
Abstract
The Clinical Interview on the Sense of Grip on Chronic Disease has been administered to 68 mothers of children affected by Hereditary Angioedema (C1-Inh HAE), Type 1 Diabetes (T1D), Juvenile Rheumatoid Arthritis (JRA). The objectives are to detect general features of the experience of parenting children with chronic illness as well as the specificities of this experience related to the different conditions. Four Profiles of Sense of Grip were identified: Adempitive, Controlling, Reactive, Dynamic. The Sense of Grip Interview is an effective clinical tool for understanding the characteristics of the disease in daily life, which can help clinicians to encourage family adjustment to disease.
Keywords
Introduction
The high prevalence of chronic diseases is a key health challenge that Europe and Western countries faces today (Chang et al., 2019) and has become an important challenge for health care systems. The scientific community believe that the widespread increase in the number of people with chronic conditions is due to improvements in health status and extended life expectancy. Furthermore, this phenomenon may also be attributed to improvements in the quality of detection techniques, and the early detection of chronic diseases (Dicker et al., 2018). Healthcare systems are overloaded by the growth of the caring needs due to chronicity. New paradigms of research and intervention are required, aiming at fostering patients’ lay competencies and engagement and their active involvement in their caring needs (Borghi et al., 2016; Busch et al., 2019; Domecq et al., 2014; Forsythe et al., 2016; Freda et al., 2019; Grande et al., 2014; Graffigna and Vegni, 2017).
When the patient is a child, research and clinical interventions must take into account the needs and engagement of both the child and family caregivers (Eccleston, 2015). Caregivers play a crucial role in assisting children to adjust physically and psychologically to chronic pediatric physical disorders (Armstrong et al., 2011; Borghi et al., 2019; Lewandowski and Drotar, 2006; Manna and Boursier, 2018). Developmental psychologists are highlighting how different the patterns of sensemaking can be when achieved through relationships with significant others (Ginot, 2015; Parrello and Giacco, 2014; Tronick, 2009). Parents who are able to recognize their children’s cognitive and affective needs toward their disease can foster children’s adjustment to the disease, by offering them the chance of talking about their emotions and sharing their worries and fears, asking about different issues related to their own disease. Nevertheless parental competence to deal with the disease of the child widely varies according to individual differences and to the characteristics of the disease itself. Moreover, such competences of helping children to deal with the disease can be temporarily impaired by the emotional and cognitive impact of the disease on parents themselves. Feelings of fear, anxiety, uncertainty, delusion, and depression may be overwhelming in several cases. While some studies describe the diagnosis of a chronic illness in childhood as a cataclysmic event (Massie and Massie, 1975) in which parental expectations are shattered (Cohen, 1999), other studies highlight that some parents expressed relief at receiving the diagnosis as it marked a significant turning point in the acceptance process and alleviated feelings of uncertainty (Cipolletta et al., 2015; De Luca Picione et al., 2015; Jerrett and Costello, 1996). Therefore we believe it is highly relevant to address our research and clinical interest to parents’ elaboration of their children’s chronic disease.
The narrative sensemaking of the chronic disease
In our opinion the narrative reconstruction of the Sense of the chronic disease is essential for understanding psychological adjustment to disease, since narrative methods are particularly appropriate for researching experiences through time, such as chronic illness (Bleakley, 2005: 337). Narrative is regarded as a mode of mental functioning and representation, which enables us to create temporal, spatial, relational and agential links between the elements of the experience (Freda, 2008; Freda et al., 2016) performing a constructive and interpretive function (Damasio, 2012; Gazzaniga, 2013). These functions draw on our past experiences and enable us to predict and hypothesize future scenarios (Barrett, 2017; Gazzaniga, 2013) and to conceive creative and innovative solutions (Ungar, 2008). In general terms, the narrative responds to the fundamental human need to experience a feeling of identity and continuity through time by constructing stories, within a specific intersubjective and cultural context (Bruner, 1990; De Luca Picione and Valsiner, 2017; De Luca Picione et al., 2017, 2018; Freda, 2008; Lichtenberg, 1988; Lichtenberg et al., 2017). Narrative constitutes one of the fundamental psychosocial processes for constructing and negotiating the sense of experience especially in conditions of uncertainty (Bruner, 1990).
In light of what the above, disease is a particular abnormal condition that triggers an upheaval in one’s daily routine and a strong sense of uncertainty, loneliness, and exclusion. In order to cope with this experience, narrative processes are activated to restore order (Gazzaniga, 2013) and to seek familiarity (Proulx and Inzlicht, 2012) with the new needs and functional limitations imposed by the disease. When affected by a chronic disease, the person has to learn to cope with the recurrence of the disease for his/her entire life. The narrative processes of constructing one’s identity and relationships are therefore constantly re-elaborating and negotiating the relationship between the disease and the various contexts and life cycles.
In the pediatric context, parental sensemaking processes help children to create an “environment of sense” and nurture their relationship with disease, which in turn enhances the children’s sensemaking capabilities (Dicé et al., 2017, 2020). It is therefore essential to understand the parental narrative sensemaking processes of the disease itself (Boursier et al., 2019). In this study, the parental sensemaking processes of their children’s illness experience are analyzed in light of the general conceptual framework of the Sense of Grip on the Disease (SoGoD).
