
Abstract
This study emphasizes the role of pain catastrophizing and state anxiety on pain tolerance and pain-related anxiety. Response expectancies for pain tolerance and pain intensity were tested as potential mediators. A cold-pressor task was used on a healthy sample. Measures were taken before and after cold-pressor procedure, while aversive versus neutral information regarding the cold-pressor task was given prior to the pain induction. An exploratory path model was conducted. Similar paths for pain tolerance and for pain-related anxiety were shown in aversive condition. Also, psychological measures may explain pain experience in aversive context.
Introduction
The main dimensions of the sensorial component of pain are pain tolerance and pain intensity (Crombez et al., 1999; Masedo and Esteve, 2007; Meesters et al., 2019). Pain tolerance is defined as the maximum amount of pain that a person can bear (Philips, 1988). Literature shows that lower levels of pain tolerance are often associated with depression, fear of future disability, frustration, anger, lower activity levels, reduced pleasure, isolation, disruption of intimate relationships, a sense of helplessness, and addiction to medication (Philips, 1988). Increased pain tolerance is an important resilience factor, which helps patients to alleviate the suffering that often comes with pain (Roebuck et al., 2018; Turk and Okifuji, 2002).
As literature suggests, since pain cannot be avoided, it is highly important to investigate it in terms of tolerance (Crombez et al., 1999). In the cognitive behavioral framework, the ability to tolerate discomfort has been defined as frustration tolerance (Ellis, 1962; Leahy, 2015). Ellis (1962) also refers to this as nonawfulizing about badness (Ellis, 1962). A high level of frustration tolerance is considered a determiner of resilience, while low levels of frustration tolerance and high levels of awfulizing/catastrophizing are predictive of large areas of psychopathology (Dryden, 2005).
Pain tolerance and pain-related anxiety are two of the most studied outcomes in patients who suffer from pain. Pain-related anxiety is one of the most frequent emotions associated with pain (Asmundson and Katz, 2009). It has been claimed that the feelings of anxiety become such a fundamental part of pain experience that patients may have difficulty differentiating between the two (Philips, 1988; Vlaeyen and Linton, 2000). Given the impact of both pain tolerance and pain-related anxiety on patient’s well-being, physical status, and mental health (Vlaeyen and Linton, 2000), research has investigated the cognitive and emotional predictors underlying these constructs. Pain catastrophizing, anxiety, and response expectancies are three of the most studied variables (Wang et al., 2016; Vlaeyen and Linton, 2000).
Pain catastrophizing, anxiety, response expectancies, and pain intensity
Pain catastrophizing is defined as a maladaptative cognition, comprising three different dimensions (magnification, rumination, helplessness), measured by Pain Catastrophizing Scale (PCS; Sullivan et al., 1995). Considerable research has shown that pain catastrophizing is a significant determiner of pain experience and pain-related outcomes (Linton, 2013). Relationships between pain catastrophizing, pain intensity, and pain tolerance have been shown in several clinical populations. It is associated with decreased pain tolerance and higher pain severity among patients with rheumatoid arthritis, with more severe and widespread pain, with higher levels of emotional distress among individuals with fibromyalgia and scleroderma, and with disability up to 6 months postoperatively in patients who have had knee surgery for osteoarthritis (see Edwards et al., 2006).
Also, anxiety is associated with pain intenity (Lauriola et al., 2019), pain tolerance as a response to pain intensification, prolonged elevation of pain levels, or anticipation of increased pain (Philips, 1988; Wade et al., 1990). Studies on clinical population suggest that preoperative psychological distress has a significant impact on postsurgical recovery, and it is associated with poor clinical outcomes (such as: high levels of pain intensity and emotional distress) after surgery to the hip, knee, and lumbar spine (Duivenvoorden et al., 2013; Pakarinen et al., 2014). Specifically, higher levels of preoperative state anxiety are associated with increased postoperative pain intensity (Hsu et al., 2005; Tang and Gibson, 2005), which may significantly influence pain tolerance (Masedo and Esteve, 2007). It is generally accepted that pain catastrophizing and anxiety are theoretically distinct from one another (Benore et al., 2015; Eccleston et al., 2005). Also, there is evidence to suggest that the two, although associated, have distinct roles in pain. For example, pain catastrophizing has been shown to predict the unique variance in functional disability over trait anxiety in a community sample of children (Vervoort et al., 2010) and the variance in pain and disability over negative affectivity in a small clinical sample of youths with chronic pain (Vervoort et al., 2010).
Given their impact on pain intensity, response expectancies emerged as a predictor of pain-related outcomes, with an important contribution in the understanding of pain experience (Sullivan et al., 2001). It has been claimed that nonvolitional responses, including pain reactions, are impacted by response expectancies (David et al., 2004; Montgomery et al., 2007). They were defined as the expectation that a nonvolitional response will occur, as a function of a behavior or a specific stimulus (David et al., 2004; Kirsch, 1985). More specifically, response expectancies regarding the appearance of a nonvolitional response are sufficient to create nonvolitional outcomes, such as memory reports, pain perception, responses to psychotherapy, sexual arousal, asthmatic responses, and mood (Kirsch, 1985). They are not mediated by other psychological variables (David et al., 2004; Kirsch, 1985). For example, in case of placebo effects, the effects of hypnotic suggestion, and the effects of pharmacological agents and medical interventions were not identified any psychological mechanisms to explain their impact on behavior (Kirsch, 1985; Montgomery et al., 2007). Moreover, response expectancies are self-confirming and might be influenced by verbal instructions, such as the informations regarding the effect that a procedure is expected to have (Baker & Kirsch, 1991; Kirsch, 1985).
