2015). Thus, it is conceivable that just as hardiness predicts health-promoting behaviors broadly, it also predicts the utilization of healthcare services specifically.
Hardiness and attitudes toward healthcare services
Attitudes toward seeking and receiving professional healthcare services (ATSRPHS) encompasses one’s feelings toward, beliefs about, and willingness to seek and receive healthcare services from healthcare professionals (Neighbors, 1985). More positive ATSRPHS is associated with greater willingness and increased likelihood to use professional mental (e.g. visiting a psychologist; Mojtabai et al., 2016), dental (e.g. visiting a dentist; Kwan and Holmes, 1999), vision (e.g. visiting an optometrist; Owsley et al., 2006), and general medical (e.g. visiting a general practitioner; DiLorenzo et al., 2015) healthcare services. ATSRPHS is especially critical for investigation given racial/ethnic differences in these attitudes (Dornelas et al., 2014; Hines-Martin et al., 2004). Still, research examining the relationship between ATSRPHS and healthcare service utilization is disproportionately qualitative, especially among those examining this relationship outside the mental health domain. Notwithstanding, extensive and well-documented research shows that positive health-related attitudes correlate positively with health-promoting behaviors (for review see; Conner and Sparks, 2005). As such, it is likely that more positive ATSRPHS will predict greater healthcare service utilization across the dental, general heath, mental, and vision health domains.
In addition to factors such as gender (Hines-Martin et al., 2014), age (Dornelas et al., 2014), and stigma (e.g. Schnyder et al., 2017), personality characteristics, which includes hardiness, affects health attitudes broadly, and ATSRPHS specifically (Lemos-Giráldez and Fidalgo-Aliste, 1997). Although limited, one study demonstrates such a relationship. Specifically, Oluyinka (2011) found that more internal (less external) health locus of control beliefs were associated with more positive attitudes toward seeking and receiving professional mental healthcare services. No other studies—to the author’s knowledge—have investigated the relationship between the other dimensions of hardiness and ATSRPHS quantitatively. Notwithstanding, it is conceivable that a positive hardiness orientation predicts more positive ATSRPHS given that hardiness influences attitudes about health-promoting behaviors (Kobasa, 1979) by “motivat[ing] people to react to stresses with effective coping, social support interactions, and lifestyle patterns” (Maddi, 2002: 177). Consequently, it is likely that a positive hardiness orientation increases healthcare service utilization by facilitating more positive ATSRPHS.
Current study
This research examines hardiness and ATSRPHS as determinants of healthcare service utilization among Black American adults. In particular, this research investigates the direct effect of hardiness—locus of control beliefs, perceived health competence, and health value—on past-year healthcare provider visit across four health domains: dental, general, mental, and vision health. In addition, this research examines the indirect effect of hardiness on past-year healthcare provider visit via ATSRPHS. It is hypothesized that a positive hardiness orientation—increasing internal locus of control beliefs (and decreasing external locus of control beliefs), increasing health value, and increasing perceived health competence—will predict greater odds of past-year healthcare provider visit. It is also expected that this direct effect will be mediated by ATSRPHS, such a more positive hardiness orientation will predict more positive ATSRPHS, which will then predict greater odds of past-year visit to healthcare provider. These relationships are expected across all health domains.
Method
Participants
780 Black American adults participated in this web-based survey study (Age: M = 37.68, SD = 14.66, Range: 18–87; % Female = 57.60; % Heterosexual = 78.30). Most participants were not college educated (% Some college = 23.70%; % high school or less = 36.80%). A majority of the participants were employed (60.00%) and made less than $39,000 a year (54.90%).
Data were collected in January 2020. All participants provided informed consent. The author’s Institutional Review Board (IRB) approved this study. Qualtrics panel aggregator was used to recruit participants (internal health locus of control.Qualtrics.com). Participants were targeted to participate if they self-identified as Black American and were 18 years of age or older. Once targeted, participants were sent an anonymous online survey link. All participants provided informed consent. After completing the study, participants were compensated based on agreement with their panel service provider, which included money, credit card points, air travel miles, as examples. Digital fingerprinting technology and IP address checks are also used to ensure that participants’ data were valid and reliable.
