
Abstract
Emerging adulthood is a turning point in the life cycle with regard mental health. To assess psychological distress and attachment styles 688 university students of which 370 requested a counselling support responded to Symptom Checklist 90 Revised and Attachment Style Questionnaire. Counselling attending students (vs counselling non-attending students) have a higher psychological risk profile, with more psychological distress and insecure attachment. A marked percentage of students not attending counselling presents psychological distress. In both groups associations emerged between psychopathological problems and insecure attachment. The importance of communication strategies aimed to those students who, albeit non requesting psychological help, display psychological distress is discussed.
Keywords
Introduction
Over the last two decades interest in the mental health of young adults has grown (Grant and Potenza, 2010; Tanner, 2016). This is due to the focus on emerging adulthood proposed by Arnett (Arnett, 2004, 2016) and shared by many researchers (Gomes et al., 2019; Umemura et al., 2017). According to this author, emerging adulthood, the period between ages 18 and 29, is a distinct developmental stage halfway between late adolescence and young adulthood. In this period individuals are transitioning between developmental stages – living an ‘in-between’ condition, i.e. neither adolescent nor adult (Arnett, 2005), while their personality is becoming consolidated (Hopwood et al., 2011).
Mental health and emerging adulthood
Emerging adulthood is characterized by instability and exploration in terms of identity and relationships (Riva Crugnola, 2017) and is considered a turning point in the life cycle as regards psychological wellbeing and the emergence of psychopathological problems (Schulenberg et al., 2004). This developmental stage involves important changes in social roles and contexts, entailing a mix of positive and negative trends for what concerns mental health with two possible outcomes: mental disorders increase and become acute or mental health becomes consolidated (Burt and Paysnick, 2012). Longitudinal studies demonstrated that a relevant protective factor for mental health in this period consists in the fulfilment of the developmental tasks of the previous adolescent stage (Burt and Masten, 2010).
Research showed that during young adulthood the onset of mental health disorders intensifies with respect to infancy and adolescence, with a total of 75% of all life onset at the age of 24 (Kessler et al., 2005). Moreover, according to international studies, around 20% of young adults have at least one mental disorder (Gomes et al., 2019; Cadigan et al., 2019), with depression, anxiety, and substance and alcohol abuse prevailing (Grant and Potenza, 2010; Hunt and Eisenberg, 2010). Furthermore, low socio-economic level, little social support from adults, and a history of adverse experiences exacerbate these disorders (Burt and Paysnick, 2012; Schilling et al., 2007). Conversely, anger and antisocial behaviour tend to decrease during this stage (Galambos and Krahn, 2008; Galambos et al., 2006; Moffitt et al., 2002), while self-esteem tends to rise as compared to adolescence (Inguglia et al., 2015).
According to different authors, in the current socio-economic and cultural context of Western societies, emerging adults receive little social support from the adult community in coping with the developmental tasks of this period of life (Arnett, 2016; Grant and Potenza, 2010); this seems to be even more the case with students attending university. The university period can be considered particularly critical since it often means being away from the family, constructing new social relationships, and following new study objectives, all in the context of a relative absence of rules and less supervision from parents and teachers compared to adolescence (Grant and Potenza, 2010). In this period, anxiety, depression and substance abuse frequently emerge in students (Hunt and Eisenberg, 2010; Tanner, 2016), although the occurrence of mental disorders is comparable to that of their peers not attending university (Blanco et al., 2008).
The university period, therefore, offers a significant opportunity to tackle mental health issues, also from the perspective of prevention with respect to subsequent life periods (Adamo et al., 2010, 2012; Riva Crugnola, 2017; Riva Crugnola et al., 2020). Research shows that failure to address mental health issues in emerging adulthood leads to a greater risk of developing serious long-term mental disorders (Carver et al., 2015). However, it also shows that only a subgroup of university students with a mental health disorder are referred to adequate treatment, because many students tend to be self-reliant, unaware of their need for psychological support, and denying their emotional difficulties (Arnett, 2004; Cadigan et al., 2019). Furthermore, difficulties in accessing university psychological counselling services represent an issue (Hunt and Eisenberg, 2010).
