
Abstract
This study examined the effect of implementation intentions on use of dental chewing gum. A total of 80 participants reported intentions to chew gum, read information about the benefits of dental gum, reported intentions again, and formed implementation intentions relating to gum use (experimental group) or solved word puzzles (control group). Seven days later, they reported the amount chewed. Results showed that among those motivated to chew gum, implementation intentions significantly increased the total amount chewed. Time 1 intentions were more highly correlated with behaviour than time 2 intentions. Further research is needed to establish the effectiveness of implementation intentions in dental settings.
Although oral health has improved over the last decade, a significant proportion of the population still suffer from poor dental health (Marcenes et al., 2013; White et al., 2012). For example, in the United Kingdom, approximately 31 per cent of individuals have dental caries, with those from lower socioeconomic backgrounds tending to have higher levels (White et al., 2012). Chewing dental gum for around 20 minutes after meals has been shown to help prevent tooth decay (Deshpande and Jadad, 2008; Dodds, 2012) and, where used as an adjunct to brushing, can also lead to small but significant reductions in plaque (Keukenmeester et al., 2014
The current study looks at whether implementation intentions could be used to increase the use of dental chewing gums. Implementation intentions are where a person specifies when, where and how they will perform a particular behaviour, linking the ‘when’ and ‘where’ to the ‘how’ using an ‘If … then …’ structure (Gollwitzer, 1993, 1996, 1999; Oettingen et al., 2000). For example, ‘If I am in the kitchen and have just finished eating my lunch, then I will select a piece of fruit to eat for dessert’. Implementation intentions are thought to work by helping people more easily identify good opportunities to act when they encounter them (Aarts et al., 1999) and also by increasing the extent to which the behaviour is performed automatically (Webb and Sheeran, 2008). There is substantial evidence to indicate that implementation intentions can be a very effective way of changing behaviour (Gollwitzer and Sheeran, 2006).
However, a number of factors have been shown to moderate the effects of implementation intentions. These include the ease or difficulty of the target behaviour (Gollwitzer and Brandstätter, 1997; Prestwich et al., 2015), the self-regulatory ability of the individual (Allan et al., 2013; Gollwitzer and Sheeran, 2006) and the degree to which the current behaviour is habitual (Maher and Conroy, 2015; Webb et al., 2009). There is also evidence to show that the effects of implementation intentions are moderated by intentions; specifically, implementation intentions will only be helpful when the individual is motivated to perform the behaviour (Prestwich et al., 2003; Prestwich and Kellar, 2014; Van Osch et al., 2008). The influence of such variables means we cannot assume that implementation intentions will be useful for all behaviours and all populations.
As far as we are aware, no other studies have examined the effects of implementation intentions on use of dental gum. The most closely related studies are those that have examined effects on dental flossing. Two studies have found implementation intentions to be helpful at increasing flossing among those who are motivated to floss (Orbell and Verplanken, 2010; Schüz et al., 2009) but the third study failed to find any effects (Lavin and Groarke, 2005). However, dental gum differs from flossing since flossing is typically carried out after brushing, meaning that the contextual cues (i.e. the ‘where’ and the ‘when’) are likely to remain relatively stable. By contrast, dental gum needs to be chewed after meals. Since meals are likely to vary in terms of location and type of food eaten, the cues for chewing gum will be more variable, making it more difficult to remember.
In the current study, because implementation intentions are only effective when the individual is motivated to change (Prestwich et al., 2003; Prestwich and Kellar, 2014; Van Osch et al., 2008), and because many individuals may be unaware of the benefits of dental gum, we asked all participants to read information outlining the benefits of chewing dental gum. We predicted that, among individuals who intended to chew gum, those who had formed implementation intentions would chew more gum over the subsequent week than those who had not. We measured intentions to chew gum both before and after participants read the information and expected intentions to increase as a result of the information. We also looked at the relationship between intentions and behaviour. We assumed that, consistent with social cognition models (e.g. Ajzen, 1991, 2005; Rogers, 1983), intentions would correlate with behaviour. We expected intentions expressed after participants had read the information sheet to show the strongest correlation with behaviour since these would more immediately precede the behaviour.