The conceptual model of Sense of Grip on chronic Disease (SoGoD)
The conceptual model of Sense of Grip on the Disease (SoGoD) refers to the set of sensemaking processes aimed at adjusting to the chronic disease in the everyday life (Freda et al., 2019).
Health Psychology literature highlights the importance of meaning making processes in fostering adjustment, engagement and autonomy in the disease management (Graffigna et al., 2017). The importance of meaning making is related to the hypothesis that a change in patients’ lay theories, cognitions, and beliefs is followed by a change in their behavioral and coping strategies, and their health outcomes. In fact, from a cognitive perspective, meaning making is considered with reference to its outcomes such as health beliefs, illness representation, health literacy (Leventhal et al., 1998).
The conceptual model of SoGoD draws from this recognition of the importance of meaning making but is aimed at focusing on the process of meaning and sensemaking in itself, rather than on its outcomes. By SoGoD we focus on the processes of semiotic connection by which the disease experience is organized. Our aim is to grasp the quality of the processes of narrative connection between the elements of the experience within each domain of the disease experience in terms of integration, evolution, and flexibility (De Luca Picione et al., 2017, 2018; Freda et al., 2019). SoGoD highlights the importance of the individual’s sensemaking processes in adjusting to chronic illness and is aimed at understanding the multidimensional nature of dealing with chronicity. This concept is derived, by an abductive research approach (Salvatore, 2016), from the narrative analysis of lay experts sensemaking of their own norms, lay theories (Joffe, 2002) and strategies on chronic illness and its daily management. In a previous study, we came to the definition of SoGoD through a conceptual synthesis of a narrative analysis carried out on a corpus of interviews administered to the parents of children affected by a specific chronic disease, Hereditary Angioedema due to C1 inhibitor deficiency (Freda et al., 2019; Savarese, 2018).
The keywords of this definition are the terms “grip” and “sense.” With the term “grip” we intend to refer to the competence of mastering and acquiring specific skills, characterized by different degrees of flexibility and fit to the contingent situations of the daily disease experience. With the term “sense” we refer to the centrality of sensemaking, in its narrative matrix, in determining the processes of psychological, social, and agentive adjustment to chronic disease (De Luca Picione et al., 2017, 2018; Freda, 2008).
The SoGoD refers to the dynamic process of dealing with chronic illness in everyday life, both in its continuity dimensions given by the chronicity of health conditions, and in its aspects of variability and transformation due to different events, contexts, and evolutionary changes. This process is articulated in a broad tension to generate resources of sense useful for comprehending the relationship between the requirements and constraints imposed by illness, personal needs and desires and the contexts of daily life. The more complex and pluralist are such narrative connections and apt at bearing the intrinsic variability of the experience, the more effective will be SoGoD. A well-organized SoGoD expresses in the competence to construct narrative connections of the disease experience between coherence and flexibility (Savarese, 2018).
SoGoD must be framed within the specific domain of chronic disease, through a binocular vertex aimed at capturing the transversal elements of the experience of chronic illness and at understanding the specifics of each pathological condition. It is now evident that chronic is not synonymous with static: the course of the disease over time is not homogeneous and inevitably merges with the maturation and development processes of the person and his/her sense of belonging and interaction (Crittenden and Landini, 2011). More specifically, SoGoD identifies three specific domains of daily life that characterize the experience of chronic illness within the family: the domain of interpretation, regarding how to elaborate explanatory hypotheses of the disease and how it affects personal life, the domain of communication, concerning the various ways in which the disease is named, expressed, communicated during the dialogues between parents and children, and the domain of management, pertinent to the various ways of constructing meaningful praxis of behavior, actions, and strategies to mediate between the needs of the disease, the family system and the various steps of the child’s development.
In the light of these considerations, the aim of this article is to explore the everyday experience of chronic illness for three different chronic conditions: hereditary angioedema, Type 1 Diabetes and Juvenile Rheumatoid Arthritis, from the perspective of parental SoGoD on their child’s illness. The chronic illness experience is explored with the clinical interview on Parental SoGoD on the Disease (SoGoD-P) (Freda et al., 2019) from a dual perspective: on the one hand, examining the general issues of the pediatric chronic illness experience; on the other hand, comprehending the specifics of the experience of each condition.
The research context
In this research we collected interviews form three different context of chronic disease: Hereditary Angioedema, Type 1 Diabetes, and Rheumatoid Arthritis. We choose these disease conditions within a local collaboration with the Department of Pediatrics of Federico II University Hospital of Naples, Italy, aiming at comparing three diseases with the common feature of chronicity and with different characteristics. HAE was our first research group due to a long-standing research collaboration with the and Center for Basic and Clinical Immunology Research (CISI), University of Naples Federico II; T1D was selected due to the wide diffusion of this condition—which makes it different from the rarity of HAE—and for the consolidated scientific knowledge of its pathophysiological mechanisms; JRA was selected due to the wide area of uncertainty and lack of knowledge of the pathophysiological mechanisms. The main characteristics of these diseases are listed below.