Measures
Health hardiness
Health hardiness was measured using the 24-item Revised Hardiness Health Inventory (RHHI; Gebhardt et al., 2001). The RHHI comprises four subscales, each with six items completed on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree): (1) The
ATSRPHS
Dental
Participants completed seven items that capture their attitudes toward seeking and receiving professional dental healthcare services on a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree). The items were developed using data from the New Hampshire Senior Center Dental Survey (Horsch, 2010). Sample items include, “I would never go for more than a year without seeing my dentist, at least for a check-up” and “Dental visits are only important if you have a dental emergency.” The appropriate items were reverse coded and then averaged. Higher values reflect more positive attitudes toward seeking and receiving professional dental healthcare services (ATSRPHS-D; α = 0.56).
General medical
Participants completed the 12-item action/intention sub-scale of the Attitudes Towards Seeking Medical Care Scale (DiLorenzo et al., 2015; Fischer et al., 2013) on a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree). The appropriate items were reverse coded and then averaged. Higher values reflect more positive attitudes towards seeking and receiving professional general medical healthcare services (ATSRPHS-G; α = 0.83).
Mental healthcare services
Participants completed the 10-item Attitudes Toward Seeking Professional Psychological Help Scale-Short Form (Elhai et al., 2008) on a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree). The appropriate items were reverse coded and then averaged. Higher values reflect more positive attitudes toward seeking and receiving professional mental healthcare services (ATSRPHS-M; α = 0.56).
Vision healthcare services
Participants completed seven items that capture their attitudes toward seeking and receiving professional vision healthcare services on a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree). The items were developed using data from qualitative work examining factors associated with the willingness to receive and seek professional eyecare and eyecare services (Alexander et al., 2008). Sample items include, “Regular eye checkups will help prevent problems” and “There is no need to go to the eye doctor if you’re not having a problem with your eyes.” The appropriate items were reverse coded and then averaged. Higher values reflect more positive attitudes toward seeking and receiving professional vision healthcare services (ATSRPHS-V; α = 0.80).
Past-year healthcare service utilization
Participants answered yes (1) or no (0) to the following four questions: (1)
Covariates
Participants completed the following socio-demographics: age, sex/gender, education, sexual orientation, relationship status, employment status, and income. In addition, participants reported their overall mental, physical health, dental health, and vision health, each on a 5-point Likert scale (1 = poor to 5 = excellent). Last, participants reported whether (yes [1], no [0]) they currently had health, dental, and/or vision health insurance. Participants were coded as having insurance if they selected one of the following options: (1) government funded insurance (Medicaid, Medicare, ADAP, VA, Ryan White), (2) Employer-based insurance (theirs of their spouse’s), (3) Private [health, dental, vision] insurance, or (4) “I have [health, dental, vision] insurance, but I do not know the type.”
Data analytic strategy
To test the direct and indirect effects of hardiness on past-year visit to healthcare provider via ATSRPHS, four path analyses—one for each health domain—were conducted using Mplus Version 8. All path analyses were fitted using the robust maximum likelihood estimator (MLR) with 500 Montecarlo integrations in order to obtain the odds ratio for the dichotomous outcome variable and robust beta estimates for indirect effects (Muthén and Muthén, 2017). All path analyses included socio-demographic variables as covariates. Health insurance and overall health were also added as covariates, however specific to the health domain (e.g. dental insurance and overall dental health were added as covariates for the dental health path model). In addition, a series of exploratory paired samples t-tests were conducted to examine differences in participants’ ATSRPHS across the four health domains.
Results
Table 1 shows the means, standard deviations, and proportions of descriptive characteristics for the total sample. Table 2 shows the means, standard deviations, and correlations of main study variables. Table 3 presents all indirect effect coefficients. In the past year, 52.8% (n = 412) of participants visited their dental healthcare provider, 52.8% (n = 412) of participants visited their vision healthcare provider, 69.1% (n = 539) visited their primary healthcare provider, and 39.1% (n = 305) visited their mental healthcare provider.
Means, standard deviations, and proportions of descriptive characteristics for sample.

Means, standard deviations, and correlations of main study variables.

ATSRP: attitude toward seeking and receiving professional.
p < 0.05. **p < 0.01. ***p < 0.001.
Indirect effect odds ratios (OR) of path models.