A review of European studies (Holm-Hadulla and Koutsoukou-Argyraki, 2015) shows prevalence rates of mental disorders among students between 20% and 25%. Other studies have analysed psychopathological problems of students who have access counselling services, showing that the amount is greater (being 58%) (Kreß et al., 2015).
Few studies, however, have compared the level of psychopathological problems of university students in general with that of students who access counselling services. Of these studies, that of Kreß et al. (2015) showed that while 15% of German university students from the community report psychopathological problems, 58% of students accessing counselling services suffer from mental disorders, with depression and anxiety prevailing.
Therefore, given the few studies conducted in this regard, evaluating and comparing the psychopathological problems of students attending and not attending counselling services is of particular interest. Such evaluation may also be useful in identifying a possible percentage of undetected psychopathological problems in the student population.
Mental health and attachment
In the last few decades, the study of attachment has been increasingly associated with crucial aspects of mental functioning involved in individual mental health such as styles of emotion regulation and interpersonal relations (Cassidy, 1994; Mikulincer and Shaver, 2015). From this perspective attachment models are conceived as relational expectations connected to representation of oneself and of the other deriving from the internalization of experiences linked to the subject’s history of attachment in infancy. They tend to be stable throughout life (Sroufe, 2005), albeit changing in the face of stressful events or of new significant relationships and serve to guide interpersonal relations during the course of life (Main et al., 1985).
In this regard, various studies showed associations between quality of attachment and psychopathological problems in adulthood (Mikulincer and Shaver, 2015). One initial line of studies examined the link between attachment patterns evaluated in infancy and psychopathological disorders emerging in subsequent stages such as adolescence and adulthood (Dozier et al., 2008). These studies show that, above all, disorganized attachment is per se a predictor of psychopathological risk in adolescence and adulthood, in particular for dissociative disorders (Sroufe, 2005) and borderline personality disorder (Lyons-Ruth et al., 2013), while the insecure attachment patterns represent a general factor of vulnerability.
A second area of study concerns the association between attachment evaluated in adulthood and psychopathological disorders present at that age. In this regard, two lines of research emerged. On the one hand there are the developmental studies which, continuing those of Bowlby and Ainsworth on patterns of infant attachment, evaluate representations with regard to adult attachment from a categorical approach, differentiating them into secure, preoccupied, dismissing, and unresolved/disorganized attachment models, through use of the Adult Attachment Interview (Main et al., 1985; Steele and Steele, 2008). In this regard, the thorough meta-analysis of Bakermans-Kranenburg and van IJzendoorn (2009) showed that, in general, insecure and unresolved/disorganized attachment models are more prevalent than secure attachment models in samples with different clinical problems.
Starting from the theories of Hazan and Shaver (1994), in the area of social personality psychology (Fortuna and Roisman, 2008), researchers applied a dimensional approach to the study of adult attachment, hypothesizing two independent dimensions of attachment styles, anxiety and avoidance (Mikulincer and Shaver, 2012). According to this perspective, the anxiety dimension involves a negative self-perception and an expectation of attachment figures as not being available in the case of need. The consequent response is an attachment hyperactivation strategy that, through the exaggerated expression of emotion, aims at establishing contact and intimacy with significant others. The avoidant dimension of attachment, on the other hand, consists in the devaluation of significant relationships and on self-reliance, with the aim of maintaining independence through a strategy of deactivation of attachment by distancing oneself from intimate relationships. In order to dimensionally assess attachment styles various self-report questionnaires have been developed (Shaver and Mikulincer, 2002), including the Attachment Style Questionnaire (ASQ; Feeney et al., 1994). Individuals with low scores on both dimensions of the ASQ – anxiety and avoidance – have a secure attachment, those with high scores on anxiety and low scores on avoidance are classified as insecure/anxious, and those with high scores on avoidance and low scores on anxiety are evaluated as avoidant.