Moreover, response expectancies are self-confirming, might be influenced by verbal instructions such as the informations regarding the effect that a procedure is expected to have (Baker & Kirsch,1991; Kirsch,1985). Also, the expected pain level is correlated with the experienced pain level (Kirsch, 1985). In chronic pain, response expectancies and pain catastrophizing influence the large individual differences that can be observed in the covariation of daily mood and daily pain (Linton and Götestam, 1985; Moldofsky and Chester, 1970; Riddle and Smith, 2019). Specifically, response expectancies for pain tolerance are predictive of pain intensity and the level of pain tolerance (Baker and Kirsch, 1991; Dolce et al., 1986; Locher et al., 2019). Thus, response expectancies might potentially explain the relationships between pain catastrophizing/state anxiety and pain tolerance/pain-related anxiety, although little is known about how they influence these relationships in aversive contexts.
Aversive versus nonaversive pain contexts
The context of a noxious stimulus is highly relevant to pain-related outcomes as it may activate dysfunctional beliefs (David et al., 2010; Merskey and Bogduk, 1994), such as pain catastrophizing. According to the literature, dysfunctional beliefs need a cue to become manifest (Beck et al., 1979), and once activated, they may have a significant impact on behavioral and emotional responses (David et al., 2010; Szentagotai and Jones, 2010). Nevertheless, aversive pain contexts are more likely to activate cognitive vulnerabilities (Ingram and Luxton, 2005); (see Figure 1 and Figure 2).
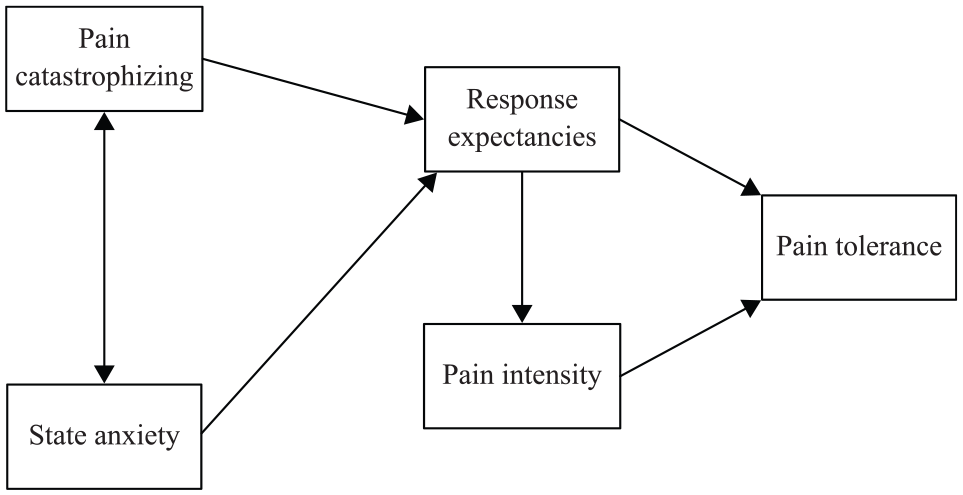
Graphic representation of paths predicting pain tolerance in aversive/neutral condition.

Graphic representation of paths predicting pain-related anxiety in aversive/neutral condition.
The path analytic model
The impact of pain catastrophizing and anxiety on response expectancies may be explained by the history of heightened pain experience, in different contexts, of individuals who catastrophize (Sullivan et al., 2001). These patients may develop expectancies of future pain experiences or may develop specific beliefs regarding the aversiveness associated with pain related contexts (Locher et al., 2019; Sullivan et al., 2001). Therefore, prior experience with pain, or associated beliefs about painfull situations of these patients may lead to expectancies that aversive contexts will bring a high degree of pain, which may impact pain tolerance (Baker and Kirsch, 1991) and distress (Sullivan et al., 2001). Therefore, whether on the basis of prior painful experience, or associated beliefs about pain-eliciting situations, individuals who catastrophize may expect that future pain-eliciting situations will be associated with a high degree of pain, which may impact pain tolerance (Baker and Kirsch, 1991) and distress (Sullivan et al., 2001). Also, literature suggests that response expectancies would predict pain tolerance and pain-related anxiety via pain intensity. The research shows that response expectancies are very good predictors of both positive (relaxation) and negative (e.g. pain intensity or distress) nonvolitional outcomes in clinical and nonclinical samples (David et al., 2006). The role of response expectancies as a psychological mechanism for producing nonvolitional outcomes, such as pain perception, memory reports, responses to psychotherapy, sexual arousal, asthmatic responses, and mood is known in the literature (see Baker and Kirsch, 1991; David et al., 2004; Montgomery et al., 2007).
Because response expectancies tend to be self-confirming (David et al., 2004), as it is amply documented by the vast literature on placebo effects, response expectancies impact pain intensity, while pain intensity influence pain tolerance. Pain tolerance may be influenced by targeting response expectancies for pain tolerance and pain intensity level. Similarly, placebos reduce self-reported pain intensity and enhance pain tolerance (Kirsch, 1985; Locher et al., 2019).