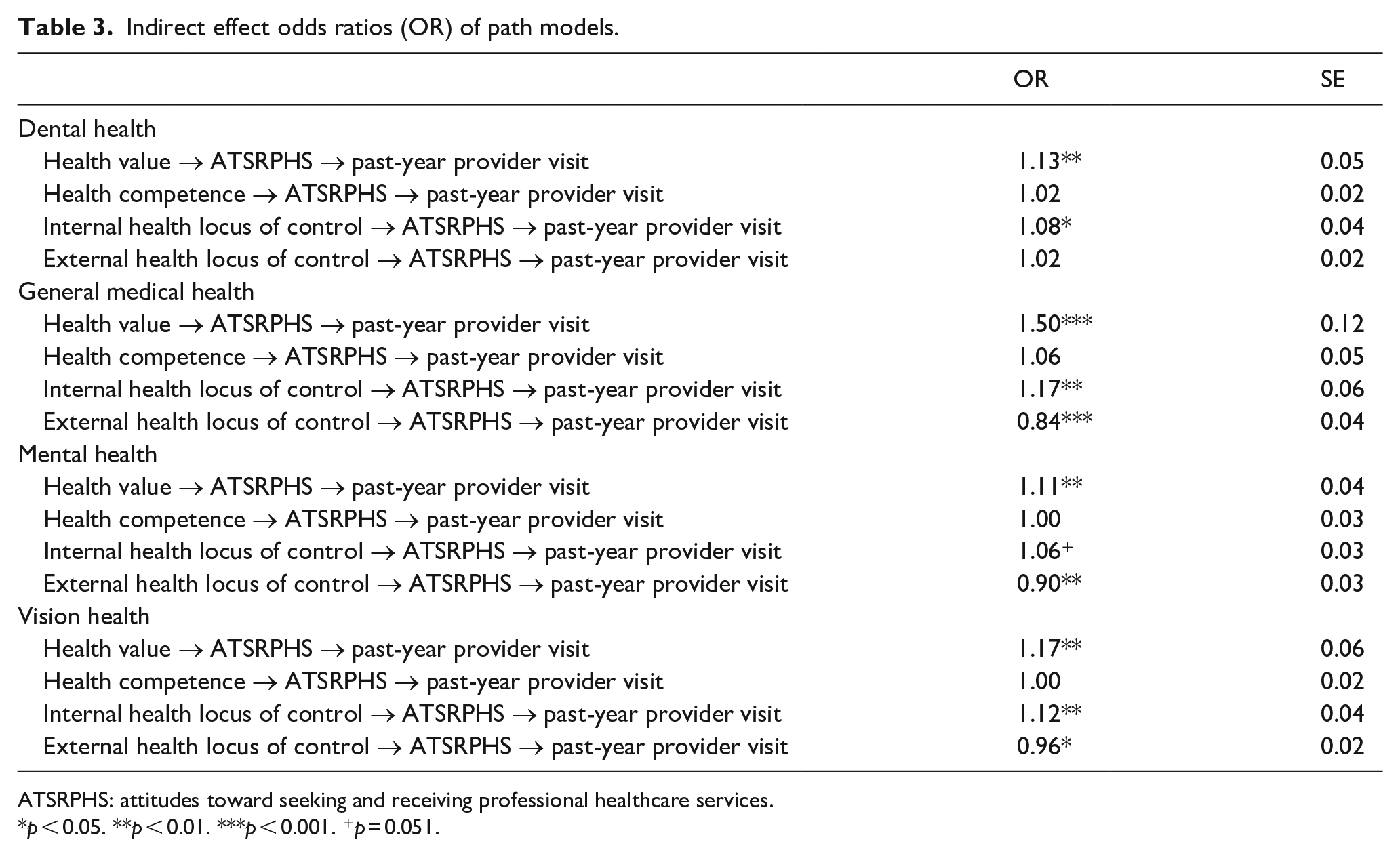
ATSRPHS: attitudes toward seeking and receiving professional healthcare services.
p < 0.05. **p < 0.01. ***p < 0.001. +p = 0.051.
Dental
Partially supporting hypotheses: (1) increasing internal health locus of control and health value, but not external health locus of control and perceived health competence, were associated with more ATSRPHS-Dental; and (2) ATSRPHS-Dental, but not internal health locus of control, health value, external health locus of control or perceived health competence, predicted greater odds of past-year dentist visit (See Figure 1 for standardized coefficients and odds ratios). In addition, supporting hypotheses, ATSRPHS-Dental mediated the relationship between (1) internal health locus of control and past-year dentist visit and (2) health value and past-year dentist visit, such that increases in either internal health locus of control or health value were associated with more positive ATSRPHS-Dental, which then predicted greater odds of past-year dentist visit. Against hypotheses, ATSRPHS-Dental did not mediate the indirect effect of either external health locus of control or perceived health competence on past-year dentist visit.

