
Abstract
High prevalence rates for depression, anxiety, and gastrointestinal (GI) symptoms are found in emerging adults. However, the consequences of mood, anxiety, and GI health on health-related quality of life (HRQOL) are not well established. The biopsychosocial model and the gut-brain axis (GBA) explains the interactions of these psychological phenomenon on social and biological functioning. Following this theoretical framework, it was hypothesized that pathways between depression, anxiety, and HRQOL would be mediated by GI health. Data was cross-sectional. Undergraduates in psychology courses (N = 956) were recruited for course credit as part of ongoing research monitoring physical and psychological health of students at a major southeastern university. Participants were between 18 and 25 years old and measures were administered online. Pathways between depression, anxiety, and HRQOL were investigated using SEM analysis. The SEM was tested and specified for mediating effects. A well-fitting latent variable of GI health was created from the PROMIS-GI® scales, advancing its utility. The mediation model demonstrated anxiety and depression have significant consequences for HRQOL in emerging adults. Direct pathways from GAD7 and PHQ9 scores were found between Physical and Mental HRQOL. Notably, the path from anxiety to Physical HRQOL was fully mediated by GI health. The direct path from depressive symptoms to Physical and Mental HRQOL was partially mediated by GI health, and anxiety to Mental HRQOL was partially mediated by GI health. Findings were consistent with the biopsychosocial model and GBA. The mediation model tested here has treatment and conceptual implications. Individuals presenting with anxiety or depression should be assessed for GI symptoms and conversely, those presenting with GI complaints should be evaluated for anxiety and depression. Research is needed to develop a scoring approach to combine the PROMIS-GI® scales, so the latent construct of GI health may be used in related applications.
Introduction
Many studies have found high rates of anxiety and depression in functional GI disorders (FGID) and conversely, patients with GI disorders may present with clinical levels of anxiety, depressive symptoms, and overall stress (Kessing et al., 2015; Lydiard, 2001; Norton et al., 1999; Solmaz et al., 2003). A recent study (Almario et al., 2018) investigated 12,419 emerging adults and found that reported GI symptoms were prevalent in this specific population. In the study, 54.6% of the sample endorsed ⩾1 or more GI symptom in the past week, as measured by the NIH PROMIS-GI scales (Almario et al., 2018). Gastrointestinal complaints in the emerging adult populations are also associated with higher levels of perceived stress and reactivity, negative coping, anxiety sensitivity, and more health-care utilization (Lee et al., 2011; Norton et al., 1999; Suarez et al., 2010). In a community based study, the association of impairments in health-related quality of life (HRQOL), irritable bowel syndrome (IBS), and indigestion could be explained by psychological functioning (Trivedi and Keefer, 2015). Research also suggests than fewer than 50% of individuals with IBS seek treatment, and those that do, have high rates (ranging from 50% to 90%) of anxiety and mood disorders. Anxiety disorders, especially Generalized Anxiety Disorder, also have a greater impact on comorbidity, outcomes and risk of IBS compared to depression. As such, GI health may serve as a potential mechanistic route in which these relationships could be occurring, as it has a significant association with anxiety, depression, and HRQOL (Bischoff, 2011; Foster and McVey Neufeld, 2013; Halder et al., 2004; Shah et al., 2014; Trivedi and Keefer, 2015).