Within this context, various researchers have pointed out that insecure, avoidant and anxious, attachment styles can be considered a general factor of vulnerability with respect to psychopathology (Ein-Dor and Doron, 2015; Mikulincer and Shaver, 2015). For example, both anxious and avoidant attachment styles are connected to depression, anxiety (Mikulincer and Shaver, 2012), obsessive-compulsive disorder (Doron et al., 2009), and externalizing pathologies (McWilliams and Bailey, 2010).
To our knowledge, only few studies considered the associations between attachment styles and psychopathological problems in emerging adulthood, although this developmental stage is considered a turning point in the life cycle from a socio-emotional and relational perspective. Pascuzzo et al. (2015) found that romantic anxious attachment is associated in general with psychopathological problems in a sample of young adults. Cerniglia (2017) showed that university students display different psychopathological problems according to different insecure attachment styles. Finally, a recent study shows that students with high psychopathological risk attending counselling services report high frequencies of anxious and avoidant insecure attachment (Wadman et al., 2019).
No studies have considered in general the distribution of attachment styles in young adults and emerging adults in the general population and in the student population. A few other studies focussed on specific issues, including the association between attachment styles and self-reported empathy in medical students (Ardenghi et al., 2020) and stability versus change of attachment styles in a sample of young adults during transition to university (Scharfe and Cole, 2006).
Thus, given the scarcity of studies in this regard, it is of particular interest to assess the distribution of attachment styles in a sample of emerging adults, with a specific focus on those who can be considered at risk, that is, students attending counselling service. Furthermore, considering the above mentioned associations between attachment styles and mental disorders in adulthood, assessing this association also in emerging adulthood would help filling a gap in this field, given the critical nature of this period for mental health and the lack of studies in this regard.
Aims of study
In light of the above, the first aim of this study is to evaluate the quality and the clinical level of psychological distress in a sample of emerging adult university students, considering both students who requested access to a university counselling service and students who did not.
The second aim of the study is to evaluate the quality and the frequency of attachment styles in the two groups of students, considering both students who requested access to a university counselling service and those who did not.
The third aim is to test the associations between attachment styles and psychological distress in the two groups. Given the associations between insecure attachment and psychopathology in adulthood reported by previous studies, we expect to find an association between insecure attachment styles and global psychopathology severity indexes in emerging adulthood too.
Methods
Participants and procedure
University students have been recruited at University of Milano-Bicocca with the aim of forming two groups: counselling attending students and counselling non-attending students.
Counselling attending students are students that asked for admission at the university counselling service between 2013 and 2019. A total of 669 counselling attending students have been invited to participate in the research. Questionnaires have been administered right after the students’ request and before counselling started. 370 (55.6%) completed all questionnaires, with a rate of dropout from the study of 44.4%. Counselling non-attending students were recruited between November 2018 and December 2019 inviting students to participate in this research during lectures at various study courses. Counselling non-attending students had never asked for admission at the counselling service at time of assessment. Out of a total of 508 students invited, 318 of them (62.5%) filled in the questionnaires that has been sent online.
Thus, final sample was composed of 370 students in the counselling attending group and 318 students in the counselling non-attending group. The socio-demographic characteristics of the participants are reported in Table 1.
Socio-demographic characteristics of the sample.

Data collection took place entirely online, after the acquisition of written informed consent. The ethics committee of the University of Milano-Bicocca approved the research project (0038353/18).
Measures
Anamnestic information
Students filled an ad hoc form to collect socio-demographic information as: age, gender, student status (bachelor or master degree course), study’s courses, living arrangement and employment status while studying, marital status, and if they have children.
