
Abstract
This qualitative study explores informal caregivers’ experiences of supporting persons with dementia’s everyday life coping. In the future, there will be fewer health personnel, increased dementia prevalence and limited nursing home availability. Accordingly, close relatives may be compelled to assume greater care responsibilities. Knowledge concerning persons with dementia’s everyday coping from the perspective of informal caregivers remains insufficient, despite these people’s importance for those with dementia. This investigation analyses informal caregivers’ perceived challenges and pleasures in providing care, how home health care affects everyday life coping and the factors that are most important to informal caregivers in supporting care receivers.
Keywords
Introduction
This study elucidates the value of incorporating informal caregivers’ experiences when planning and delivering psycho-social services to home-dwelling persons with dementia. Growing numbers of persons are forecast to suffer from dementia in the future, rendering this a pertinent societal challenge (World Health Organization [WHO], 2012). Dementia is likely to consume an increasing proportion of national resources, both financially and professionally. Many nations aim to help persons with dementia stay in their homes longer with adequate care (Kraijo et al., 2015; WHO, 2012), and in the future it is expected that there will be fewer health personnel and limited access to nursing homes. Consequently, informal caregivers like cohabitants, sons, daughters, daughters- or sons-in-law, friends and neighbours are expected to substitute for some of the municipal care currently provided to those with dementia (WHO, 2012).
Dementia diseases are characterised by impaired mental capacity and psychological processing (WHO, 2012). Persons suffering from dementia may develop behavioural disorders and psychological symptoms, like restlessness, confusion, depression, hallucination, paranoia, anxiety and delusion (Engedal and Haugen, 2018). These symptoms will be observed by their informal caregivers.
Informal care and home health care represent two different support network systems: primary and secondary relationships, respectively (Bø and Schiefloe, 2015). Primary caregivers are those who spend most of their time with the home-dwelling person with dementia, whereas secondary caregivers are those who play a supplementary role in providing care (Gaugler et al., 2003). The connections between primary and secondary relationships are dynamic, with no strict boundaries.
The majority of persons with dementia live in their own homes, cared for by informal caregivers (Jackson et al., 2019), who usually constitute their most important support (Austin et al., 2016; Colquhoun et al., 2019; Lamore et al., 2017). Society may prove more successful in enabling persons with dementia to cope in everyday life by cooperating with such informal caregivers (Austin et al., 2016; Kitwood, 2019; WHO, 2012). Everyday life coping can be defined as a health-promoting and preventive mindset, regardless of an individual’s functional level (Tuntland and Ness, 2014). Developing strategies for supporting persons with dementia requires knowledge about the utility of closer collaboration between informal caregivers and municipal professionals.
Dementia has an immense impact on the lives of the family members as the disease develops, especially straining the main caregiver psychologically (Austin et al., 2016; Colquhoun et al., 2019; Nordtug and Holen, 2011; Nordtug et al., 2010; Quinn et al., 2015; Stall et al., 2019). One Norwegian study revealed that over half of the cohabitants of people with dementia were found to have a mental illness such as severe depression, anxiety and insomnia (Nordtug et al., 2010). Informal caregivers’ distress related to their caregiving role may also exacerbate the health outcomes of the person with dementia, including behavioural and psychological symptoms and elder abuse (Stall et al., 2019). In addition, informal caregivers may experience social withdrawal from their family and friends (Nordtug et al., 2010; Quinn et al., 2010). This can lead to them losing much of their former social support, including emotional and instrumental assistance, as well as information and appraisals relevant to their self-evaluations (Ali et al., 2018; Giddens and Sutton, 2013).
In spite of these findings, caring for a persons with dementia may also result in positive outcomes, like new insights, pride in one’s role, wisdom, satisfaction, mastery, emotional rewards, better relationships and satisfaction in the notion of reciprocity (Austin et al., 2016; Bédard et al., 2005; Lloyd et al., 2016). Informal caregivers may come to feel grateful to the person with dementia and participate actively through positive reframing, acceptance, humour, seeking emotional social support, providing religious support and demonstrating caregiving competence (Lau and Cheng, 2017; Márques-González et al., 2007; Papastavrou et al., 2011).