Health-Related Quality of Life (HRQOL) is a multi-dimensional construct including physical, emotional, and social functioning, as measured by an individual’s self-appraisal of these domains. Several studies have demonstrated that depressive and anxiety-related disorders can lead to substantial impairments in these domains, and at its most extreme cases, consequences may include suicide (Hansson, 2002; Hedegaard et al., 2018; Hohls et al., 2019; IsHak et al., 2011; Zhou et al., 2017). Specifically, in emerging adults, the National Institute of Health (2016; Harvard Medical School, 2007) indicates that the prevalence of major depressive episodes is the highest, 10.9%, among individuals in emerging adulthood as compared with other age groups (SAMHSA, 2016). According to Mojtabai et al. (2016), 12-month major depressive episodes in young adults has increased from 8.8% to 9.6% over a ten-year period (Mojtabai et al., 2016). Furthermore, the National Institute of Mental Health (2017; Harvard Medical School, 2007) and results of the National Comorbidity Study Replication (NCS-R) by Harvard Medical School reported that anxiety disorder prevalence during the past year was 22.3% for individuals ages 18–29, and those between the age of 18–25 experienced the highest prevalence rate for any mental illness, as described by emotional, behavioral, or mental disorders (Kessler et al., 2005; Mojtabai et al., 2016; SAMHSA, 2016).
The biopsychosocial model offers a framework for our understanding of the interconnected relationship between biological functioning (i.e. GI health), social, and psychosocial processes. The biopsychosocial model posits that biological and psychosocial systems interact in the expression of illness and diseases at multiple levels. These systems will determine the presence, severity, and duration of somatic experiences and are an important component of an individual’s subjective experience of their overall HRQOL (Borrell-Carrió et al., 2004; Engel, 1977; Van Oudenhove et al., 2016). As such, biopsychosocial research has evolved to encompass a multidisciplinary approach to wellness, to include questionnaires to assess for psychosocial domains such as HRQOL, to measure patient’s perceptions and behaviors, and to include these psychosocial assessments as standard of care in healthcare settings. Thus, it is crucial to include multivariate statistical methods to investigate these interacting biopsychosocial variables in emerging research (Borrell-Carrió et al., 2004; Drossman and Hasler, 2016; Engel, 1977). The gut-brain axis (GBA) or gut-brain connection provides a model for the association between GI function and psychological distress. The gut-brain axis (GBA) is a complex model which describes the different channels of communication between the central and the enteric nervous system and provides an explanation why psychological factors can alter GI functioning and vice versa. The GBA provides links between emotional and cognitive centers of the brain and GI functions (Carabotti et al., 2015). Taken together, the biopsychosocial model and the GBA provides the theoretical underpinnings of how psychological stress and cognitive-affective processes are potential risk factors for the experience of GI symptoms in emerging adults (Drossman et al., 2002; Van Oudenhove et al., 2016). Up until the present study, GI health is commonly assessed by specific symptoms or symptom groupings. No underlying construct of GI health has been created.
The purpose of this study is not only theoretical, but it also has practical implications for assessment and treatment. While the present study does not include direct measures of GI system activity through physiological tests, self-report measures of functioning in these systems should correspond to GBA endpoints. There are well established self-report measures available for the depression, anxiety, and HRQOL endpoints. The NIH PROMIS-GI® scales measure various self-reported GI symptoms. However, no method has been proposed to combine them into a construct of GI health until now. Each of the measures used in the present study are in the public domain and thus available to student health and primary healthcare settings.
Hypotheses
The primary variables of interest in this study were depressive and anxiety symptomatology as measured with the Patient Health Questionnaire (PHQ-9) and the Generalized Anxiety Disorder 7-item (GAD-7) scale. HRQOL was measured with the 36-Item Short Form Health Survey (SF-36), and GI Health was measured with the PROMIS-GI® symptom scales. It was hypothesized that anxiety and depression would predict HRQOL outcomes, and this relationship would be mediated by GI Health.
Method
Participants
Data was cross-sectional. Undergraduates in psychology courses (N = 956) were recruited for course credit as part of ongoing research monitoring physical and psychological health of students at a major southeastern university. Introductory psychology is a required course for all majors at this university. Eligibility criteria excluded vulnerable populations and required participants to be between the age of 18 and 25 years and able to complete an online questionnaire in the English language. All measures were administered online. This study was approved by the Institutional Review Board.