We hope that by expanding the pathways that explain pain tolerance and pain-related anxiety, and by exploring possible common predictors of both sensorial and affective dimensions of pain, to facilitate a better understanding of the processes involved in pain and emotion. As literature indicated (Le Borgne et al., 2017; Linton, 2013), investigating the ways in which cognitive and emotional factors interact in specific conditions might increase the effectiveness of interventions for pain management.
The transdiagnostic model
Since pain and comorbid emotional distress appear to be inseparable processes, a transdiagnostic perspective would facilitate the flexibility in delivery of psychotherapeutic interventions (Linton, 2013). Psychological interventions are useful for patients with acute pain, who follow painful medical preocedures, or for patients who developed chronic pain (Gatchel et al., 2018). As literature suggests, a painful event might activate specific beliefs about pain and threat, which activate negative dysfunctional emotions (David et al., 2008; Merskey and Bogduk, 1994), with a negative impact on recovery (see Asmundson and Katz, 2009). For example, patients with depression are three times less likely than nondepressed patients to adhere to treatment recommendations (DiMatteo et al., 2000). Also, patients who reported depression symptoms reported significantly more pain (Koechlin et al., 2018), while the presence of persistent pain significantly increases the risk of future depression, major depression or anxiety, and vice versa (Tunks et al., 2008). Bair et al. (2003) found that the prevalence of major depression in patients with pain ranged between 13 percent and 85 percent. Likewise, people with chronic pain frequently report significant expressions of fear and anxiety in both community and treatment-seeking samples (Asmundson et al., 2008). Conversely, the prevalence of pain among patients with major depression ranged between 15 percent and 100 percent (Bair et al., 2003). The relation between pain and emotion is bidirectional (Edwards et al., 2006). Therefore, hospitalized patients who follow painful procedures could benefit the most from interventions addressed to the management of dysfunctional emotions and pain, preventing them from developing chronic pain, disability, or psychopathology (Nicholls et al., 2018).
As previously mentioned, the transdiagnostic approach assume that certain psychological processes contribute in a causal way to the development and maintenance of symptoms and suggest that they are underpinned by common psychological mechanisms (Le Borgne et al., 2017). From this perspective, it would be useful to identify the adaptive strategies and to facilitate the integration of psychotherapy into diverse health care settings (Dindo et al., 2017). In addition, the transdiagnostic model for pain and emotion may facilitate crossover treatments, namely treatments whose efficacy has been demonstrated for more than one of a cluster of component symptoms, and which may be beneficial in treating the symptom cluster as a whole (Kwekkeboom et al., 2010). Where there is a broad spectrum of effects on other symptoms in the cluster, Kwekkeboom et al. (2010) noted that (1) the symptoms may share a common etiology, (2) diminishing one symptom may prevent exacerbation of the others, and (3) single interventions may be indicated for more than one symptom. As Kwekkeboom et al. (2010) noted, the generation of “crossover” treatments has the possible benefit of using a single intervention to simplify treatment, which may reduce costs.
Overview of the present study
The impact of anxiety and pain catasatrophizing has been investigated in separate models, without considering the shared variance (Benore et al., 2015; Eccleston et al., 2005). Therefore, we need to clarify the interconnected relations between the variables using a single model for each outcome of interest, investigating whether pain catastophizing and anxiety are statistically distinct, or whether they are uniquely related to pain-related outcomes (see Tran et al., 2015). Moreover, the relationships between pain catastrophizing/state anxiety and pain tolerance/pain-related anxiety have been extensively investigated in the literature, but the mechanisms behind these associations remain poorly understood.
Therefore, the present study aims to expand on the pathways that explain pain tolerance and pain-related anxiety by exploring pain catastrophizing and state anxiety as possible predictors. Drawing on the previous findings, response expectancies for pain tolerance and their impact on pain intensity were investigated as potential mechanisms. By identifying the paths that may explain both pain tolerance and pain-related anxiety, we will take a step toward a transdiagnostic perspective for pain and anxiety (Linton et al., 2016). Given the need for a threatening activator for dysfunctional cognitions (Beck et al., 1979; David et al., 2010), we manipulated the threat value of the pain associated with cold-pressor task using verbal information about its potential consequences. We expected that participants in aversive condition would report higher levels of state anxiety than participants included in neutral condition. We also expected that in aversive condition, pain catastrophizing and state anxiety would indirectly predict pain tolerance and pain-related anxiety via response expectancies. In addition, we expected that response expectancies for pain tolerance would indirectly predict pain tolerance and pain-related anxiety via pain intensity.
Finally, the assessment of distorted cognitions in aversive contexts is a major concern of the literature. Research highlights that state measures of pain catastrophizing are more valid than trait measures, which may not adequately capture the variance in reported pain (Beck et al., 1979). Literature also suggests that aversive pain contexts represent one possible solution for highlighting state pain catastrophizing in experimental studies (Lin et al., 2013), thereby increasing the generalizability of results (see Polit and Beck, 2010).
Methods
Participants
In total, 78 undergraduate students were included in the study. The participants ranged in age from 19 to 33 years (mean = 21.74). Individuals suffering from medical conditions associated with persistent pain (such as migraine, headache, and back pain) and those with other conditions that might be adversely affected by pain procedure (e. g. cardiovascular problems, previous episodes of frostbite, etc.) were not considered for participation. All participants signed a written informed consent.
