
Abstract
The aim of this investigation is to examine the structure and the content of different social groups’ representations of the human microbiome. We employed a non-probabilistic sample comprising two groups of participants. The first group (n = 244) included university students. The second group included lay people (n = 355). We chose a mixed-method approach. The data obtained were processed using IRaMuTeQ software. The results allow us to identify the anchoring and objectification processes activated by the two different groups of interviewees. The results could be useful to those in charge of implementing campaigns aimed at promoting health literacy.
Introduction
The human microbiome is the entire complement of microorganisms that exists in and on every human body (Hawkins and Doherty, 2011). Today, microbiome research challenges established beliefs and dogmas by opening one of the most promising research scenarios in recent decades as the following references clearly demonstrate. O’Doherty et al. (2016), for example, underlined that much research on microbiome has focused on individual health, with a paucity of attention to public health implications, or on the consequences of social behaviour. In fact, recent studies show that the microbiome holds promise in explaining antisocial behaviour among humans (Gato et al., 2018). Human microbiome research raises important ethical considerations, and its long-term implications determine the possibility of fundamental shifts in the understanding of human life and health (Mcguire et al., 2008). In other words, this kind of research has the potential to transform the practice of medicine, fundamentally shifting the ways in which we think not only about human health, illness and disease but also about clinical practice and public health interventions. Drawing from a larger qualitative study on the ethical, legal and social dimensions of human microbiome research, Slashinski et al. (2013) documented perspectives related to the translation of human microbiome research into social practices, focusing particularly on implications for health promotion. In their interesting paper, O’Doherty et al. (2016) stated that Research on the human microbiome is advancing rapidly and, although still in its early stages, is showing promise of having important effects on human health. Currently, most health interventions seem to be focused on the individual and clinical levels, although broader public health benefits from this research seem likely. [. . .] Microbiome research is allowing us to better understand the impact of certain practices – such as exposure of infants to antibiotics, mode of infant delivery, and modern patterns of food consumption – on the human microbiome and subsequent health outcomes. [. . .] Evidence is accumulating that such practices, irrespective of their benefits, may have critical negative consequences. Evidence is accumulating that suggests particular microbial exposures during critical periods of infancy and childhood have long-term or even permanent effects. [. . .] With advancing knowledge of ideal healthy microbiomes, there seems to be scope for developing broad community based interventions for supporting or supplementing diets with probiotics or prebiotics. Such interventions may lead to important health benefits. However, such interventions should. (pp. 417–418)
Continued advances in human microbiome research and technologies raise several ethical, legal and social challenges. Slashinski et al. (2012) stated that ‘these challenges are associated not only with the conduct of the research, but also with broader implications, such as the production and distribution of commercial products promising maintenance or restoration of good physical health and disease prevention’ (p. 1). They have also documented several challenges associated with the commercialisation of human microbiome research, focusing particularly on how this research is exploited within economic markets for new public health uses.
Despite the amount of research just mentioned, international literature seems to lack psychosocial contributions to the study of what Moscovici defined ‘systems of values, ideas and practices that establish an order that enables individuals to become familiar’ (as cited in Herzlich, 1973: xiii) with unfamiliar objects as the microbiome. In other words, there is no research dedicated to the representations co-constructed and circulating in our society related to this very important topic. Nevertheless, we know that secondhand, socially mediated knowledge is needed to clarify some concepts or ideas for ourselves. Some practical examples can help: Are vaccines harmful or useful? Are climatic variations ‘divine punishments’ or the consequence of irresponsible human behaviour? Are genetically modified organisms (GMOs) to be considered the greatest eugenic experiment in our history or simply a useful method to save some plants from extinction? Social knowledge, in fact, is built from two distinct resources: knowledge we accept as true, without having had any direct experience, or knowledge totally originating from our direct experience (Kronberger, 2015).
Theoretical framework
As Moscovici (1999) stated, under certain circumstances, people can incorporate aspects of reality which they never paid attention to before. According to Elejabarrieta (1996), these circumstances correspond, first of all, to the appearance of an unknown object (object, situation, person, etc.), in the social context of a group. Because of the threats involved, the interest it arouses or the conflicts it generates, this object becomes salient, that means, important for the group. This gives rise to a collective communication process during which the constitutive knowledge of a social representation is elaborated and shared. It should be noted that the elaboration of this knowledge activates specific processes different from those usually used by scientists or experts of a particular domain. In summary, we can, therefore, say that social representations are constructed starting from joint processes of elaboration and exchange of knowledge. In some ways, when interacting with others, people independently produce information about events, trying to integrate real-world notions with new ideas. Everyone, therefore, acts as a ‘naive scientist’; an amateur who consumes, synthesises and transforms scientific knowledge, up to the point of producing their own medical, economic and philosophical theories (i.e. those ‘popular philosophies’ that are able to modify social reality according to human behaviour). It is well known that Moscovici dedicated his entire career to studying what happens when such transformations occur, from science to common sense, and what effect they can have on knowledge and human behaviour. Within the context of these transformations, in which new content is generated, social representations prevail, and thanks to these, people re-elaborate the information they have primarily received, solicited and even created.
In line with Abric (2001), social representations explain reality, guide social practices, retrospectively justify the positions taken and define the identity of the groups. In their construction, through the interaction between group members, representations are also influenced by extra-group conditions, such as expert knowledge transmitted by information sources (Cabecinhas, 2004). Since communication, mainly through language, constitutes the system that forms social representations (Moscovici, 1981), the main techniques to explain them aim to identify the linguistic symbols shared by people. The elements of these representations and their links with the sources of scientific knowledge and information provide clues about cognitions related to attitudes towards the object and to the strength of the link existing within the knowledge which originated the events unrelated to the life of the group.
Every day, scientific journals report new discoveries. Only a few of these discoveries become known by ordinary people through the mass media and go on to be discussed among friends, family and colleagues. How scientific information taken from the media is integrated into social knowledge shows how people give a common interpretation to the unfamiliar scientific phenomena they encounter in their daily lives. The way people understand, interpret and describe the scientific discoveries they learn about from the media and from the interpersonal communication is influenced by their social representations of the object.