Persons suffering from dementia usually prefer to remain in their homes, but they may perceive home health care as it is performed today as a threat to their individual independence (Stephan et al., 2018). According to the WHO (2012), persons with dementia and their informal caregivers should be involved in plans and services that relate to them. Society, informal caregivers and persons with dementia share mutual interests in making adequate home health care a feasible option for as long as possible. Nevertheless, knowledge concerning persons with dementia’s everyday life coping seems to be lacking from the perspective of informal caregivers. There is a need to listen to the voices of the informal caregivers of persons with dementia in order to gain useful knowledge that can be operationalised when planning future dementia care. Accordingly, the aim of this study is to explore informal caregivers’ experiences of what affects everyday coping of home-dwelling persons with dementia’ and their carers.
Method
The study has a qualitative design, based on three focus group interviews (Krueger and Casey, 2000).
Sample
The study was approved by the Privacy Issue Unit of the Norwegian Social Science Data Services (Project number 58922). The informants were purposively selected from informal caregivers of home-dwelling persons with dementia in Norway. They were recruited by the Municipal Dementia and Memory Teams in three municipalities, with approximately 3000, 15,000 and 50,000 inhabitants, respectively.
The informants received written and verbal information via municipal nurses. Written consent was obtained from all. They were assured full anonymity and were free to withdraw from the study at any time with no consequences. Fourteen informants participated: seven cohabitants, of whom four were wives; and seven children, of whom four were daughters. The youngest was 49 years old, while the oldest was 82.
Interviews
The focus group interviews took place between May and June 2018. A semi-structured guide directed the interviews, which explored the caregivers’ relationships to their care receiver, the kind of care they provided, the experiences they had with the challenges of the illness both for the person with dementia and themselves, formal help and the aspects they regarded as important to the person with dementia in order to cope in everyday life. They were encouraged to talk freely and a moderator followed up with questions when needed (Krueger and Casey, 2000). The moderators were researchers and the co-moderator either a researcher or a research assistant. All three interviews were audio-recorded and transcribed verbatim. The three interviews each lasted up to 2 hours.
Data analysis
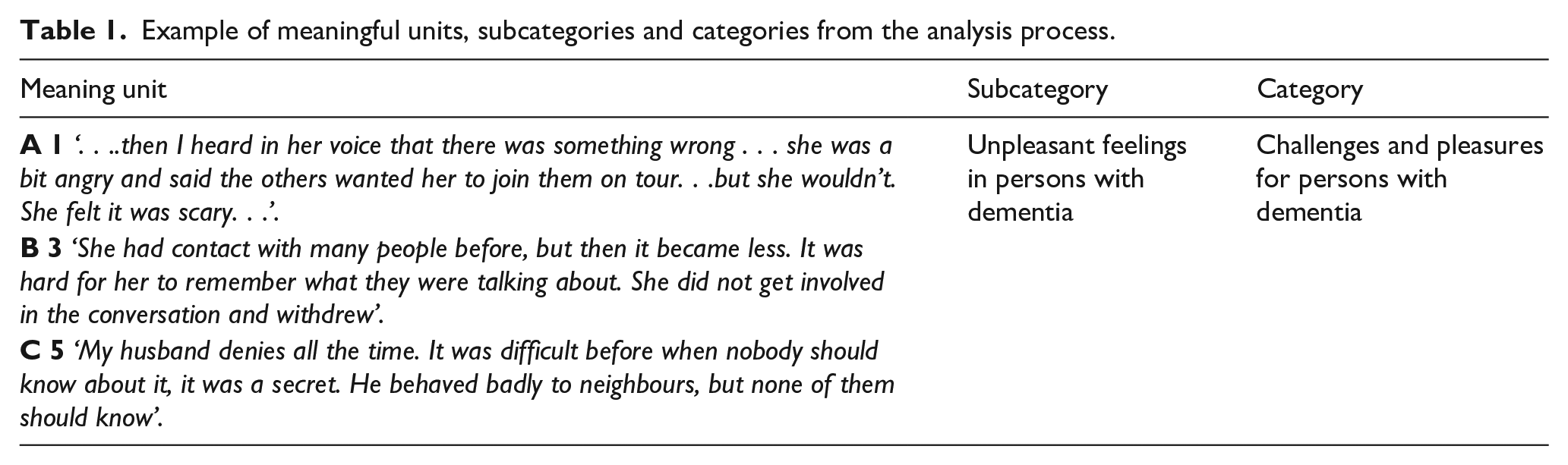
The text was analysed by manifest content analysis, inspired by Graneheim and Lundman (2004). First all the text was read several times to develop an overall impression. Next, meaning units relevant to the aim of the study were identified and then sorted. Those dealing with the same unit were placed within the same subcategory. The subcategories’ similarities and differences were identified and each was placed under different concepts, which constituted two main categories (see the example in Table 1 below).
