
Abstract
The use of various forms of contraception in Ghana gained prominence after the government resorted to investing more in family planning programs when maternal mortality was declared an emergency in the country. In Ghana, the intention to use and actual usage of contraceptives is influenced by many factors, which may lead to non-usage or discontinuation. This quantitative study was conducted to determine risk and protective factors impacting on the intention and usage of contraceptives. Survey data from the Ghana 2014 Demographic and Health Survey (DHS) (n = 9396) was used. A sub-sample of 7661 women in their reproductive age were included in this study, who reported being sexually active within the last year. Logistic regression analyses were conducted to test the association between a broad range of risk and protective factors including religion, early sexual intercourse, frequency of sex, number of lifetime sexual partners with intention to use contraception. We controlled for income, educational attainment, and age. Overall (n = 3661; 47.8%) reported no intention of contraception use. Logistic regression analysis revealed that no formal education (OR = 1.49; 95% CI, 1.29–1.72; p < 0.001), and primary school as highest educational level (OR = 1.19; 95% CI, 1.04–1.25; p < 0.001), Islamic religion (OR = 0.73; 95% CI, 0.59–0.90; p < 0.001), not currently employed (OR = 1.50; 95% CI, 1.34–1.69; p < 0.001), husband opposing contraception use (OR = 2.19; 95% CI, 1.42–3.46; p < 0.001), and currently pregnant (OR = 1.30; 95% CI, 1.09–1.54; p < 0.001) were also positively associated with no intention of use. Engaging religious leaders for advocacy in the community was identified as an approach to address barriers and increase awareness on contraceptive use. Targeted family planning programs should intensify public education on safe sex behaviors.
Introduction
Family planning and contraception play an important role in reducing maternal morbidity and mortality by preventing unintended pregnancies (Atakro et al., 2019; Nyarko, 2020). This is in line with the Sustainable Development Goal (SDG) that focuses on ensuring healthy lives and promoting well-being for everybody at all ages (Nyarko, 2020; Pradhan et al., 2017; UNCG SDGs, 2017). Also, Ghana’s population has continued to increase at large rates (Cooke et al., 2016; Kpessa-Whyte, 2018). The Government of Ghana enacted the National Population Policy in 1969 to help manage the country’s population, reduce constraints on future economic growth, and to facilitate economic stability (Aviisah et al., 2018). The policy was revised in 1994 to reduce the country’s total fertility rate to three by 2020 (Nketiah-Amponsah et al., 2012). One way to partly achieve the reduction in total fertility rate was to ensure an increase in the contraceptive prevalence rate to 50% by 2020 (Nketiah-Amponsah et al., 2012).
However, according to the 2014 Demographic and Housing Survey, the prevalence of modern contraceptive use among women of reproductive age in Ghana stands was reported at 22% (Aviisah et al., 2018). This prevalence rate, which is similar to that of many Sub-Saharan African countries is very low (Creanga et al., 2011; Rossier and Corker, 2017). However, when compared to the global prevalence rate (63%) of modern contraceptive use among women of reproductive age, the rate is about one-third (Aviisah et al., 2018).
Socio-cultural factors have affected the demand and uptake of contraceptives in many Sub-Saharan African countries (Aryeetey et al., 2010; Gyimah et al., 2012; Hindin et al., 2014). This gives reason to why family planning continues to be undermined in these countries as well as the high population growth (Apanga and Adam, 2015; Aviisah et al., 2018; Gyimah et al., 2012). Religion is one such factor affecting the use of contraceptives in Africa (Gyimah et al., 2012; Laryea et al., 2016); A study showed that Muslim and Traditional women in Ghana, were more likely to have never used any form of contraceptive (Gyimah et al., 2012). Socio-economic and contextual factors such as proximity to health facilities also affect contraceptive use in Ghana (Nyarko, 2020). A study showed that women who were either uneducated, unemployed, or never-married were most likely to never use any form of contraceptive (Nyarko, 2020). Moreover, studies have found that over half (58%) of all births to Ghanaian women aged 15–19 and one-third of births to those aged 20–24 were unintended, which reinstates the need to continue dialogue on usage of contraceptives (Ghana Statistical Service [GSS], Ghana Health Service [GHS] and ICF International, 2015; Grindlay et al., 2019).