Medical communication is traditionally perceived as a linear diffusion of scientific facts translated by the media for the general audience (Bucchi, 2004). This predominant vision looks at true scientific knowledge as something objective and pure, which is distorted during the transmission path to the naive public. These distortions are the cause and the consequence of an information gap between experts and their audience although a clear boundary cannot be drawn between ‘real’ and ‘popular’ science. This ‘deficit model’ minimises the specificity of the process of constructing knowledge among experts and non-experts, as already highlighted by the theory of social representations. Paraphrasing Wibeck (2014), the focus on the information gap neglects the role of the interviewees as an active participant in interpreting scientific or medical messages in accordance with the previous experience and in interaction with a variety of information sources; it also neglects the role of sociocultural factors in influencing public engagement. In our case, the transformation of scientific information is considered as a creative reconstruction: ideas from the public are not considered as false or distorted, but as correlated to the reality of the subjects who create them (Bauer and Gaskell, 1999). In this perspective, the symbolic and emotional aspects, in addition to factual knowledge, contribute to the determination of collective meanings of scientific phenomena (Joffe, 2003; Wagner et al., 2002). The thought of common sense, moreover, is shaped by pragmatic concerns. When people become aware of an important scientific discovery, they focus on the information that confirms their previous beliefs, co-constructing a coherent representation of the discovery itself. Scientific news, therefore, is elaborated and inserted in a pre-existing cognitive framework.
When medical discoveries are spread to the public sphere, the experts’ terminology used in scientific articles is replaced by everyday terminology, necessary to make the content of the scientific articles understandable. Everyday terminology contains metaphors that allow the reader to visualise a scientific phenomenon (Kua et al., 2004) and to create new meanings (Lakoff and Johnson, 1980).
As in the case of any other scientific concept, medical knowledge is altered when it is spread to lay people, who try to make sense of new, surprising or unusual information. The theory of social representations, as already mentioned, deals with the processes through which scientific information is integrated into common thought (Moscovici, 1976 [1961]), then contributing to the creation of the so-called ‘common-sense theories’ typical of the consensual universe. Nevertheless, the proliferation of the sciences has determined and continues to determine a multiplication of reified universes. Events, information and theories that dwell in the reified universes must be duplicated, reproduced at a more concrete level and transferred to those consensual universes, where it is possible to represent them. To allow this process, two mechanisms are necessary: anchoring and objectification. The former tends to ‘anchor’ unusual ideas, reducing them to daily and family categories and images; the latter affords the task of transforming abstract concepts into something concrete, almost physical. Moreover, while the anchor allows people to transfer unusual concepts in a reference frame where it becomes possible to compare and interpret it, objectification allows the reproduction of this object among visible and tangible things, so that the object itself becomes manageable. Anchoring, therefore, is a process through which representation engages the society. It has two complementary functions. On one hand, information related to the object of the representation will be interpreted from pre-existing fields of knowledge; then on the other hand, information works itself as a frame of reference.
Objectification gives reality to an unfamiliar concept. What was once located in a faraway universe appears to us now physical, accessible and handy. To objectify means to discover the iconic aspect of an idea that is not well-defined, to reproduce a concept into an image. We move, therefore, from knowing about something to knowing something. We move from the knowledge distant from its scientific object to the knowledge based on the experience of the object. The generative processes of anchoring and objectification are crucial to understand how people relate to the complex and polymorphic microbiome phenomenon: Anchoring classifies and names foreign and threatening phenomena in terms that resonate with those attempting to understand the phenomena. [. . .] Working in tandem with anchoring, objectification transforms the new phenomenon into concrete existence by way of more tangible images, concepts and symbols. (Smith and Joffe, 2013: 18–19)
The purpose of this work is to analyse these particular psychosocial processes operating in the transformation of scientific information, starting from an analysis of cognitive–affective modalities, through which people relate to a scientific discovery. The aim of this investigation is to examine the structure and content of different social groups’ representations of the human microbiome and their relation with specific social practices. The study has been articulated starting from the following research questions: ‘Do different social groups (experts or non-experts) construct different social representations of the human microbiome? What are the differences between these social representations?’ The link between different social representations and different social groups is something that characterises the theory of social representations development. It regards not only different ways of accessing the information that different social groups have (Jodelet, 1984 [1989]) but also the whole articulation of the social representation. Different social groups do not articulate scientific or non-scientific elements in the same way, because social actors establish very specific science/non-science connections, according to the different social practices and different universes of signification that they belong to. So, being part of a professional group (even if in training) can activate particular social representations. It can also determine different ways of organisation inside the central core of these groups’ social representations (Fasanelli et al., 2016; Galli et al., 2017; Schember et al., 2015; Tuselli et al., 2015).
Method
The individuals who have some knowledge about an object probably feel more involved with it and develop more practices related to it. Knowledge is a dynamic variable, in the sense that circumstances occurring over a life span can modify it. For example, each individual can modify or change his or her own level of knowledge about the microbiome by developing information about gut illnesses or food characteristics, by changing or developing his or her lifestyle and by adapting his or her food habits to his or her social relations or new life conditions (Urdapilleta et al., 2016). Bordarie and Gaymard (2015) underline that the link individuals have with the object constitutes an important element for the understanding of individuals’ representation. However, there are very few studies interested in this link. Rouquette (1994, 1997) evokes the importance of individuals’ implication towards the object and distinguishes three factors: valorisation, identification and action capacity. Abric (2001) theorises the concept of ‘Distance from the Object’ (DO). Dany and Abric (2007) published one of the rare studies testing this concept. DO is constituted by three components (Dany et al., 2014): knowledge (more or less adequate identification of the social object); involvement (the degrees of concern, through social participation, towards the social object) and level of practice (behaviours regarding the social object). According to Mouret et al. (2013), the degree of knowledge of a given object influences the level of competence about the object itself and it in turn influences the DO. For this pilot study, we decided that it was sufficient to use a simple dichotomous variable – knowledge/non-knowledge of the microbiome – as a DO proxy. Therefore, to simplify, we have specifically labelled the study participants as ‘experts’, even if in training (the ones closest to the object-microbiome) and ‘non-experts’ (the most distant from the object-microbiome). The participants belonging to the first group declared their specific knowledge of the object of study (69.58%), while the interviewees belonging to the second group mostly declared that they knew nothing about it (77.46%). Information collected by the following questions: ‘Have you ever heard of the human microbiome before?’ (Y/N) ‘If so, who did you hear about it from?’ (check list: parents, friends, professionals, newspapers, magazines, scientific publications, radio, television, Internet, social media and related specifications).
Sample
Specifically, the first group was composed by university students, considered experts in training, attending various departments of the University of Naples ‘Federico II’: Agricultural Sciences; Veterinary Medicine and Animal Production; Biology; Chemical Sciences; Physics; Chemical, Materials and Production Engineering; Earth, Environment and Resources Sciences; Translational Medicine; Molecular Medicine and Medical Biotechnologies; Public Health; Pharmacy; Clinical Medicine and Surgery (n = 244; average age = 23.01 years; Mdn = 23.00 years; Mo = 24.00 years; standard deviation (SD) = 2.73 years). We used only the university departments of ‘Federico II’ involved in the task force on microbiome studies. The second group, therefore, was composed by lay people (n = 355; average age = 39.82 years; Mdn = 35.00 years; Mo = 30.00 years; SD = 16.26 years). The main characteristics of these interviewees are summarised in Table 1. Both groups of participants were convenience samples. Strategies adopted to contact interviewees vary in each group: the students were reached at the university between classes and the lay people were contacted on the street, next to/inside shops and grocery stores. Data were collected from the month of November 2018 to the month of January 2019. Participants provided their informed consent verbally, in accordance with the Italian Psychological Association guidelines.