Path model presenting the direct and indirect effects of health hardiness on past-year visit to dental healthcare provider via attitudes toward seeking and receiving professional dental healthcare services (ATSRPHS-D). β: standardized regression (path) coefficients; OR: odds ratios. Only significant covariates are included. *p < 0.05. **p < 0.01. ***p < 0.001.
General medical
Supporting hypotheses: (1) increasing internal health locus of control and health value were associated with more positive ATSRPHS-General Medical; and (2) increasing external health locus of control was associated with more negative ATSRPHS-General Medical. However, against hypothesis, perceived health competence was not associated with ATSRPHS-General Medical. In addition, supporting hypotheses: (1) increasing internal health locus of control was associated lower odds of past-year primary healthcare provider visit and (2) increasing ATSRPHS-General Medical was associated with greater odds of past-year primary healthcare provider visit. However, against hypothesis, external health locus of control, health value, and perceived health competence did not predict past-year primary healthcare provider visit (See Figure 2 for standardized coefficients and odds ratios).

Path model presenting the direct and indirect effects of health hardiness on past-year visit to mental healthcare provider via attitudes toward seeking and receiving professional general healthcare services (ATSRPHS-M). β: standardized regression (path) coefficients; OR: odds ratios. Only significant covariates are included. *p < 0.05. **p < 0.01. ***p < 0.001.
Also supporting hypotheses, ATSRPHS-General Medical mediated the relationship between (1) internal health locus of control and past-year primary healthcare provider visit and (2) health value and past-year primary healthcare provider visit. Specifically, increases in either internal health locus of control or health value was associated with more positive ATSRPHS-General Medical, which then predicted greater odds of past-year primary healthcare provider visit. Also supporting hypotheses, ATSRPHS-General Medical mediated the relationship between external health locus of control and past-year primary healthcare provider visit, such that increases in external health locus of control was associated with more negative ATSRPHS-General Medical, which predicted lower odds past-year primary healthcare provider visit. Last, against hypotheses, ATSRPHS-General Medical did not mediate the indirect effect of perceived health competence on past-year primary healthcare provider visit.
Mental
Supporting hypotheses: (1) increasing internal health locus of control and health value were associated with more positive ATSRPHS-Mental; and (2) increasing external health locus of control was associated with more negative ATSRPHS-Mental. However, against hypothesis, perceived health competence was not associated with ATSRPHS-Mental. In addition, supporting hypotheses increasing external health locus of control and ATSRPHS-Mental were associated with greater odds of past-year mental healthcare provider visit. However, against hypothesis, internal health locus of control, health value, and perceived health competence did not predict past-year mental healthcare provider visit (See Figure 3 for standardized coefficients and odds ratios).

Path model presenting the direct and indirect effects of health hardiness on past-year visit to general healthcare provider via attitudes toward seeking and receiving professional general healthcare services (ATSRPHS-G). β: standardized regression (path) coefficients; OR: odds ratios. Only significant covariates are included. *p < 0.05. **p < 0.01. ***p < 0.001.
Also supporting hypotheses, ATSRPHS-Mental mediated the relationship between (1) internal health locus of control and past-year mental healthcare provider visit and (2) health value and past-year mental healthcare provider visit. Specifically, increases in either internal health locus of control or health value was associated with more positive ATSRPHS-Mental, which then predicted greater odds of past-year mental healthcare provider visit. Also supporting hypotheses, ATSRPHS-Mental mediated the relationship between external health locus of control and past-year visit to the mental healthcare provider, such that increases in external health locus of control was associated with more negative ATSRPHS-Mental, which predicted lower odds of past-year mental healthcare provider visit. Last, against hypotheses, ATSRPHS-Mental did not mediate the indirect effect of perceived health competence on past-year mental healthcare provider visit.