Hereditary Angioedema (HAE). HAE is a rare autosomal dominant disease caused by a deficiency in complement C1 inhibitor, which induces swelling of the skin and mucosal tissue that may vary greatly in terms of localization, frequency, and intensity both within and between individuals (Kemp and Craig, 2009; Zotter et al., 2014). Swelling can occur in various parts of the body, including the arms, legs, face, abdominal mucosal tissues, and laryngeal mucosal tissues. Of these, laryngeal attacks are potentially life threatening because of the risk of asphyxiation. Above all other aspects, the issue of uncertainty, which is intrinsic to the HAE experience is often considered more distressing than the impact of physical symptoms (Bova et al., 2018; Bygum et al., 2015; Freda et al., 2016; Lumry et al., 2013). Uncertainty can make it difficult to schedule one’s daily activities without fearing an attack, especially when planning a trip where emergency treatment is unavailable; consequently, patients can be left in fear that any physical or emotional stress could harm the body (Savarese et al., 2017, 2018).
Type 1 Diabetes (T1D). The incidence of childhood onset diabetes is increasing in many countries, with an overall annual increase estimated at around 3% (Paterson, 2003). The cause of T1D remains unknown even if there is growing evidence linking diabetes with a genetic predisposition and that environmental factors can trigger an autoimmune destruction of the beta cells leading to absolute dependence on insulin treatment. Living with T1D remains a challenge for the child and his/her family even in countries where medical care is easily accessible. Poor metabolic control may result in acute complications such as hypoglycemia and ketoacidosis, poor growth and chronic microvascular and macrovascular complications. Episodes of severe hypoglycemia or ketoacidosis, especially in young children, are risk factors for structural brain abnormalities and impaired cognitive function which may cause schooling difficulties and limit future career choices (Ferguson et al., 2005). Moreover the prospects of future long-term complications can psychologically affect children with diabetes, especially in their teens (Persson et al., 2013).
Juvenile Rheumathoid Arthritis (JRA). JRA is one of the five most common classes of chronic pediatric diseases (Cassidy and Nelson, 1988). JRAs are characterized by unpredictable flares during which children may experience an abrupt exacerbation of symptoms such as joint swelling, pain and limitation of movement. Traditional treatment plans are aimed at reducing inflammation, maintaining joint function, and preventing deformities (Sandstrom and Schanberg, 2004). Research shows that both youths and their parents are at increased risk for psychosocial adjustment difficulties, general distress, and depression (LeBovidge et al., 2003).
Methods
In this study we used a mixed method research based on the analysis of narratives collected through the ad hoc clinical interview. The transcriptions of the interviews were analyzed using an ad hoc grid validated in a previous study in which we employed a semiotic-narrative analysis methodology of the sensemaking processes (Freda et al., 2019). The results of the qualitative coding of the interviews were subsequently transposed into a codebook. The obtained data were then analyzed using the TwoStep cluster analysis to find homogenous trajectory of the sensemaking processes across the three specific domains (interpretation, communication and management) of the chronic disease experience in daily life.
Participants
N. 68 mothers of young people aged 6 to 17 suffering from HAE (n = 28), T1D (n = 21) and JRA (n = 19) were selected by a purposive sampling and agreed to participate in the study. The response rate was 85%. The study protocol was approved by the Ethics Committee of the University Hospital Federico II (Protocol n.118/16). All procedures performed in this study were in accordance with the ethical standards of the study coordinating center and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Prior to study participation, patients and their parents signed an informed consent document.
Rationale for the participants’ selection. Only mothers of children in school age were recruited without differences between age ranges. Age ranges have been taken into account during the analytic process, when evaluating of the appropriateness of the dialogue between parent and children according to their cognitive and affective needs.
We enrolled only mother who received the diagnosis at least 1 year before the interview trying not to interfere with the initial elaboration of the diagnosis. A period of 1 year on average is also indicated as ethically admitted in such research contexts (see Marvin and Pianta, 1996) .
Exclusion criteria:
- Mothers of young persons under the age of 6 or over the age of 17;
- Reception from diagnosis for a period of less than 12 months;
- Conditions of psychopathological risk or child psychopathology (assessed with the Child behaviour Check-list (CBCL, Achenbach and Rescorla, 2001)
Tools
The Clinical Interview on The Parental Sense of Grip—SoGoD(P)—on chronic disease (Freda et al., 2019) is a clinical interview aimed at understanding the characteristics of the sensemaking processes related to the domains of interpretation, dialogical processes, and disease management discussed in the previous paragraph. The questions were constructed with the aim of obtaining diachronic narratives of the disease experience, by evoking both the semantic memory (e.g.: “What are the key elements required for managing Hereditary Angioedema in your daily life?”) and the episodic memory (e.g.: “Can you tell me about one of your most recent distressing HAE episodes?”) for each of the areas under study. The current version of the interview includes 11 questions and was built and modified during the first validation study (Freda et al., 2019).