Lay people’s descriptive variables (n = 355).

Data collection techniques
We chose a mixed-method approach to find out the structure and the content of the microbiome’s social representation for each social group following the structural approach (Abric, 1994; Flament, 1994a, 1994b; Guimelli, 1994; Vergès, 1994a, 1994b, 1995). In this theoretical framework, to reach the significant elements of the social representation of the ‘human microbiome’ and to reconstruct the organisation of these elements, we chose the method of hierarchised evocation (Abric, 2003; Vergès, 1992; Vergès and Bastounis, 2001). In other words, we asked the participants to answer to a free association and hierarchisation task, as Vergès’ method provides. It consists of a free association task starting from an inductor term, which has the double advantage of joining the frequential dimension of the terms and the importance given to them by the subjects. As Abric (2003) reminds us, a central element, because of the role that it plays in a specific social representation, has all the possibilities to be frequent in the verbal expression of its ‘producers’. This frequency, thus, represents an indicator of centrality if it is completed by a more qualitative information, the importance, expressed by the attribution of a hierarchy between elements, that subjects are requested to assign to it. The intersection between these two criteria is the only aspect that makes the identification of constituent, or significant elements, possible. In particular, we asked the participants to write the five most important words they freely associate to the inductor ‘human microbiome’ to motivate their choices in writing a justification for each evocated word and to list the five nouns or adjectives in order of importance. We completed the free association task with open-ended questions about the subjective justification linked to each of the associated terms, to avoid lexical ambiguity, malapropisms, and so on, typical of this kind of data (Galli et al., 2018; Marzana et al., 2016). Synthetically, our research materials consisted, for each subsample of participants, in a corpus of free associated words, a corpus of open-ended answers for every single chain of associated terms and a corpus of information deriving from all the other items related to the descriptive variables, as well as the knowledge of the microbiome.
Analysis strategy
The terms evoked by the participants were first treated with a lexical and categorical analysis. In the lexical phase, they were aggregated on the basis of the synonymy criterion in order to obtain clusters of terms substantially coincidental with the manifest meaning (Bardin, 2003). Therefore, using a semantic criterion, terms were further aggregated starting from their justifications. Each of the obtained clusters was associated with a new label. Every label was identified using, as a selective criterion, the high semantic proximity and frequency of occurrence of every term aggregated inside of it. Five independent judges completed the whole analytical process. Each judge worked first individually; then, afterwards, all of them discussed their analysis and agreed on a shared position. We choose an inclusion threshold for the obtained categories, which allowed us to process only those that contain words provided by at least 5 per cent of participants. In this way, we obtained 14 different categories of interviewees for both groups (Tables 2 and 3) containing 80.14 and 82.51 per cent of all evocations, respectively, for the experts in training and lay people. The obtained data were then processed by the software IRaMuTeQ. A prototypical analysis was allowed to reach the elements, which enabled us to hypothesise the central core and the correspondent periphery configuration of the social representation of the human microbiome, for each group of participants.
Experts in training – shared semantic field (threshold 5%).

Lay people – shared semantic field (threshold 5%).

Data were also treated with a similarity analysis (Flament, 1962). This analysis (a particular type of network analysis) was also supported by the software IRaMuTeQ (R interface freeware), which has the advantage of better showing the organisational structure of the significant elements of every social representation. The procedure consists of an elaborate matrix of similarity starting from the selected index, which depends on the nature of the relationship among the considered variables. In our case, the Russel and Rao (1940) (RR) index was selected. The RR index is a distance measure (Chay et al., 2010; Hwang et al., 2001) used, in our case, because of its exclusion of negative co-occurrences (Meyer et al., 2004). The output of this analysis consists of a graph, on which the structural elements of the social representation are shown with different kinds of links (more or less marked), on the basis of their RR value. The selected threshold expresses the relations (and their strength) between structural elements and their network. The final graphs were elaborated using the logic of the ‘maximum tree’, in order to provide the best summarised information about the clustering elements (Vergès and Bouriche, 2009). In the listed figures, the size of the colourful vertices is proportional to the word frequency, and the edges’ thickness indicates RR index strength of the words’ link.
Moreover, a descriptive statistical analysis was conducted on all the variables used in questions in the first part of the interview (previous knowledge, age, gender, educational level and employment).
Results and discussion
Do groups of participants with different distances from the object produce different representations of the human microbiome? This research question guided the empirical process already described. Studying a social representation, in the structural approach, means discovering the constitutional elements of its structure. The central core theory has an essential methodological consequence: a social representation study is, first and foremost, looking for its central core components. The results were obtained by comparing the entire corpus of freely associated terms to the inductor ‘human microbiome’ and categorised as shown in Tables 2 and 3. Prototypical analysis was carried out through the analysis of the correlation between rank of importance and frequency of appearance, by means of the IRaMuTeQ software (Table 4).
Experts in training – prototypical analysis.

The analyses of the structural elements in the left upper quadrant (Figure 1) – which constitutes the hypothetical central core of the students’ representation of the human microbiome – reveal that the category microorganisms (which aggregates terms like microbes, bacteria, virus, and germs) reaches the highest number of preferences (Freq. 173; 71.25% of these interviewees) and the most important position (Mimportance = 2.00). Many experts in training write that ‘I imagine it makes up most of the microorganisms present everywhere in the body’ (B28_F); in fact, ‘the bacteria physiologically cooperate in the human body to maintain the normal homeostasis’ (O11_M 1 ), essentially ‘because some bacteria are the main basic microorganisms of the body, which perform some fundamental functions’ (O13_M).

Internal configuration of the social representation of the experts in training (similarity analysis).
In the same quadrant, we found biology (which aggregates all the references specifically to the discipline) that also reaches a lot of preferences (Freq. 91; 37.92% among the students) and a significant position of importance (Mimportance = 2.3). In this case, participants justify their choice using short sentences like ‘This is the field of study related to living organisms’ (Q17_F); biology is ‘the discipline that analyses microorganisms’ (A16_F), because ‘I link it to this area, even though I’ve never heard of the microbiome’ (E18_M).