Vision
Supporting hypotheses: (1) increasing internal health locus of control and health value were associated with more positive ATSRPHS-Vision; and (2) increasing external health locus of control was associated with more negative ATSRPHS-Vision. However, against hypothesis, perceived health competence was not associated ATSRPHS-Vision. In addition, supporting hypotheses increasing health value and ATSRPHS-Vision were associated with greater odds and internal health locus of control was associated with lower odds of past-year vision healthcare provider visit. However, against hypothesis, external health locus of control and perceived health competence did not predict past-year vision healthcare provider visit (See Figure 4 for standardized coefficients and odds ratios).
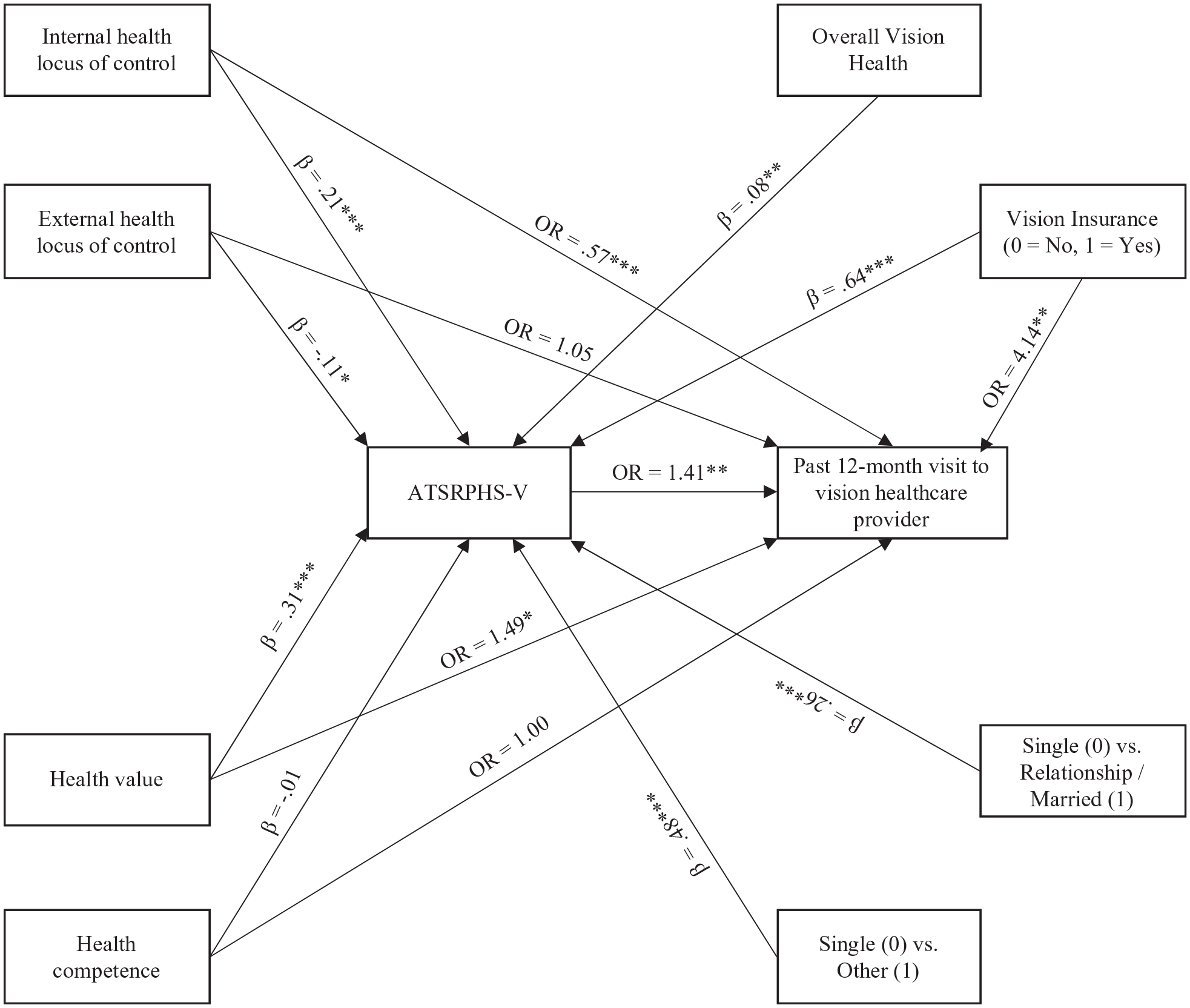
Path model presenting the direct and indirect effects of health hardiness on past-year visit to vision healthcare provider via attitudes toward seeking and receiving professional vision healthcare services (ATSRPHS-V). β: standardized regression (path) coefficients; OR: odds ratios. Only significant covariates are included. *p < 0.05. **p < 0.01. ***p < 0.001.