Procedure
Experimental manipulation of anxiety
Participants were randomly assigned to one of two experimental conditions: (1) the aversive condition (n = 41) and (2) the neutral condition (n = 37). Written information regarding the task was given. Participants were told that important information about the task will be given, and they were told to read carefully before signing the informed consent. Participants from the aversive condition received written information which informed them that in some extreme cases, the cold-pressor task could be dangerous and might result in a serious degeneration of the immersed hand, while those in the neutral condition were told that the task was very similar to searching for a drink in a freezer and that it would not result in any physical injury. After signing the informed consent, participants were then instructed to place their hand into the water and to keep it immersed for as long as they could tolerate. After 5 minutes, participants were told to extract their hand. The data were screened for missing values and outliers, as these can have a significant impact on path analyses. For both experimental conditions, the path analytic model was tested separately for each of the main outcome in the study, namely pain tolerance and pain-related anxiety.
Measures
Pain catastrophizing
The PCS ( Sullivan et al., 1995) is a 13-item self-report measure of pain catastrophizing that assesses the negative thoughts associated with pain. The PCS measures three dimensions of catastrophizing: rumination, magnification, and helplessness. Participants rate their feelings of pain on a five-point Likert-type scale (where 0 is “not at all,” and 4 is “all the time”). PCS scores range from 0 to 52, where higher scores indicate more pain catastrophizing. In the present study, the Cronbach’s alphas were as follows: full scale, α = .87; helplessness, α = .78; magnification, α = .63; rumination, α = .82.
State anxiety
The State-Trait Anxiety Inventory (STAI; Spielberger et al., 1983) is a commonly used measure of trait and state anxiety. The most popular version has 20 items for assessing trait anxiety and 20 for state anxiety. We used the items from state anxiety subscale. Higher scores indicate greater anxiety. Internal consistency coefficients for the scale range from .86 to .95; test–retest reliability coefficients over a 2-month interval range from .65 to .75 (Spielberger et al., 1983). Considerable evidence attests to the construct and concurrent validity of the scale (Spielberger, 1989). Studies have also shown that scores can vary with changes in health and other individual characteristics (Shewchuk et al., 1998).
Response expectancies for pain tolerance
Participants were asked to rate on a visual analogue scale (VAS), the level of pain tolerance they expected to have during the cold-pressor task by marking a line between 0 (no pain tolerance) and 100 (extreme pain tolerance).
Example of item: Please rate how much pain tolerance you are expecting to have during cold-pressor test.
Pain-related anxiety
Participants were given a VAS scale for completion after cold-pressor procedure. Reports of the anxiety they experienced were collected by marking a line between 0 (no anxiety) and 100 (extreme anxiety).
Pain measures
Pain tolerance was the total time, in seconds, that the participant’s hand was immersed in the water, minus pain threshold time.
Pain threshold was determined by asking participants to report the moment when they began to feel pain or discomfort. The time, in seconds, between the start of the immersion and the reporting of the pain was recorded as the pain threshold.
Pain intensity was the pain experienced during the cold-pressor task, measured using a VAS, which ranged from 0 (no pain) to 100 (extreme pain). Participants were asked to mark a line between 0 and 100 to suggest the intensity of pain. Example of item: Please rate the level of pain intensity you experienced during experimental procedure.
Apparatus
A cold-pressor apparatus was used to induce pain. The apparatus consisted of a refrigeration unit that cooled constantly circulating water in an insulated container measuring 30 cm × 40 cm × 30 cm. The water temperature was maintained at 5°C. Water at room temperature (21°C) was used to standardize the temperature of the hand before immersion in the cold water container. The apparatus was a Refrigerated Bath Circulator, Model JSRC-13C.
Statistical analyses
Student’s t-test was used to evaluate whether the experimental manipulation influenced state anxiety before pain induction. Path analysis was used to identify the model that was the most predictive for pain tolerance and pain-related anxiety. We found one model that fit the data well. This model was tested for each experimental condition, considering pain tolerance and pain-related anxiety as separate outcomes. This statistical method is an extension of multiple regression. Unlike multiple regression, which focusses on the prediction of a single dependent variable, path analysis provide the posibility to investigate more than one dependent variable (Schreiber, Nora, Stage, Barlow, & King, 2006). It is a usefull statisical method in the research of bio-psycho-social relationships because it assess multiple relations within a model, offering a theoretical, directional, and a predictive model of those relationships, (Schreiber et al., 2006). It presents a theoretical, directional relationship (both direct and indirect) between variables, and as such, offers a predictive model of those relationships (Schreiber et al., 2006). In this study, the hypothesized model was tested in an exploratory manner, based on the contributing variables, namely pain tolerance and anxiety. Following the recommendations of Weston and Gore (2006), model-data fit was examined using several fit indices, including the comparative fit index (CFI), the nonnormed fit index or Tucker–Lewis index (TLI), the root mean square error of approximation (RMSEA), and the standardized root mean square residual (SRMR). Statistical significance of the path coefficients was also analyzed. We used R (R Core Team, 2012) and Lavaan Package (Rosseel, 2012) to perform these analyses.
Results
Descriptive analyses
We had 41 participants in the aversive condition and 37 participants in the neutral condition. They were undergraduate psychology students, in the second and third year of study. Means and standard deviations were calculated for each measure (see Table 1).