Methods
Participants
A total of 80 participants (60 females, 20 males) with a mean age of 26.9 (standard deviation (SD) = 6.29) years were recruited using both word-of-mouth and advertising placed in and around the university. The study was described as being about dental health behaviours. Inclusion criteria were being aged 18 years or above and accessing email on a daily basis (the latter being required for the follow-up questionnaire). Participants received course credits for taking part or simply volunteered their time. Ethical approval was provided by the City, University of London Psychology Department Research Ethics Committee, and written informed consent was obtained from all participants.
Manipulation
Participants in the experimental condition were asked to form at least five ‘if-then’ plans specifying when, where and how they would chew gum. Participants in the control condition were asked to complete a series of health-related anagrams and a health-related word search.
Measures
Background questions
Participants were asked for details of their age, gender, how often they chewed gum (rated on a scale of 1–7, anchored by ‘I never chew gum’ and ‘I chew gum every day’) and, where relevant, their reasons for chewing gum (‘Dental health reasons’, ‘Other’, ‘Both’).
Intentions
Participants’ intentions to chew gum were assessed by asking them to rate the extent to which they agreed with the statement ‘Over the next week, I intend to chew gum after eating or drinking’. Ratings were on a 7-point sale anchored by ‘Strongly disagree’ and ‘Strongly agree’.
Behaviour
Gum chewing behaviour at follow-up was assessed using three questions emailed to participants: ‘How many pieces of sugar-free gum do you have left since taking part in the study?’; ‘Of the gums that you’ve chewed since taking part in the study, how many pieces did you chew within half an hour of eating or drinking?’; and ‘How many pieces did you chew at other times?’
Procedure
Participants were alternately allocated to the experimental or control condition. They first completed the background questions before rating their intentions to chew gum. They were then given some written information on sugar-free gum and its benefits for dental health in the form of questions and answers that covered approximately two sides of an A4 page. This was followed by five written questions, included to help ensure participants engaged with the information. Participants were given 5 minutes to read the information and answer the questions. They were then given 5–7 minutes to form implementation intentions relating to chewing gum (experimental condition) or complete the word puzzles (control condition). Finally, all participants were asked to complete the intention measure for the second time and were given one 14-piece pack of sugar-free gum to take away with them and told they would be contacted via email in 7 days time. Seven days later, they were emailed the questions on their gum chewing behaviour.
Results
Participant characteristics
As shown in Table 1, participant characteristics were generally well matched across experimental and control conditions. Of the 69 participants (86%) who reported chewing gum, just 3 (4%) said they chewed it for dental health reasons, 46 (67%) said they chewed it for other reasons and 20 (29%) said they chewed it for both dental health and other reasons.
Characteristics of study participants as a function of condition.
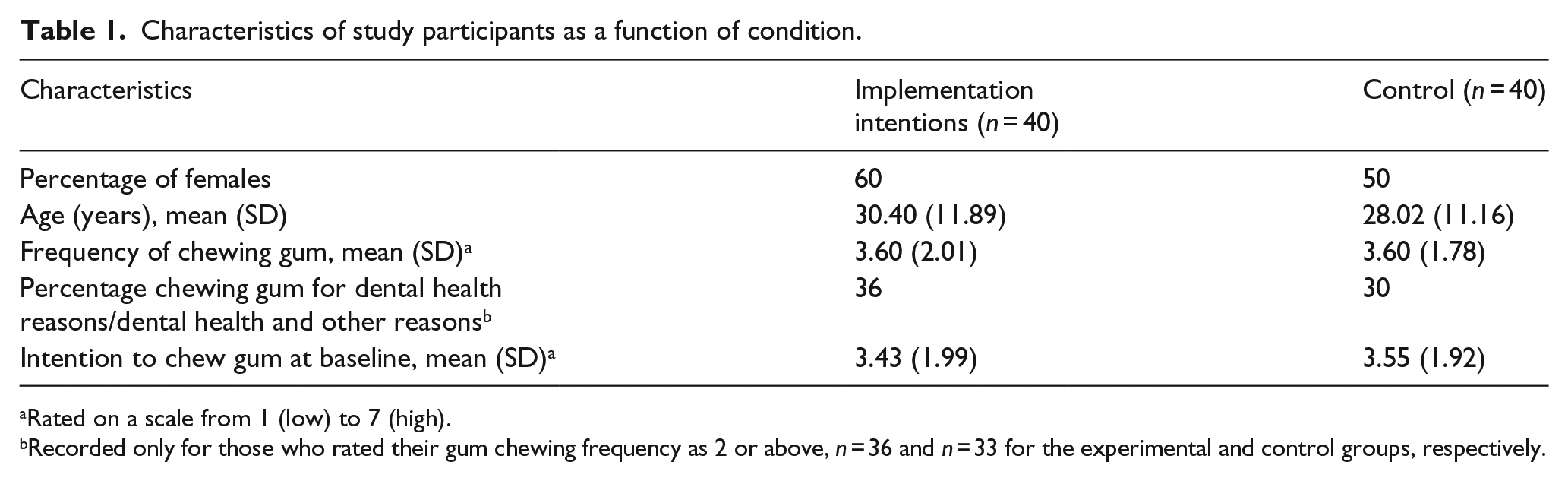
Rated on a scale from 1 (low) to 7 (high).