Also supporting hypotheses, ATSRPHS-Vision mediated the relationship between (1) internal health locus of control and past-year vision healthcare provider visit and (2) health value and past-year vision healthcare provider visit. Specifically, increases in either internal health locus of control or health value was associated with more positive ATSRPHS-Vision, which then predicted greater odds of past-year vision healthcare provider visit. Also supporting hypotheses, ATSRPHS-Vision mediated the relationship between external health locus of control and past-year vision healthcare provider visit, such that increases in external health locus of control was associated with more negative ATSRPHS-Vision, which predicted lower odds of past-year vision healthcare provider visit. Last, against hypotheses, ATSRPHS-Vision did not mediate the indirect effect of perceived health competence on past-year vision healthcare provider visit.
Exploratory analyses
Participants reported more positive ATSRPHS-General Medical, ATSRPHS-Dental, and ATSRPHS-Vision than ATSRPHS-Mental, t(778) = 10.92, p < 0.001, d = 0.36, t(778) = 6.99, p < 0.001, d = 0.24, and t(778) = 11.17, p < 0.001, d = 0.36, respectively. In addition, participants reported more positive ATSRPHS-Vision and ATSRPHS-General Medical than ATSRPHS-Dental, t(779) = 4.79, p < 0.001, d = 0.12 and t(779) = 4.32, p < 0.001, d = 0.12, respectively. Last, participants no difference in ATSRPHS-General Medical and ATSRPHS-Vision, t(779) = 0.09, p < 0.001, d = 0.00.
Discussion
This research examined the direct and indirect effects of hardiness on past-year dental, mental, general health, and vision healthcare provider visit via attitudes toward seeking and receiving professional healthcare services (ATSRPHS) among Black American adults.
ATSRPHS
Replicating and extending previous work (e.g. Oluyinka, 2011) increasing health value and internal health locus of control predicted more positive ATSRPHS across all health domains (i.e. dental, mental, general health, vision). Also supporting hypotheses, increasing external health locus of control was associated with more negative attitudes toward seeking and receiving professional mental, general health, and vision healthcare services. However, against hypotheses, external health locus of control did not predict attitudes towards seeking and receiving professional dental healthcare services. This suggests that Black Americans’ utilization of dental healthcare services is driven by beliefs in their own (relative to external factors) abilities to affect their dental health.
Last, against hypotheses perceived health competence did not predict ATSRPHS across any health domain, contrary to past research (e.g. Tromp et al., 2005). This suggests that the extent which Black Americans believe that they possess the skills and knowledge necessary to engage in health-promoting behaviors does not predict their attitudes toward seeking and receiving professional healthcare services. This finding, although against predictions, is consistent work showing that feeling of competence increasingly predict attitudes when the two variables are more (vs less) related to the same construct (Le Deist and Winterton, 2005; Satter, 2007). That is, perceived health competence, a global measure of health self-efficacy, is better able to predict general attitudes toward health and health behavior than more specific health attitudes such as seeking and receiving professional healthcare services (Bandura, 1982).
Healthcare service utilization
Supporting hypotheses, and replicating previous qualitative and quantitative findings (e.g. Mojtabai et al., 2016; Owsley et al., 2006), more positive ATSRPHS predicted greater odds of past-year visit to healthcare providers across all health domains. However, against hypotheses, internal health locus of control predicted lower odds of past-year vision and general healthcare provider visit, and external health locus of control predicted greater odds of past-year visit mental healthcare provider visit. These findings, while contrary to previous work (e.g. De Jesus and Xiao, 2014), are consistent with findings by Kesavayuth et al. (2020) who found that increasing internal health locus of control (decreasing external health locus of control) was associated with lower likelihood of utilizing outpatient and inpatient healthcare services (see also Mautner et al., 2017). On the one hand, it is likely that increasing internal health locus of control predicts lower odds of healthcare service utilization because those with higher internal health locus of control are more likely to report being healthy, which then decreases their perceived need to utilize of healthcare service (Kesavayuth et al., 2020; Mautner et al., 2017). It is also likely those who believe that external factors, and not themselves, dictate their health or health outcomes are more likely to seek out healthcare service providers (Ouellette and DiPlacido, 2001).