The right upper quadrant identifies the first periphery of the social representation of human microbiome constituted by four different categories. The experts in training involved in the research frequently refer to the whole human body, to the organism and its functions, as shown in these sentences classified as integrated-human-body (Freq. 87; 36.25% among the students; Mimportance = 2.8): ‘Something that characterises the human body and its functionality’ (L13_M) and ‘Lives in symbiosis with our body’ (M05_F). The label mankind (Freq. 85; 35.42% among the students; Mimportance = 3.0) overlaps with one of the most frequent words freely associated to the inductor, but characterised by the most synthetic justifications: ‘The microbiome has to do with mankind’ (M15_F). The next category research&experimentation (Freq. 84; 34.17% among the students; Mimportance = 3.3) contains, within it, all the references to the world of scientific research and useful tools to achieve it, such as microscope, laboratory, reagents and test tubes. All these elements are considered by the participants to be highly important ‘because without research it’s impossible to know and prevent diseases linked to the human microbiome’ (P17_F)
The last category in this quadrant, cellular-genetic-material (Freq. 75; 30.42% among the students; Mimportance = 2.9), collects all references to cells, chromosomes, genes and so on, justified with sentences phrases that testify a lack of knowledge of the research object, even among expert respondents: ‘Because microbiome concerns something small that is inside the cells’ (N12_F).
In the lower right quadrant, we found the second periphery of the human microbiome social representation characterised by all the structural elements that are entering the social representation or that are becoming less important: in other words, all the most fluctuant cognitions about the object. The first category in this quadrant life (Freq. 48; 20.00% among the students; Mimportance = 3.1) assembles all the references to the etymological origin of the word microbiome, as testified by the interviewee who wrote ‘bios from the Greek means life’ (M06_M). The category parts-of-the_human-body (Freq. 47; 19.17% among the students; Mimportance = 3.0) is constructed from the terms employed by participants to locate the microbiome in the blood, in the organs or in the tissue, in general, even if, as stated bythe majority of the respondents, ‘much of the process takes place in the gut’ (H09_F). Next category, pathological aspects (Freq. 44; 18.33% among the students; Mimportance = 3.2), is characterised by ambivalent assertions which refers to the microbiome as a cause of illness or as a remedy for it, as testified by these interviewees: ‘Microbiome reminds me of melanoma, something that has assonance with a disease’ (B20_F); ‘The malfunctioning of one of the elements of the biome could lead to diseases and not allow the perfect function to others’ (A01_F). The label of the category medicine-doctors-garrisons (Freq. 36; 15.00% among the students; Mimportance = 3.2) summarises all the nouns corresponding to the medical semantic area because most of the respondents who refer to it affirm that ‘the microbiome makes me think of the medical field’ (N02_M) or ‘I believe that the study of the human microbiome can lead to the production of specific medicines’ (Q17_M). In the same way, the tag health (Freq. 33; 13.75% among the students; Mimportance = 3.1) also reflects accurately the type of material categorised essentially because for our respondents ‘a correct microbiome has one of the favourable effects on the health of the organism’ (Q12_M). In the category environment&nature (Freq. 26; 10.83% among the students; Mimportance = 3.0), we could find all references to the exchanges between human beings and the environment in which they live: ‘because I think it is part of the environmental interactions of microorganisms’ (H05_M) that compose the entire microbiome. The label genetic (Freq. 20; 8.33% among the students; Mimportance = 3.2) groups all the terms that refer directly to this scientific discipline: ‘It reminds me of genetics’ (M20_M) and ‘It has to do with research related to genetics’ (Q14_M). The last category in this quadrant is therapies&drugs (Freq. 15; 6.25% among the students; Mimportance = 3.7), which contains expressions such as ‘The microbiome brings me back to the world of pharmacopoeia and the use of drugs’ (Q21_M) or ‘Today and future therapies acting on the microbiome certainly have a great importance’ (Q12_M).
The absence of nouns in the lower left quadrant might be explained by the absence of a subgroup of participants who share a different vision of the object, testifying to a high consensus on the semantic field of these interviewees.
Table 5 shows the results for lay people. In this case, the first quadrant of the prototypical analysis output contains a higher number of elements in comparison with the results obtained from the experts in training. The first category, microorganism (Freq. 155; 43.87% among the lay people; Mimportance = 2.6), contains the largest number of free associations such as bacteria, virus, microbe and germs, pathogen agents which underpin a negative representation of the human microbiome as indicated by many respondents: ‘The microbiome is linked to bacteria, to viruses’ (A25_F) and ‘it seems to me to be something infected’ (H22_F). Non-expert people made a large number of references to DNA, genome, mitochondria, ribosomes and blood cells and we classified them as cellular-genetic-material (Freq. 126; 35.90% among the lay people; Mimportance = 2.4). Free association justifications such as ‘because microbiome is made up of proteins that catalyse cellular reactions’ (F7_M) and ‘because I think the microbiome is in the DNA’ (G18_M) guided our choice for this label. The hypothetical nucleus of the microbiome’s social representation is also composed by the concepts classified as integrated-human-body (Freq. 125; 35.61% among the lay people; Mimportance = 2.6). In this category, we included verbal expressions such as part of the human body, ‘it is the essential element of our organism’ (G11_M) and ‘the human microbiome has developed a symbiotic relationship with the organism that hosts it’ (K9_M). Another important element of this quadrant is biology (Freq. 116; 33.05% among the lay people; Mimportance = 2.7) that aggregate all that terms which ‘pertains to the scientific field, the biology’ (C22_F). The last category medicine-doctors-garrisons (Freq. 89; 25.36% among the lay people; Mimportance = 2.7) contains nouns such as medicine, hospital, doctors and nurse, generally justified as follows: ‘The microbiome is the subject of study of medicine’ (E19_F); ‘I think it’s a disease to be treated in the hospital’ (J1_M).
Lay people’s prototypical analysis.