Example of meaningful units, subcategories and categories from the analysis process.
Results
The two categories identified indicate informal caregivers’ views of what affects coping in everyday life for home-dwelling persons with dementia. The first category pertains to persons with dementia, while the second refers to informal caregivers.
Challenges and pleasures for persons with dementia
These observations were about the persons with dementia’s emotions, their everyday coping issues, and reactions to the given practical professional help.
Unpleasant feelings in persons with dementia
This subcategory illustrates the subjective perceptions of different negative feelings. One daughter described a phone call with her mother, during which they discussed a tour to which the latter was invited: ‘. . .. then I heard in her voice that there was something wrong . . . she was a bit angry and said the others wanted her to join them on tour . . . but she wouldn’t. She felt it was scary’. Here the daughter perceived anger and fear in her mother’s voice.
Another daughter explained: ‘She had contact with many people before, but then it became less. It was hard for her to remember what they were talking about. She did not get involved in the conversation and withdrew’. The daughter thus understood the reason why her mother withdrew from others.
Some of the persons with dementia struggled to accept the disease. One wife said: ‘My husband denies all the time. It was difficult before when nobody should know about it, it was a secret. He behaved badly to neighbours, but none of them should know’. In this way, her husband did not want anybody to know about the disease but behaved inadequately to their neighbours.
Problematic practical coping of persons with dementia
In many cases, the persons with dementia did not eat sufficiently or ate excessive unhealthy food. One daughter stated: ‘The food from home health care he was supposed to warm up . . . it just stood there all weekend. I think he has started drinking a lot of coffee and eating brown sugar . . . an incredible amount of sugar’. The daughter thus believed that her father was unable to eat properly.
One husband described how his wife deemed it unnecessary to shower and hence refused to do so. He used to explain to her: ‘There is no choice, I have showered and now it is your turn. So far it has gone well’. He therefore had to make decisions about her hygiene and force her to shower.
Pleasures in everyday life for persons with dementia
The informants believed that being with like-minded people could help build pleasure among persons with dementia: ‘Get out and meet other persons with dementia . . . it gives her so much (at the day care centre). That’s what makes her days important . . . meaningful’. The daughter thus perceived that her mother liked being among other persons with dementia at the day care centre; otherwise, she would not be with her old friends as before: ‘When she was invited to the birthday of an old friend, she told them she couldn’t come because she wasn’t able to walk . . . But she does go on walking tours (facilitated by municipality care) with persons with dementia once a week’. Here the daughter noted that her mother seemed to prefer joining like-minded persons with dementia above others and would thus find excuses to withdraw.