In addition, supporting hypotheses health value predicted greater odds of past-year vision healthcare provider visit. However, against predictions, health value did not predict past-year dental, general, or mental healthcare provider visit, replicating previous research (Tromp et al., 2005). In particular, Tromp et al. (2005) found no group differences in health value between individuals who delayed seeking medical care and those who did not delay seeking medical care. According to Tromp et al. (2005), health value does not predict specific health behaviors (i.e. healthcare service utilization) as it is a general measure of global health behaviors (e.g. leading a healthy lifestyle). Thus, in the case of vision health it is likely that visiting one’s vision healthcare service provider represents a global vision-promoting behavior (Owsley et al., 2006). Indeed, in this study those with (vs without) vision insurance were four times more likely to visit their vision healthcare provider in the past year.
Also, against hypotheses, perceived health competence did not predict past-year healthcare provider visit across all health domains. Here again, it is likely that one’s perceived health competence does not directly predict their likelihood of visiting their healthcare service provider, but might predict one’s beliefs in their ability to navigate the healthcare system and overcome health barriers (Lee et al., 2004). Thus, given that perceived health competence does not capture specific beliefs and attitudes toward behaviors related to healthcare service utilization, it did not predict past-year healthcare provider visit (Tromp et al., 2005).
Further supporting hypotheses, ATSRPHS mediated the indirect effect of (1) health value and (2) internal health locus of control on past-year healthcare provider visit across all health domains. Partially supporting hypotheses, ATSRPHS mediated the indirect effect of external health locus of control on past-year healthcare provider visit for general medical, mental, and vision healthcare service provider (because external health locus of control did not predict attitudes toward seeking and receiving professional dental healthcare services (see previous explanation)). Last, against hypotheses, perceived health competence did not mediate the indirect effect of ATSRPHS on past-year provider visit across all health domains (because perceived health competence did not predict attitudes toward seeking and receiving any professional healthcare service (see previous explanation)).
Altogether, except for perceived health competence, these results support hypotheses suggesting that a positive hardiness orientation predicts more positive attitudes toward health-promoting behaviors (Kobasa, 1979), which then “motivate[s] people to react to stresses with effective coping, social support interactions, and lifestyle patterns” (Maddi, 2002: 177). This increased motivation afforded by a positive attitude toward seeking and receiving healthcare services increases one’s engagement in health-promoting behaviors, in this case past-year healthcare service provider visit.
Importantly, these indirect of hardiness on past-year healthcare provider visit through ATSRPHS highlights ATSRPHS as an important determinant of healthcare service utilization among Black American adults. These results suggest a need to develop interventions that promote positive ATSRPHS (see Hawe, 2015). The different direct and indirect effects of hardiness on past-year provider visit across the four health domains suggests a greater demand for research that examines the determinants of healthcare service utilization broadly, and research that examines the health domain-specific determinants of healthcare service utilization (Andersen, 1995). Altogether, this research points to a continued focus on global and health domain-specific determinants of health (Williams et al., 2019).
Differing from previous studies, this research examined differences in ATSRPHS across four health domains quantitatively, although exploratory. For example, results show that participants reported the least positive attitudes toward seeking and receiving mental healthcare services and the most positive attitudes toward seeking and receiving vision healthcare services. Future research should examine factors that uniquely predict attitudes toward seeking and receiving professional domain-specific healthcare services. As examples, previous work shows that stigma and fear predict attitudes toward seeking and receiving professional mental and dental healthcare, respectively (Conner et al., 2010; Siegel et al., 2012). Future research should examine these unique determinants to design health domain-specific interventions that improve healthcare service utilization (Hawe, 2015).
Implications and limitations
Importantly, this research has implications for understanding the underutilization of healthcare services among Black American adults. Particularly, this research suggests that in addition to addressing structural determinants of healthcare service utilization (e.g. barriers to seeking and receiving professional health care such as location of healthcare services), future research can also focus on interventions that engender a positive hardiness orientation among Black Americans. Such interventions can include behavior change techniques that also focus on increasing one’s perceived health value, perceived health competence, and internal health locus of control beliefs (Glanz and Bishop, 2010).