Participants were between the age range of 18 and 25 (M = 18.97, SD = 1.47) with 58.3% identifying as female, and 57.3% identifying as Caucasian, 1.00% American Indian or other Native American, 9.6% Asian or Pacific Islander, 11.90% Black or African American, 1.5% Mexican-American, 5.30% Puerto Rican, 11.3% Other Hispanic, and 2.00% identified as Other. Research participants were undergraduates in their freshman (n = 594), sophomores (n = 173), juniors (n = 115), and seniors (n = 72). Only one research participant identified themselves as a graduate student in the research sample (n = 1) and one identified themselves as an “unclassified” student (n = 1).
Measures
PHQ-9
The Patient Health Questionnaire (PHQ-9) is a nine-item, self-report scale utilized to screen for depressive symptoms over the past 2 weeks (Kroenke and Spitzer, 2002). Participants rate each item on a four-point Likert scale ranging from 0 (not at all) to 3 (nearly every day). The PHQ-9 has demonstrated good internal consistency, test-retest reliability, criterion validity, and construct validity across diverse racial ethnic groups, college populations, and primary care studies in previous psychometric studies (Eisenberg et al., 2011; Huang et al., 2006; Kroenke and Spitzer, 2002). We conducted reliability analysis and the PHQ-9 indicated good reliability (α = 0.88).
GAD-7
The Generalized Anxiety Disorder 7-item (GAD-7) scale is utilized to assess for cognitive symptoms of anxiety (Spitzer et al., 2006). Each item asks participants to indicate the frequency with which they have experienced a symptom during the past 2 weeks on a four-point Likert scale ranging from 0 (not at all) to 3 (nearly every day). Research has indicated the internal consistency of the GAD-7 is excellent (α = 0.92), and the test-retest reliability is good (Spitzer et al., 2006). We conducted reliability analysis and the GAD-7 indicated excellent reliability (α = 0.92).
SF-36
In this study, health-related quality of life was measured using the 36-Item Short Form Health Survey (SF-36) developed to assess medical outcomes (Hays and Morales, 2001). This measure includes eight subscales: physical functioning, emotional well-being, role limitations due to personal or emotional problems, role limitations due to physical health problems, social functioning, energy/fatigue, bodily pain, and general health perceptions (Ware and Sherbourne, 1992). We conducted reliability analysis for the SF-36 scales. The scales indicated good to excellent reliability. They are as follows: Physical Functioning (α = 0.91), Role limitations due to Physical Health (α = 0.80), Role limitations due to Emotional Problems (α = 0.73), Energy/Fatigue (α = 0.74), Emotional Wellbeing (α = 0.82), Social Functioning (α = 0.81), Pain (α = 0.76), and General Health (α = 0.70). These scales were combined into mental health and physical health latent constructs. The physical health component was computed from four subscales: physical functioning, role functioning due to physical problems, bodily pain, and general health perceptions. The mental health component was computed from four subscales: role limitations due to emotional problems, emotional well-being social functioning, and energy (Cunningham et al., 2003; Farivar et al., 2007; Lins and Carvalho, 2016; Ware and Sherbourne, 1992). The physical health component summary score will be referred to as “Physical HRQOL” and the mental health component summary score will be referred to as “Mental HRQOL” in our results.
PROMIS-GI®
The National Institute of Health has developed the Patient-Reported Outcomes Measurement Information System (PROMIS). The PROMIS is a standardized set of patient-reported outcomes that assess for multiple domains of health, including physical, psychological, and social health. The PROMIS-GI® was developed to assess specific GI symptoms such as gas and bloating, reflux, constipation, diarrhea, nausea, and belly pain separately (Spiegel et al., 2014). Research has indicated the symptom scales demonstrate good construct validity in the general population and diverse gastrointestinal patients. These symptom scales have been developed to be used for both clinical practice and research. Health Measures has collected extensive normative reference data and scale information. Scale reliability is high for each of the symptom scales. Internal reliability are as follows: abdominal pain (α = 0.87), gas/bloating (α = 0.94), diarrhea (α = 0.88), constipation (α = 0.89), gastroesophageal reflux (α = 0.88), and nausea/vomiting (α = 0.76) (Spiegel et al., 2014). As recommended by the authors, the present study used the recommended T-scores for analyses (Broderick et al., 2013; Spiegel et al., 2014). No method for combining scales into a general measure of GI health has been previously proposed.