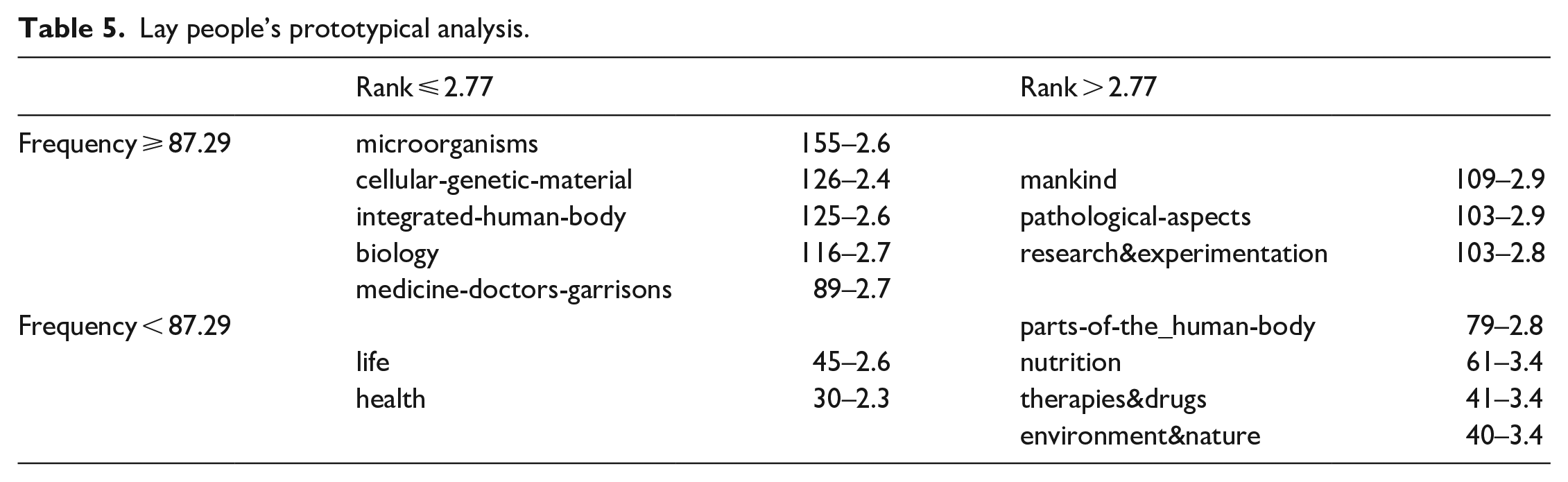
In the upper right quadrant, the category mankind (Freq. 109; 31.05% among the lay people; Mimportance = 2.9) was constructed using the most frequent word freely associated by respondent to the inductor to express this kind of cognition: ‘The human microbiome concerns mankind’ (K14_M). With the label pathological-aspects (Freq. 103; 29.34% among the lay people; Mimportance = 2.9), we classified all the references to illness, cancer and pathology, in general. Interviewees justify these associative choices affirming that ‘I think it’s a disease’ (I14_F), in fact ‘the name (microbiome) seems to recall a serious pathology’ (K13_M) or worst ‘usually leukoma, myoma are linked to the word cancer’ (G29_F). Finally, the category research&experimentation (Freq. 103; 29.34% among the lay people; Mimportance = 2.8) contains nouns like science, microscope, discovery, laboratory and many other terms ‘connected to the research world’ (A13_M).
In the lower right quadrant, the category part-of-the_human-body (Freq. 79; 22.51% among the lay people; Mimportance = 2.8) contains nouns such as gut, eyes, stomach, heart, skin, bones and mouth, all considered ‘the place where these microorganisms live’ (K16_F). Next is a category absent from the social representation’s structure of the expert respondents, nutrition (Freq. 61; 16.52% among the lay people; Mimportance = 3.4), which contains evocations such as food, diet and obviously nutrition itself. Also, in this case, we found an ambivalent orientation among the interviewees which are convinced that the microbiome ‘is connected to a healthy diet’ (I10_F) and at the same time they consider it as a pathogen agent affirming that ‘Always for these diseases caused by microbes, attention must be paid to nutrition’ (I38_F). In the same section of the table, the category therapies&drugs (Freq. 41; 11.68% among the lay people; Mimportance = 3.4) contains references to cure, surgery, antibiotics, probiotics and so on. It is interesting to note that the respondents who used the terms in this category think of the microbiome as a disease to be treated: ‘The microbiome can be treated with drugs’ (A17_F) and ‘because maybe it’s a disease’ (F3_M). In the category environment&nature (Freq. 40; 11.40% among the lay people; Mimportance = 3.4), we found concepts like ecosystem, environment, ecology and so on, which are essentially used by the respondents to express their idea that the human microbiome is ‘influenced by the external environment’ (H17_F).
The lower left cell includes the last two categories. The first is life (Freq. 45; 12.82% among the lay people; Mimportance = 2.6) ‘because “bios” from the Greek means life’ (M6_M). The second is health (Freq. 30; 8.55% among the lay people; Mimportance = 2.3) because the human microbiome ‘helps determine human health’ (I32_F)
To identify the most important category between those derived from the analysis just outlined, we used Sutrop’s (2001) cognitive salience index (CSI), from which we obtained the following ranking (Tables 6 and 7).
Experts in training – cognitive salience index (CSI) ranking (n = 244).

Lay people’s cognitive salience index (CSI) ranking (n = 355).
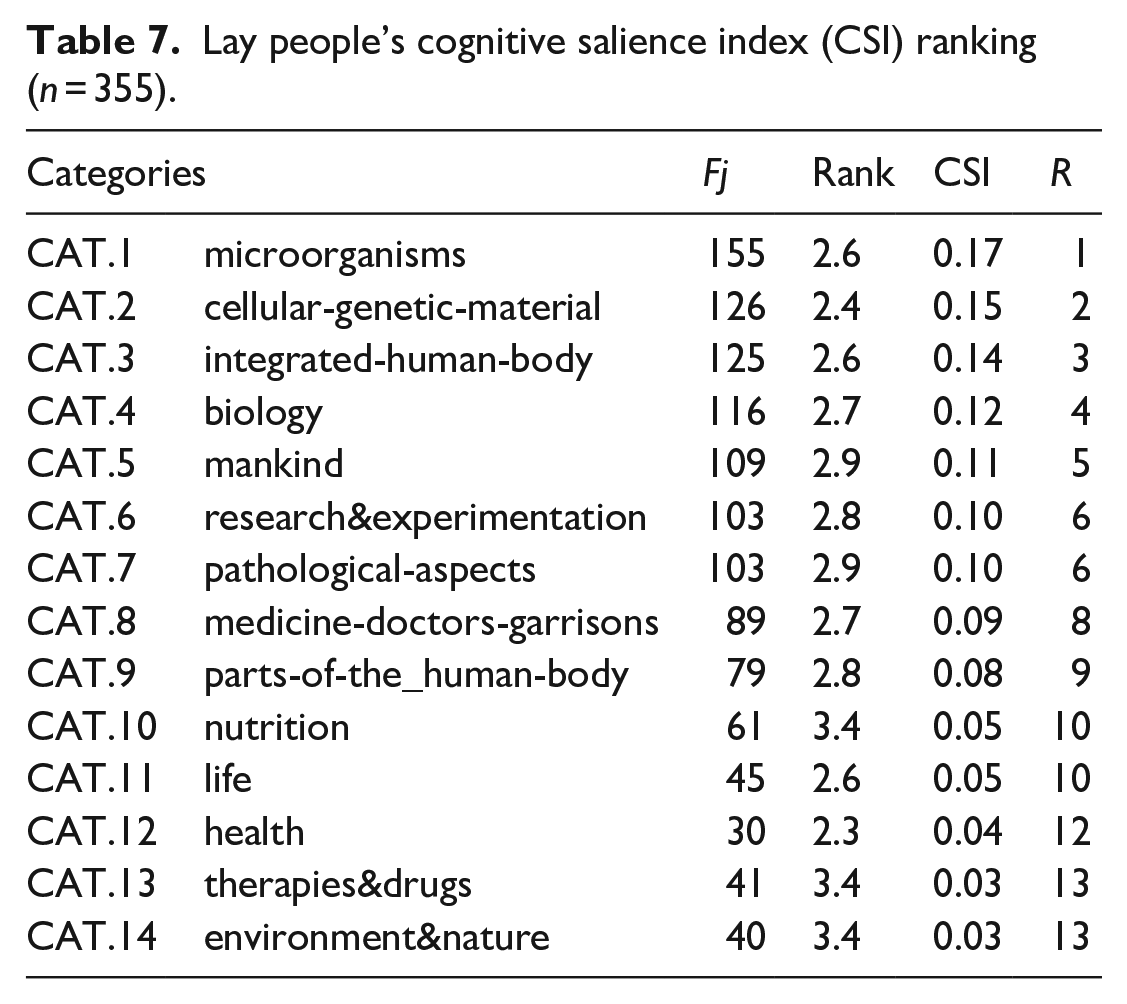
From the classification obtained using the Sutrop index, it is possible to note the evident salience of the category microorganism that was most frequently mentioned by both experts in training and lay people. This is confirmed by the centrality of this element in the configurations presented in the following graphs (Figures 1 and 2), through which it will be possible to reconstruct the existing interrelations between the constitutive elements of the structure of the social representation of the human microbiome. In fact, as stated by Abric (2003), it is not enough to know the content dimension of a social representation, and it is the organisation of this content that gives meaning to the entire representation. It also permits the comparison between groups: identical contents which may correspond to a totally different symbolic universe and, consequently, imply dissimilar social representations.