Symptom checklist 90 revised (SCL-90 R)
The SCL-90 R (Derogatis, 1994; Italian version: Prunas et al., 2011) is a 90-item self-report questionnaire (rated on a 5-point Likert scale ranging from 0 ‘not at all’, to 4 ‘extremely’) that measures the perceived severity of psychopathological symptoms over the previous 7 days. SLC-90 R includes 9 subscales: Somatization (SOM), Obsessive–Compulsive (O-C), Interpersonal Sensitivity (I-S), Depression (DEP), Anxiety (ANX), Anger-Hostility (HOS), Phobic Anxiety (PHOB), Paranoid Ideation (PAR) and Psychoticism (PSY). The instrument also has three global indexes – Global Severity Index (GSI), Positive Symptoms Total (PST) and Positive Symptoms Distress Index (PSDI). In this study, the Global Severity Index has been used as a global index. The SCL-90 R subscales showed good reliability in this study (.75 < α < .90) and the global index scale showed high reliability in this study (α = .97).
Attachment Style Questionnaire (ASQ)
The ASQ (Feeney et al., 1994; Italian version: Fossati et al., 2003) is a 40-item self-report scale (evaluated on a 6-point Likert scale ranging from 1 ‘Totally disagree’ to 6 ‘Totally agree’) which yields five factor scores. One factor (Confidence in self and others) is related to secure attachment, whereas each of the other four scales (Discomfort with Closeness, Relationships as Secondary, Need for Approval and Preoccupation with Relationships) represents a particular aspect of insecure attachment.
The ASQ scales have been grouped together in order to highlight differences with respect to the two types of insecure attachment. As indicated by Fossati et al. (2003) through the four scales which measure insecure attachment it is possible to identify the dimensions of insecurity: Avoidance and Anxiety. Following Monteleone et al. (2008), two new scales have been created relating to insecure attachment: Avoidant Attachment which is the average of the scores of the Discomfort with Closeness and Relationships as Secondary scales and Anxious Attachment which is the average of the scores of the Preoccupation with Relationships and Need for Approval scales. The ASQ scales showed good reliability in this study (.77 < α < .81).
Data analysis
All analyses were conducted using the software SPSS Statistic 26.0. Pearson’s chi-squared test has been used to compare counselling attending students and counselling non-attending students in relation to the distribution of attachment and psychopathological range. MANCOVAs have been used to compare the two groups with respect to the SCL-90 R scales and the ASQ scales. Correlation analyses have been carried out in each group to identify associations between the examined variables.
Results
Preliminar analyses
Chi-square test or t-test have been used to examine the differences between counselling attending students and counselling non-attending students on the socio-demographic variables (see Table 1). In the counselling attending group students had an higher age (t = 2.12; p = .034), were more likely to live outside of the family (χ2 = 24.01; p = .000), and to have a job (χ2 = 5.01; p = .025) as compared with the counselling non-attending group. Therefore age, student living arrangement and job have been considered as covariates in subsequent analyses.
Students attending counselling service versus students non-attending
Psychological distress
First, counselling attending students and counselling non-attending students have been compared in terms of prevalence of participants falling within the clinical, subclinical and non-clinical cut offs of the SCL-90 R according to the normative sample reported in the Italian manual (Sarno et al., 2011). In the counselling attending group, 19.7% of students (N = 73) were in the non-clinical range, 36.7% (N = 136) in the sub-clinical range, and 43.6% (N = 161) in the clinical range. In the counselling non attending group 39.3% (N = 125) were in the non-clinical range, 35.2% (N = 112) in the sub-clinical range, and 25.5% (N = 81) in the clinical range. The chi-squared test indicated a significant difference in the distribution of the SCL-90 R ranges of the two groups (χ2 = 38.71; p = .000). There were more students in the clinical range (adj = 4.9) and fewer students in the non-clinical range (adj = −5.7) in the counselling attending group than in the counselling non-attending group.