Likewise, the informal caregivers perceived that their care receiver enjoyed doing activities in which they were still competent. One example was a daughter who perceived that her mother was proving successful in undertaking her customised daytime activities: ‘It was amazing, and she was really looking forward to it. She worked in the kitchen every day, set and cleared the tables. Washed windows, dusted and folded clothes. . .she had a new job. On the weekends she slept and waited for Monday’. Her mother thus found pleasure in doing meaningful work at the day care centre.
Other persons who were more significantly affected by dementia were also seen to benefit from customised daytime activities. As one wife explained: ‘He can’t converse anymore . . . and he falls easily. He is very happy at the day care centre. He eats well, because he has gained weight. If people are gentle and safe, he is fine’. She thus recognised his pleasure of being at the day care centre, despite his shortcomings.
Not all persons with dementia could attend activities. Nevertheless, their informal caregivers acknowledged the pleasure they found. One daughter said: ‘What gives her pleasure is that we are there, and to be outside when the weather is nice. I see how happy she is when we come’. Indeed, her mother enjoyed nature and being with her family.
Many professionals, inadequate attitudes and limited time
One daughter described the following of the home health care personnel: ‘They must respect the persons with dementia. Some speak with a childish voice . . . my mother reacts to that . . . and does not want help from them’. Thus, this person with dementia did not like being spoken to in an infantile way. Staff who behave with respectful, calm attitudes were said to receive better reactions: ‘She recognises some faces . . . these friendly faces. . . she has noticed them’. The daughter therefore observed that her mother could recognise friendly and calm, non-verbal signals.
Another daughter explained how her mother did not want to be washed by some professionals: ‘They say they can’t force her, but then it’s strange that some of them get to bathe her while others don’t’. The informant thus observed contrasting behaviour among the home health care personnel, sometimes resulting in successful bathing and sometimes not.
The challenges faced by the home health care personnel in doing their work were acknowledged by another daughter: ‘Two or three minutes they spent with my mum. How should they be able to motivate her to shower, eat and so on?’ In this way, the daughter understood the difficulties of their work.
The informal caregivers in large municipalities recognised that many different home health care personnel are involved in supporting persons with dementia. One husband said: ‘I do not like how 10 to 12 different people come . . . there are too many . . . I can see she gets confused’. He thus noted how his wife can become confused when she must relate to too many professionals.
Informal caregivers’ needs
The importance of having an understanding informal network, having the opportunity to obtain professional information, and safety for the person with dementia emerged as informal caregivers needs.
Gaining understanding from informal networks
The informal caregivers highlighted the importance of having affirmative conversations about their caring situations, whether with fellow informal caregivers or other people. One wife explained: ‘The constant confirmation that others are also experiencing the same thing is OK’. In this way, she liked to hear that others shared her experiences.
One husband said: ‘I talk to the group I meet every day at the mall . . . Talk about the dementia challenges . . . and they help me . . . The family withdraw, but these people follow up’. He thus appreciated talking with his group, even as the family withdrew.
Others were distrusted by their family and their network: ‘My husband isn’t demented they say, and they meet him for only 5–10 minutes, and then he seems normal’. This wife thus felt distrusted.
Some siblings shared care responsibilities for their parents. As one daughter noted: ‘We four siblings provide care one week each’. Thus, these siblings collaborated to provide care.
Possibility of obtaining professional information about caring
One daughter narrated: ‘We got information about the disease when it was diagnosed, but nothing about how the disease turned out’. She thus desired additional information.
Others enjoyed access to specialised health personnel in their municipality, who could be contacted when necessary. As one wife said: ‘If anything happens, I can make a phone call to X (a geriatric nurse). So, I feel I have very open dialogue with those in the dementia team’. She was pleased by the opportunity to contact professionals with knowledge and skills in dementia care.
During the development of the illness, new challenges always arose. One husband explained: ‘I feel so helpless, and it’s not just about going out and getting more help either’. Thus, he felt inadequate, having nobody to talk to about his challenges.
Another husband said: ‘What makes everyday life easier is about what goes on in your own mind, your own thoughts . . . that you have a good conscience, but I feel that I am not doing it right, just as you think a little wrong, even it’s not the point’. In this way, he was unsure if he was acting appropriately.