Descriptive statistics.
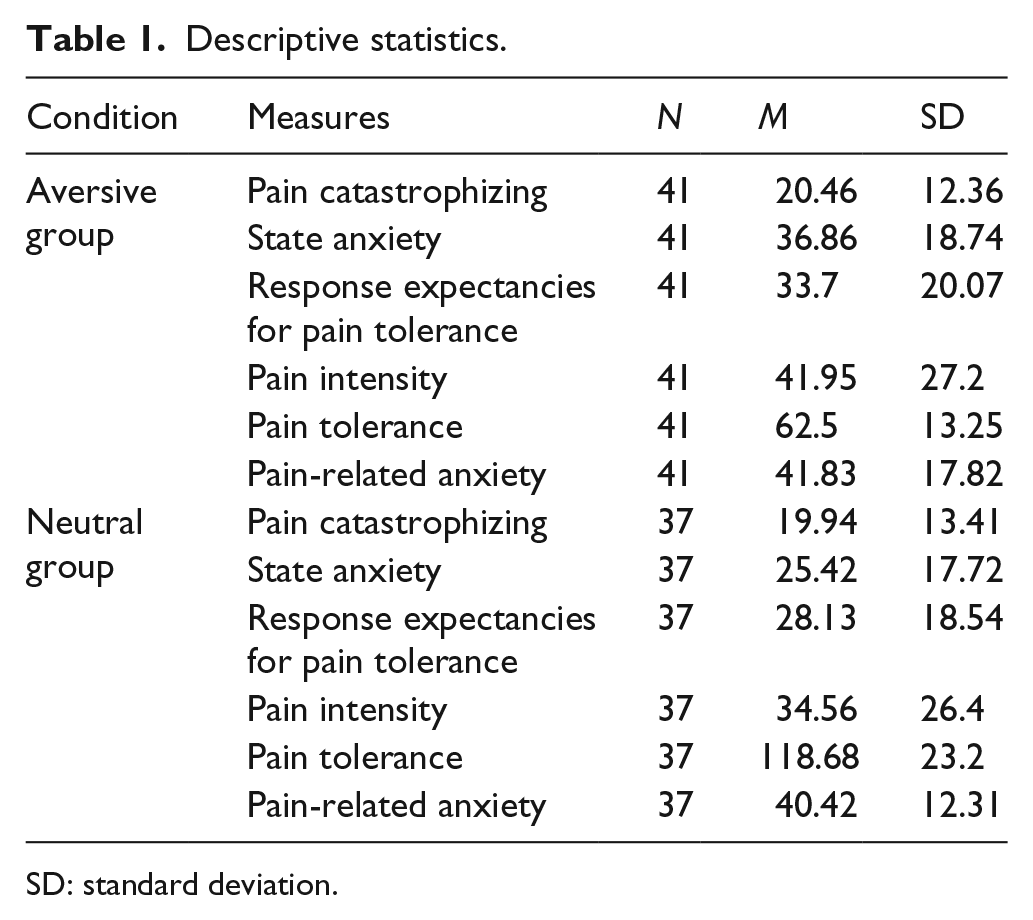
SD: standard deviation.
Manipulation check
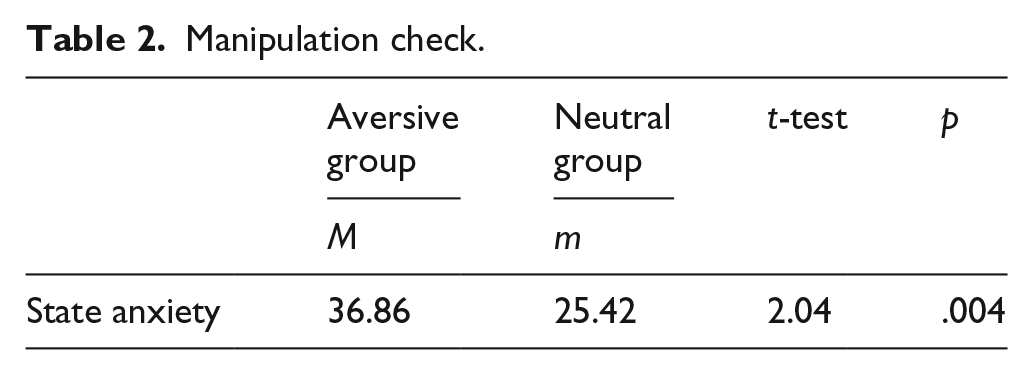
Our results showed that the experimental manipulation was effective. There were significant differences between conditions on state anxiety level (t = 2.04, p < .05; see Table 2).
Manipulation check.
The path model for predicting pain tolerance
Various fit indices were used to assess the adequacy of the path models. The goodness-of-fit index (GFI) of 0.993 indicated an excellent fit. The root mean square residual (RMSEA) of 0.024 was within the expected range of unaccounted variance (<0.05) and represented a high level of closeness of fit for the model. The Tucker–Lewis coefficient and CFI were 1 for both aversive and neutral conditions, also indicating a good fit.