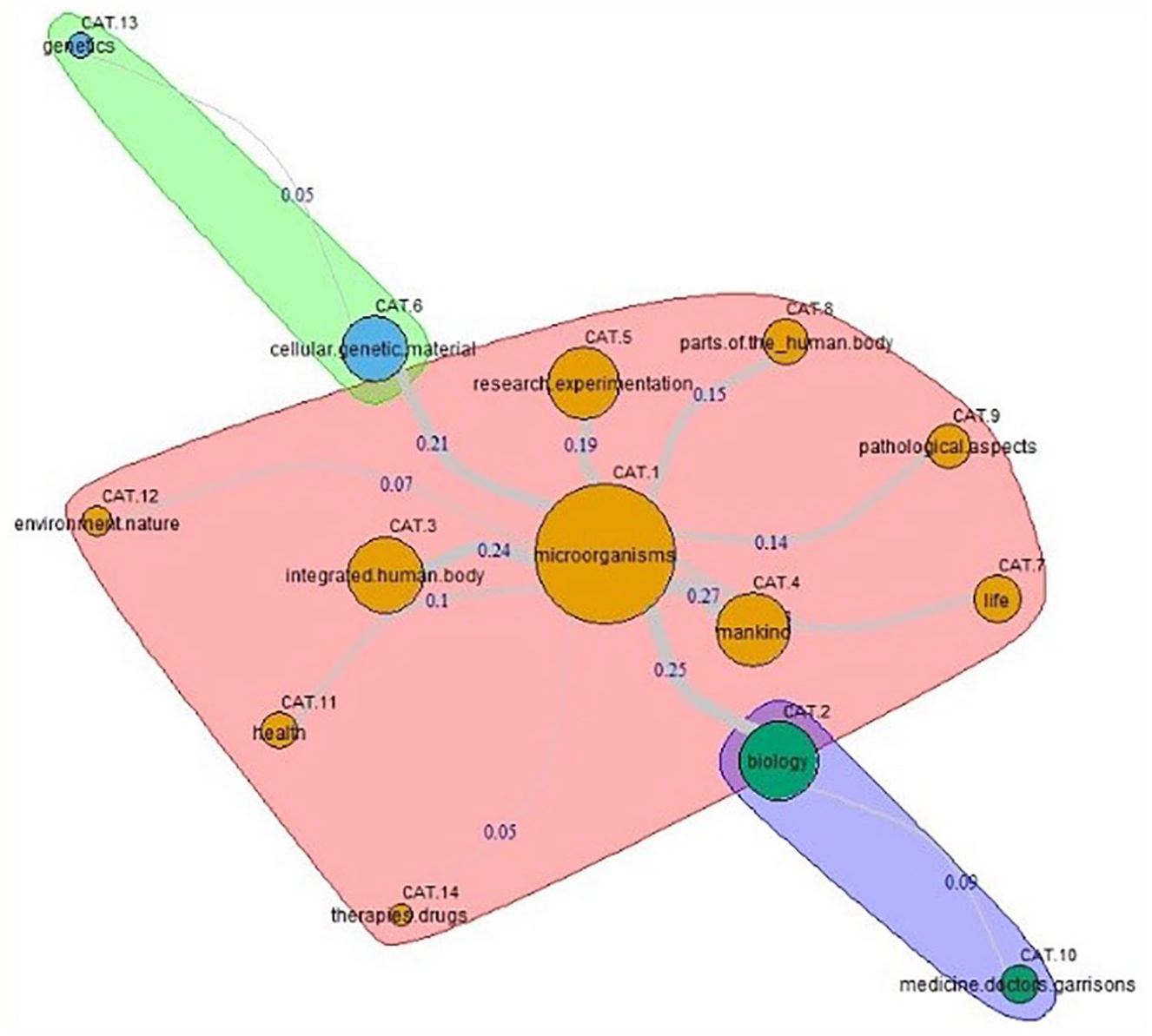
Internal configuration of the lay people’s social representation (similarity analysis).
The first configuration concerns students’ understanding of the human microbiome. As already mentioned, we chose the RR (Russel and Rao, 1940) coefficient to weigh the strength of the semantic link existing between each structural component of the representation.