Safety for persons with dementia
Some of the informants valued having time for themselves and were confident that their care recipient would be well at such times: ‘Knowing that he is well and not sitting being anxious, makes me feel safe when I am away’. Another informant said: ‘The municipality has a person who can be with persons with dementia, while I am doing something for myself’. In this way, the municipality could enable informal caregivers to enjoy some free time.
Furthermore, receiving customised offers in dementia home health care made life easier for the informal caregivers: ‘Now offers come more and more, I know I can relax more now; dinner delivery, day care centre, visitor friends, tour groups’. Therefore, this daughter felt that she could relax more now that her mother receives a greater number of offers during the week.
Discussion
The main findings have highlighted the challenges and pleasures experienced by home-dwelling persons with dementia, affecting their coping in everyday life, as perceived by their informal caregivers. In order to adequately support the person with dementia, the informal caregivers needed knowledgeable information about the illness and its symptoms, support from their primary relationship and to know that the person with dementia is safe when they are alone.
Perceived challenges for persons with dementia
The informal caregivers seemed to recognise the person with dementia’s emotions and situations earlier and more clearly compared to health care personnel. One example was the husband acknowledging his wife’s confusion by noting that there were too many home health care professionals.
Some informants perceived that the person with dementia was struggling to accept the dementia diagnosis, like the one who behaved badly to his neighbours. Crisis reactions like anger, despair, shame and the use of psychological adaptive mechanisms such as denial and repression all appeared in our study. Dementia may affect the persons with dementia’s self-esteem before they come to terms with their illness (Nordtug et al., 2018). Self-esteem is a perception of one’s own worthiness and self-respect as well as that others deem one worthy and respectable (Mruk, 2006). When a persons’ integrity and self-respect are compromised, shame and violent rage often ensue (Wurmser, 1995). An expression of dementia might be revealed by others, exposing the persons with dementia’s inner vulnerability that they do not want others to see (Wurmser, 1995). Such a revelation may be perceived by the person with dementia non-verbally and provide a reason to withdraw from others (Colquhoun et al., 2019). One example here was the mother who withdrew more and more from others because she could not remember what they were discussing, surely a significant loss for her.
As long as persons with dementia wrestle with strong negative feelings, their possibilities of developing new mental strategies that might strengthen their self-esteem, self-respect and dignity are diminished (Nordtug et al., 2018; Tranvåg et al., 2015). Adapting the situation for persons with dementia seems to be easier when they are supported by informal caregivers (Austin et al., 2016; Gilbert, 2013) from their primary relationship. Support may be more coherent and accepted when it comes from respected informal caregivers (Ali et al., 2018; Gilbert, 2013). Such relationships are often marked by trust and safety (Bø and Schiefloe, 2015), established long before the illness appears. Thus, informal caregivers may provide safe conditions for persons with dementia. Such primary relationships are more likely to flourish in cooperative contexts where the individuals know one another in multiple roles, support each other and respond affectively to emotional needs (Bø and Schiefloe, 2015). The daughter who heard fear in her mother’s voice illustrates the sensitivity of such a close relationship, where the mother’s fear was the challenge.
The cooperative context in primary relationship may also be true when the person with dementia does not agree, as in the case of the wife who deemed it unnecessary to shower, as her husband managed the task. Informal caregivers’ motivation is usually marked by emotional bonds and a sense of obligation, including companionship (Quinn et al., 2010), rendering the care meaningful (Quinn et al., 2015).
Secondary relationships are characterised by formal, impersonal and distanced contacts with fewer yet more well-defined roles (Bø and Schiefloe, 2015). Relationships between members are to a lesser extent based on trust and are less likely to lead to strong loyalties or durable social bonds (Bø and Schiefloe, 2015). The home health care personnel referred to by the informants in this study, conducting short visits of just a few minutes in their homes, were not always recognised by the person with dementia. Likewise, the informants revealed that some measures under the direction of municipal care, such as bringing dinner, were unable to solve the real challenge of nutrition. The measures were not evaluated by talking to the informal caregivers and the person with dementia was not always able to answer the professionals adequately.