The coding grid
For the analysis of the interview corpus, we used an ad hoc grid that was developed in a previous study (Freda et al., 2019) based on a semiotic-narrative methodology aimed at grasping which sensemaking processes are implemented while facing with the issues of chronicity. The analysis of these elements enabled us to identify a series of “sensemaking modalities” (SM) for each domain of the interview. By the terms “sensemaking modalities”(SM), we refer to the product of the semiotic narrative analysis which is aimed at detecting the logics of the narrative construction of the links between the elements of the experience, as well as to the general purpose and objectives to which the narration, in its agentive function, responds (Baldwin, 2009; De Luca Picione et al., 2019; Proulx and Inzlicht, 2012). Therefore, analytical attention was not only paid to the semantic contents of the narration (the “what” the narrator deals with), but also to the characteristics of the links that orient the points of connection between the elements of the experience within each domain (the “how” the narrator presents and articulates her story). Below we give a description of the analytic level together with a narrative excerpt as an example:
(a) The connection among events, for the domain of the interpretation of the disease variability;
e.g. narrative excerpt: Mother: “. . .attacks don’t always occur for the same reason, I try to ask my son what happened before the attack, if he bumped into something, if he was nervous .. . . It seems that when he has the flu it happens more frequently, we made this association, that’s probably how it goes. . .” (Int. n. 3, p. 4, lines 13–16. Sensemaking modality: hypothetical—A.2, see Table 1)
The coding grid of the clinical interview on the sense of grip on the disease-SoGoD.

(b) The connection between self and other, for the domain of the dialogue;
e.g. narrative excerpt: Mother: “. . .no, I prefer not to talk about it . . .I don’t want to make him feel bad. . .he already has to live with all this. . .” Int. n. 20, p. 3, lines 74–76. Sensemaking modality: alarmistic—B.2, see Table 1).
(c) The connection among sensemaking and actions, for the domain of the management of the disease;
e.g. narrative excerpt: Mother: “I try not to limit her freedom. When she asks me to practice a sport we try to do the one that best fits for her, for example she wanted to do modern dance and I suggested she opt for a musical because it's still fun, but requires less effort. . .” (Int. n. 10, p. 7, lines 191–193. Sensemaking modality: flexible—C.3, see Table 1).
These modalities are coded as mutually exclusive and give an account of the articulation of the parenting sensemaking processes (Freda et al., 2019). Three SM were identified for the domain of interpretation: closed, hypothetical, and confused. Five SM were identified for the domain of dialogic processes: pragmatic, alarmistic, neutralizing, delegating, and silent; while three SM were identified for the domain of management: limitation, avoidance, and flexibility (see summary Table 1).
Procedures
The interviews were administered by two clinical psychologists and psychotherapists specially trained to successfully administer each interview, which were audio-recorded and transcribed verbatim according to the APA rules with the informed consent of the participants, in compliance with the privacy legislation.
The interviews were analyzed by three independent researchers suitably trained in the use of the semiotic-narrative analysis grid.
The obtained data were then analyzed using the TwoStep cluster analysis algorithm developed in SPSS (Version 23), to find homogenous trajectory of the sensemaking processes across the three specific domains (interpretation, communication and management) of the chronic disease experience in daily life, which have been interpreted as Profiles of SoGoD.
In the TwoStep cluster analysis algorithm the log-likelihood method was used for similarity measures. The minimization of the Bayesian Information Criterion (BIC) was used identifies the optimal number of clusters and the best partitions in clusters.
The interpretation of Profiles took into account the distribution of the categories (which herein we refer to as sensemaking modalities-SM) of interpretation, communication and management across clusters, searching for categories that characterized each profile. The silhouette measure of cohesion and separation was used a measure of overall goodness-of-fit of the cluster structure.
A data-driven approach was, in essence, used to obtain the partition, combining it with a knowledge-based approach (used to define clusters). Such mixed methodology is gaining wide recognition in Psychological Research (Dolce et al., 2020).
Data were reported as number of patients (%). The relationships between the obtained profiles and the pathologies were analyzed using the Fisher’s exact test and multinomial logistic regression.
All statistical analyses were performed using SPSS (Version 23) and R 3.6.0 software environment. The level of significance was set at α = 0.05.
Results
Objective (A) to explore the general features of the experience of parenting children with chronic health conditions from the mothers’ perspective: Clinical Profiles of SoGoD
From the statistical analysis of data from the qualitative analysis of the interview on the SoGoD to mothers, we derived four Profiles of SoGoD as a synthesis of the sensemaking processes of mothers of children with a chronic disease (Table 2). The silhouette measure indicated a fair overall goodness-of-fit of the cluster structure. The obtained cluster distribution was as follows: 14 (20.6%) subjects in cluster 1, 15 (22%) in cluster 2, 25 (36.8%) in cluster 3 and 14 (20.6%) in cluster 4.
The clinical interview on the sense of grip on the disease-SoGoD (Freda et al., 2019).