Statistical analyses
Data was reviewed prior to analyses to eliminate respondents with inconsistent responding, missing data, and duplicates. Descriptive statistics were conducted using SPSS Version 26. All SEM analyses were conducted using MPlus8 Version 1.6.
Statistical analyses were conducted via SEM measurement and mediation models. All SEM analyses were conducted in MPlus using maximum likelihood estimator with robust standard errors. To test for mediation, the most common methods utilized are the Baron and Kenny Method (Baron and Kenny, 1986) and the Path Model Method (Cheung and Lau, 2008). In the present study, the mediation model was conducted by the SEM model method. A measurement model was utilized to identify latent variables using modification indices to test for model fit. The tracing rule was utilized to examine direct and indirect effects. Finally, an SEM structural model was tested and specified. Paths were added and removed as warranted by indicated modification indices, and bootstrapped total and indirect effects were calculated. This was done by conducting biased-corrected bootstrap confidence intervals from 10,000 bootstrap iterations.
Results
Descriptive statistics
See Table 1 for descriptive and correlation statistics of the primary variables of interest in this study. Results were consistent with the biopsychosocial model and GBA. Overall, the emerging adult sample used here represented a range of functioning in anxiety, depression, and GI symptoms. In respect to anxiety symptomatology, 38.1% of our sample met the clinical cut off for moderate to severe anxiety. Regarding depression, 33% of our sample endorsed mild depression, and 21.2% of our sample reported moderate to severe depressive symptoms levels. Lastly, 25.8% of our sample reported experiencing at least one moderately severe GI symptom such as gas or bloating, or belly pain.
Correlation table and descriptive statistics.

Significant at the 0.01 level. **Significant at the 0.05 level.
Primary analyses: Measurement model
Initially, a measurement model was tested to create a higher-order construct of GI health using the PROMIS-GI® symptom scales. Latent GI health was estimated from six symptom scales to assess for gas and bloating, reflux, constipation, diarrhea, nausea and vomiting and belly pain (Spiegel et al., 2014). The fit indices for the GI health measurement model were: χ2(9) = 67.91, p < 0.001, CFI = 0.96, RMSEA = 0.08, (90% CI 0.07, 0.10), SRMR = 0.03. This model indicated good fit and supports the use of creating a higher-order construct of GI health using the six PROMIS-GI® symptom scales.
Then, a measurement model was tested using all variables of interest. This included anxiety and depression predicting health-related quality of life (HRQOL) and these variables were associated with HRQOL through GI health. The fit indices for this measurement model were χ2 (74) = 393.15, p < 0.001, CFI = 0.92, RMSEA = 0.07, (90% CI 0.06, 0.07), SRMR = 0.05. Then, modification indices were examined, and two correlated error terms were iteratively freed. Specifically, diarrhea with constipation and reflux with belly pain. The final measurement model fit indices were χ2 (72) = 345.81, p < 0.001, CFI = 0.93, RMSEA = 0.06, (90% CI 0.06, 0.07), SRMR = 0.05. Results indicated that the re-estimated model with two correlated errors fit significantly better than the original model without correlated errors. The original measurement model was compared with the final measurement model using Satorra-Bentler Scaled Chi Square test of model fit: Satorra-Bentler Scaled χ2(2) = 43.98, p < 0.001. Additional correlated error terms may have significantly decreased Chi square, however, these lacked theoretical basis or were across latent variables. Thus, they were not freed and remained in the final, revised, measurement model (see Table 2).
Standardized factor loadings for measurement model.