Furthermore, a lack of knowledge about dementia seemed to characterise some home health care professionals’ attitudes, such as through talking in a childish manner. Such behaviour might result in a reinforcement of their shortcomings and insecurity, diminishing their quality of life (Næss et al., 2011), rather than supporting their everyday life coping (Gilbert, 2013; Giddens and Sutton, 2013).
At any rate, there seems to be a need to reduce the number of home health care personnel visiting persons with dementia and to increase their knowledge about the illness and special dementia caring. This requires strategic changes to the organisation of home health care visits and financial support for staff’s further education.
Informal caregivers’ perceptions represent useful knowledge for health professionals, as the assessment basis for decisions can become more comprehensive. Co-creating measures together with informal caregivers in order to come to terms with the mental losses and challenges experienced due to the disease might result in more person-centred caring (Gilbert, 2013; Kitwood, 2019; Rokstad et al., 2013) and may help process challenges and facilitate better everyday life coping. Thus, the co-creation of solutions with informal caregivers may lead to better measures, and the most potent measures might be co-creating with professionals having knowledge about dementia care (Kitwood, 2019). However, having the opportunity to continue collaborating and to evaluate measures along the way represent prerequisites.
Perceived pleasure in persons with dementia
The informants perceived positive feelings of pleasure in their care recipients, linked to situations where they seemed safe, felt understood and were happy in their way of being and experienced no devaluating shortcomings. According to some informants, the persons with dementia would remember these situations, such as the mother with dementia who looked forward to Mondays, when she could work in the kitchen at the day care centre. By thinking about positive situations, the persons with dementia would experience a temporary surge in self-esteem and satisfaction, positive aspects of quality of life (Bruner, 1990; Hughes, 2013; Næss et al., 2011; Surr, 2006). These activities were meaningful and connected to positive interpersonal relations. Satisfaction and other positive emotions alongside a strong sense of self might boost a person’s ability to cope (Gilbert, 2013; Giddens and Sutton, 2013). This might also apply to persons with dementia. Participating in pleasurable activities may counterbalance some of the pain associated with the illness (Austin et al., 2016; Elliot et al., 2014). It may not be obvious which activities result in pleasure for a specific individual, but informal caregivers might know (Tretteteig et al., 2016). One example from our study was the mother who enjoyed visits from her family and sitting outside on sunny days. To facilitate pleasurable targeted activities that support persons with dementia’s everyday life coping, municipal health care professionals should collaborate with informal caregivers.
Support of informal caregivers from their primary relationships
The informal caregivers emphasised the utility of talking to those in their primary relationships, especially like-minded peers. Sharing experiences and challenges in dementia care helped them to be seen, gain understanding and receive help and support. These findings are in line with other studies (Colquhoun et al., 2019; Gilbert, 2013). One informant would talk to his friends at the mall, while others would chat with peers in pre-arranged groups, or with their siblings. Such collaboration appears to provide a safe, natural sociocultural learning environment that might promote creativity, development and recognition (Rienecker et al., 2015), involving emotional support, information and appraisal relevant to self-evaluation, as also reported elsewhere (Ali et al., 2018; Colquhoun et al., 2019). Consequently, people can increase their capacity to meet the challenges of caring. Informal dementia caring entails a lot of uncertainty and carers’ receipt of confirmation that they are performing correctly reinforces their self-esteem and personal identity and leads to better coping (Gilbert, 2013; Giddens and Sutton, 2013).
However, some informants noted that some persons in their primary network did not believe the person with dementia was ill. Not being believed or receiving criticism represented a burden. Other persons in their network withdrew, an important issue because a lack of social support is linked to decreased mental health (Nordtug et al., 2010). Preparing informal caregivers for such situations can mitigate some of their unpleasant outcomes. Municipal health care might consider creating regular opportunities for informal caregivers to talk to other informal caregivers of persons with dementia in order to overcome these issues.