Considering the subscales and the total scale of SCL-90 R the results showed significant differences between the two groups (Pillai’s Trace F(10, 653) = 13.09; p = .000). The univariate tests indicated that the counselling attending group reported higher scores on all the subscales and on the total Global Severity Index (GSI) scale of the SCL-90 R as compared to the counselling non-attending group (see Table 2).
Comparison of psychopathological problems and attachment styles between counselling attending students and counselling non-attending students.

dl (1, 686).
p < 0.05. **p < 0.01. ***p < 0.000.
Attachment styles
The Confidence scale of the ASQ has been used to identify the distribution of secure/insecure attachment styles compared to the normative sample. Scores below the 25th percentile are considered an indicator of insecure attachment while scores above the 25th percentile are considered an indicator of secure attachment. In the counselling attending group 45.5% of students (N = 166) had secure attachment and 54.5% (N = 199) insecure attachment. In the counselling non-attending group 56.9% (N = 181) showed secure attachment and 43.1% (N = 137) insecure attachment. The chi-squared test indicated that the difference in the distribution of attachment between the two groups was significant (χ2 = 8.89; p = .003), with more insecure attachment in the counselling attending group.
Furthermore, significant differences between the two groups with respect to the ASQ scales have been found (Pillai’s Trace F(3,678) = 12.92; p = .000). The counselling attending group had lower scores on the Confidence scale and higher scores on the Avoidant Attachment and Anxious Attachment scales than the counselling non-attending group (see Table 2).
Associations between psychological distress and attachment styles
Significant associations between psychopathological problems and attachment both in the counselling attending group and in the counselling non-attending group have been found (see Table 3). By means of partial correlations (age, student living arrangement and job as covariates) significant associations have been found between the examined variables in the counselling group. The ASQ Confidence scale was associated negatively with all the sub-scales and with the Global Severity Index of the SCL-90 R. The Avoidant Attachment and Anxious Attachment scales were positively associated with all the subscales and with the total scale of the SCL-90 R.