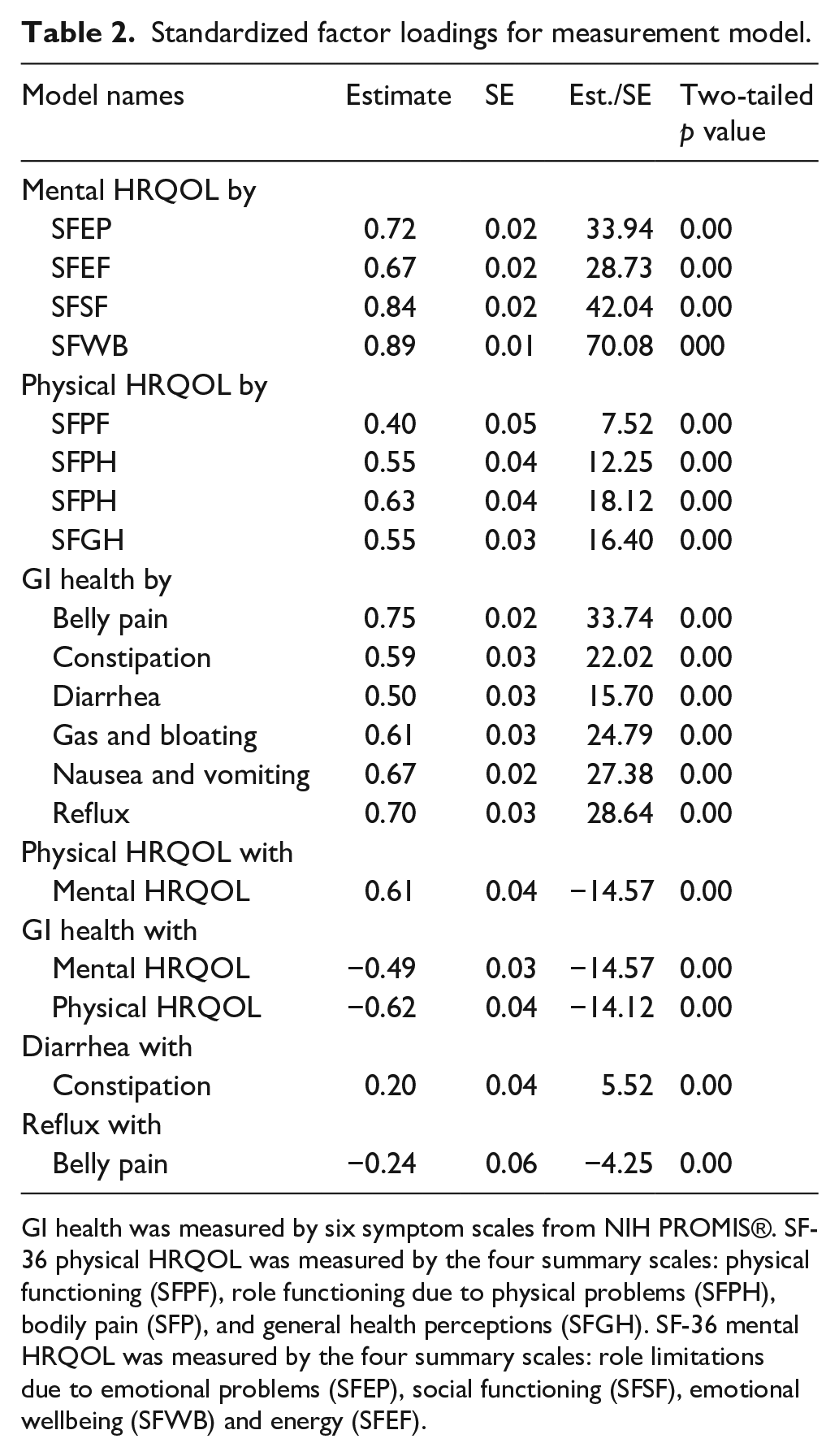
GI health was measured by six symptom scales from NIH PROMIS®. SF-36 physical HRQOL was measured by the four summary scales: physical functioning (SFPF), role functioning due to physical problems (SFPH), bodily pain (SFP), and general health perceptions (SFGH). SF-36 mental HRQOL was measured by the four summary scales: role limitations due to emotional problems (SFEP), social functioning (SFSF), emotional wellbeing (SFWB) and energy (SFEF).