Direct and indirect paths for pain tolerance: aversive vs. neutral condition
The first path analysis model was constructed to investigate whether pain catastrophizing and state anxiety are indirect predictors of pain tolerance. For the aversive condition, with the exception of one path, all the estimated direct paths were statistically significant. Pain catastrophizing had a direct effect on response expectancies (β = 3.29, p < .005). State anxiety had a direct effect on response expectancies (β = −2.81, p < .001). Response expectancies had a direct effect on pain intensity (β = .78, p < .000). Pain intensity did not predict pain tolerance (β = −2.86, p < .68). Response expectancies had a direct effect on pain tolerance (β = 2.90, p < .009). Pain catastrophizing did not predict pain tolerance via response expectancies (β = −.25, p < .57). In contrast, state anxiety significantly predicted pain tolerance via response expectancies (β = −0.91, p < .003). A significant indirect path was also found from response expectancies to pain tolerance via pain intensity (β = −2.25, p < .004).
For the neutral condition, the only significant paths were from state anxiety to response expectancies (β = −1.05, p < .003) and from response expectancies to pain intensity (β = .71, p < .000; see Figures 3 and 4; Table 3).

Graphic representation of paths predicting pain tolerance in neutral condition.

Graphic representation of paths predicting pain tolerance in aversive condition.
Direct and indirect paths for predicting pain tolerance.

CI: confidence interval.
The path model for predicting pain-related anxiety
Various fit indices were used to assess the adequacy of the path model for the aversive and the neutral condition. For aversive condition, the GFI was 0.983, indicating an excellent fit. The RMSEA was 0.024, the Tucker–Lewis coefficient was 0.93, and the CFI was 0.98, also indicating a good fit. In the case of the neutral condition, the GFI was 0.951, RMSEA was 0.000, indicating a good fit, while the TLC was 0.27 and the CFI was 0.71, which indicates a medium to low fit with the model.
Direct and indirect paths for pain-related anxiety: aversive vs. neutral condition
We analyzed whether pain catastrophizing and state anxiety were indirect predictors of pain-related anxiety. For the aversive condition, with the exception of one path, all the estimated directs paths were statistically significant. Pain catastrophizing had a direct effect on response expectancies (β = .36, p < .006). State anxiety had a direct effect on response expectancies (β = .26, p < .001). Response expectancies had a direct effect on pain intensity (β = 1.13, p < .000). Pain intensity predicted pain-related anxiety (β = −.28, p < .000). Response expectancies did not predict pain-related anxiety (β = −.004, p < .980).
Pain catastrophizing was not a significant predictor of pain-related anxiety via response expectancies (β = −.02, p < .708). In contrast, a significant indirect path was found from state anxiety to pain-related anxiety via response expectancies (β = −.16, p < .003). A significant indirect path was also found from response expectancies to pain-related anxiety via pain intensity (β = −.32, p < .009).
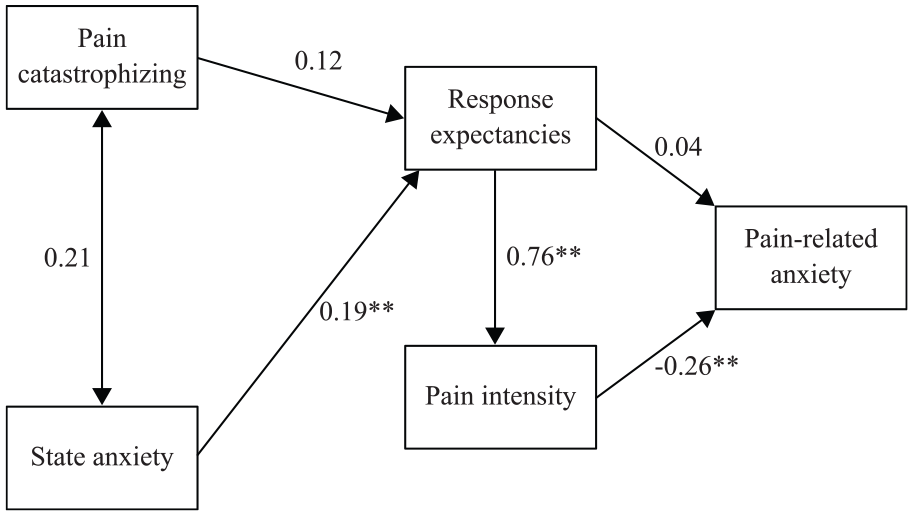
For the neutral condition, the paths from pain catastrophizing to response expectancies and from response expectancies to pain-related anxiety were insignificant. The direct path from state anxiety to response expectancies was significant (β = .19, p < .002). The direct path from response expectancies to pain intensity was significant (β = .76, p < .000). The path from pain intensity to pain-related anxiety was also significant (β = −.26, p < .000), while the only significant indirect path was from response expectancies to pain-related anxiety, via pain intensity (β = −.20, p < .005; see Figures 5 and 6; see Table 4).

Graphic representation of paths predicting pain-related anxiety in neutral condition.
Graphic representation of paths predicting pain-related anxiety in aversive condition.
Direct and indirect paths for predicting pain-related anxiety.

CI: confidence interval.