Some studies have looked at the factors that influence the intention of contraceptive use after childbirth within the Maternal Care Health services context in Ghana (Appiah et al., 2020; Yaya et al., 2019). A recent study conducted in Ghana showed that counseling on family planning during antenatal clinics increases the intention of contraceptive use in the future (Wuni et al., 2017). Quite admittedly, well-documented knowledge about the risk and protective factors associated with the intent for contraceptive use among women of reproductive age in Ghana is limited. It is important to consider both risk factors, which predicts likelihood of non-intention, and factors that reduce the risk of non-intention of use. This study examines the factors influencing the intent for contraceptive use among women of reproductive age in Ghana and estimates those that are risk and those that protective. The findings of this study have considerable implications for the provision of universal access to sexual and reproductive healthcare services in Ghana. Thus, it provides a clear understanding of the risk and protective factors associated with the intent for using contraceptives, which is crucial in prioritizing groups in family planning programs to increase contraceptive use prevalence in the country.
Methods
The data for the study was obtained from the women’s files from the 2014 Ghana Demographic and Health Survey. The Demographic and Health Survey (DHS) captures data on various aspects of women’s health and wellbeing, including issues of interpersonal violence. The survey is a nationally representative study, with a representative sample of 9396 women aged 15–49. The 2014 GDHS was conducted using an updated frame from the 2010 Population and Housing Census, which was prepared by the Ghana Statistical Service (GSS). The current sub-sample included 7661 women, who reported being sexually active in the last 12 months.
Outcome variable
Lifetime report intent to use contraception use was coded dichotomously based on the contraception and intention of use query. Report of no intention of use was coded 1 based on “Does not intend to use,” and 0 for other responses.
Covariates
Covariates include wealth, educational attainment, religion, marital status, employment status, age, and psychosocial factors were included in the models. Wealth was coded based on the wealth index score with “poor,” and “poorest” dummy coded as “low income,” “rich” and “richest” as “higher income,” and middle as the referent group. Educational attainment was based on highest level of education as reported by the participant, including no education, primary, secondary (referent), and higher. Religion was dummy coded as “Catholic,” “Islam,” “Other Christian,” “Pentecostal/charismatic” (referent), and “Presbyterian.” Marital status was coded binary with “not married” coded 1, while all other responses coded 0. Currently employed, and currently pregnant were also included in the model and coded binary. Age category was included in the descriptive table, and also included in the model as a continuous variable. Psychosocial variables were also included in the model including following constructs: Reason for not using contraceptive: husband/partner opposed, postpartum amenorrheic, and beating justified if wife refuses to have sex with husband. Reason for not using contraception: husband/partner opposed was coded binary, with 1 representing yes, and 0 representing no. Postpartum amenorrheic, and beating justified if wife refuses to have sex with husband were also coded binary, with 1 representing yes and 0 representing no.
Analysis
All coding was conducted in SAS, with analyses conducted in Stata Version 14 (StataCorp LP, College Station, TX). First, chi-square tests were conducted to determine if there were significant differences for alcohol and all covariates between those who reported intention of use versus no intention of use. In the final step, logistic regression was used to assess whether a broad range of risk and protection factors were associated with the outcome variable, intention of contraception use.
Ethics approval
All study participants gave oral and written consent. Ethical approval was given by individual national institutional review boards and by ICF International institutional review board. Permission to use these data were requested from Measure DHD, and publicly available at www.measuredhs.org.
Results
Table 1 shows descriptive statistics for the sample, and chi-square test of differences by intention of use. Overall, (n = 3661) 47.8% of participants reported no intention of use. Educational attainment (χ2 = 33.57; p < 0.001), religion (χ2 = 32.13; p = 0.01), marital status (χ2 = 50.19; p < 0.001), age category (χ2 = 508.51; p < 0.001), pregnancy status (χ2 = 18.93; p < 0.001), and employment status (χ2 = 9.12; p = 0.003) were all reported as significantly different between intention of use of use status. Wealth index was not reported as significantly different between intention of use and no intention of use.