In addition, this points to hardiness as a determinant of Black American’s health. It is conceivable that in addition to influencing attitudes toward seeking and receiving professional healthcare services, hardiness might also influence the extent to which Black Americans trust their healthcare service provider. For example, previous research shows that a high internal locus of control orientation is associated with greater trust in one’s physician (Gabay, 2015). If, and the extent to which, hardiness predicts healthcare provider trust is a critical relationship to investigate as relative to non-Hispanic Whites, Black American express more distrust toward healthcare providers—largely because of the discrimination they experience and a history of unethical medical practices that were carried out on Black American patients (Kennedy et al., 2007; Ross et al., 2012). Investigating these relationships would help build trust between Black Americans and healthcare service providers.
Relatedly, this research also informs our understanding of the John Henry hypothesis. The John Henry hypothesis argues that “prolonged high-effort coping with chronic psychosocial stressors may be associated with elevated risk for negative health outcomes among those without sufficient socio-economic resources” (Bennett et al., 2004: 369), particularly among Black Americans. Indeed, it is conceivable that overtime greater levels of psychological hardiness can lead to increased John Henryism among Black Americans. This increased John Henryism can then have negative health consequences. For example, Hudson et al. (2016) found that greater levels of John Henryism were associated with increased odds of depression in a representative sample of African American adults. Similar, Merrit and colleagues found that among Black men with low (but not high0 education, high vs low) John Henryism was associated with higher systolic blood pressure. These examples point to a need to examine psychological hardiness using longitudinal designs.
Although this study has many strengths, it has some limitations. First, this study’s cross-sectional design limits a claim of causality. In particular, the cross-sectional nature of this study’s design limits claims of the effects of hardiness or attitudes on healthcare utilization as healthcare utilization occurred in the past. However, longitudinal data suggests how those positive attitudes toward receiving professional (mental) health treatment predicts the utilization of (mental) health services over a 1-year period (Adler et al., 2015) and other work shows no variation in psychological hardiness over a 3-year period (Hystad et al., 2015). Still, although the specified model of this research is informed by previous longitudinal investigations, future research should examine the relationship among hardiness, ATSRPHS, and healthcare service utilization over time.
Second, this study used a non-random, non-representative online sample of Black Americans. As a result, results of this study cannot be generalized across Black Americans. Still, although responder and sampling biases exist in web-based studies (e.g. responder age, income; Mayr et al., 2012), internet findings generalize across presentation formats (Gosling et al., 2004). Notwithstanding, future research should replicate this study using a representative sample of Black Americans, including Black Caribbeans and Black Africans. Controlling for socio-demographic characteristics also increases confidence in this study’s results. In particular, the results suggest that the relationship among psychological hardiness, health attitudes, and past-year healthcare provider visit remain even when accounting for factors such as age, gender, income, and insurance status. Still, future research should examine socio-demographic moderators of these effects to understand within-group variations among African American adults.
Third, this study uses self-reported past-year healthcare service provider visits to capture healthcare service utilization. This is limiting as this measure does not capture healthcare services that do not require having health, dental, and/or vision insurance (e.g. free health clinics), neither does it capture the frequency of and reason for visiting healthcare service providers. In the same way, the measure of healthcare service provider visit does not fully capture the range of healthcare service utilization or engagement in other health-promoting behaviors. Future work should examine the relationship between psychological hardiness and other forms of healthcare service utilization (e.g. alternative medicine) among Black American adults. Even still, given the broad nature of the service provider visit questions (i.e. “. . .visited or talked to any. . .”), it is likely that participants included healthcare services such as health clinics in their response. In addition, controlling for health insurance status and overall health also addresses some of these concerns.
Last, the measures of attitudes toward seeking and receiving professional dental and vision healthcare services are not validated. However, although constructed for the purposes of this study, the two measures were informed by informed by previous research. In addition, providing evidence of convergent validity, both measures were positively correlated with the other measures of ATSRPHS. Notwithstanding, future research should replicate this study using validated and reliable measures of ATSRPHS.
Conclusion
This research examined the direct and indirect effects of hardiness on past-year dental, mental, general health, and vision healthcare provider visit via attitudes toward seeking and receiving professional healthcare services among Black American adults. Altogether, results show—with the exception of perceived health competence—that a positive hardiness orientation predicts more positive attitudes toward seeking and receiving professional healthcare services, which then predicts greater odds of past-year healthcare service provider visit. This research contributes to our understanding of determinants of healthcare service utilization among Black American adults and, as a result, has implications for reducing racial health disparities.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.