Discussion
The aim of the present study was to investigate whether pain catastrophizing and state anxiety are indirect predictors of pain tolerance and pain-related anxiety. Response expectancies for pain tolerance were tested as a mechanism of both pain tolerance and pain-related anxiety. We also tested whether response expectancies for pain tolerance indirectly predict pain tolerance and pain-related anxiety, via pain intensity. Two different activating contexts (aversive and neutral) were experimentally induced. The threat value of cold-pressor pain was manipulated using written information about the task and the procedure was performed by healthy/pain-free volunteers. Our results showed that the experimental manipulation was successful: participants in the aversive condition reported significantly higher levels of anxiety prior to the task. The proposed path model, which was based on a priori considerations and past research, fit the data well. Our results demonstrate that aversive contexts have an important influence on pain tolerance and pain-related anxiety. Significant paths were found for the aversive condition, separately predicting pain tolerance and pain-related anxiety. Our results indicate that these outcomes are influenced by an aversive perception of the task, which activates threat anxiety and distorted cognitions (Robinson et al., 2013). The path analytic model shows that for the aversive condition, response expectancies for pain tolerance significantly predict pain intensity and pain tolerance, while in neutral condition they predict only the intensity of the pain. Interestingly, response expectancies were not the mechanism for the relationship between pain catastrophizing and pain tolerance/pain-related anxiety, but instead they mediated the relationship between state anxiety and pain tolerance/pain-related anxiety. Pain intensity also mediated the relationship between response expectancies and pain tolerance/pain-related anxiety, in separate models. These results emphasize the findings described in literature, namely that response expectancies predict nonvolitional responses (David et al., 2006; Kirsch, 1985). Nevertheless, in aversive contexts, response expectancies may also be expressed in the form of behavioral responses, such as pain tolerance (Dolce et al., 1986). We have therefore demonstrated that they are relevant mechanisms which may influence the level of perceived pain, pain tolerance, and pain-related anxiety.
In the aversive condition, pain catastrophizing significantly predicts pain tolerance and pain-related anxiety, while in a neutral context it is not predictive. Therefore, as the previous literature suggests, pain catastrophizing might represent a latent construct, requiring sufficient activation in order to exert its effects (Edwards et al., 2006). These results confirms that a negative activating event may highlight cognitive vulnerabilities or may emphasize latent maladaptive thoughts in need of a cue to become manifest (Beck et al., 1979). Catastrophic or dysfunctional beliefs need threat, real or inferred, to elicit emotional or behavioral responses (Dryden, 2005; Vlaeyen and Linton, 2000). Since context may activate underlying beliefs, the literature suggests that it is strongly relevant to pain-related outcomes (Merskey and Bogduk, 1994). Once activated, maladaptive beliefs may also have a significant impact on behavioral and emotional responses (Szentagotai and Jones, 2010). Catastrophizing is one of four irrational beliefs, a main mechanism, and an important target for Cognitive Behavioral Therapy (CBT) interventions in broad area of psychopathology (David, 2003; David et al., 2008; Dryden et al., 2010; Garratt et al., 2007). Pain catastrophizing have also been treated as an index of change of dysfunctional cognition and represents a therapeutic mechanism by which CBT can reduce pain and improve functioning (Burns et al., 2012).
In our study, state anxiety predicted pain tolerance and pain-related anxiety by the way of response expectancies, with higher levels of anxiety predicting lower response expectancies for pain tolerance. These results replicate previous findings described in the literature, which state that the mechanism through which anxiety perpetuates its effect is based on response expectancies (Clark and Beck, 2010). As recent findings suggest, these are the core mechanisms of anxiety (Rief et al., 2015), enhanced by avoidance cognitions and dysfunctional behaviors (Sibrava and Borkovec, 2006; Stapinski et al., 2010).
For the advance in the field, research suggests that identifying the mechanisms that would afford a greater understanding of both problems would facilitate the progress concerning the theoretical understanding and treatment of pain and emotion (Linton, 2013). Also, given the lack of a clear theoretical understanding of the processes involved, the treatment of these comorbid factors needs more research (Le Borgne et al., 2017). Our study showed that cognitive and emotional factors are closely linked with pain tolerance and pain-related anxiety, especially in aversive condition. Also, these results highlight that pain tolerance and pain-related anxiety share common mechanisms when threat is perceived. As previously stated, in order to add data to the transdiagnostic model for pain and emotion, we need to emphasize certain psychological processes contributing in a causal way to the development and maintenance of various symptoms observed across patients (Le Borgne et al., 2017). Therefore, our data may add significant support for the transdiagnostic model of pain and emotion.
Although CBT is a theoretical approach with a powerful empirical support, efficacious either alone or as an adjunct to medication, and highly efficient regarding relapse and recurrence (Beck and Dozois, 2011; David et al., 2018), there is still a strong need to address specific cognitive factors in order be more effective in reducing certain emotional dysfunctionalities (Mehl et al., 2015). Thus, literature encourages a better understanding of the involved cognitive factors and mechanisms of change assumed to increase the effectiveness of intervention packages (Clark and Beck, 2010). Our study investigated possible therapeutic targets underlying the process of patient adaptation to aversive circumstances. From a CBT perspective, they consist in patient cognitions and behaviors (see David et al., 2008). Our study confirms that for patients who suffer from acute pain, thoughts/cognitive processes, emotions, and behaviors are interconnected (Nicholls et al., 2018). Therefore, adaptive ways of thinking, feeling, and behaving in threatening situations can be achieved to help patients cope with pain and dysfunctional emotions related.