Descriptive characteristics of sample by intention of contraception use (N = 7661).

Percentage with each category.
Chi-square tests of differences between intention of use status.
p < 0.01. ***p < 0.001.
In Table 2, we used logistic regression to examine the association between independent variables with the outcome variable of intention of use. We found that no formal education (OR = 1.49; 95% CI, 1.29–1.72; p < 0.001), and highest level of education of primary school (OR = 1.19; 95% CI, 1.04–1.25; p < 0.001) were positively associated with no intention of use. Islam religion (OR = 0.73; 95% CI, 0.59–0.90; p < 0.001), not currently employed (OR = 1.50; 95% CI, 1.34–1.69; p < 0.001), currently pregnant (OR = 1.30; 95% CI, 1.09–1.54; p < 0.001), and husband opposing contraception use (OR = 2.19; 95% CI, 1.42–3.46; p < 0.001) were also positively associated with no intention of use.
Logistic regression analyses predicting no intention of contraception use.
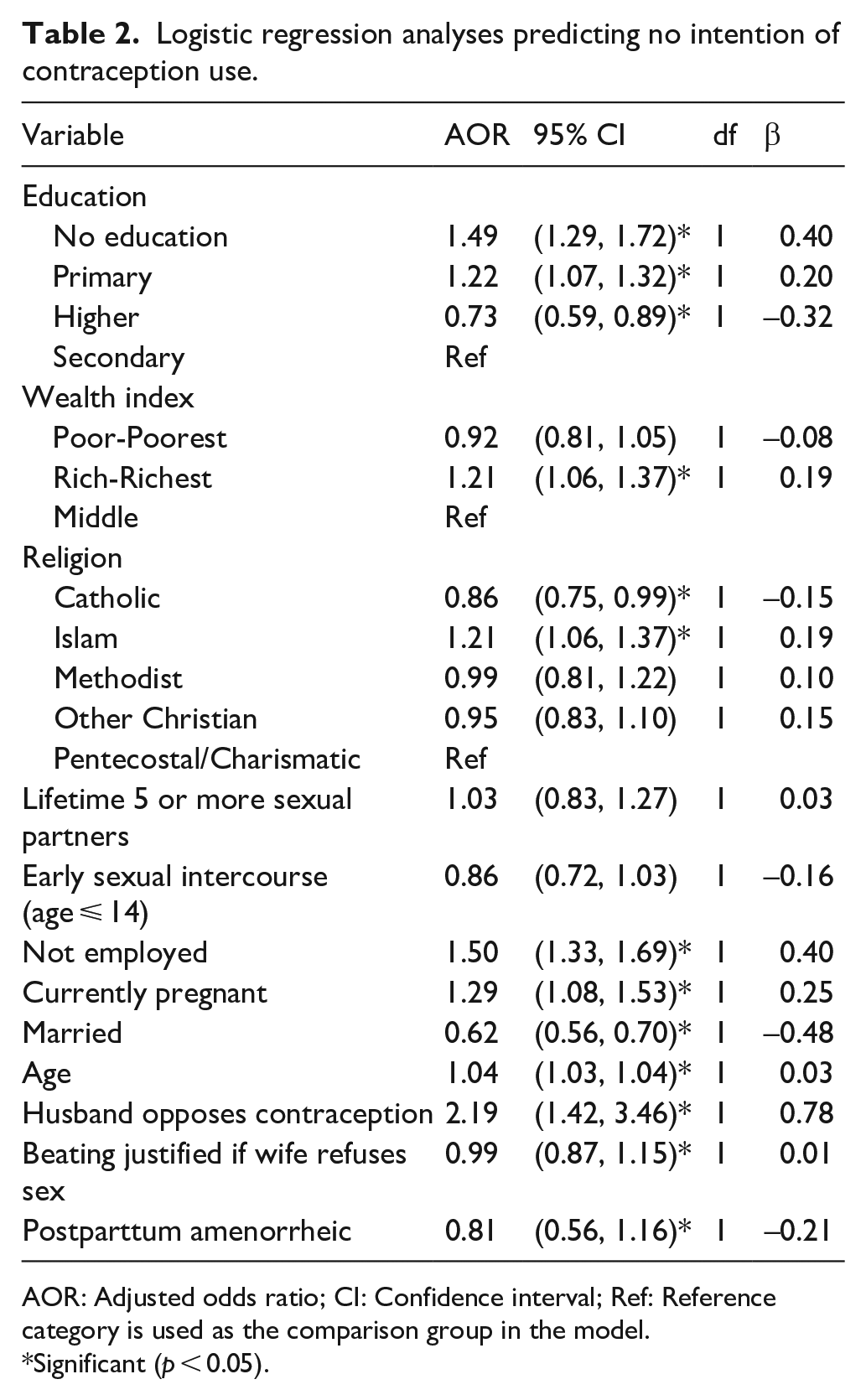
AOR: Adjusted odds ratio; CI: Confidence interval; Ref: Reference category is used as the comparison group in the model.