As shown in the graph, the most important category is microorganism. Due to 11 links (Figure 1) that add an RR coefficient of 1.8 (92.78% of the whole graph coefficient), microorganism is the element with the highest degree of relatedness. The centrality of this category in the social representation structure is evidenced by the interconnections existing between the distinct justifications that respondents use to explain their free associations. For example, the student M15_F argues that the microbiome corresponds to ‘microorganisms that have to do with the human body, because they are situated in the human body’ (CAT.1–CAT.3; RR: 0.24), 2 ‘they remind me of biology’ (CAT.1–CAT.2; RR: 0.25) and ‘all this has to do with the mankind’ (CAT.1–CAT.4; RR: 0.27). The interviewee D06_F associates ‘the microbiome with the genetic patrimony’ claiming, however, that ‘it is micro-organisms similar to viruses or bacteria’ (CAT.6–CAT.1; RR: 0.21); in his opinion, ‘the activity of the microbiome can be influenced by diseases’ (CAT.1–CAT.9; RR: 0.14) and ‘knowing more about the microbiome could open new doors to the medical field, where interesting experiments could be conducted’ (CAT.1–CAT.5; RR: 0.19). The student N13_F affirms that ‘the term “micro” refers to something small, microscopic’, while ‘the term “bio” refers to biology’ (CAT.1–CAT.2; RR: 0.25), ‘therefore all that concerns the nature from a human and environmental point of view’ (CAT1–CAT12; RR: 0.07); ‘The human adjective refers to the quality of the microbiome, which is therefore related to the human body [. . .] because there is an integration with man and his body’ (CAT.1–CAT.3; RR: 0.24). The participant P20_F thinks that ‘the life of our cells depends on the microorganisms of the microbiome’ and that ‘it is part of our body’ (CAT.1–CAT.3; RR: 0.24); ‘Its malfunction is the cause of pathologies’ (CAT.1–CAT.9; RR: 0.14); however, ‘we are looking for a way to guarantee its correct functionality through research that is focused on this topic’ (CAT.1–CAT.5; RR: 0.19). For his part, the student Q11_M believes that the microbiome is composed of ‘fungi and bacteria that are normal residents of the intestinal mucosa’ (CAT.1–CAT.8; RR: 0.15); in his opinion, ‘trying not to alter the human microbiome is of fundamental importance [. . .] to enjoy good health and well-being’ (CAT.1–CAT.11; RR: 0.1), so much so that it ‘is used in specific therapies for some patients’ (CAT.1–CAT.14; RR: 0.05).
Also, the two side clusters to the most relevant aggregate placed at the core of the graph are strongly interconnected with the nucleus of the representation, as shown by the direct links with the central category and the concatenations that derive from it. According to the participant D10_F, for example, ‘the particles that make up the microbiome are infinitesimal’ and strictly ‘linked to human life’ (CAT.1–CAT.7; RR: 0.13); ‘I have the impression that they carry out their activities mainly in the brain’ (CAT.1–CAT.8; RR: 0.15), which ‘are studied by biology’ (CAT.1–CAT.2; RR: 0.25), but ‘I associate them with medicine’ (CAT.2–CAT.10; RR: 0.09). To further confirm, the participant D18_F believes that the prefix ‘micro corresponds to microbe’ and that her ‘mind brings me back to the concept of genetic heritage’ (CAT.1–CAT.6; RR: 0.21). ‘Everything refers to reminiscences of genetics in general’ (CAT.6–CAT.13; RR: 0.05).
The graph representing lay people (Figure 2) shows a totally different articulation of the structural elements. In fact, in this case, we have three different clusters that are quite similar in weight. The most important aggregate, also in this case, is the one composed by the closest cognemes to the category labelled microorganisms (six links that together add a RR coefficient of 0.66–50.76 per cent of the whole graph coefficient). The second aggregate, generated starting from the category integrated-human-body, is composed of four links that together add an RR coefficient of 0.35–26.92 per cent of the whole graph coefficient. The last cluster aggregates categories that gravitate around biology (three links that together add an RR coefficient of 0.29–22.31 per cent of the whole graph coefficient).
Also in this case, when participants were asked to justify their free associations, they used brief expressions strictly linked between them. The woman A22_F, for example, affirms that ‘the microbiome is linked to the cell virus and it is part of every human being’ (CAT.1–CAT.5; RR: 0.15). In her opinion, the microbiome is ‘a sort of disease: perhaps the microbiome attacks the cells’ (CAT.1–CAT.6; RR: 0.14). The reason why the elements inside this cluster are so connected between them became evident in the motivations offered by the respondent I4_M: regarding the study of everything related to microorganisms, cells and their endogenous and exogenous functions, the microbiome has to do with something extremely small, like germs, which can give both positive and negative effects on the human body, also generating pathologies (CAT.1–CAT.6; RR: 0.14). Also, the participant G19_M considers the microbiome something dangerous, ‘because it is a microbe, it is a disease’, even if it ‘could be healed’ through the use of therapies&drugs (CAT.1–CAT.12; RR: 0.04). The relationship between microorganisms and environment&nature is explained by the interviewees I7_F: ‘Bacteria are the first thing that came to my mind, it makes me think of something that has to do with nature, the ecosystem, ecology’ (CAT.1–CAT.13; RR: 0.05).
The next conglomerate, generated from the existing link between microorganisms and integrated-human-body categories, finds its explanation in the affirmation of the respondent A5_F who states that ‘from the word micro, I thought microbe, that makes me think of something integrated in our body’ (CAT.1–CAT.3; RR: 0.15). Another woman C30_F affirms, ‘it (microbiome) seems to me something inherent in the human body, something genetic’ (CAT.3–CAT.2; RR: 0.15). Respondent A26_F is more specific, claiming that ‘the microbiome is the whole of the genetic heritage, it is formed by the microorganisms that are present in the intestine, one of its sites within the human body’ (CAT.2–CAT.9; RR: 0.09). In addition, participant G3_F says, ‘I believe that the microbiome is in the blood, because I thought about the analysis of the human cell’ (CAT.2–CAT.9; RR: 0.09) and ‘it is always linked to human life’ (CAT.9–CAT.11; RR: 0.06). Finally, ‘the man in the street’ L10_M says that ‘the human microbiome concerns the sphere of bacterial function present in human beings as it consists of microorganisms integrated in the human body’ (CAT.1–CAT.3; RR: 0.15); ‘I suppose it concerns the health domain relating to the well-being of the individual’ (CAT.3–CAT.13; RR: 0.05).
The third cluster generated by the strong link between microorganisms and biology aggregates references to the research&experimentation, medicine-doctors-garrisons and nutrition as testified by the following assertions. The interviewee C2_F ‘refers to microscopic bacteria living in the body and has to do with genes’ considering the microbiome ‘related to microscopic biology’ (CAT.1–CAT.4; RR: 0.13). Another participant F6_M thinks that ‘it is related to the field of biology, referring to the human organism, I think it refers to research on stem cells’ (CAT.4–CAT.7; RR: 0.11) and ‘it concerns studies in the medical field’ (CAT.7–CAT.8; RR: 0.11). The relatedness between these categories is explained also by the respondent H1_M who admits, ‘Not knowing it (microbiome), I think it may be something new or otherwise part of scientific research; I imagine it is something usable in the medical field; could be in relation to health, to the cure of diseases’ (CAT.7–CAT.8; RR: 0.11). The last connection in this cluster is justified by the man J2_M who says: ‘I think it’s something related to biology and I connect it to nutrition’ (CAT.4–CAT.10; RR: 0.07).