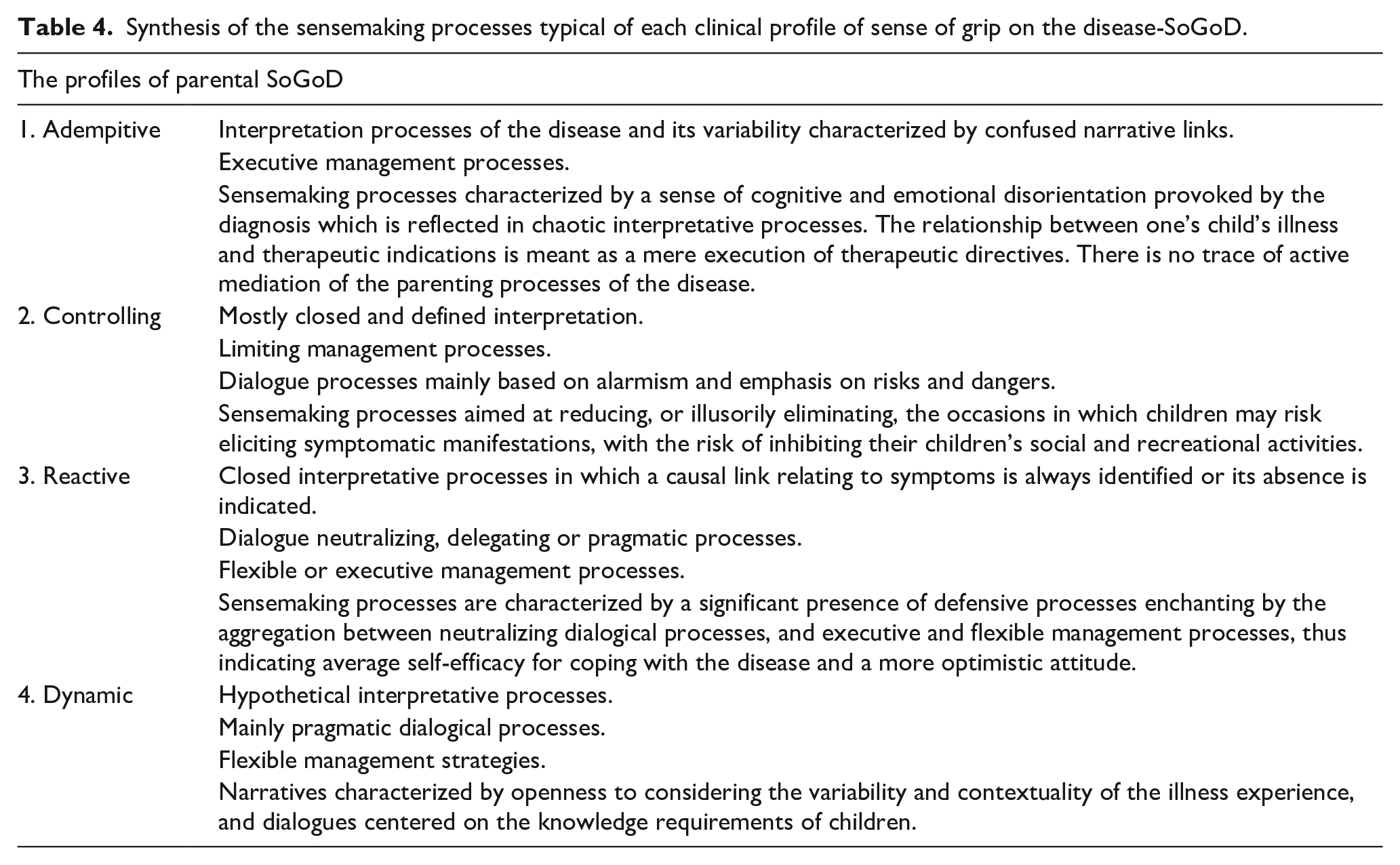
Each cluster was interpreted on the basis of the configuration of the types of MS within each domain, identifying four profiles that we called: Adempitive, Controlling, Reactive, Dynamic (Table 3). Their characteristics are listed below in semiotic terms and synthesized in Table 3.
Distribution of the SM within each cluster and interpretation of the clinical profiles.

Data are reported as number of patients (%).
Note. The most representative SM in each cluster are reported in bold.
Adempitive Grip Profile
The classification which best identifies it refers to confused interpretation processes and executive management processes. We selected this denomination because we observed that the parents’ sense of cognitive and emotional disorientation caused by the diagnosis results in confused and chaotic interpretative processes. In fact, the narrative is characterized by the total absence of hypotheses or, on the contrary, by the confusion in logical and causal terms of a multitude of connections, which are sometimes in contradiction with one another, which conveys the speaker’s lack of clarity (reader). The linguistic indicators are based on negation and absence of knowledge “no,” we don’t know,” “nothing,” . . .; or, alternatively, in the “hypertrophy of connections,” reflecting in summation indicators “also,” “too” associated with the affirmation “yes,” “it is so,” etc. This prevents the construction of a functional framework of sense to personalized disease processes replaced by the strict adherence to therapeutic guidelines. Parents seem to abdicate from any active role of intermediation and negotiation in the relationship between their child’s illness and therapeutic indications.
Controlling Grip Profile
This profile is characterized by management processes aimed at reducing or eliminating the occasions on which children may be at risk of provoking symptomatic manifestations. These occasions are related to every social, sports or recreational activity. However, apart from these activities, the real risk is to hinder the development of one’s child’s social and sporting skills, which can have a negative impact on mental health. This modality is associated with a predominantly closed and defined interpretation of the disease and the factors that trigger the symptoms, and dialogic processes mainly based on alarmism and on emphasizing risks and dangers.