Recorded only for those who rated their gum chewing frequency as 2 or above, n = 36 and n = 33 for the experimental and control groups, respectively.
Relationship between intentions and behaviour
The total number of chewing gum pieces chewed was calculated by subtracting the number left in the packet from 14 (i.e. the number available). Both these data and the intentions data had non-normal distributions that could not be corrected with transformations. As such, non-parametric tests were employed. Mean intentions to chew gum were 3.49 (SD = 1.94, median = 3.50) at time 1 and 5.56 (SD = 1.57, median = 6.00) at time 2 (i.e. after participants had read the information on dental chewing gum), and a Wilcoxon signed-rank test showed that this increase was statistically significant (Z = 6.97, p < .001). However, Spearman’s correlations showed that intention at time 1 was better correlated with the total amount of gum chewed compared with intentions at time 2 (r = .37, p = .001 vs r = .30, p = .006, respectively). Intentions were not significantly correlated with gum chewed within 30 minutes of eating (r = .05, p = .66 vs r = .13, p = .24 for time 1 and time 2, respectively).
Effect of implementation intentions on behaviour
Because implementation intentions are only effective when individuals are motivated to perform the behaviour (Prestwich et al., 2003; Prestwich and Kellar, 2014; Van Osch et al., 2008), we excluded participants who reported low intentions to chew gum (i.e. who recorded ratings of 1 or 2 on the scale of 1–7). Given that intention at time 1 was a better predictor of behaviour than intention at time 2 (see above), we performed two sets of analyses, one with exclusions based on time 1 intentions (n = 52) and one with exclusions based on time 2 intentions (n = 74).
For exclusions based on time 1 intentions, total pieces of gum chewed were 10.59 (SD = 2.85, n = 27, median = 11.00) in the implementation intentions group and 8.80 (SD = 3.32, n = 25, median = 9.00) in the control group. Pieces of gum chewed within 30 minutes of eating were 6.23 (SD = 3.17, n = 27, median = 7.00) in the implementation intentions group and 4.68 (SD = 2.56, n = 25, median = 5.00) in the control group. Mann–Whitney’s tests showed that the difference was significant for the total amount of gum chewed (U = 220.50, p = .031) and showed a trend towards significance for gum chewed within 30 minutes (U = 238.50, p = .068).
For exclusions based on time 2 intentions, total pieces of gum chewed were 9.32 (SD = 3.94, n = 38, median = 11.00) in the implementation intentions group and 8.58 (SD = 3.38, n = 36, median = 9.00) in the control group. Pieces of gum chewed within 30 minutes of eating were 5.79 (SD = 3.29, n = 38, median = 6.00) in the implementation intentions group and 5.17 (SD = 2.58, n = 36, median = 5.00) in the control group. Mann–Whitney’s tests showed that these differences were not significant for the total amount of gum chewed (U = 577.50, p = .25) or for gum chewed within 30 minutes (U = 608.00, p = .41).