Significant (p < 0.05).
Endorsing higher education was protective and associated with significantly reduced odds (OR = 0.73; 95% CI, 0.59–0.90; p < 0.001) and Catholic religion (OR = 0.86; 95% CI, 0.75–0.99; p < 0.001), and currently married (OR = 0.62; 95% CI, 0.56–0.70; p < 0.001) were also protective factors, and thus associated with a reduced odds of non-intention of use.
Discussion
Low adoption of contraception use is an ongoing global health concern, that has disproportionally effects women in Ghana. This study examines factors that contribute to future intention of use. The prevalence of intention to use contraception amongst Ghanaian women in this study is higher than expected. After excluding women who had not been active within the past year, 52.2% of the women surveyed indicated current or future intention of contraceptive use by any method. The aim of the current study was to examine factors that contribute to no intention of use, which account for the 47.8% of sexually active women in the study. No formal education and lower educational attainment (primary school as the highest level) were positively associated with non-intention to use contraceptives. Also, religious affiliation such as Islam religion and marital status (unmarried) were positively associated with non-intention to use contraceptives.
Of the total number of women who intend to use contraceptives in this study, most were in their twenties, with 20.7% aged 20 to 24 years, and 20.8% aged 25 to 29. Although this is partly due to having a younger study population, women in their twenties also showed the greatest intention of contraceptive use. Sexually active women in these younger age groups were about 15% more likely to use or consider future use of contraceptives (64.4% prevalence for ages 20–24; and 65.6% prevalence for ages 25–29) than women aged 35–39 (51.9% prevalence). These findings could potentially be attributed to the concerns younger women may have about their likelihood of pregnancy and desire to space their pregnancies. Given that higher education and employment are also protective factors in our study, it is possible that a focus on higher education and career advancement by women in their twenties, prior to reaching greater financial stability, is a partial contributor to the high intention to use contraceptives at these ages. Older women may believe their likelihood of unintended pregnancy is lower, and may also be more socially or financially secure should another pregnancy occur, thus they may have less interest in contraceptive use. The results obtained for women aged 20 to 39 are consistent with those from a similar study conducted on contraceptive use in Ghanaian women, where the prevalence of intention to use contraceptives at these ages was approximately 50% for current use, and 75% for future use (Wuni et al., 2017).
Interestingly, being currently married was a protective factor for current and future contraceptive use. This is surprising given that all women had been active within the last year, and active unmarried respondents were more likely (45%) to currently use contraception than married women (27%) (GSS, GHS and ICF International, 2015) included women with future intent to use contraceptives, which may have increased the number of married women who intend to use contraception. The greater number of unmarried women indicating non-intention is primarily due to the survey respondents who were widowed, divorced, or never married, and may be active infrequently; whereas current or future interest in contraceptives was higher in those who lived with their partner but were not married, as well as those who were separated.