Reactive Grip Profile
This profile is thus named because of the closed nature of the interpretation of the disease, which suggests a semiotic saturation process of the interpretation of the factors associated with the disease and its variability, leaving no room for interpreting the variability of the disease experience or to question interpretations already put forward. When speaking of any associated or unassociated factors with the symptomatic manifestations of the disease in question, the parent uses expressions that refer to certainty, such as “certainly,” “always,” “surely,” “without a doubt,” etc. . . . In the construction processes of such meanings it is not uncommon to find a widespread use of negations, which support the unequivocal nature of the causal link. The dialogical processes focus mainly on neutralizing and minimizing the impact of the disease and the emotions involved with living with disease in everyday life. The management processes can be alternatively classified as variables, in which there is no single management strategy but a process of continuous negotiation between the child's wishes and needs and the procedures needed for managing the disease, or executive, which requires total adherence to medical suggestions and there is no mediation process between these and the subjective background of experience. It was therefore chosen to attribute this interpretative denomination to highlight the large number of defensive processes that came to light in the neutralizing dialogical processes, which aggregate with executive and flexible management strategies at the same time, thus indicating average self-efficacy for coping with the disease and a more optimistic attitude.
Dynamic Grip Profile
Within this profile, the domain of interpretation is categorized as hypothetical, by which we intend narrative openness toward the aspects that vary, change and transform the experience according to different contexts and times. Reliable sensemaking processes are characterized by a marked sensitivity to situated and contextual dynamics, without necessarily arriving at general theories from which all of the hypotheses on disease variability are derived. In order to identify these narratives, it may be advisable to use probability indicators such as “I think,” “we think,” “maybe,” “it seems,” etc., and indicators such as “sometimes,” “once” . . . which contextualize the narration to a specific moment. The domain of management is classified as flexible for all cases belonging to the cluster, this method is attributed to narratives in which there is no single management strategy, but rather a continuous negotiation process concerning the wishes and needs of the child and the procedures required for managing the disease, while making a conscious effort to make the child capable of coping autonomously with his/her disease. Dialogue processes mainly pragmatic: speaking of the disease is characterized by the parent’s ability to indicate the child’s knowledge requirements according to his/her stage of cognitive and affective development and moment of life. The Dynamic denomination was therefore chosen to underline the degree of openness to interpreting the variability and contextuality of the disease experiences, with the dialog centered on contingent knowledge requirements and management based on negotiation between the request for their child’s autonomy and the limitations imposed by the disease. In Table 4 we make a synthesis of the main characteristic for the clinical detection of each Profile.
Synthesis of the sensemaking processes typical of each clinical profile of sense of grip on the disease-SoGoD.
Objective (B) to identify the specificities of this experience related to the different conditions under study. Relationships between Profiles of SoGoD and specificity of the pathology
The most common type of profile observed within our corpus is profile 3, interpreted as Reactive (37%), followed by the other three profiles that are homogeneously subdivided in the rest of the interview corpus, each with a value around 20%.
Furthermore, some associations were found between the type of diagnosis and SoGoD profiles, as shown in Table 5.
Relationships between the illness and the profiles of sense of grip on the disease-SoGoD- (pathology 1 = Hereditary angioedema; pathology 2 = Type 1 diabetes; pathology 3 = juvenile rheumatoid arthritis).

Data are reported as number of patients (%). p-values were computed using Fisher’s exact test.
On analyzing Table 5 it emerges that the interviews relating to “hereditary angioedema” were almost equally classified in the Reactive (39%) and Dynamic (36%) SoGoD profiles. Overall, the profile mainly represented by hereditary angioedema is the Dynamic one (71%). The interviews relating to “diabetes” were classified mainly in the limiting profile (52%). Furthermore, diabetes represented 73% of the cases. These results are also confirmed by the output of the logistic regression (Table 6) which shows that which shows that:
(1) the odd that a case is included in the Dynamic profile, over the Adempitive profile, is larger if it belongs to Hereditary Angioedema over JRA (OR = 7.00, p = 0.048);
(2) the odd that a case is included in the controlling profile, over the Adempitive profile, is larger if it belongs to Diabetes pathology over JRA (OR = 19.25, p = 0.008).
Multinomial logistic regression model (Parameter: SoGoD profile n.1).