Knowing that the person with dementia is safe
To obtain the full advantages of meeting other informal caregivers or participating in desired activities, the caregivers needed to know that their care receiver felt (and was) safe while they were away. Otherwise, the informal caregivers felt bothered and concerned, as described elsewhere (Neville et al., 2015).
When dementia progresses, self-reliance declines while the need for care and the caring burden both increase (Nordtug and Holen, 2011; Stall et al., 2019). At the same time, a person with dementia’s capacity to reciprocate, care and participate in activities with others dwindles. Less care and less positive support from the person with dementia may imply less confirmation of an informal caregiver’s identity. This might undermine their ability to cope with their caring challenges (Giddens and Sutton, 2013). Enabling informal caregivers to find some time for themselves might strengthen their caring capacity (Neville et al., 2015; Nordtug et al., 2010), but they also need to know that their care recipient is safe. According to the informants, some municipalities now have arrangements for this and cooperating with volunteers could represent a potential part (Malmedal et al., 2020).
In addition, facilitating opportunities for informal caregivers to do things for themselves while knowing that their relative is safe, can have an indirect effect on the person with dementia’s ability to cope in everyday life.
The need for information
This study has shown how informal caregivers need more information about dementia, how the disease might develop, caring management and available municipal support. The need for confirmation that one is doing the right thing or finding other ways to care is crucial. Information and support can attenuate behavioural and psychological symptoms and behavioural disorders (Nogales-González et al., 2015; Stall et al., 2019).
The information and its extent given to the municipalities differed greatly. Nevertheless, the informants experienced better understanding and cooperation with geriatric nurses compared to others. An additional advantage of the nurses was that they knew the unique caring situation in question, enabling conversations to become more person-centred, with the informal caregiver not needing to explain the situation in detail each time. Continuity and efficiency were safeguarded and time was saved.
The fact that the caring burden of informal caregivers might result in mental illnesses in spite of the home health care being provided (Nordtug et al., 2010) indicates that municipal care is not being developed in line with informal caregivers’ needs. Creating a service whereby informal caregivers can ask and discuss caring questions with knowledgeable professionals may prevent them from becoming overwhelmed (Kraijo et al., 2015; Siegel, 2012; Stall et al., 2019). Co-creating measures built on informal caregivers’ perceptions of the challenges and the pleasures of the person with dementia, alongside increased dementia knowledge, might enable caregivers and care receivers alike to become better adapted to cope with everyday life. Other studies have shown that competent health personnel are sought to answer informal caregivers’ questions (Bunn et al., 2016). Figure 1 depicting that collaboration and shared understanding between informal caregivers, persons with dementia and health professionals strengthens the system.