Across the whole sample, the total pieces of gum chewed were 9.25 (SD = 4.08, n = 40, median = 11.00) in the implementation intentions group and 8.28 (SD = 3.52, n = 40, median = 9.00) in the control group, while pieces of gum chewed within 30 minutes of eating were 5.68 (SD = 3.39, n = 40, median = 6.00) and 4.95 (SD = 2.58, n = 40, median = 5.00) in the implementation intentions and control groups, respectively. These differences were not statistically significant (U = 650.00, p = .15 vs U = 693.00, p = .30 for total gum and gum chewed within 30 minutes, respectively).
Discussion
The results of this study showed that forming implementation intentions helped motivated participants increase their total use of dental chewing gum over a 7-day period. These findings extend previous research in this area on flossing (Lavin and Groarke, 2005; Orbell and Verplanken, 2010; Schüz et al., 2009) by showing that implementation intentions can also help promote oral health care behaviours that are potentially more difficult to remember.
However, the results showed no significant effects on behaviour when motivation was indexed by intentions reported after participants had read information about dental chewing gum. It is possible that this second measure of intentions was subject to social desirability and/or demand bias and so less accurately reflected participants’ true intentions. Alternatively, this measure may have reflected more short-lived, less stable intentions, formed in response to the information that had just been read. In the absence of repeated motivational targeting, participants’ intentions may have quite quickly reverted to the intentions they reported at the start of the session, meaning that it was this first measure that moderated the effects of the implementation intentions. Indeed, temporal stability of intentions has been shown to moderate the relationship between intentions and behaviour, with more stable intentions being better predictors of behaviour (Cooke and Sheeran, 2004). In the current study, intentions reported after participants had read the information sheet were less closely correlated with behaviour compared to intentions reported at the start of the session. This finding supports the interpretation that the second measure of intentions was either less valid or reflected less stable intentions than the measure at the start of the session.
The results also showed no significant effects of implementation intentions on dental gum chewed within 30 minutes of eating or drinking. Since the means for this measure were in the predicted direction, it is possible that the study was simply underpowered to detect such effects and/or these reports may have been more subjected to inaccuracies stemming from recall errors. Nevertheless, it would be important for future research to confirm that implementation intentions can increase the use of dental gum after eating and drinking rather than just use in general.
It would also be helpful for future research to look at the effects of implementation intentions among individuals most likely to benefit from chewing dental gum, especially given the social gradient in dental health (White et al., 2012). The current study recruited participants from in and around the university. Thus, they may have been more likely to already engage in good oral health care behaviours, and we took no measures of dental health to assess this. Examining effects among more at-risk populations would help better establish the real-world utility of using implementation intentions to improve oral health. Given that implementation intentions tend to be more effective among those with lower self-regulatory skills (Allan et al., 2013; Gollwitzer and Sheeran, 2006), it is possible that effects may even be stronger.
In future studies, researchers may also want to consider giving gum to participants at the start of their appointment rather than at the end, as it is possible that the measures of intention collected in the current study in part reflected participants’ access to gum. In particular, participants may have reported weak intentions to chew gum simply because they did not possess any gum and did not anticipate buying any. Providing the gum at the start of the appointment could thus result in more valid measures of intention.
Given the relative simplicity of implementation intentions, they could be used by oral health care providers and future research could examine effects on outcomes such as plaque and decay. However, it is important to consider how this type of intervention might be delivered in an applied setting. For example, if providing individuals with gum is considered too costly or impractical, it would be important to test the effects of implementation intentions when no gum is given. This approach may be less effective due to additional barriers for participants, such as cost and remembering to purchase gum. However, more benefits may occur where gum is provided for a longer period since this may help ensure there is sufficient time for the behaviour to become a habit (Lally et al., 2010). Since habits are quite resistant to change (Neal et al., 2011), this could help sustain the behaviour over long term. The current study only looked at gum chewing over 7 days and we do not know to what extent the increases continued beyond this period.
In summary, this study showed that implementation intentions can promote the use of dental chewing gum among motivated individuals. However, further research would be needed to establish the utility of implementation intentions in oral health care settings.
Footnotes
Acknowledgements
The authors would like to thank those who took part in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.