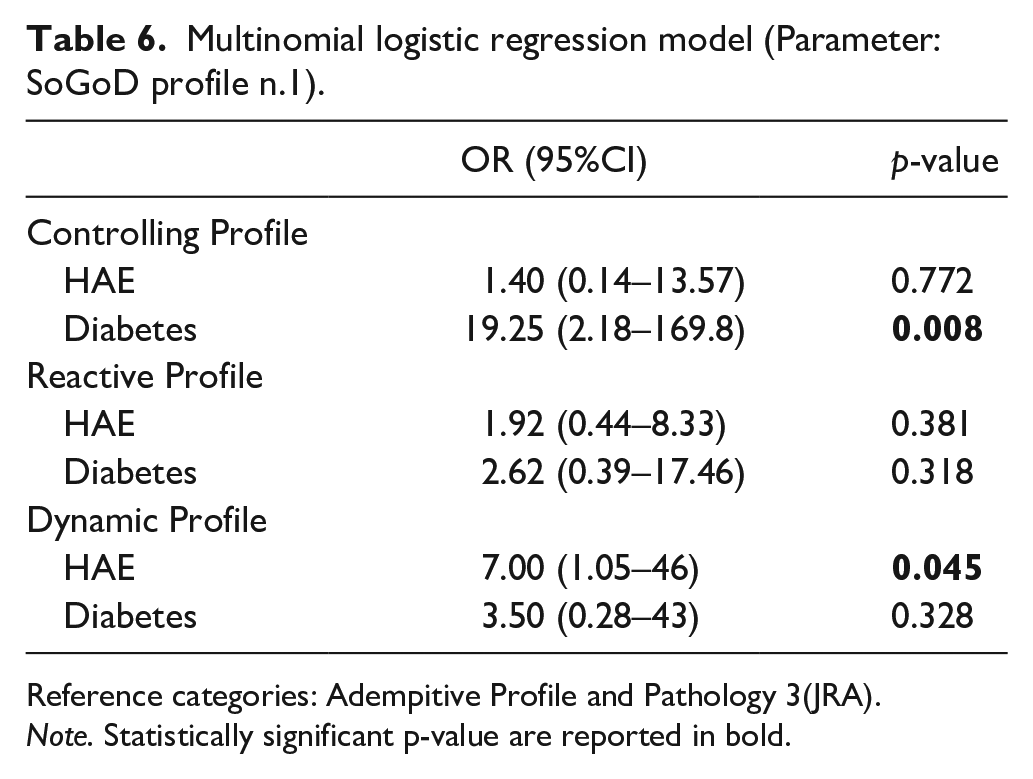
Reference categories: Adempitive Profile and Pathology 3(JRA).
Note. Statistically significant p-value are reported in bold.
As regards juvenile rheumatoid arthritis, most of the interviews were classified as Adempitive (37%) and Reactive (42%). Compared to the profiles, that of Adempitive profile is 50% in correspondence of the cases referred to this disease.
This association seems to reflect some of the characteristics of the illnesses from an interpretative point of view as if one is actually experiencing them: if the HAE narratives are classified as Reactive and Dynamic, it may be due to the fact that if they are unable to refer to standardized and generalizable therapeutic protocols to deal with the disease, which is highly likely both from an intraindividual and interindividual point of view, parents could be stimulated to overcome this lack of procedures with active SoGoD strategies based on one’s own experience or one’s own lay experience.
On the other hand, the most represented profile for the parents of young people with T1D is the Controlling profile, which reflects therapeutic practices based on blood sugar control, sports activity and general lifestyle of their children, who are at risk of becoming hypertrophic and assuming the form that we identify with the Limiting SoGoD Profile which, as previously mentioned, may hinder the child’s social and recreational life.
The narratives of parents of young people with JRA reveal that it is impossible to gain an understanding of the etiology and phenomenology of the disease, which is characterized by extremely disabling symptoms or by periods of drug-induced remission. Many of the cases classified as Adempitive fall into this category, consistent with the belief that the greater the case in interpretation, the more the parents narrate of passive adherence levels to the therapies and suggestions of their doctors.
Discussion
In short, the analyses reveal that the Clinical Interview on the Parental SoGoD on Chronic Disease—SoGoD(P)—proves to be a useful tool for understanding the overall characteristics of the experience of being parents of young people suffering from Chronic Diseases. In fact, the profiles are distributed in various ways for the different illnesses under study. At the same time, it is possible to monitor each of the illnesses under study, as shown by the association that emerges between some of the profiles and disease specificity. In fact, it was observed that the SoGoD(P) is more influenced by disease specificity in cases where stronger therapeutic directives and foreseeable symptomatic manifestation are available, as in the case of diabetes, which is classified in the profile 2 Controlling. While in cases in which the disease is less predictable and there is a lack of medical information and therapeutic protocols as in the case of HAE, the reference to the Parental lay experience and family agency seems to be stimulated, which is reflected in a Reactive or Dynamic Profile.
The specific configurations of the SoGoD(P) that have been highlighted through our analyses have enabled us to identify some of the trajectories in the sensemaking of the illness experience within the family system with respect to the interpretative, dialogic, and agentive domains. The narrative process involved in the construction of the space-time frame and the frame of meaning referring to the interpretation of the disease and its variability contributes to orienting the dialogical exchanges, choices and daily disease management practices.
It is important to note that this is not a process that ends at a specific time. It is a continuous meaning-construction process, as a function of variables such as time passed since diagnosis, emotional and cognitive processing, knowledge of the pathology, the phenomenology of pathologies and the “objective” challenges, the enabling factors outside the health care setting, the resilience resources available in a given context, and the child’s growth and his/her venturing into new developmental tasks.
Each Clinical SoGoD Profile should be understood as a narrative strategy aimed at finding forms of adaptation in order to ensure a certain continuity of everyday life for the person immersed in his primary relationships, which is effective within the original context in which it was generated. Each Profile is therefore to be considered as a context-specific sensemaking process which, will prove to be effective in protecting the individual from concrete or emotional dangers from a viewpoint that emphasizes physiological resilience to the critical conditions of the individual.