Conclusion
Our results allowed us to identify the anchoring and objectification processes activated by the two different groups of interviewees. Specifically, experts in training anchor the human microbiome primarily to the structure of DNA. There are numerous references to this prototypical image of scientific knowledge as it emerges from the words of the participants, when they claim that ‘Thinking about the microbiome the helical structure of DNA appeared to me’ (D04_M). They are also convinced that ‘the microbiome could depend on our DNA and therefore be genetically transmissible’ (D20_F) and that ‘all the microbiome microorganisms are found in the genetic heritage’ (M03_F). According to these experts in training, ‘It is absolutely necessary to have clear vision of the information contained in the genome, because with the manipulation of genetic information it is possible to safeguard the health of many people’ (L18_M).
These same respondents clearly objectivated the microbiome in its constituent elements, the microorganisms, to which, however, they attribute a negative value. In fact, for many experts in training ‘the microbiome is a microbe’ (P01_M) in the sense that ‘the microorganisms of the microbiome are the cause of pathologies’ (L07_F) or that ‘the microbiome is made up of micro-organisms similar to viruses or bacteria’ (D06_F). One participant, more specifically, wanted to point out that ‘the plasmid is the characterising element of microbiome bacteria, and thanks to its genetic information, it can give resistance to antibiotics or virulence’ (L14_M).
The anchoring of lay people appears to be surprisingly similar to those of experts in training; in fact, most of them link the human microbiome to DNA. These interviewees ‘believe that the microbiome belongs to our DNA’ (E34_F), that ‘it’s something about human DNA’ (K2_M), something that makes them ‘think of a DNA sequence’ (H11_F), because ‘the microbiome is connected to the concept of human genome, to genetic makeup’ (E18_F). Even their objectifications are similar to those of experts in training and, therefore, also testimonies of a negative representation. ‘The microbiome is a kind of virus’ (K18_F), ‘or a disease recently discovered through medical research’ (K21_F). In particular, the microbiome ‘is made up of pathogenic bacteria’ (M20_F) or even by ‘a microbe that attacks the ovaries’ (G24_F).
On the basis of the obtained results and taking into account the processes of anchoring and objectifications produced by the two distinct groups of participants, it appears legitimate to state that there are no such differences to allow us to answer affirmatively the questions that have guided the entire research path presented. It is therefore not possible to speak of two different social representations of the human microbiome, because, although articulated differently in the speeches of experts and non-experts, the representational contents, the structural elements and, above all, the meanings attributed to them converge towards a negative vision of the object of analysis. In fact, the modes of thinking of experts and lay people are not completely independent of each other; instead, they coexist such that one system can capture information produced with the standards of the other. This last point corresponds to the notion of “cognitive polyphasia” in social representation theory and is of importance because it gives common sense a real epistemological status. (Jovchelovitch, 2007, 2008 as cited in Courvoisier et al., 2013: 289)
The lack of knowledge about the microbiome has given rise to explanations essentially focused on the attempt to reconstruct the etymology of the word. As it is known, common sense re-elaborates cognitively and emotionally the concepts, rather than using them more or less rationally. For this reason, the ‘micro’ prefix has become unmistakably a synonym of microorganism, understood as a bacterium, virus and so on, and the suffix ‘oma’ has been linked by assonance to pathologies such as melanoma and sarcoma. Therefore, it seemed difficult for people involved in the study to think as positive something constituted by negative components. Medical communication, in order to be truly effective, should ‘intervene surgically’ precisely on these negative representational dimensions, allowing people to build their own naive theories on the human microbiome, starting from the immeasurable benefits that a healthy microbiome can bring to human health and quality of life. In fact, according to O’Doherty et al. (2016): To benefit public health, human microbiome research needs to prove its utility on both the clinical and the community level. Lessons learned from public health campaigns, such as vaccination and screening programs, will help convince the public of the acceptability of programs derived from microbiome research. Public trust in the regulation and oversight of such products and campaigns is essential to their success. (p. 418)
So, if people construct and share common-sense theories starting from a negative vision of the microbiome, if their social representations are generated from a bad association between microbiome and lethal illnesses like melanoma, lymphoma and sarcoma, they never could accept the healthy consequences of an increasing knowledge about this fundamental resource of our body.
Anyway, although unexpected, the positions expressed by experts in training of scientific disciplines and lay people involved in this research do not appear surprising. In a recent article appearing in Nature, Herd et al. (2018) assert that ‘the microbiome is now considered our “second genome” with potentially larger importance than the genome in shaping human health’ (p. 808). Even the World Health Organization (WHO) – India (2016) has compared the microbiome to a mere instrument to combat antibiotic resistance, proposing a bio-medical model, aimed at prevention, rather than a bio-psychosocial model, intended to promote health. In doing so, the Country Office for India contradicted WHO general directives, promulgated in Agenda 2030 (Goal 17) during the Ninth Conference on Health Promotion held in Shanghai in 2016. Fortunately, in the work plan for the next 10 years, this same organisation proposed the development of global policies, aimed at a new form of promotion, and ‘Health Literacy’ (WHO, 2016) and asked research centres and academic institutions to develop and improve useful methodologies to ‘measure the culture of health’. Through this study, we tried to accept this proposal, because using a psychosocial point of view to study the issues concerning the health of people can be taken as a reference to a broader network of social representations held together as an organised whole by a community (Duveen, 2007). One of the main principles of this theory is that it proposes that social change does not simply imply the substitution of old ideas by new ideas but, instead, that it often results in the co-existence of conflicting meanings within the same society, groups and individuals, during a certain period of time. (Batel and Devine-Wright, 2015)
The study so far represents only a starting point which will have to be followed by research conducted on larger and more representative samples of the different instances present in our sociocultural context. However, we hope that the results we obtained can be useful to those who are charged with implementing campaigns aimed at promoting new and more effective ‘Health Literacy’.
Supplemental Material
LayPeople_engl_matrix_1 – Supplemental material for Public understanding of science and common sense: Social representations of the human microbiome among the expert and non-expert public
Supplemental material, LayPeople_engl_matrix_1 for Public understanding of science and common sense: Social representations of the human microbiome among the expert and non-expert public by Ida Galli and Roberto Fasanelli in Health Psychology Open
Supplemental Material
LS-plus-PE_engl_matrix_1 – Supplemental material for Public understanding of science and common sense: Social representations of the human microbiome among the expert and non-expert public
Supplemental material, LS-plus-PE_engl_matrix_1 for Public understanding of science and common sense: Social representations of the human microbiome among the expert and non-expert public by Ida Galli and Roberto Fasanelli in Health Psychology Open
Footnotes
Acknowledgements
We thank Mrs Dianna Pickens and Mrs Nadja Dominique Ismail for the English revision of the manuscript. We also acknowledge Prof. Danilo Ercolini for his helpful advices and comments and Prof. Francesco Giannino for his encouragement and generous support.
Author contributions
All authors contributed equally to this work.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Data availability statement
All datasets generated for this study using IRaMuTeQ software are included in the manuscript/supplementary files.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.