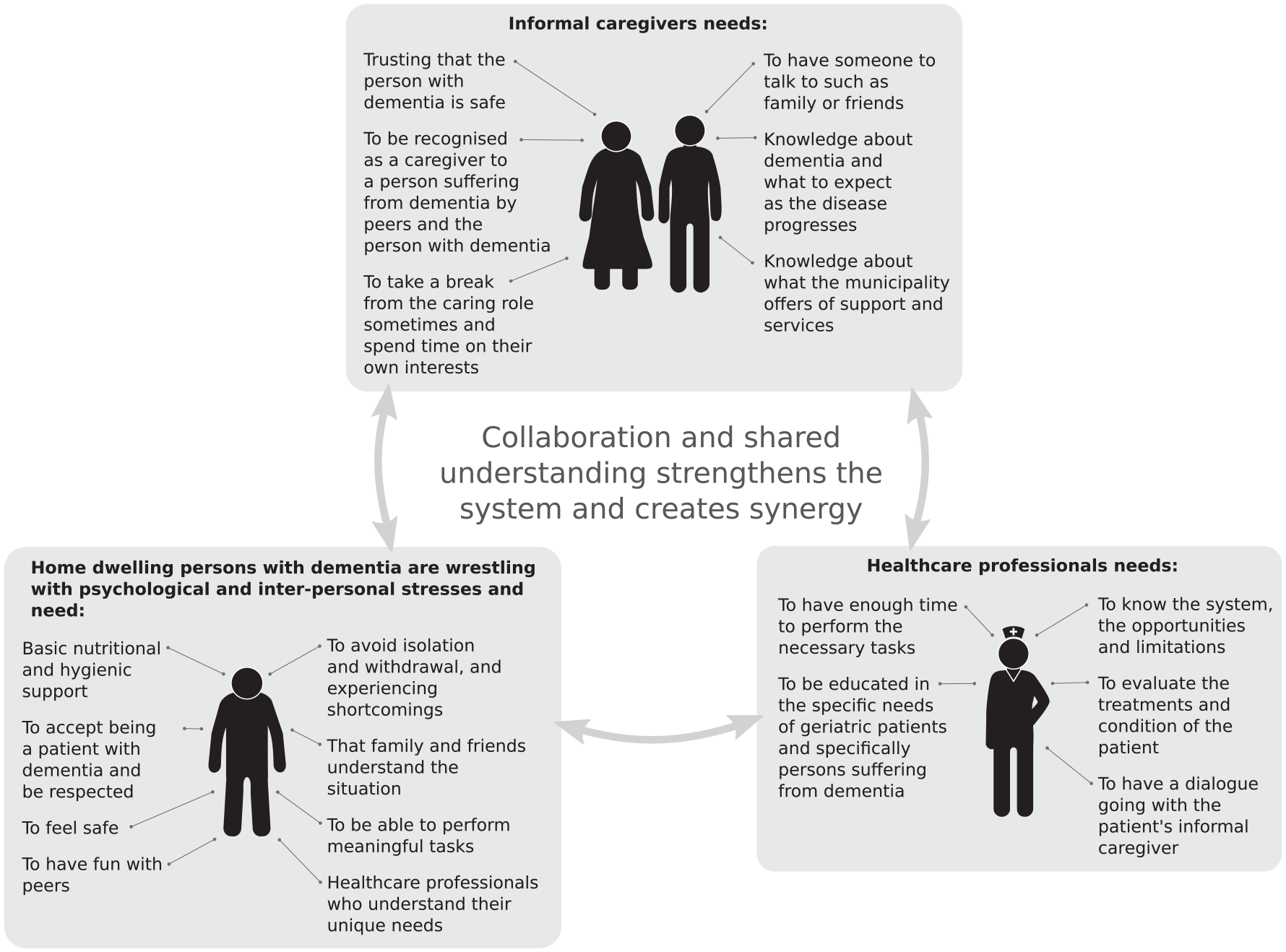
Figure illustrating that collaboration and shared understanding between informal caregivers and health professionals strengthens the system and creates synergy.
Conclusion
Informal caregivers are usually the most important persons to home-dwelling persons suffering from dementia. The relationships and the contact they offer their care recipients often constitute a resource in person-centred dementia care. Informal caregivers are frequently available for longer periods than home health care personnel on short visits. To increase the person with dementia’s everyday life coping, informal caregivers’ perceptions and knowledge of the person with dementia seem to be valuable information. Home health care personnel may co-create measures together with informal caregivers and re-evaluate these solutions as the illness develops. This requires that home health care personnel receive more expertise on dementia and dementia care. In addition, informal caregivers need opportunities to obtain more information and discuss their caring challenges during the illness period, both with knowledgeable professionals and like-minded people. Furthermore, informal caregivers need to feel confident that their care recipients are safe when they take time for themselves. This study demonstrates that sharing information and experiences can assist persons with dementia, their care-givers, and home health care personnel to better understand and respond to each other’s needs so that their responses can fit well and contribute to efficacy and wellbeing for all role-players.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Regional Research Fund Mid-Norway.