In two profiles (Adempitive and Limiting) the serious lack of flexibility in the narrative is highlighted. This semiotic rigidity needs to be seriously considered, since it may depend on the family's attempt to develop a normative reference system for constructing daily practices, with the risk that it may turn intro a rigid and stereotyped system. Such rigidity is not effective in facing with the developmental challenges of the child’s progressive psychosocial development toward an increasing degree of autonomy (Martino et al., 2019). These two profiles stimulated us further reflections on the sensemaking process. In this Profiles the narratives seem to be characterized by an absence or weakness of a narrative theory on illness experience and in an adherence to the representation of disease offered by medicine. The critical aspects—which need to be elaborated for each parent—are revealed in the narration through sensemaking processes whose consistency takes form into different types of rigidity (in which there is a hypertrophy of causal links) or in the lack of any form of personal hypothesis, of understanding, of subjectivation of what is happening.
In the Reactive profile, we find a proactive agentive tendency that sets the family system in motion when confronted with the difficulties of the child's illness, even if often in the form of reaction or negation (namely, reduction of the scope of the problem, trivialization, social confrontation strategies toward others who are in worse condition, etc). However, these narrative strategies open new signs of agency and it is often possible to find less blocked or fixed forms of interaction with different contexts.
In the Dynamic profile we are able to capture more contextualized and flexible forms of constructing a narrative on what happens within the family system. We observe how the characterizing element of flexibility in this profile takes the form of open interpretations, capable of grasping multiple hypothetical elements, of dialogical processes capable of comprehending the emotional and cognitive needs of children during development and of forms of disease management capable of balancing needs and desires, constraints, and opportunities.
Therefore, the SoGoD Interview proves to be an effective clinical tool for understanding the characteristics of the disease in daily life through the Profiles, which can help doctors and clinicians in all areas of study and provide them with the skills required to encourage family adjustment to disease.
In psychological terms, we believe that the characteristics that the functions of the narrative assume with the aim of constructing a parental Sense Of Grip on illness experience, can be interpreted in terms of the development of some psychological parenting skills, which may prove useful for coping with the disease:
Competence to make distinctions
This competence is developed by enhancing one’s ability to distinguish the specificity of the manifestations of the disease and the differences between the doctors’, parents’ and young patients’ perceptions of the disease. In the context of chronic disease, this competence takes on a central role because it enables us to observe the transformations, the changes that occur over time and to keep the different disease perspectives distinct.
Attunement competence
It enables parents to recognize (once identified) the health and emotional needs and the knowledge requirements of their child, as well as their own. In fact, recognizing diversity enables one to enter into a relationship in a virtuous way and to be capable of supporting the processes of growth, autonomy, and development.
Integration competence
The development of this competence is aimed at the possibility of integrating multiple life experience plans. One should bear in mind that a chronic disease (which can never be cured or healed) may strongly affect the affective, cognitive, and relational dimensions of patients and their families, it is therefore essential to develop integration processes which will enable us to increase the patient’s psychosocial well-being and allows for the integration of the disease with identity processes.
These skills represent developmental trajectories of narrative function, which we have captured by studying the narratives of parents of young patients. Future research should be aimed at developing these trajectories of competence in order to increase parental Sense Of Grip, which we conceive as a narrative competence for constructing the meaning of the disease, a meaning which is based on the agentive and relational processes of disease management, coping, and sharing.
Promoting Sense Of Grip is a hard work, a deliberate effort to create a space, a time and a place far from the illusion of always finding causal relations between events. The aim of this work is fostering new potential sensemaking pathways and the awareness of the “polysemicity” of the disease experience. Therefore, the goal is to help the person to experiment and to construct new narratives, which are essential for implementing new disease management strategies (Savarese, 2018).
In light of these encouraging results, we consider that much more work can be done for the progression of Sense of grip research. The first phase of our research work was aimed at an in-depth study of the sensemaking dynamics that parents realize in managing their children’s chronic disease. The future efforts go in some different but joint directions: (a) to refine these psychological models and implement the theoretical framework in light of the results; (b) to explore the development of sensemaking processes over time in a diachronic perspective; (c) to develop a more agile and lighter clinical tool to explore the experiences of parents and to personalize communications and interactions between the medical staff and the family.
The strengths of this research on the Sense of Grip on the Chronic Disease are that it relies on an abductive narrative research approach that is aimed at construing new knowledge on chronic disease. The lay experts’ knowledge has been widely explored by a narrative semiotic methodology. Nonetheless, a deep knowledge of the theoretical and methodological foundation of the SoGoD is required to administer and analyze the interviews and the analytical procedure has to be shared in a group of three researchers for its reliability. The Interview on SoGoD is therefore to be considered an “expensive” tool in terms of professional and time resources, this resulting in a limitation in the possibility of disseminating the use of the Interview. Further work is needed to transform the SoGoD Interview and its coding system in a more agile tool to be administered by doctors in order to detect an overview of the Profile of Grip and of the psychological needs and of the needs of knowledge of the patients—in this case of parents of little patients. Future work is needed to create a system of stepped and targeted interventions addressed to families of children affected by chronic diseases making reference to the SoGoD Profiles.
Footnotes
Authors’ Note
Riccardo Senter is now affiliated with University of Padua, Italy. Maria Bova is now affiliated with Department of Translational Medical Sciences and Center for Basic and Clinical Immunology Research (CISI), WAO Center of Excellence., University Federico II, Naples, Italy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.