Structural model
Next, the full, structural model was tested and specified with direct and indirect paths consistent with the original hypothesis: a structural model in which the relationship between anxiety and depressive symptoms and HRQOL was fully mediated by GI health. The original model fit statistics were: χ2(94) = 402.65, p < 0.001, CFI = 0.94, RMSEA = 0.06, (90% CI 0.05, 0.07), SRMR = 0.04. Results indicated there were significant direct effects: anxiety symptoms predicting GI health (estimate = 0.27, p < 0.001), depressive symptoms predicting GI health, (estimate = 0.27, p < 0.001), and GI health predicting Physical HRQOL (estimate = –0.49, p < 0.001). GI health also predicted Mental HRQOL (estimate = –0.07, p < 0.01) and depressive symptoms predicted Physical HRQOL (estimate = –0.32, p < 0.001). Consistent with previous research, anxiety symptoms were negatively and significantly associated with Mental HRQOL (estimate = –0.32, p < 0.001), and similarly; depressive symptoms were negatively and significantly associated with Mental HRQOL (estimate = –0.56, p < 0.001).
Next, the model was refined to provide the most parsimonious model by removing one direct path: anxiety symptoms on Physical HRQOL (estimate = 0.03, p = 0.70). The re-estimated, final model fit statistics were: χ2(95) = 401.53, p < 0.001, CFI = 0.94, RMSEA = 0.06, (90% CI 0.05, 0.06), SRMR = 0.04. Removing this path did not significantly change model fit: Satorra-Bentler Scaled χ2(1) = 1.05, p = 0.07.
Then, bootstrapped total and indirect effects were calculated. This was done by conducting biased-corrected bootstrap confidence intervals from 10,000 bootstrap iterations. Results indicated three significant indirect effects. First, an indirect effect from depression to Physical HRQOL and secondly an indirect effect from anxiety to Physical HRQOL by means of GI health. Lastly, results indicated an indirect effect from anxiety to Mental HRQOL via GI health. Most notably, anxiety symptoms to Physical HRQOL was fully mediated by GI health. In addition, results indicated two direct effects. First, a direct effect from depression to Physical HRQOL and a direct effect from anxiety to Mental HRQOL. Thus, depressive symptoms are associated with physical and Mental HRQOL and this relationship is partially mediated by GI health. Further, the impact of anxiety symptoms on Mental HRQOL is partially mediated through GI health (see Table 3 and Figure 1).
Standardized total, total indirect, specific indirect, and direct effects.


Structural equation model.
Discussion
The rising incidence of depression, anxiety, and GI symptoms in emerging adults is having an impact on their HRQOL. The results presented here support that GI health is an important route through which this relationship may be occurring. The emerging adult sample used here represented a range of functioning in anxiety, depression, and GI symptoms. Results indicated the relationship between anxiety symptoms and Physical HRQOL was fully explained by GI health. In addition, results revealed depressive symptoms are strongly associated with Physical HRQOL, although this relationship is partially explained by gastrointestinal health. Similarly, anxiety symptoms to Mental HRQOL is also partially mediated by GI symptoms. This relationship was also found for depressive symptoms to Mental HRQOL via GI symptoms.