Theoretical and clinical implications
A patient’s personal experience of pain in aversive contexts may be explained by pain catastrophizing, state anxiety, and response expectancies for pain tolerance. The findings of the present study encourage a transdiagnostic perspective for treating pain-related outcomes, such as pain tolerance and pain-related anxiety. The transdiagnostic model promotes the transfer of practical and theoretical advances between disorders, facilitates the transfer of research findings to a broader range of disorders, and provides an explanation for the comorbidity observed in clinical practice (Harvey et al., 2004). By identifying the common features driving both problems, the transdiagnostic model aims to better understand the procesess involved (Linton, Flink, Schrooten & Wiksell, 2016). Our study found similar mechanisms of pain tolerance and pain-related anxiety in aversive condition. As previously mentioned, it is relevant to highlight the overlapping features or common maintaining mechanisms in order to support a transdiagnostic view (McHugh et al., 2009). Our results also provide more empirical support for the use of the CBT approach with patients who suffer from acute pain by showing the association between cognitive/emotional factors and clinically relevant aspects, and the path through which they affect pain outcomes. Also for these patients, changing dysfunctional evaluations may be considered an important mechanism for changing dysfunctional outcomes (see David and Hofmann, 2013; Nicholls et al., 2018). Numerous studies have shown pain catastrophizing to be associated with dysfunctional beliefs regarding the ability to cope with the difficulties caused by the experience of pain, with the exaggeration of problems, and with ignoring the positive aspects of the situation, such as the availability of resources (Wojtyna, 2012), resulting in fear of pain, depression, and disability (Leeuw et al., 2007).
Our results also highlight that framing painful events in terms of threat may increase the level of reported anxiety (Cameron, 2003), while an interaction between threat and distorted cognitions could lead to emotional and behavioral difficulties (Beck et al., 1979). Moreover, such framing may influence an individual’s behavioral decisions and pain tolerance (Payne et al., 1992). It is important to emphasize the effect of information communication in health-threatening situations, since numerous studies indicate that the behavioral and emotional outcomes of the patient are influenced, on one hand, by their underlying cognitions, and on the other hand, by the general framing offered by health care providers (Krishnamurthy et al., 2001). Nevertheless, screening for the cognitive and emotional predictors of dysfunctional health-related outcomes is a low-cost method by which individuals who might benefit the most from psychological interventions can be identified.
Nevertheless, our study has a significant impact in terms of generalizability to population who suffer from acute pain. As defined by Polit and Beck (2010), generalization involves drawing broad conclusions from particular instances, or making an inference about the unobserved based on the observed. The statistical generalization, namely the applicability of research findings beyond the particular people who took part in a study, is met in our study due to the research design and experimental manipulation. Although our results may not be generalized to clinical patients (mainly because of the health status of our sample-healthy population), it may be extrapolated to healthy patients who are following specific threatening procedures (acute pain), since our data showed that the aversiveness of the task was successfully induced and different results followed.
Also, random distribution of participants is another important aspect of generalization. The best strategy for achieving a representative sample is to use probability (random) methods of sampling (Polit and Beck, 2010). Nevertheless, due to the threat induction through experimental manipulation, our study supports transferability of results to patients who follow painfull medical procedures.
The limitations of the present research have implications for the generalizability of the findings to clinical samples. The participants were undergraduate students who were not suffering from pain-related health conditions. The applicability of the results to patients suffering from a clinical condition or chronic pain is thus uncertain. The second issue is one of measurement. Although using a visual analogue scale to evaluate pain-related anxiety and response expectancies is a common practice, it has several limitations (Wewers and Lowe, 1990) which may have influenced our results. First limit addressed by Wewers and Lowe (1990) is concerning the subject’s ability to conceptually understand the method itself, although the VAS is described as being independent of language. It includes the ability of the subject to conceive the unit of the line as a representation of a personal perception of an abstract concept. Therefore, any mark along the line between these two extremes is totally dependent upon the subject’s unique interpretation (Wewers and Lowe, 1990). The second limit underlined by the authors mentioned above is based on the inaccuracy of reproduction of the instrument due to the distortion that often appear on Xeroxing, known to distort the length of the line. In addition, there may appear some effects eye-hand coordination (Wewers and Lowe, 1990). Furthermore, we used only observational and self-report data, which may result in under-reporting of the main outcomes. Future studies should also focus on physiological measures of the sensorial characteristics of pain and pain-related anxiety in order to gather more complex and valid information (Sweet and McGrath, 1998).
Conclusion
As literature indicated (Le Borgne et al., 2017; Linton, 2013; Linton et al., 2016), there is a strong need to increase the effectiveness of interventions for pain management. Our study identified mutual factors driving both problems, which may afford expanding the pathways that explain pain tolerance and pain-related anxiety. By exploring possible common predictors of both sensorial and affective dimensions of pain, we ultimately aimed to facilitate a better understanding of the link between pain and emotion, as well as improving knowledge of the processes involved. In aversive condition, pain catastrophizing significantly predicts pain tolerance and pain-related anxiety, while in a neutral context it is not predictive. Therefore, as the previous literature suggests, pain catastrophizing might represent a latent construct, requiring sufficient activation in order to exert its effects (see David et al., 2010; David et al., 2008; Edwards et al., 2006). Nevertheless, our study may add significant input for populations who are following aversive procedures and acute pain, emphasizing the mechanisms involved in pain tolerance and pain-related anxiety.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.