Only 41% of women aged 15–19 indicated intention to use contraceptives. Considering that 39% of the 20–24 year age cohort in Ghana had their first birth by the age of 20 (GSS, GHS and ICF International, 2015) substantial portion of these women may be in the early stages of family building, and thus disinterested in current contraceptive use. The lack of future intent to use contraception by this age group was unexpected, and conflicts with findings by Wuni et al. (2017) that show mothers of similar age in Ghana to have a high future intention of contraception use (88%). Because teenage women are less likely to be married, the lower interest in contraceptive use is probably a contributor to our finding of current marriage status as protective.
Educational attainment plays an important role in a woman’s intention to use contraception. Consistent with existing studies, we found that lower educational levels were positively associated with non-intention to use contraceptives (Adanikin et al., 2013; Sileo et al., 2015). Women who had no formal education or had primary school as their highest form of education indicated no interest in utilizing contraception as opposed to women with higher levels of educational attainment. This underscores the need for government and health care policies that efficiently provide women with accurate knowledge of family planning options regardless of their socioeconomic status. Counseling sessions and antenatal services cannot be overemphasized, especially in Africa where there exists a high rate of infant and maternal mortality. There is also a need for the government and health sector to form partnerships with non-governmental organizations that actively promote safe reproductive health for women.
As mentioned by Beson et al. (2018), education at primary and secondary school levels can also focus on fostering positive attitudes towards contraceptives, correcting misinformation, and empowering women against non-liberal religious beliefs. Empowerment of women in general is an important component of reducing unintended conception, as evidenced by modern contraceptive use being positively associated with women’s ability to participate in decision making with her partner, and negatively associated with women’s justification of reasons for wife-beating (Ghana Statistical Service, 2014). In rural Ghana, teenage childbearing is higher (17%) than in urban areas (12%), and rural women on average have shorter birth intervals and lower empowerment indices (Baiden et al., 2016). The common use of covert birth control (using contraception without a partner’s knowledge) in Ghana also indicates the existence of different partner beliefs regarding family size and contraception (Baiden et al., 2016) suggesting that positive messages about contraception and family planning might be more effective when directed towards both males and females.
Religion also has a powerful influence on decisions related to family planning. A 2018 study in the Greater Accra Area found that use of modern contraception was predicted by one’s religious beliefs, with those who factored in their religious beliefs when deciding to use contraception being less likely to use modern contraceptives (Beson et al., 2018). In our study, we found that Islam religion was positively associated (OR= 1.20, 1.05–1.37) with non-intention to use contraceptives. Studies of American Muslim women and their contraceptive usage indicate that their unwillingness to effectively utilize contraception is multi-faceted and ranged from modesty, gender preference in healthcare providers, and misconceptions regarding illnesses attributed to the use of contraceptives (Budhwani et al., 2018). The Ghanaian Islamic woman’s non-intention to use contraceptives may not be far from reasons cited for that of American Islamic women. Other studies in Africa (Abdi et al., 2020) and worldwide noted many potential causes of decreased contraception use in some Muslim communities. This includes misinterpretations of Islamic teachings on whether contraception is allowed, cultural preference for boys and large family sizes, beliefs that contraceptive use indicated infidelity or could lead to infertility, and the belief that sexual education may promote promiscuity(Alomair et al., 2020). Islamic and Traditionalist women in Ghana are more likely than other religious groups to use contraceptives covertly than non-covertly, and to voice concern over dire consequences if their contraception use is not kept confidential (Baiden et al., 2016). Thus, health care practitioners should actively engage and educate their patients, correct misguided concerns about contraception use, and offer a variety of contraceptive options discreetly and confidentially. In addition, it is essential that religious leaders are involved in advocating for contraceptive use in women, because of the impact religion has on family planning choices and reverence for religious leaders.
Limitations
A key limitation of this study is that our sample may have different family planning goals, and thus did not focus on drivers of non-intention in women who have the greatest need for contraception, those who do not wish to become pregnant soon. Understanding why sexually active women who wish to delay pregnancy choose to forego contraception, and identifying high risk sociodemographic and geographic populations, will help to direct educational and other resources to those with unmet family planning needs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.