Correlations between psychopathological problems and attachment styles.
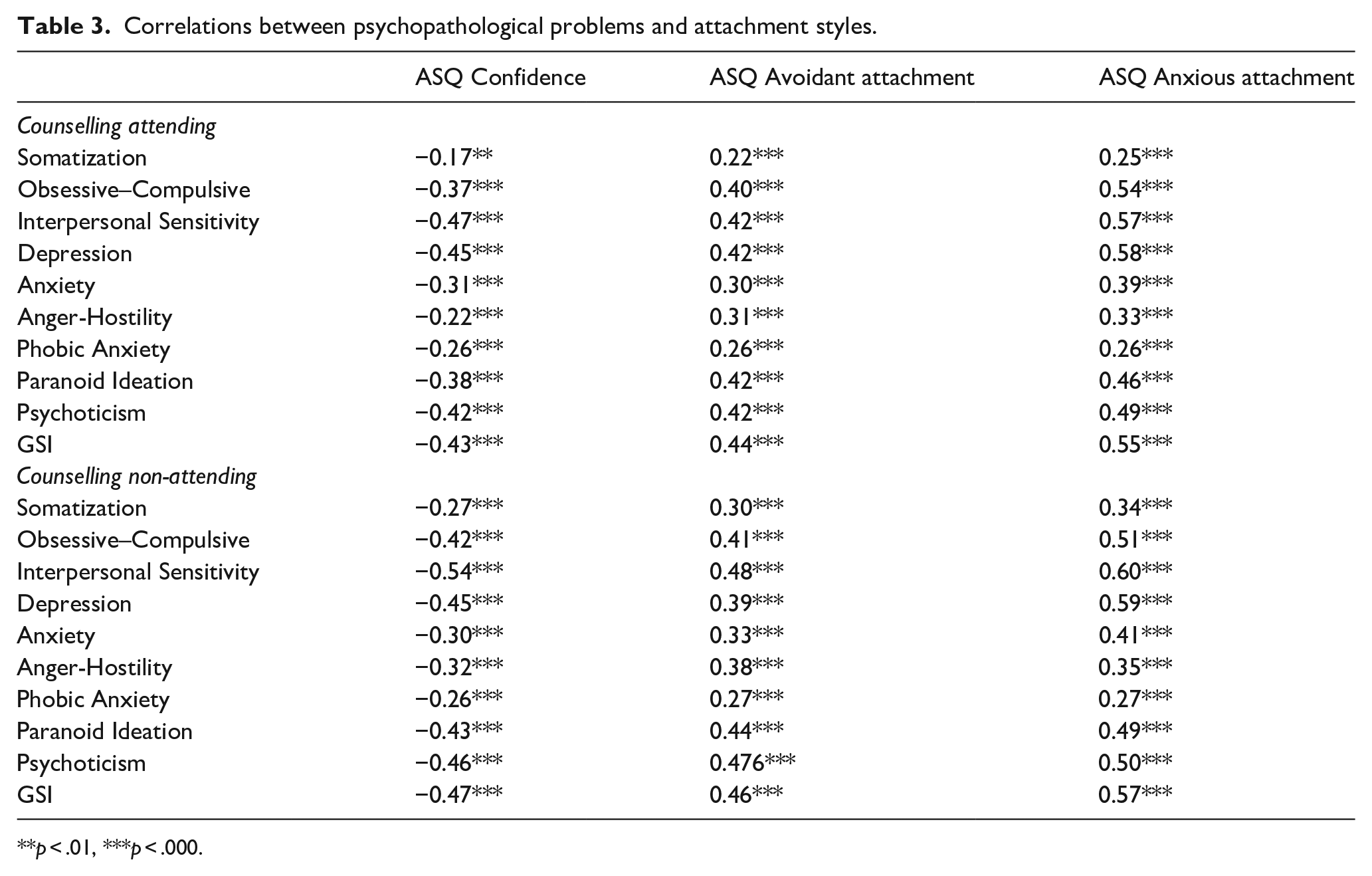
p < .01, ***p < .000.
Significant associations have been found in the counselling non-attending group (see Table 3). The ASQ Confidence scale was negatively associated with all the subscales and with the total scale of the SCL-90 R. The Avoidant Attachment and Anxious Attachment scales were positively associated with all the subscales and with the total scale of the SCL-90 R.
Discussion
The main aim of this study was to evaluate and compare level and quality of psychological distress and attachment styles in two groups of emerging adult students: counselling attending and counselling non-attending. Furthermore, this study aimed to highlight possible associations between psychopathological problems and attachment styles in both groups.
Firstly, the results show that most of the students who requested counselling were in the clinical (43%) and subclinical (36%) range of SCL-90 R. These results are quite similar to those reported by Kreß et al. (2015) on a German sample, according to which around 54% of students who request support from the university counselling centre have clinically significant symptoms. Furthermore, students of the counselling attending group differed from those of the counselling non-attending group in that they reported a generalized psychopathological profile, with higher scores on all the subscales and on the total scale of the SCL-90-R. In other words, they reported more psychopathological symptoms across the externalizing (Anger-Hostility), internalizing (Somatization, Depression, and Anxiety), psychotic (Psychoticism and Paranoid Ideation), obsessive-compulsive dimensions and in terms of global symptom severity.
The results also underline that 25% of the counselling non-attending students, albeit not requesting psychological support, showed psychopathological problems falling within the clinical range. In the aforementioned German study (Kreß et al., 2015) the prevalence of psychopatological symptoms among students who do not use the counselling centre is lower with a percentage about 15%. On the other hand, another review on samples of European students found that 20%–25% of students in general reported a mental disorder (Holm-Hadulla and Koutsoukou-Argyraki, 2015). This study therefore provides further results in the field of European student populations, given the few studies on this subject.