The SEM used here demonstrated the significant role of gastrointestinal symptoms as a mediating mechanism in the relationship between anxiety and depressive symptoms and health-related quality of life in the emerging adult population. Further, this model revealed that the relationship between anxiety and physical health quality of life outcomes can be explained by gastrointestinal symptomatology. Consistent with trends presented in the literature, our SEM demonstrated significant pathways consistent with both the biopsychosocial model and gut-brain axis (GBA). Collectively, our study supports the theoretical underpinnings of the biopsychosocial model and the GBA. Our findings are consistent with the theory that psychological stress and cognitive-affective processes are potential risk factors for the experience of GI symptoms in emerging adults. Specifically, the present study revealed that gastrointestinal health, as hypothesized, is a crucial variable in the relationship between mood (anxiety and depression) and its impact on emerging adult’s HRQoL. In other words, gastrointestinal health partially explains why clinicians may see strong consequences between mood and HRQoL in emerging adults. As hypothesized, anxiety had a direct mediational effect, which is supported in previous research that has revealed that anxiety disorders have a greater impact on the risk, comorbidity, and outcome of irritable bowel syndrome (IBS) compared to than depression (Roy-Byrne et al., 2008). Nonetheless, depressive symptoms were also strongly associated with both GI health and HRQOL, as findings revealed a partially mediated effect. This finding partially supported our initial hypothesis. Of note, the application of the biopsychosocial and GBA theory were also supported in a relatively understudied population: emerging adults. Interestingly, these relationships demonstrate how adverse gastrointestinal symptoms and related functional outcomes are relevant across the lifespan. Finally, the model demonstrated significant associations of depressive and anxious symptoms on gastrointestinal health, indicating that increased mood symptoms predicts gastrointestinal symptomatology.
Limitations
There were a few limitations in the present study. This study used cross-sectional data from an undergraduate college sample. This may limit the generalizability of the results, as information was not collected from emerging adults who were presenting for clinical services nor were repeated measures obtained over time. Further research investigating these variables, in a repeated measures design, will provide crucial information about causal relationships and temporal precedence. Variables of significance may include the role of antibiotics, probiotics, changes to diet, and micro-and macro-nutrients as interventions to target gastrointestinal health are potential avenues for future studies. In addition, further research can utilize ecological momentary assessment (Goldstein et al., 2018) or 24-hr recall methods (Subar et al., 2012) to examine daily nutritional and dietary intake and enhance the model presented here.
Conclusion
Of importance, this study’s measurement model found that a latent factor of GI health could be constructed using the NIH PROMIS-GI scales, advancing this instrument’s utility. This model indicated very good model fit. To the author’s knowledge, this study was the first of its kind to create a high-order factor model of GI health using the NIH PROMIS-GI scales. These scales were originally developed to measure the separate symptom domains of functional gastrointestinal disorders (FGID) specified in the Rome IV Diagnostic Criteria (Drossman et al., 2002). The separate scoring and interpretation of these scales is continued to be recommended. There may be additional benefits for developing an effective scoring approach to combining these scales, so that the latent construct of GI health can be further studied. One approach might be to simply average the T-scores of the scales used without weighing them. The standardized factor loadings of the scales range from a low of .55 for diarrhea to a high of .71 for belly pain. This averaging approach may underestimate impairment in individuals with very high T-scores in one symptom area and average scores in the other areas. Ideally, a total GI health index score may need to be formulated by the developers, taking advantage of IRT and CAT methodologies. Taken together, our findings have both treatment and conceptual implications for mood related symptoms and quality of life outcomes in emerging adults. Individuals presenting with anxiety or depression should be assessed for GI symptoms and conversely those presenting with GI complaints should be evaluated for anxiety and depressive symptoms. The Clinical Health Psychologist can provide behavioral and lifestyle interventions or collaborative care referrals with Gastroenterologists and Registered Dietitians.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This article does not contain any studies with animals performed by any of the authors. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Article processing charges were provided in part by the UCF College of Graduate Studies Open Access Publishing Fund.
Informed consent
Informed consent was obtained from all individual participants included in the study. The University’s Institutional Review Board determined the present study to be human subjects research that is exempt from regulation.