For what concerns attachment styles, the comparison of the two groups revealed a significant difference in the distribution of security/insecurity, computed through the ASQ Confidence scale. In the counselling attending group, there was a prevalence of insecure attachment while in the counselling non-attending group secure attachment style was the most prevalent. Students in the counselling attending group showed lower scores on the Confidence scale which relates to secure attachment and higher scores on both Avoidant Attachment and Anxious Attachment insecure scales.
The distribution of attachment styles found in the two groups is in line with the international literature on clinical and non-clinical samples that relies on the AAI (Bakermans-Kranenburg and van IJzendoorn, 2009). Students in the counselling non-attending group have a percentage of secure attachment which is similar to that of the general population, whereas students in the counselling attending group have a percentage of secure attachment which is similar to that of clinical samples. These results, bringing new finding to the literature, thus show that the distribution of attachment of emerging adult students is similar to that of the non-clinical and clinical populations of other ages for both the counselling non-attending group and the counselling attending group. A more specific comparison would, however, require normative data gathered with the ASQ questionnaire.
The data relating to significant associations between psychopathological problems and attachment styles are particularly interesting. It is important to observe in this regard that similar associations in both groups between psychopathological problems and attachment styles have been found. In both the counselling attending group and the counselling non-attending group general psychopathological problems and specific symptoms were all associated with lower levels on the ASQ Confidence scale, and with higher scores on the Avoidant Attachment and Anxious Attachment insecure scales. However, no specificity of associations emerged between psychopathological problems and attachment styles. In this regard the results confirm hypotheses of the study and those of, inter alia, Mikulincer and Shaver (2012, 2015) whereby insecure attachment styles can be considered in general to be a dimension of personality involving vulnerability with respect to psychopathology rather than being associated with specific psychopathological disorders.
The study does have its limits. The first concerns the composition of the sample which is mainly female; this could influence the generalizability of the results. It must, however, be pointed out that there are also more females than males in the relevant normative samples of young adults as regards both attachment and psychopathological problems. Furthermore, the study was carried out with students from a University in Northern Italy; for greater generalizability of the data, the study should be extended to other Italian regions.
Moreover, psychopathological problems were assessed through self-report questionnaires and not through diagnostic interviews. It might be that online administration of self-report questionnaires was responsible for the high rate of drop-out in this study. Future studies should address this issue. For example, measures, online or in person, could be administered as routine intake assessment to all individuals asking for admission at the counselling centre.
Conclusions and clinical implications
This study shed light on the psychopathological profile of emerging adults who attend counselling services. Such profile is characterized by general psychopathological distress and psychopathological problem of both internalizing, externalizing and psychotic dimension and by quality of attachment styles with more insecure than secure attachment. The study also underlines that among students who do not request support to counselling service there is a marked percentage of students with a clinical psychopathological profile and insecure attachment styles.
Furthermore, the study shows the close relationship between insecure attachment and psychopathological problems, both in counselling attending students and non-attending students, highlighting insecure attachment as a possible risk factor with respect to the onset of psychopathology in emerging adulthood.
The results of this study have significant clinical implications. First, they confirm the usefulness of counselling services, since the group of students who turn to them have, a high percentage of psychopathological problems. Given the association between psychopathological problems and insecure attachment, the results also suggest the importance of paying particular attention in psychological counselling for students not only to psychopathological problems but also to anxious or avoidant insecure attachment styles.
Lastly, it is important to note that this study found, in the counselling non-attending group, a number of ‘silent’ students who, albeit not requesting psychological help, display psychopathological problems. This is particularly significant in relation to the implementation of communication strategies by universities, which can intercept students who, although at risk as regards both psychopathology and attachment, have not yet been reached by counselling services. This could expand the eminently preventive function that counselling services traditionally serve by supporting emerging adult students in the difficult transition to young adulthood.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.